53
Dr. Kıvanç Metin Dokuz Eylül University Faculty of Medicine Department of Cardiovascular Surgery Izmir, TURKEY

Dr. Kıvanç Metin
Dokuz Eylül University Faculty of Medicine
Department of Cardiovascular Surgery
Izmir, TURKEY

ECMO or ECLS
• ECMO = Extra Corporeal Membrane Oxygenation
• ECLS = Extra Corporeal Life Support
• ECCO2R = ExtraCorporeal CO2 removal
• ECLA = ExtraCorporeal Lung Assist
• PALP = Pump Assisted Lung Perfusion
• PECLA = Pumpless ExtraCorporeal Lung Assist
ECMO
• oxigenación extracorpórea con membrana
• Extrakorporale Membranoxygenierung
• extracorporeal membrane oxygenation
• 活体外部的膜氧化
• .الجسم من الخارجة الدموية للدورة األكسجة غشاء
• Εξωσωματική οξυγόνωση μεμβράνης
• ऑक्सिजनीकरण अवायवीय extracorporeal झिल्ली • 멤브레인 extracorporeal oxygenation
• 膜酸素化能体外
• экстракорпоральные оксигенаторы мембранной оксигенации
• سيار extracorporeal اينطور مچنين

Popularity
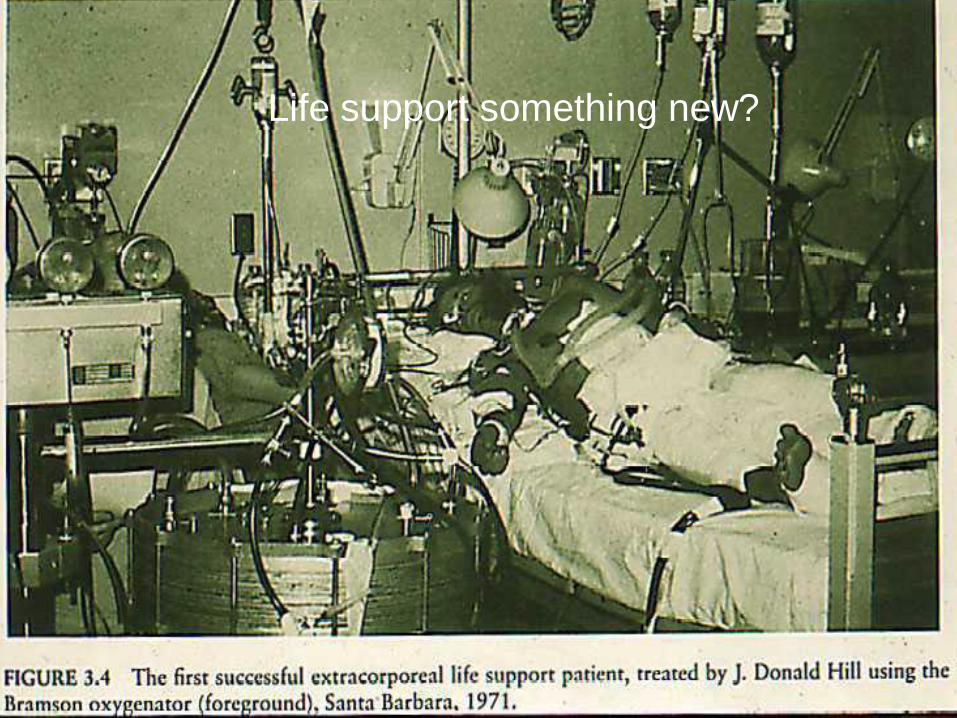
Life support something new?



Post Cardiotomy
Bridge to…

H1N1 Veno-Venous

• Provides cardiorespiratory support in patients
whose own cardiac and / or respiratory function is inadequate.
• Similar to what a cardiopulmonary bypass circuit provides during cardiac surgery.
WHAT DOES ECMO DO ?

• Take some blood out of the body
• Oxygenate / remove CO2
• Warm it back to body temperature
• Pump it back into the body
Respiratory
Support
Cardiac Support

WHEN? • Reversible Pathological Process
• Nature of the disease • Length of time already on mechanical ventilation
• Failure of maximal conventional medical therapy • Varies patient to patient • Varies between diseases • Varies center to center

HLS CANNULAE
DISPOSABLES
Arterial cannulae Venous cannulae

PERCUTANOUS INSERTION KIT
DISPOSABLES

Percutaneous cannulation
Accessing a peripheral
artery or vein via the
minimal invasive
“Seldinger Technique”
It does not involve any
surgical access
The skin should form a
tight seal around the
cannulae
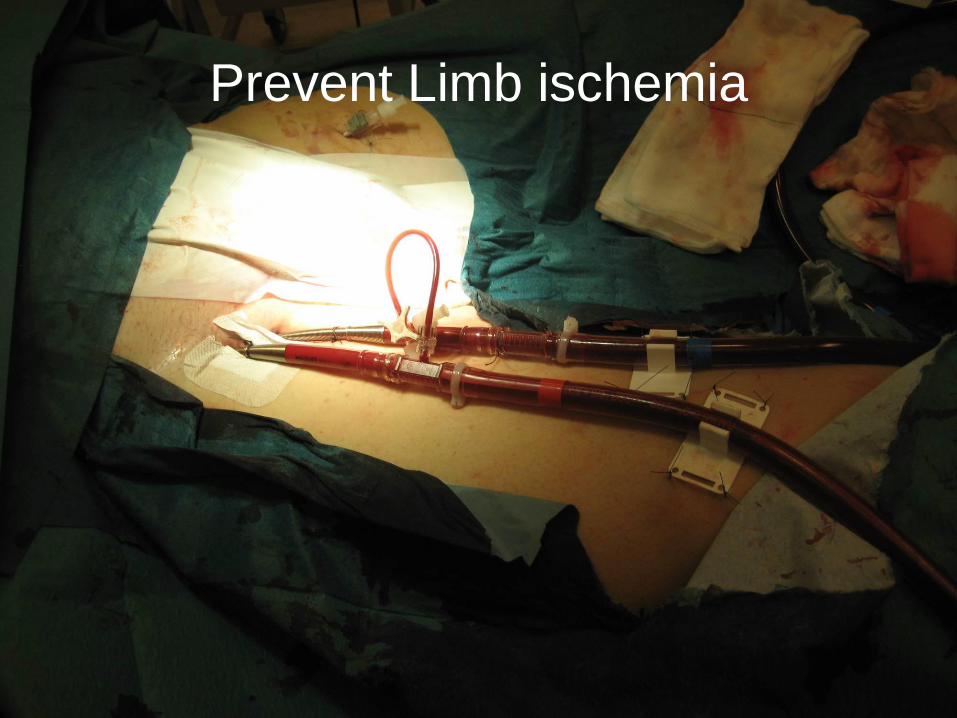
Prevent Limb ischemia

A simple method of vascular access to perform emergency coronary angiograhy in patients with veno-arterial extracorporeal membrane oxygenaton Dierk H. Endemann, Alois Philipp, Christian Hengstenberg et. al. Intensive Care Med published Oct. 2011
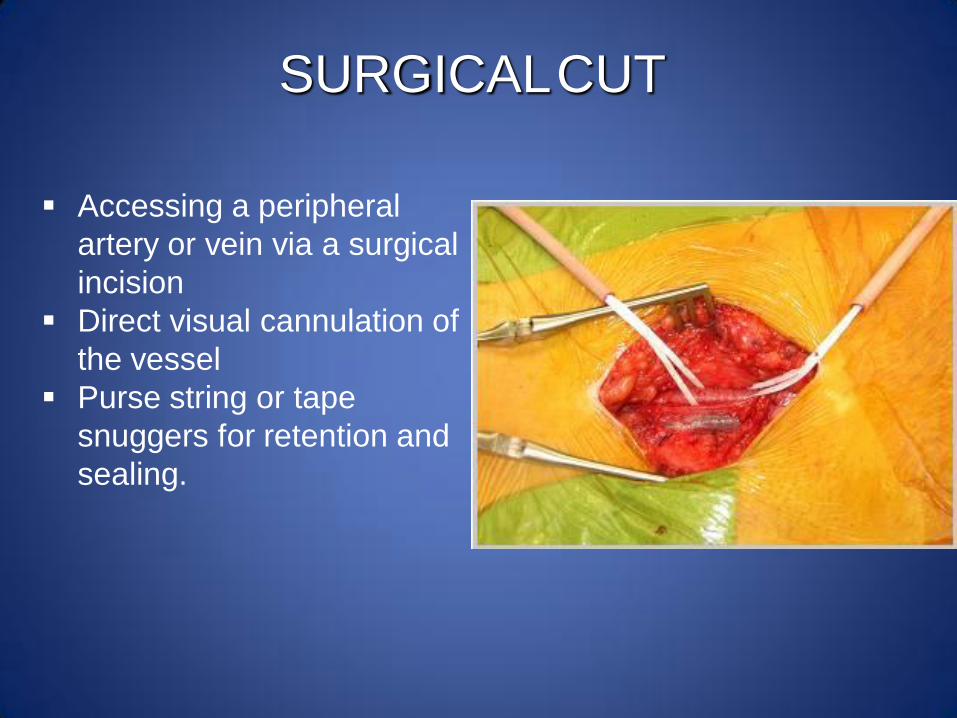
SURGICAL CUT
Accessing a peripheral
artery or vein via a surgical
incision
Direct visual cannulation of
the vessel
Purse string or tape
snuggers for retention and
sealing.
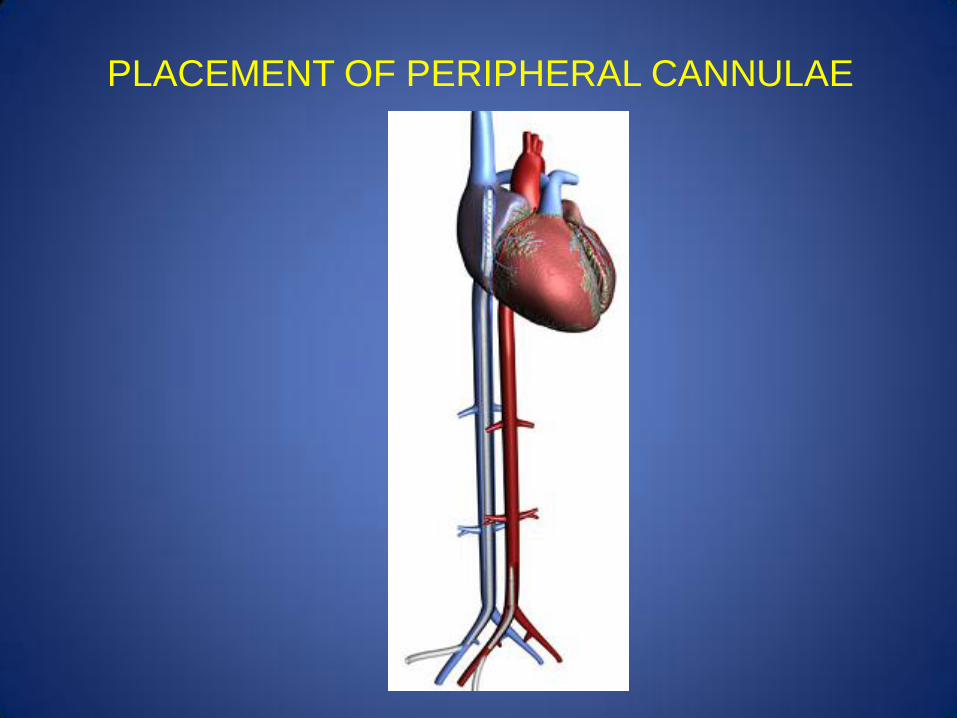
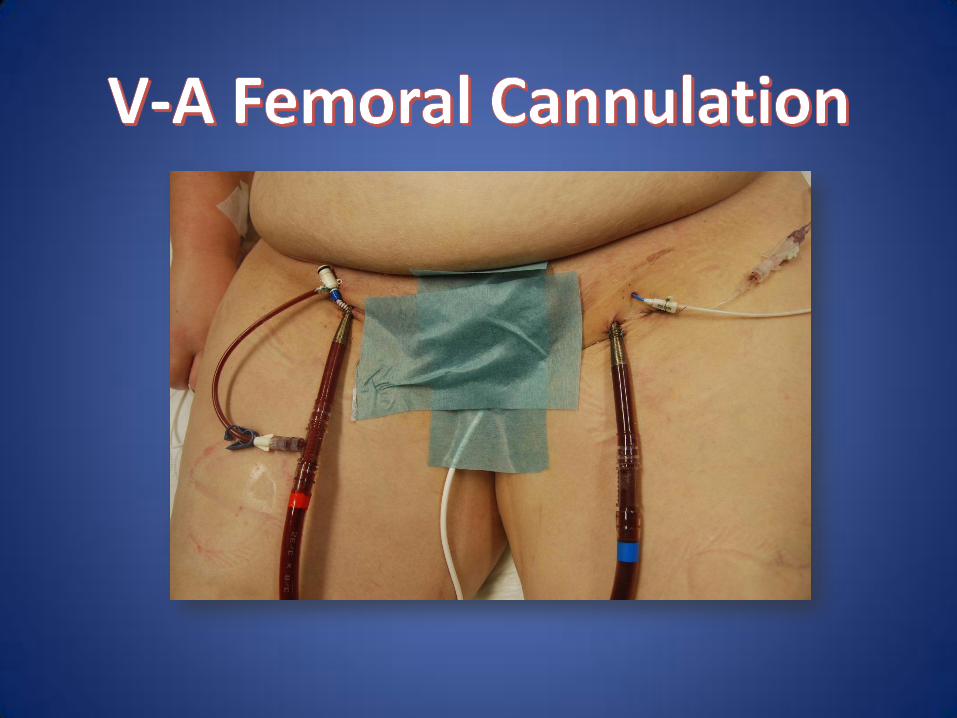
PLACEMENT OF PERIPHERAL CANNULAE

• VenoArterial (VA)
– Two cannulas
• Arterial – Right Common Carotid Artery to Aortic Arch
• Venous – Right Internal Jugular Vein to Right atrium
– Provides cardiac and respiratory support
– Sacrifices the Right Carotid Artery
– Can use femoral vessels in larger patients
ECLS CANNULATION

ECLS CANNULATION
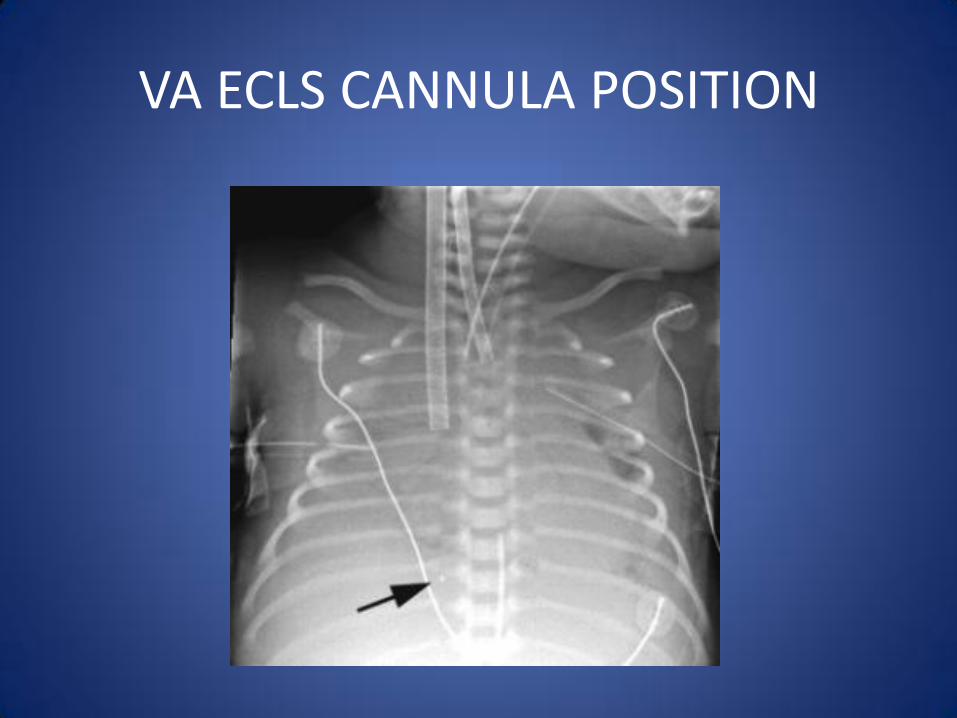
VA ECLS CANNULA POSITION
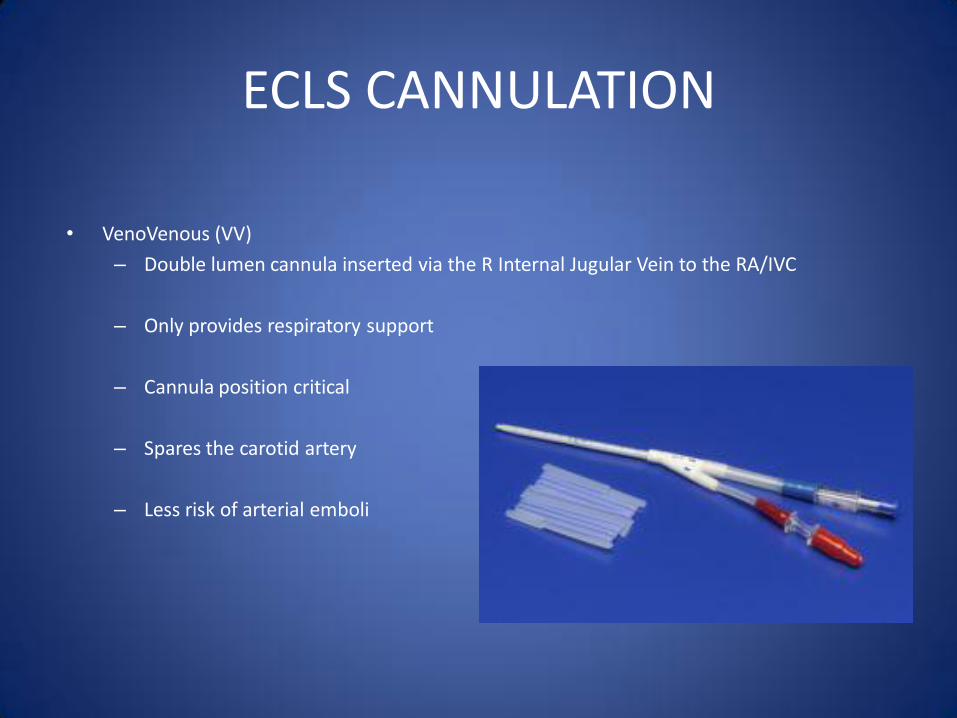
• VenoVenous (VV)
– Double lumen cannula inserted via the R Internal Jugular Vein to the RA/IVC
– Only provides respiratory support
– Cannula position critical
– Spares the carotid artery
– Less risk of arterial emboli
ECLS CANNULATION
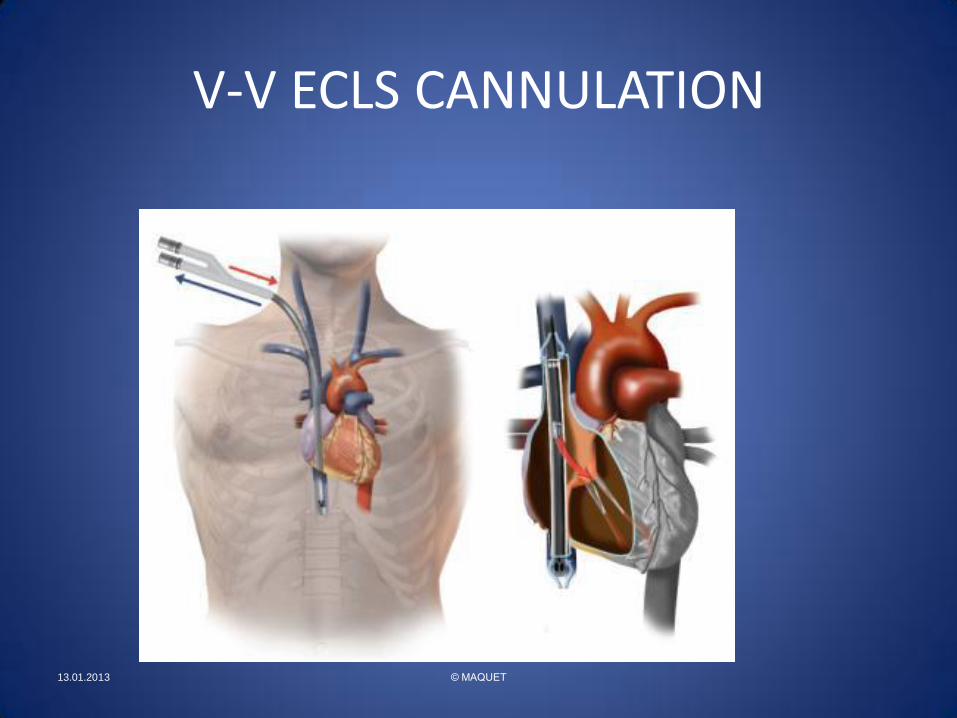
V-V ECLS CANNULATION
13.01.2013 © MAQUET

V-V ECLS CANNULA POSITION

Pulmonary failure Circulatory failure
V-v ECMO V-a ECMO
4 essential components:
1. Vascular access (percutaneous dilatational technique)
2. Pump
3. Membrane oxygenator
4. Tubing
Extracorporeal Modality

Low hemolysis without heat generation No stagnant areas No leakage possible High durability
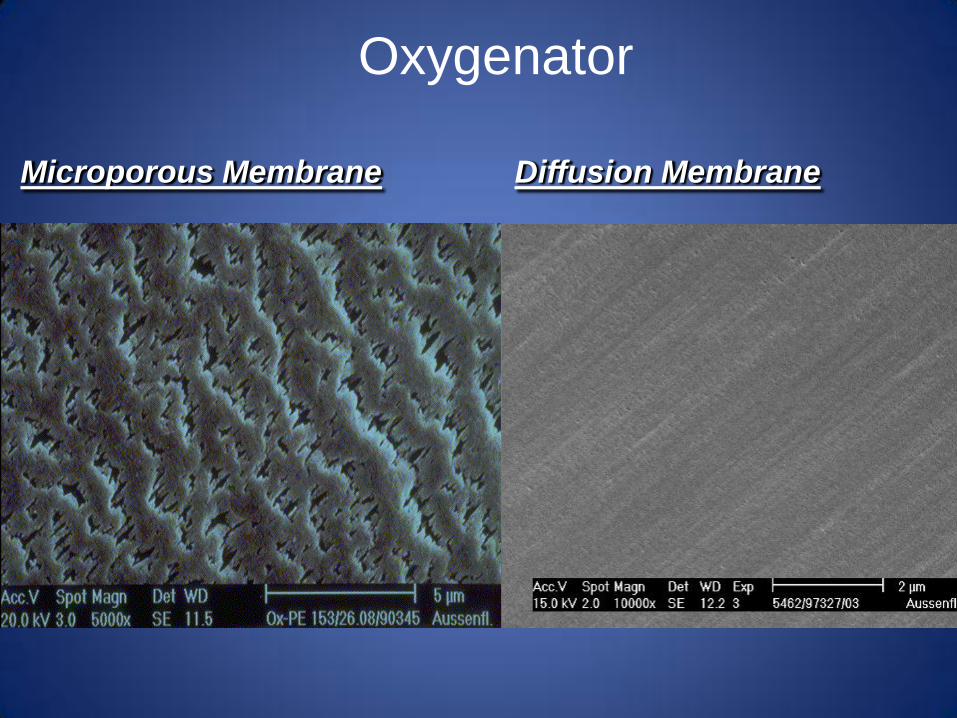
Oxygenator
Microporous Membrane Diffusion Membrane
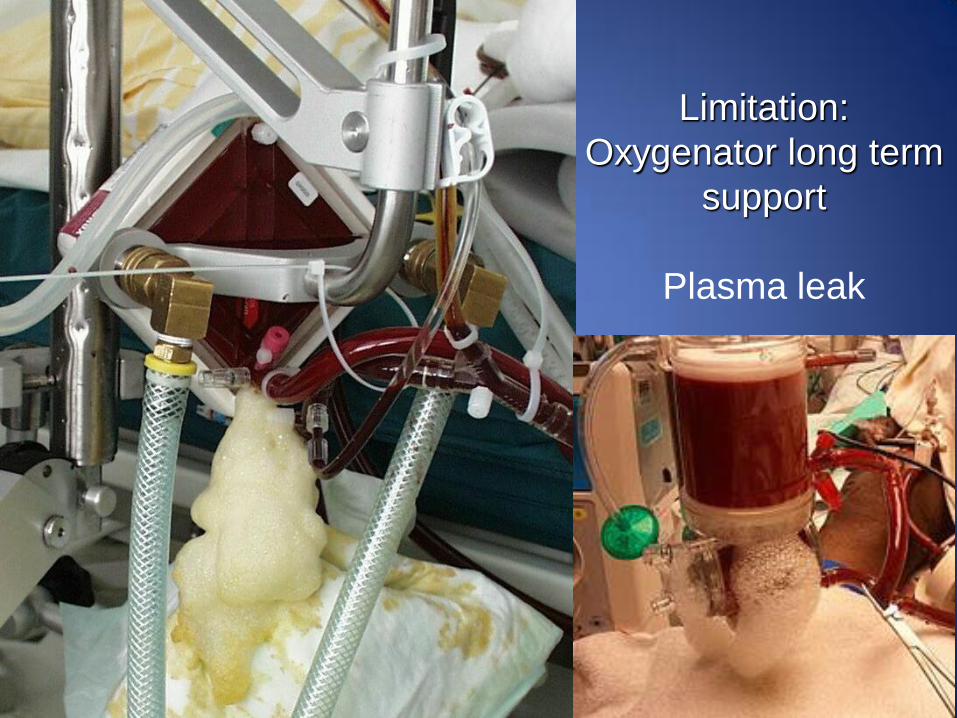
Limitation:
Oxygenator long term
support
Plasma leak
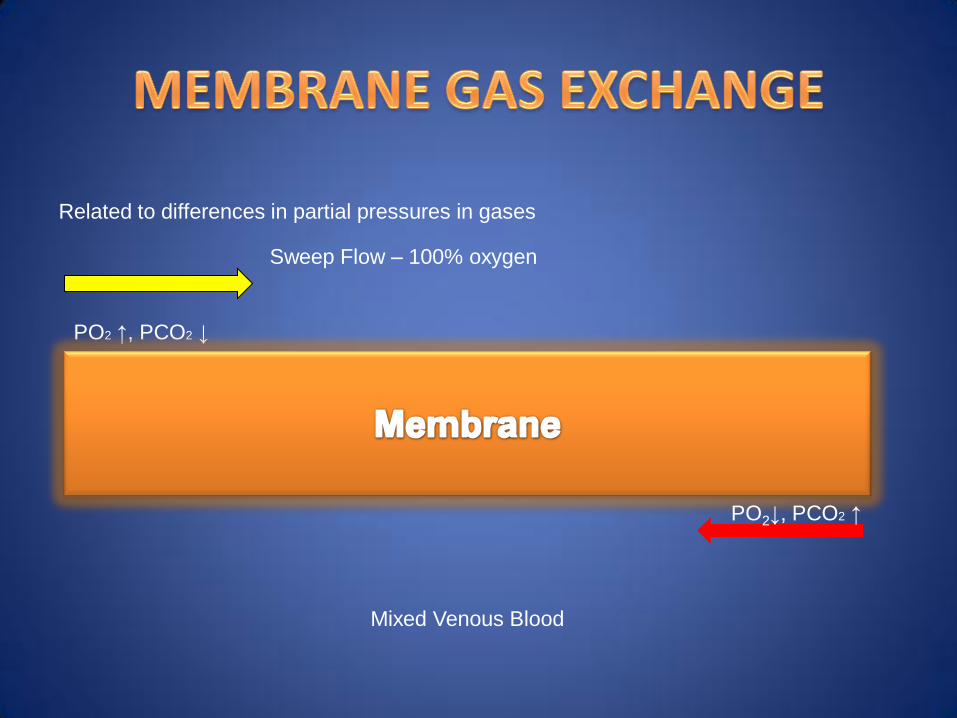
Related to differences in partial pressures in gases
Sweep Flow – 100% oxygen
PO2 ↑, PCO2 ↓
PO2↓, PCO2 ↑
Mixed Venous Blood

Veno – Arterial ECLS THERAPY
in cases of serious cardiac insufficiency and/ or
respiratory failure.

Veno – Venous ECLS THERAPY
ARDS (Acute Respiratory Distress Syndrome) as a result of:
pneumonia, sepsis, multiple trauma or aspiration without
serious cardiac failure.

Arterial-Venous ECLS
gas exchange disorders e.g. inadequate CO2 elimination.
Indications
• Primary reversible respiratory failure
• ARDS (H1N1)
• Severe pneumonia (Bacteria, Viral or aspiration)
• Acute lung failure following LTX
• Pulmonary contusion
• Smoke inhalation/ Burns
• Near drowning/ Hypothermia
• Reversible cardiogenic shock
• Non ischaemic cardiogenic shock
• Cardiomyopathy (bridge to longer VAD)
• Post cardiac surgery (unable to wean)
• Drug overdose or Sepsis profound cardiac depression
Contra indications
• Unlikely to be reversed in 10 – 14 days
• Multi-organ failure
• Severe irreversible brain injury
• Significant CPR (out of Hospital arrest)
• Contraindication to anticoagulation (Hep. İnd.T, multitrauma)
• Uncontrolled metabolic acidosis
• Terminal disease / malignancy
• Chronic lung disease
• Chronic myocardial dysfunction
• Immunosuppression

Relative contraindications
• Mechanical ventilation >6 days
• Septic shock
• Severe pulmonary hypertension
(MPAP >45 or >75% systolic)
• Cardiac arrest
• Acute, potentially irreversible myocardial
dysfunction
CLINICAL APPLICATIONS
• Meconium Aspiration Syndrome
• Persistent Pulmonary Hypertension
• Hyaline Membrane Disease
• Pneumonia
• Sepsis
• Pulmonary Air Leak
• Congenital Diaphragmatic Hernia
Neonatal Respiratory Diseases
• Post-operative cardiopulmonary failure
• Post-operative cardiac transplant
• Myocarditis
• Cardiomyopathy
CLINICAL APPLICATIONS Cardiac Diseases
• Average run length depends on the reason for cannulation
– Shorter for PPHN, Meconium Aspiration, HMD
• ~5 – 7 days
– Longer for CDH, Sepsis
• ~7 – 14 days
• Can be on ECMO for longer
– ECMO Circuit has more risk of failure
– More likelihood of inability to survive without ECMO
HOW LONG?
SELECTION CRITERIA
• Cardiovascular / Oxygen Delivery Criteria
• Plasma lactate: >45 mg/dl (5 mM/L) and not improving, despite volume expansion and inotropic support.
• Inotropic equivalent (IE) >50 for 1 hour or >45 for 8 hours.
IE = DOPamine(mcg/kg/min) + DOBUTamine(mcg/kg/min) + EPInephrine (100Xs mcg/kg/min) + NORepinephrine (100Xs mcg/kg/min) + ISOproterenol(100Xs mcg/kg/min) + MILrinone (15Xs mcg/kg/min).
• Mixed Venous Sat of <55% for 30 min.
• Rapidly deteriorating or severe ventricular dysfunction
• Intractable arrhythmia with poor perfusion
• Cardiac Arrest
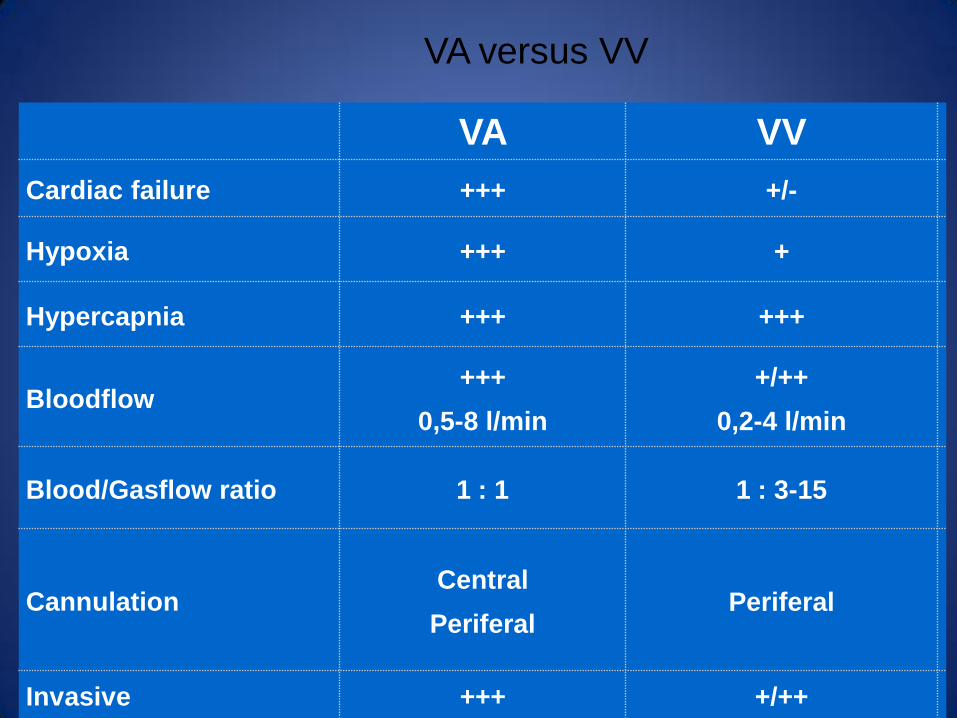
VA versus VV
VA VV
Cardiac failure +++ +/-
Hypoxia +++ +
Hypercapnia +++ +++
Bloodflow +++
0,5-8 l/min
+/++
0,2-4 l/min
Blood/Gasflow ratio 1 : 1 1 : 3-15
Cannulation Central
Periferal
Periferal
Invasive +++ +/++

Complications in ECLS
• Anticoagulation: Clotting PLS, Bleeding
• Vessel (Bleeding, Infection, ischemia, dislodgement Cannula)
• Air (Emboli)
• Volume management patient
• Steal effect
• Sepsis
• Renal failure
• Decubitis ulcers
• Neurologic damage
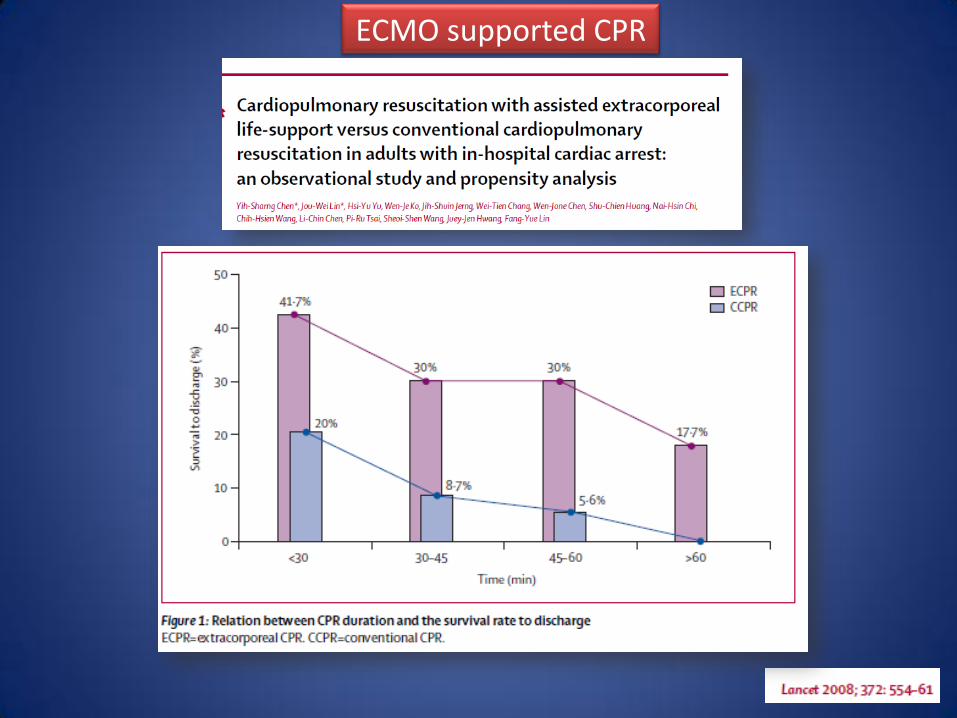
ECMO supported CPR


Patient Management during ECLS
• Anticoagulation – First 12 h after CPB: No hep. necessary
– After 12h, blood loss <5ml/h: Hep IV 400 IU/h
– No prev. CPB: 5000 IU bolus.
– Monitoring: • APTT 55-60
• ACT 180
• Ratio Ventilation PLS/ Respirator
• Gasflow
• Bloodflow
• Prone position
• Visual inspection of the system
Criteria for changing the system
• Massive deposition of fibrin, clots
• Severe hypoxia despite FiO2 100%
• Severe thrombopenia
• Massive Hemolysis
• Pump, Motor, Controller dysfunction

Insufficient anticoagulation

VA ECMO Weaning Protocol
• Hemodynamic stabilization
• Reducing Bloodflow under TEE monitoring
• Low flow < 2L/min -> Higher anticoagulation
VV ECMO Weaning Protocol
Weaning: Sweep gas flow set at 0 L/min Pump flow not modified
Adjust FiO2 and Vt on the respirator
PaO2 >60 mmHg, SaO2 >90% FiO2 on the respirator <60%
Inspiratory plateau pressure <30 cm H2O
if echocardiography reveals no signs of acute cor pulmonale
For at least 1-2 hours and up to 12 hours
Conclusion
ECMO
• Is not a therapy but always a bridge
To recovery
To decision
To transplant
• Has a high potential for complications
Bleeding
Leg ischemia
Thrombosis
Systemic emboli


















