57
DR. MARWA SHAALAN PHARM-D
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | felicia-brokenshire |
| View: | 218 times |
| Download: | 0 times |
DR. MARWA SHAALAN
PHARM-D
Basic functions of the respiratory system Breathing (Pulmonary Ventilation) – movement of air in and out
of the lungs Inhalation (inspiration) draws gases into the lungs. Exhalation (expiration) forces gases out of the lungs.
Gas Conditioning – as gases pass through the nasal cavity and paransal sinuses, inhaled air becomes turbulent. The gases in the air are • warmed to body temperature• humidified• cleaned of particulate matter
Gas Exchange - respiration• Supplies body with oxygen• Disposes of carbon dioxide
Produces Sounds
Protects respiratory surfaces
Site for olfactory sensation
Respiration – four distinct processes must happenPulmonary ventilation – moving air into and
out of the lungsExternal respiration – gas exchange
between the lungs and the bloodTransport – transport of oxygen and carbon
dioxide between the lungs and tissues Internal respiration – gas exchange
between systemic blood vessels and tissues
Respiratory organsNose, nasal cavity, and paranasal sinusesPharynx, larynx, and tracheaBronchi and smaller branchesLungs and alveoli

Figure 21.1
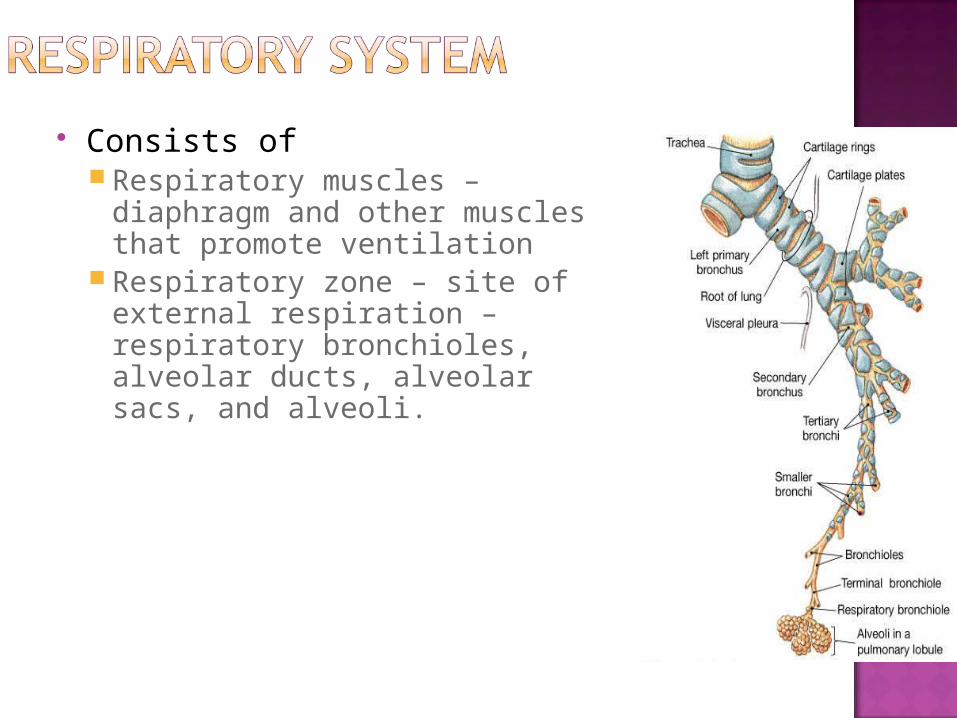
Consists of Respiratory muscles –
diaphragm and other muscles that promote ventilation
Respiratory zone – site of external respiration – respiratory bronchioles, alveolar ducts, alveolar sacs, and alveoli.
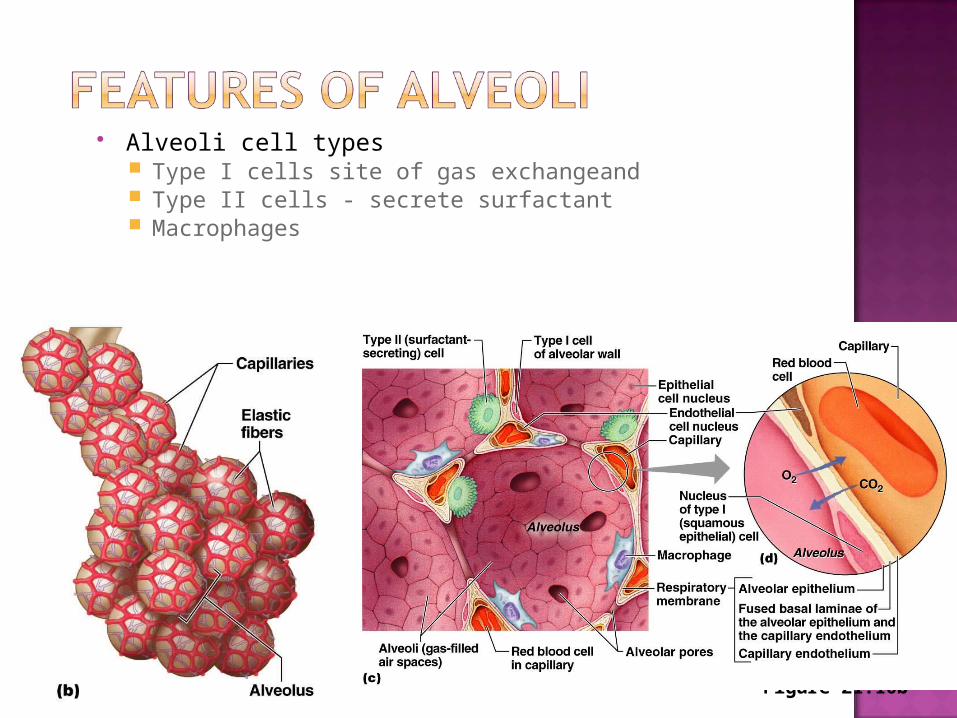
Alveoli cell types Type I cells site of gas exchangeand Type II cells - secrete surfactant Macrophages
Figure 21.10b
RESPIRATORY DISORDERS







TRIALS




-If it necessary – hospitalization with i/v infusion of glucocorticosteroids and euphyllin

Cough is a useful physiological mechanism that serves to clear the respiratory passages of foreign material and excess secretions.
It should not be suppressed indiscriminately.
There are, however, many situations in which cough does not serve any useful purpose but may, instead only annoy the patient or prevent rest and sleep.

Chronic cough can contribribute to fatigue, especially in elderly patients, in such situations the physicians should use a drug that will reduce the frequency or intensity شده of the coughing.
Cough reflex is complex, involving the central and peripheral nervous systems as well as the smooth muscle of the bronchial tree.

It has been suggested that irritation of the bronchial mucosa causes bronchoconstriction, which in turn, stimulates cough receptors( which probably represent a specialized type of stretch receptor) located in the tracheobronchial passages.
Afferent conduction from these receptors is via fibers in the vagus nerve; central components of the reflex probably involve several mechanisms or centres that are distinct from the mechanisms involved in the regulation of respiration.
The drugs that directly or indirectly can affect this complex mechanism are diverse.
-For example , cough may be the first or only symptom in bronchial asthma or allergy, and in such cases bronchodilators(e.g., 2 – adrenergic receptor agonists have been shown to reduce cough ) without having any significant central effects, other drugs act primarily on the central or the peripheral nervous system components of the cough reflex.
Forceful release of air from lungs
Sudden, often involuntary (protective) reflex and major defensive mechanism
Cont…..

Expulsion of respiratory secretion or foreign particles or irritant or excessive mucus from air passages
Symptom an underlying respiratory and/or cardiovascular pathology
Causes of cough :
A) Acute cough =lasting<3 weeksB) Chronic cough =lasing >8 weeks
Cough may be i) Un productive (dry) cough ORii) Productive cough (sputum)
cont.
Common cold, Upper/lower respiratory tract infection Allergic rhinitis Smoking Chronic bronchitis Pulmonary tuberculosis Asthma Gastroesophageal reflux Pneumonia Congestive heart failure Bronchiectasis Use of drugs (e.g., Angiotensin-converting enzyme inhibitors)

1) Antitussives (cough centre suppressants)
2) Expectorants (Mucokinetics)3) Mucolytics 4) Antihistamines5) Bronchodilators 6) Pharyngeal Demulcents

Drugs suppress cough & produces symptomatic relief
MOA Mainly suppress cough centre in medulla (both
central & peripheral effects) E.g., Opoid drugs (codeine, pholcodeine,
noscapine, dextromethorphan)Opioid = most effective for cough

Codeine= prodrug metabolized to morphine It is an alkaloid found in Opium poppy plant Has less addiction resp. centre depressant ↓ Has useful antitussiveaction at low doses (<15 mg) Produce drowsiness, thickening of sputum & constipation
Related to papaverine Do not have addictive, analgesic &
constipating properties Do not interfere with mucocilliary movement Noscapine (15 mg) & pholcodeine (10
mg)=syrup

Available in syrup, tablets, spray formsMOANMDA receptor antagonistUsesCough suppressant, temporary relief of
cough caused by minor throat & bronchial irritation (accompanies with flu & cold), pain relief
Ad Effects= Nausea, vomiting, drowsiness, dizziness, blurred vision

Act peripherally Increase bronchial secretion OR Decrease its viscosity facilitates its
removal by coughing Loose cough ►less tiring & more
productive
Cont….

Classified into b) Directly acting E.g., Guaifenesin (glyceryl guaiacolate),
Na+ & K+ citrate or acetate, b) Reflexly actingE.g., Ammonium salt
They act directlyActions: ▲Bronchial secretion by salt
action
ii) Guaifenesin Expectorant drug usually taken by
mouth Available as single & also in
combination MOA=Increase the volume & reduce the
viscosity of secretion in trachea & bronchi
Ammonium saltsGastric irritants reflexly bronchial
secretions + sweating

Help in expectoration by liquefy the viscous tracheobronchial secretions
E.g., Bromhexine, Acetyl cysteine,
i) BromhexineSynthetic derivative of vasicine (alkaloid=
Adhatoda vasica)Cont….

MOA of Bromhexinea) Thinning & fragmentation of
mucopolysaccaride fibersb) ↑ volume & ↓ viscosity of sputum
ii) AcetylcysteineGiven directly into respiratory tract
cont.

Opens disulfide bond in mucoproteins of sputum =↓ viscosity
UsesCystic fibrosis (to viscosity of sputum)Onset of action quick---used 2-8 hourlyAdverse effectsNausea, vomiting, bronchospasm in
bronchial asthma
Added to antitussives/expectorant formulation Due to sedative ا& anticholinergic actions
produce relief in cough but lack selectivity for cough centre
No expectorant action =▼secretions (anticholinergic effect)
Suitable for allergic cough (not for asthma)
E.g., Chlorpheniramine, diphenhydramine, promethazine
Bronchospasm or stimulation of pulmonary receptors = induce or aggravate ادهQزي cough + bronchoconstriction
e.g. β2-agonist (salbutamol, terbutaline)
MOA of bronchodilators in cough ▲surface velocity of air flow during cough→
Clear secretions of airway Not used routinely for every type of coughمهمه
but only when bronchoconstriction is present
Soother the throat (directly & also by promoting salivation)
▼ afferent impulses from inflamed/irritated pharyngeal mucosa
Provide symptomatic relief in dry cough arising from throat
E.g. lozenges, cough drops, glycerine, liquorice, honey
Etiology of cough Treatment
1) Upper/lower respiratory Appropriate antibiotics tract infections
2) Smoking/chronic bronchitis Cessation of smoking
3) Pulmonary tuberculosis Antibiotics
4) Asthmatic cough Inhaled β2-agonists/iprat-
ropium/corticosteroid
5) Postnasal drip (sinusitis) Antibiotics, nasal decon-
gestants, antihistamines

THANK YOU

















