83
Dr. Ken Madden Associate Professor Division of Geriatric Medicine Department of Medicine University of British Columbia
Dr. Ken Madden Associate Professor
Division of Geriatric Medicine Department of Medicine
University of British Columbia

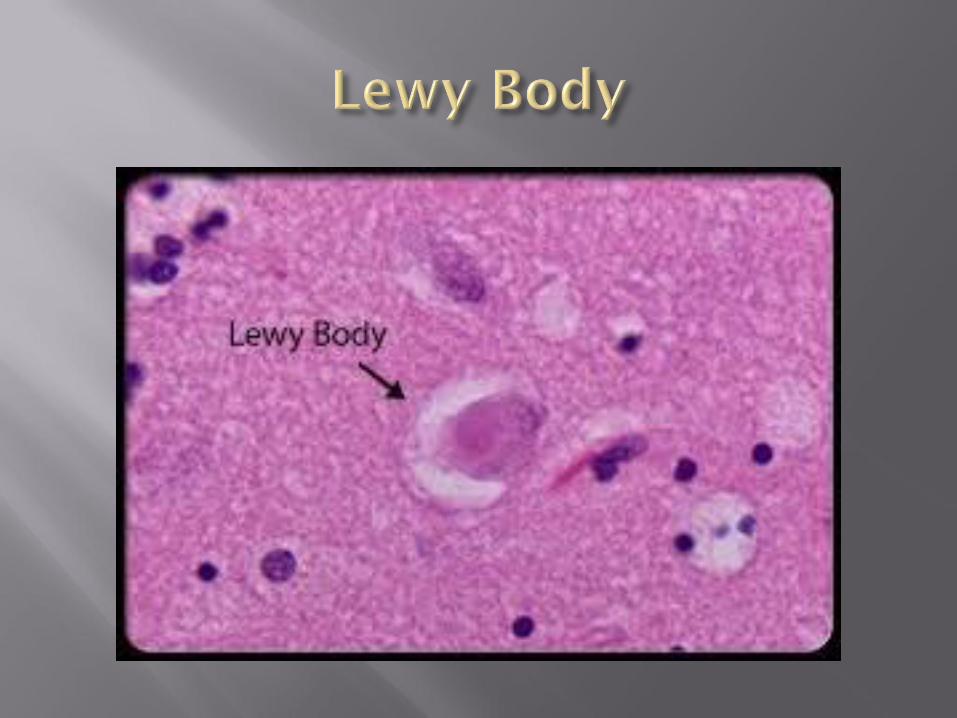
abnormal intracytoplasm inclusions
Noted in 1912
In a patient with Parkinson’s Disease
In 1961, Okazaki first described a relationship between the presence of cortical Lewy bodies and dementia
In 1984, Dr. Kosaka
Suggested new disease entity, which they termed ‘diffuse Lewy body disease’
Epidemiology of DLB
―Standard‖ Presentation, why problematic
Examples of Nonstandard presentations (―Actually Standard‖)
Diagnositic Criteria and Evidence
Case-based Examples of Presentations
Evidence for Treatments
Dementia of Lewy Body (DLB) is the second most common neurodegenerative dementia
Range of 10 to 22 percent of dementia cases
Prevalence of 0.7 percent of subjects over 65 years of age
J Neurol Neurosurg Psychiatry 2003;74:720-724
Mean age at presentation—75 years
Possible predilection for men
Up to 66 percent
Often overlooked due to heterogeneous presentation
J Neurol Neurosurg Psychiatry 2003;74:720-724
76 year old woman
Presents with slowly progressive decrease in short term memory over 3 years
3 year history of difficulty walking
Course seems quite variable
Fluctuates up and down throughout the day, becoming quite confused occasionally
Family physician gave a ―pill to calm‖and patient became very confused
Physical exam shows extrapyramidal signs
Increased tone
Shuffling, unsteady gait
No tremor
The problem with classic presentations is that they aren’t as common as one would like
Criteria are useful
Mixed bag of symptoms makes DLB diagnosis difficult
Progressive dementia
deficits in attention and executive function are typical. Prominent memory impairment may not be evident in the early stages.
Fluctuating cognition with pronounced variations in attention and alertness
Recurrent complex visual hallucinations
Spontaneous features of Parkinsonism.
REM sleep behaviour disorder (RBD), which can appear years before the onset of dementia and Parkinsonism
Severe sensitivity to neuroleptics occurs in up to 50% of LBD patients who take them
Low dopamine transporter uptake in the brain's basal ganglia as seen on SPECT and PET imaging scans

Repeated falls and syncope (fainting)
Transient, unexplained loss of consciousness
Autonomic dysfunction
Hallucinations of other modalities
Visuospatial abnormalities like depth perception, object orientation, directional sense and illusions
Other psychiatric disturbances like systematized delusions, aggression and depression.
A probable LBD diagnosis requires:
Dementia plus two or more core features
Dementia plus one core feature and one or more suggestive features.
A possible LBD diagnosis requires:
Dementia plus one core feature
Dementia plus one or more suggestive features
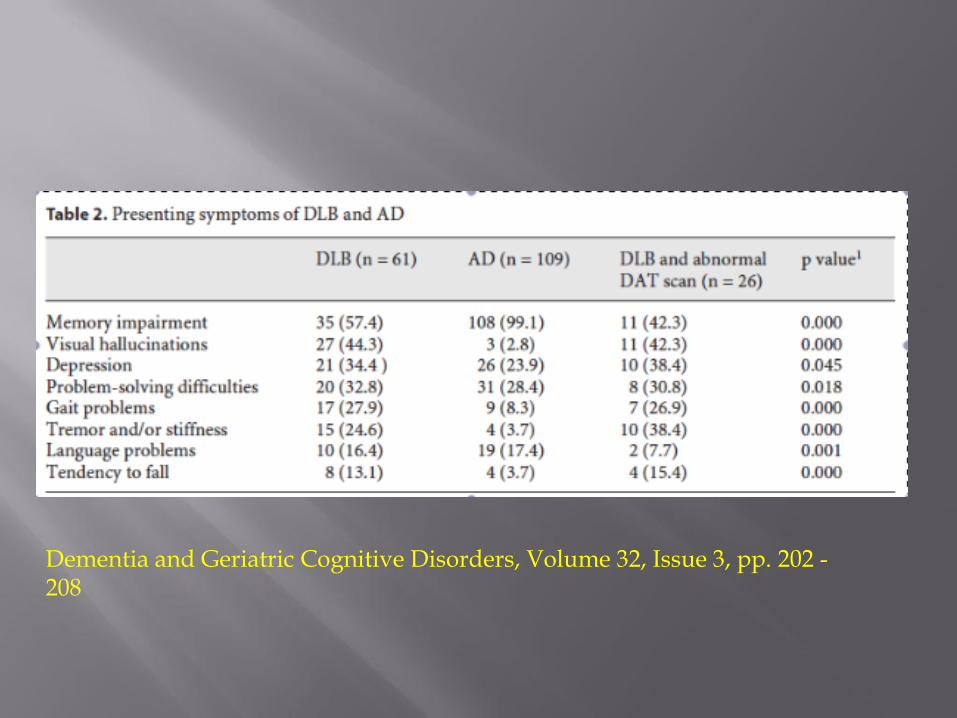
Dementia and Geriatric Cognitive Disorders, Volume 32, Issue 3, pp. 202 - 208

Litvan et al., Mov Desord 2003; 18:467-86
Fluctuating levels of consciousness over a background of progressive deterioration
Easier said than recognized
combination of cortical and subcortical
substantial attentional deficits
frontosubcortical and visuospatial dysfunction
Memory complaints less
DLB do better than those with Alzheimer’s disease on tests of verbal memory but worse on visuospatial performance tasks
Late stages impossible to tell

Can be over minutes, hours or days
In 50 to 75% of patients
Caregiver reports
Formal testing
I honestly have a hard time outside of inpatient unit
70 year old man who lives on a ranch outside of Burns’ Lake
Progressively started ―acting weirder‖ over the last year
Started seeing people and animals that weren’t there
2 days ago had hallucination wild dogs were attacking his family and biting his hands
Ran around his farmhouse shooting at the dogs with a shotgun
RCMP called, scene from Chuck Norris movie ensues

Admitted to hospital (obviously)
Physical exam shows cogwheeled rigidity, shuffling gait
Mild cognitive dysfunction
25/30
Temporal spatial, attention
Usually visual
3-dimensional
Detailed and vivid
Often frightening
Usually patient believes they are real
Generally mute
Visual hallucinations are associated with greater deficits in cortical acetylcholine
Predicts better responses to cholinesterase inhibitors (abstract only)
hallucinators (n=66) and non-hallucinators (n=23)

Lewy bodies in the posterior temporal lobes and amygdale are associated with hallucinations
These areas involved in emotion and visual processing
A.J. Harding, et al. Brain, 125 (Pt. 2) (2002), pp. 391–403
Postulated irritant effect?
A.J. Harding, et al. Brain, 125 (Pt. 2) (2002), pp. 391–403
30–50% of DLB patients
Ninety-four patients were included (15 with DLB, 36 with PDD, 26 with PD, 17 with Alzheimer's disease
A.J. Harding, et al. Brain, 125 (Pt. 2) (2002), pp. 391–403
Severe neuroleptic sensitivity only occurred in patients with Lewy body disease: DLB (8 [53%]), PDD (14 [39%]), and PD (7 [27%])
did not occur in Alzheimer's disease
(p = .006)
Family brings to family doctor
9 month history of memory issues
Losing objects
Also hallucinations of dead relatives
Delusions of theft

Cognitive testing shows mild memory impairment
Prominent inattention and temporalspatial issues
Cognition fluctuates, according to caregivers
Physical exam shows no extrapyramidal signs
Gait normal
Can this be DLB?
Presesentation is subjectively quite different
Poorly studied
Retrospective analysis of case notes of 21 autopsy patients with DLB and 37 cases with AD
McKeith IG, et al. Psychol Med. 1992 Nov;22(4):911-22.
At the time of diagnosis
50% of DLB patients have extrapyramidal motor symptoms
75% developing them during some stage of the disease course
McKeith IG, et al. Psychol Med. 1992 Nov;22(4):911-22.
Arbitrary rule
Patients with DLB must develop motor symptoms within 1 year of cognitive symptoms
Otherwise, need to consider parkinson’s associated dementia
Rule is neat and tidy
Unfortunately from the book of made up medicine in the sky
Wife bring in to doctor
―Driving her crazy at night‖
Numerous night time issues
Moving around
Flailing arms
Sleep walking
Sleepy during the daytime
Patient denies any of this
REM behavioural disorder is the most common one
A lack of muscle atonia in combination with vivid dreams
Usually diagnosed on history
Another option is increased EMG activity during sleep study
To date, no RCTs to guide us
Numerous agents suggested
Cholinesterase inhibitors
Sedatives (danger)
Melatonin
Quetiapine
Modify sleep environment for safety!
DLB association website has excellent suggestions for caregivers
His wife brings him back, and says he is falling down
Feels light headed when standing up
Physical exam shows orthostatic hypotension

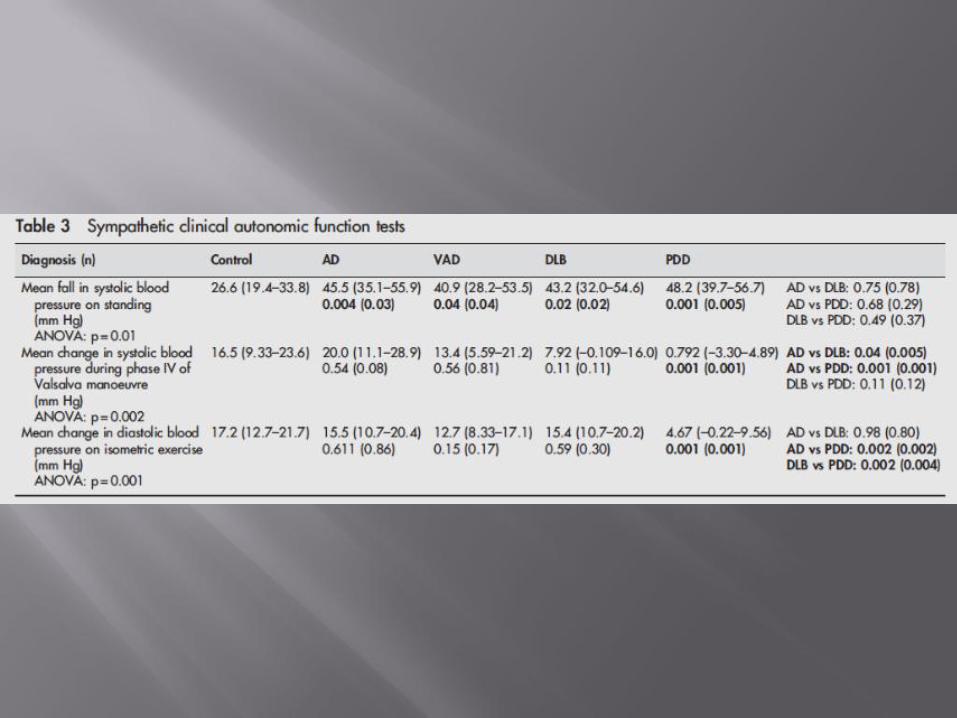
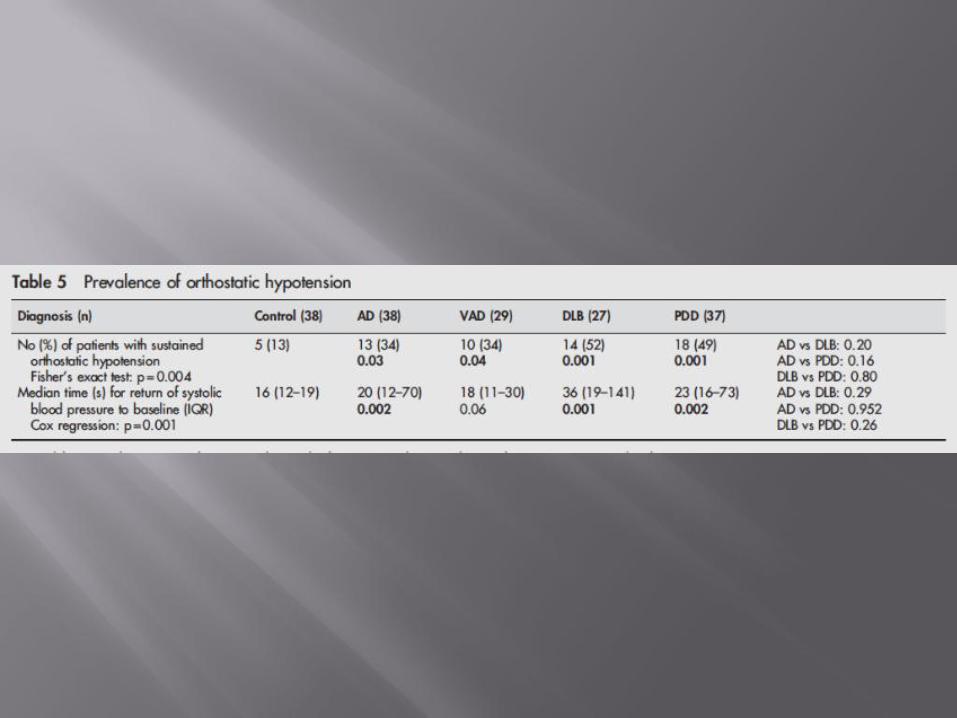
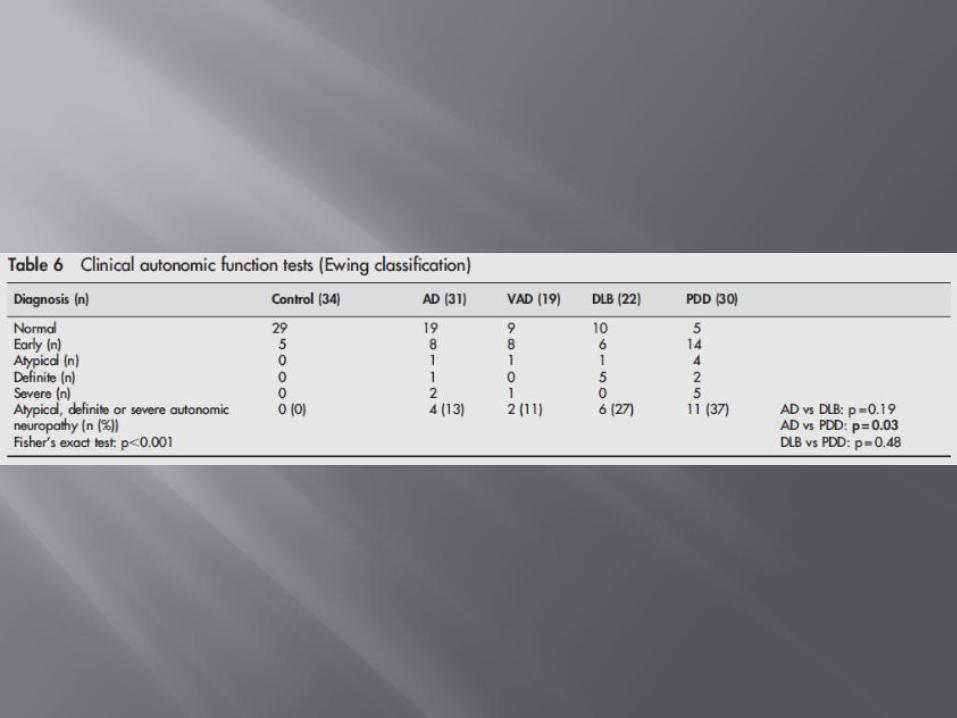
DLB has been associated with autonomic instability
Most common manifastation is orthostatic hypotension or urinary incontinence
39 patients with AD
30 with VAD
30 with DLB
40 with PDD
38 elderly controls
Ewing’s battery of autonomic function tests
HRV testing
Kenny et al, J Neurol Neurosurg Psychiatry 2007;78:671–677

Based on limited evidence
Symptomatic
Targeted at specific symptoms
No disease-modifying agents
Survival time in DLB is a mean of 7.7 years (compared with 9.3 years with AD)
Shorter time to institutionalization
First line therapy
Limited evidence for
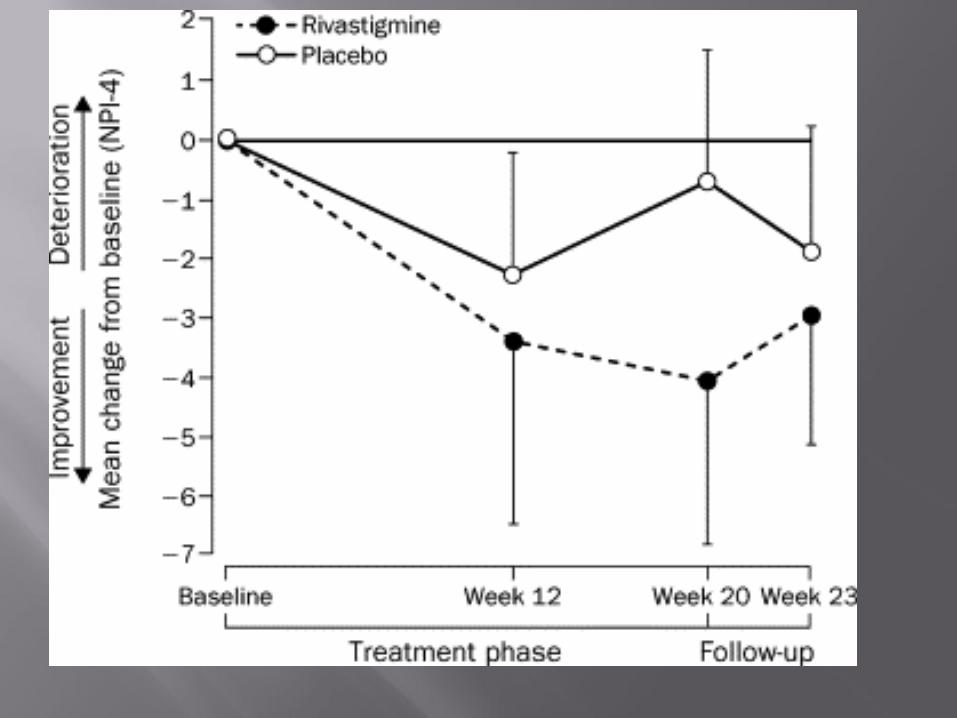
Rivastigmine
Donepezil
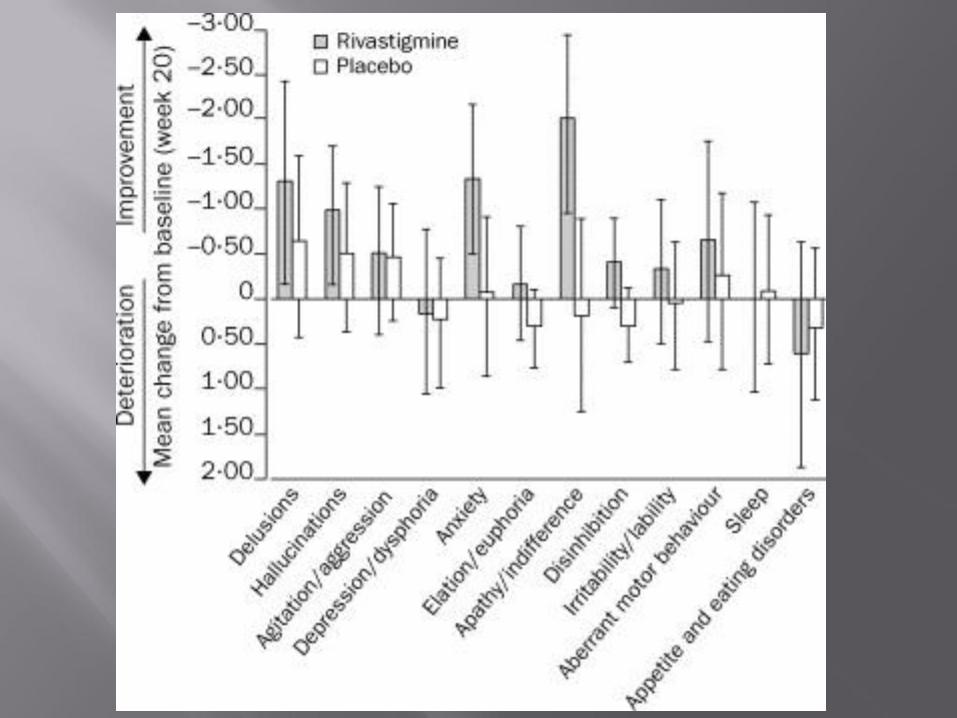
Benefits reported for
Cognition
Fluctuations
Apathy, indifference
Psychotic symptoms
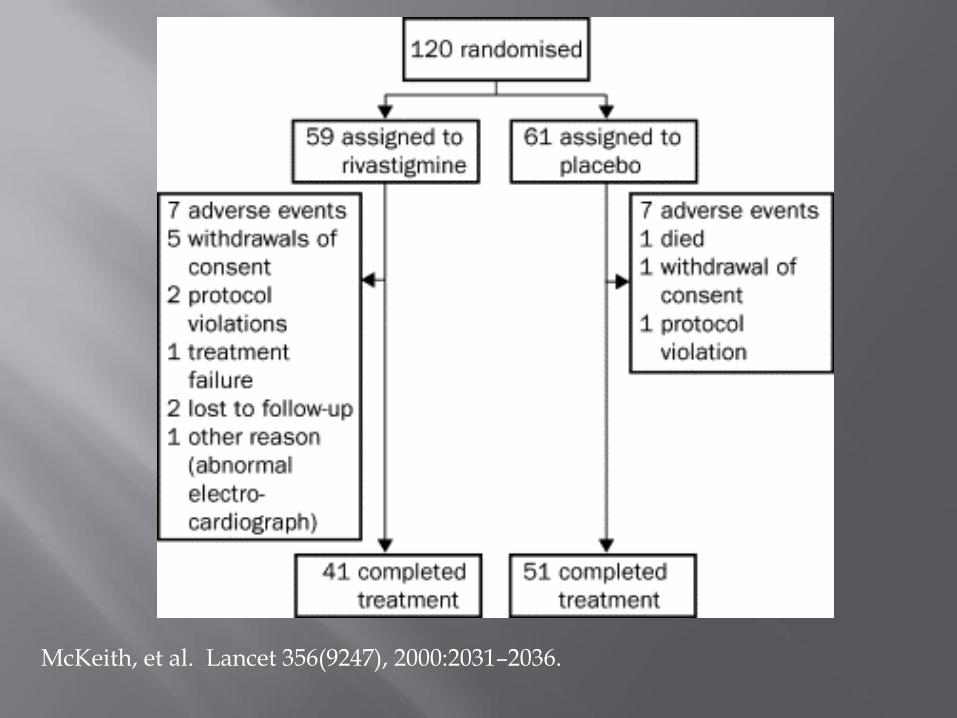
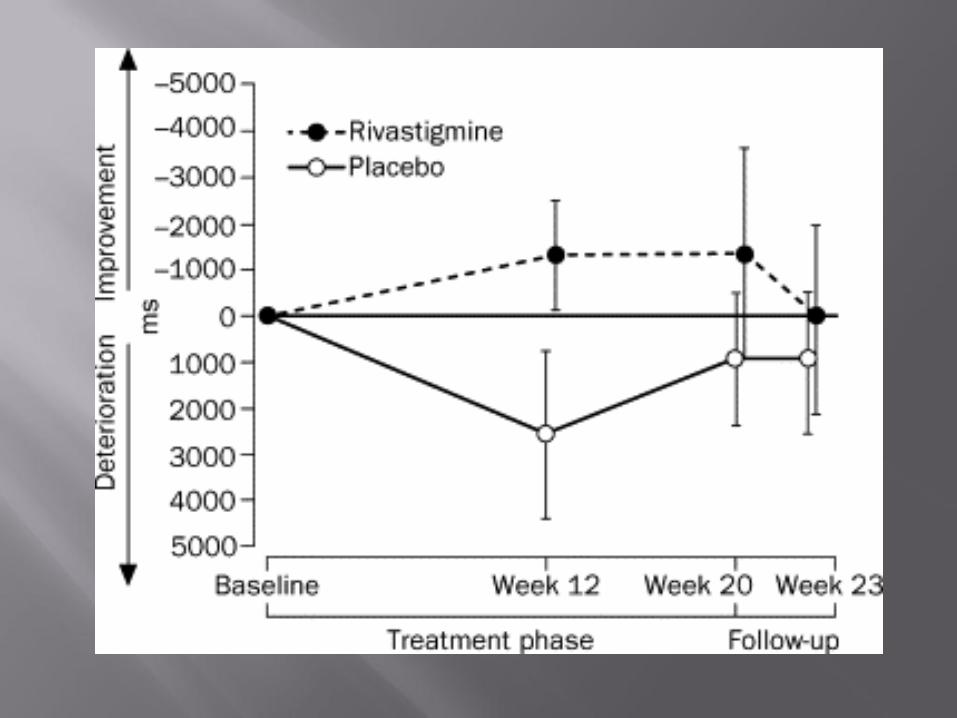
McKeith, et al. Lancet 356(9247), 2000:2031–2036.
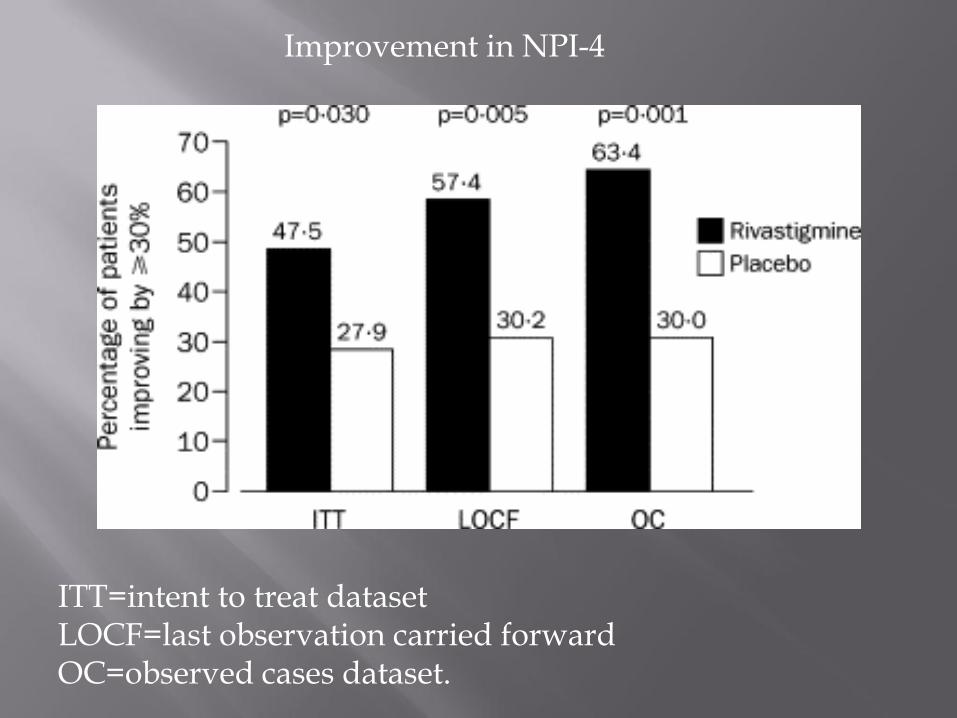
ITT=intent to treat dataset LOCF=last observation carried forward OC=observed cases dataset.
Improvement in NPI-4
Case reports of worsening
Cognitive function
REM sleep disorder
Parkinsonism
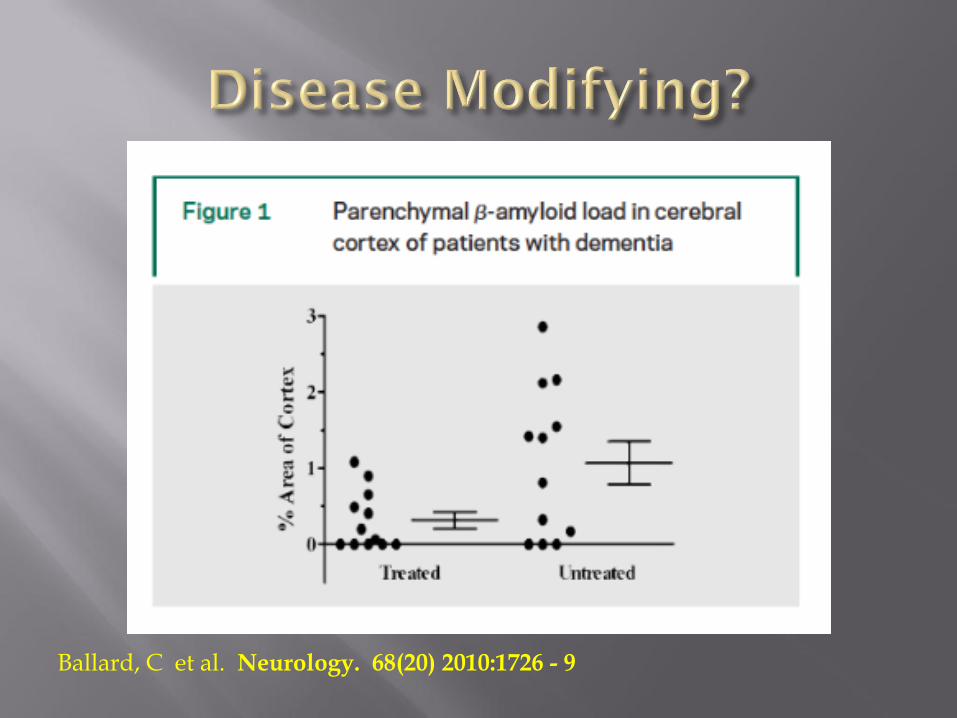
Ballard, C et al. Neurology. 68(20) 2010:1726 - 9
Improved outcomes on primary outcome measure
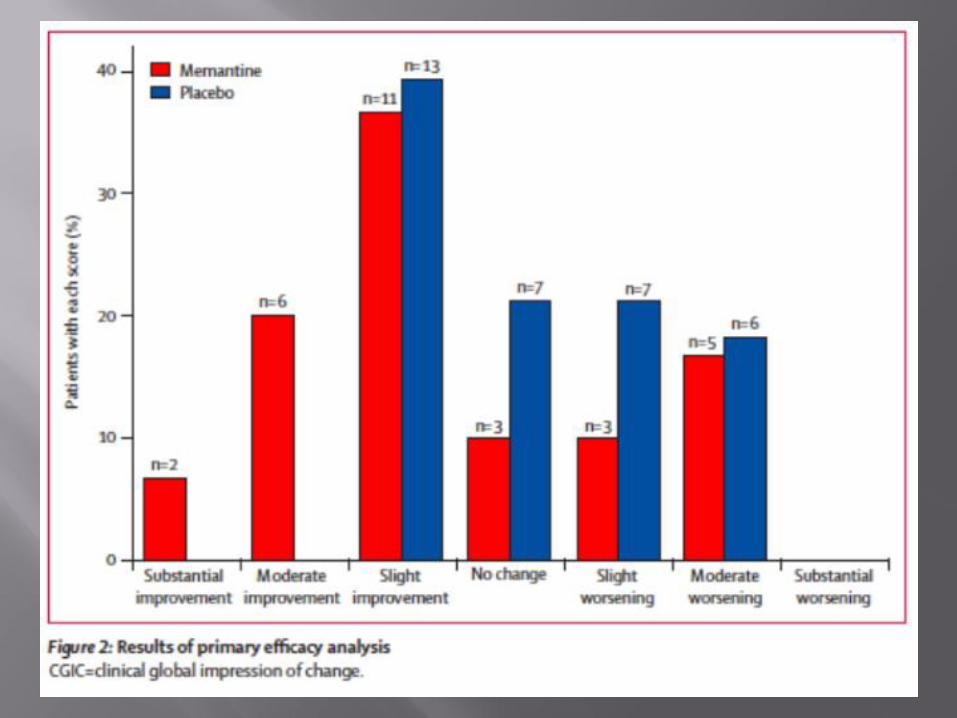
Clinical global impression of change
No improvements on any other secondary outcomes
Recruited DLB or PD-related dementia

Case reports of worsening
Delusions
Hallucinations
What about neuroleptics?
Severe neuroleptic reactions are characteristic of the disease
Exacerbation of: Parkinsonism
Confusion
Autonomic Dysfunction
Consider Cholinesterase inhibitor first or lower dose of dopaminergic agent
Use only atypical antipsychotics and at lowest possible dose
Quetiapine
Olanzapine
Risperidone
Cloazapine (neutropenia)
Switch agents instead of raising dose
Nonpharmacological interventions
Anticholinesterase inhibitors
Atypical Antipsychotics
NEVER:
Benzodiazapines (except maybe REM sleep disorder)
TCAs
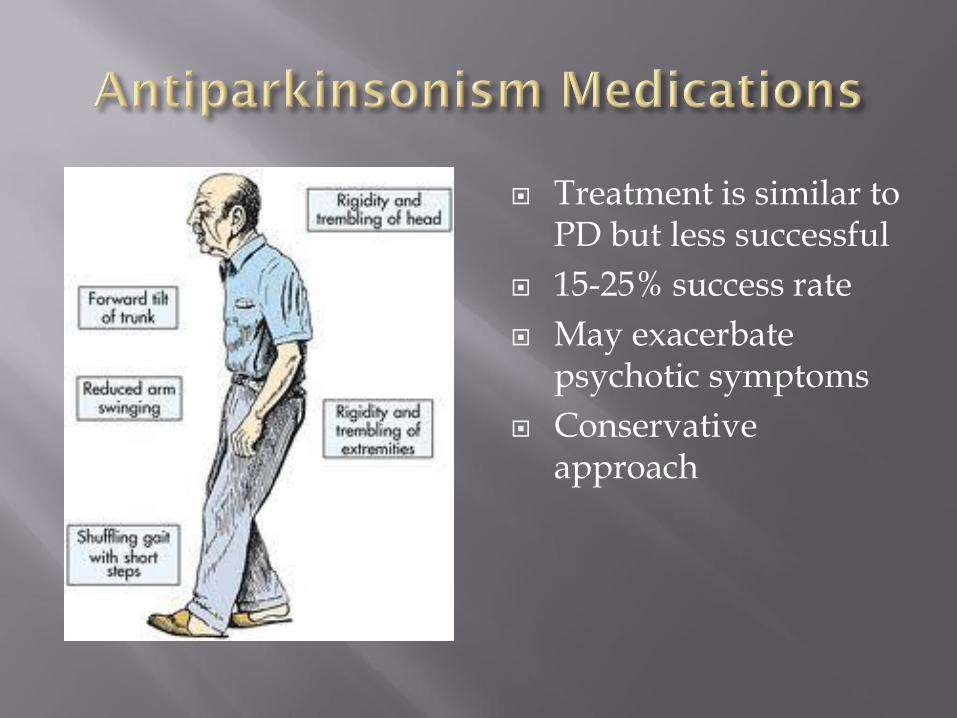
Treatment is similar to PD but less successful
15-25% success rate
May exacerbate psychotic symptoms
Conservative approach

Carbidopa-levodopa 25/100 mg
One-half tablet po tid
Titrate slowly over several weeks as tolerated

Dopamine agonists tend to be poorly tolerated
Anticholinergic agents are contraindicated
Standard therapies
High salt
Leg stockings
Fludrocortisone
Midodrine
Avoid anticholinergic agensts