“PRF is easy to handle and modify, providing the defect with not only a matrix permitting cell
migration into the surgical site but also with crucial biological cues potentially accelerating the
wound healing process.” (Ghanaati et al 2014)
L-PRF: Simple Preparation
•
•
24 gauge butterfly
needle
plastic tube coated internally with silica particles
2700 RPM (400g) 12 minutes
RBCs
Fibrin Clot (PRF)
Acellular Plasma (PPP)
Intra-Lock.com
L-PRF:Preparation (cont)
•
•
•WBC
and PLT
Fibrinclot
RBC
Li et al 2013
PRF ‘s naturally polymerized fibrin network sustains a slow release of growth factors and matrix glycoproteins for 7 - 14 days (Ling 2009; Dohan-Ehrenfest et al 2009; He et al 2009; Wu et al 2012; Kawase et al 2015)
FRAGMENTSMEMBRANES PLUGS GF-ENRICHED BONE GRAFT MATRIX(PRF-BLOCK®)
Standard 12 Minute Protocol Modified 3 Min Protocol
PRF BLOCK
We graft sockets to offset the post-extraction catabolic process and minimize alveolar ridge degradation
•
•
•
The positive effect of growth factors in L-PRF could be particularly relevant when combined with osteoconductivescaffolds with slow healing dynamics (Torres et al 2009; Anitua et al 2010), where bone metabolism is compromised (eg. osteoporosis) as well as in early implantation scenarios (Chen et al 2004).
My “Socket Cocktail”
CaSO4, PRF, D/M/FDB
PRF has shown promising results in the early phases of extraction socket healing
•
•
•
•
Flapless Extractions
• Socket grafted to a level 2 to 3 mm below free gingival margin
PRF provides an organized matrix at the start of healing, increasing the speed of vascular ingress and wound coverage (Dohan et al 2006)
Flapless Extractions
1 wk 4 wks
•1 or 2 PRF plugs placed in socket and secured with mattress and interrupted sutures
In Sites With Severe Bone Loss, Ridge Augmentation Is Usually Performed 6-8 Weeks After Tooth Removal
This Delayed Approach Provides Additional Soft-tissue Coverage Over The Augmented Site
1 WEEK
Maintenance of primary closure is essential to maximize bone gain
8 WEEKS after ext’s
L-PRF over Frenectomy and in Socket
8 wks
Ridge augmentation done simultaneously with ext #9 would require a larger flap with extensive
release, increasing postop pain and swelling as well as the risk of wound dehiscence.
Autogenous bone goes
here
PRE-OP
Toffler M. Guided Bone Regeneration (GBR) Using Cortical Bone Pins in Combination with Leukocyte- and Platelet-Rich Fibrin (L-PRF). Compend Cont Ed Dent 2014;35(3).
Salvin Dental
Cortical Bone Pins: Clinical Advantages
•No screws to retrieve
•Membrane support
•Graft retention
2 mm twist adjustable stop (hhco-store.com)
10-day post-op
Comparative healing at 6 months
• 6 months post-op • Pre-op
Stage-2 Final
Dr Michael Woloch
PRF BLOCK®
PREOP6 MOS
Consistent Use of L-PRF in Sinus Elevation Surgery for the Last 10 Years
• Slow sustained release of key growth factors (Ling 2009; Dohan-Ehrenfest et al 2009; He et al 2009; Wu et al 2012; Lauritano et al 2013; Kawase et al 2015)
• Expedited sinus graft healing (Choukroun et al 2006; Inchingolo et al 2010; Tatullo et al 2012; Cruzat et al 2015)
• Maintenance of primary wound closure (Khiste & Tare 2013; Baiju et al 2013; Toffler et al 2014)
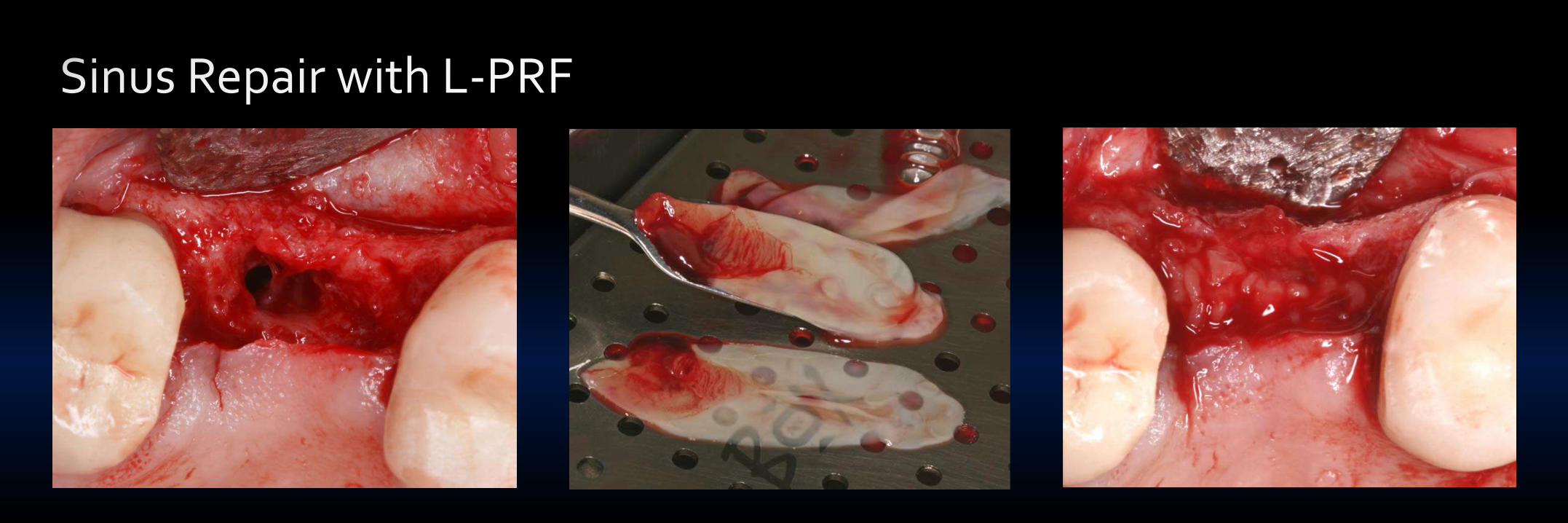
• Membrane protection (Diss et al 2008; Toffler et al 2010) and repair (Choi et al 2006; Shin & Sohn 2005; Baykul & Findik 2014; Toffler & Rosen 2015)
All My Approaches to Sinus Floor Elevation Incorporate L-PRF
Transcrestal/Simultaneous LWOTranscrestal/Staged
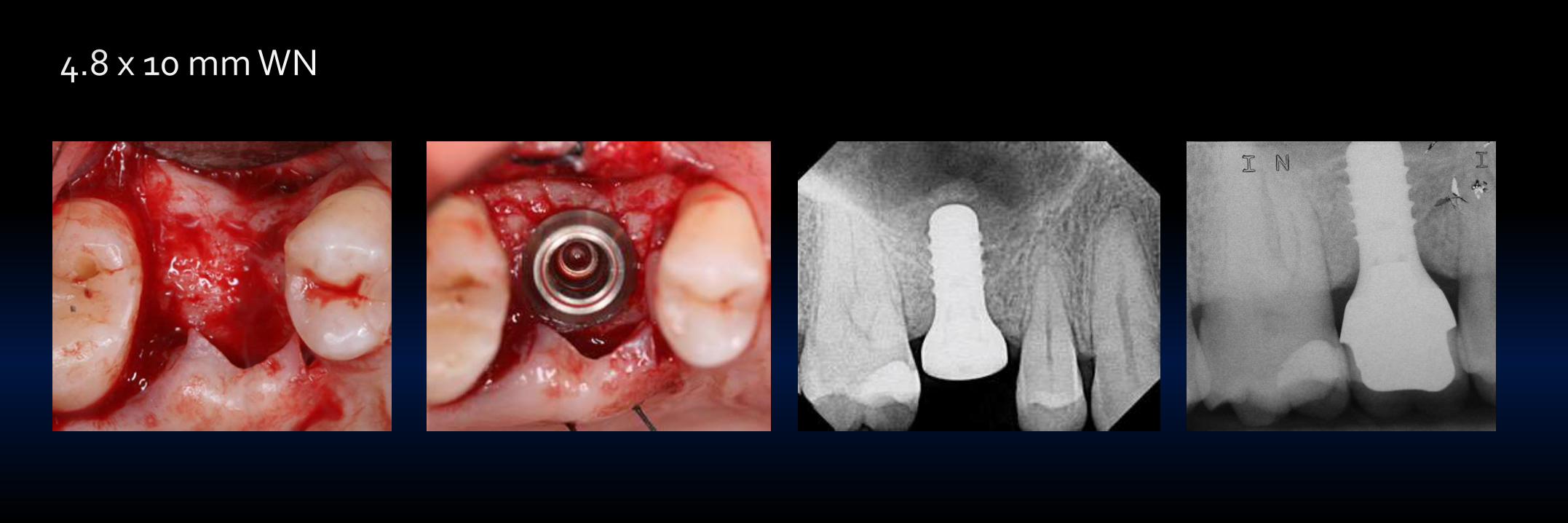
10 mm long implants
“I use a transcrestal approach as often as I can, but prefer using a lateral (visual) approach not only in severely atrophic sites but also in………….
…….patients with ≤ 4 mm of subantral bone and significant sinus pathology.”
Optical and Instrumental Access to Optimize Healing Response
……and for extra added
safety, platelet-rich fibrin
(PRF) lines the sinus
membrane prior to grafting
Single Stage Placement 6 Months Later
10 mm
4.0 x 11 mm Implant PREOP
5 mm core prepped to a depth 3 mm
Subantral bone
height is now
doubled (7- 8 mm)
PRF in TSFE and Simultaneous Implant Placement
PRF will be added immediatedly after accessing sinus via direct infracture , drilling or piezosurgery
Direct Infracture Drilling/Controlled Erosion Piezosurgery
Sohn2010
2.8 mm tip to elevateWiden osteotomy
to 4.1 mm
PRF
PREOP
Bone Densification and Placement 5 x 11 mm Thommen Implant
PRF in Membrane Repair
Perforation Transcrestal Approach
PRF
Perforation Transcrestal Approach
4 mos
CBCT 3 years
At 4 months, full repair and 6.7 mm RSBH
6.73
6.73
3-4 mm of TSFE
4 years
64 y/ F, heavy smokerImplants placed 10 years ago, referred for tx peri-implant diseaseSevere sinusitis, failure of implants 13 (floor intact), 14 (OAC)
I hope I have demonstrated the potential benefits of incorporating PRF into:
Extraction Sites• Serves as a matrix to accelerate the healing of wound edges much like a fibrin bandage
7 days
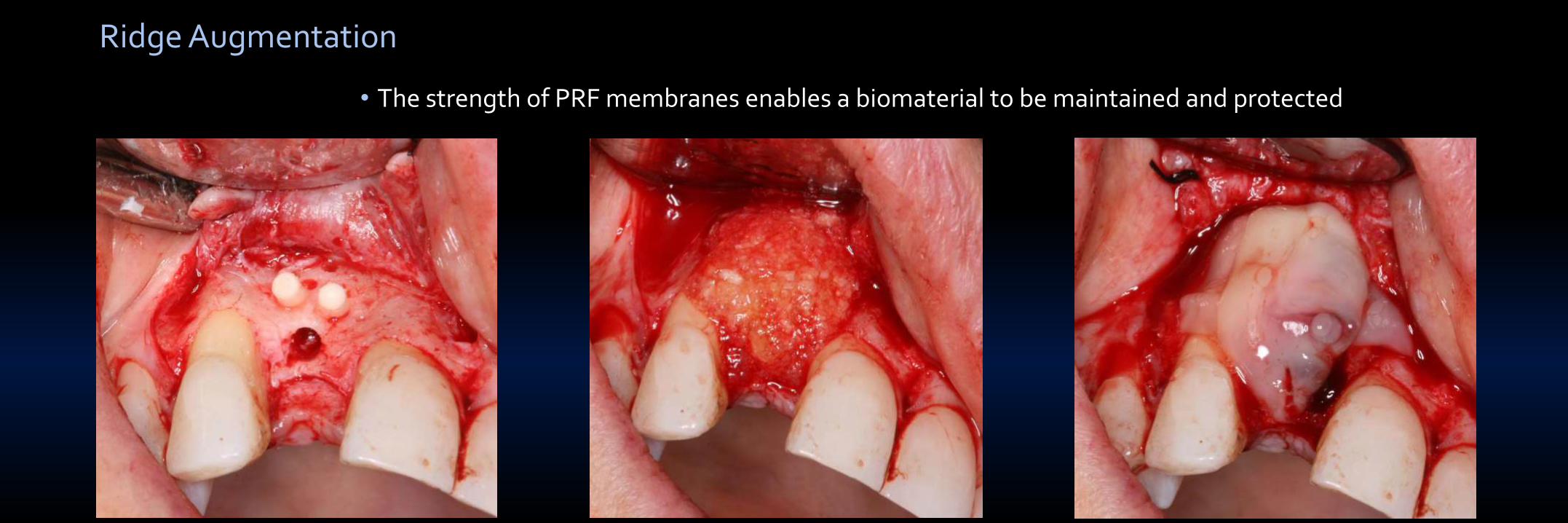
Ridge Augmentation
• Aids in hemostasis
• Provides a high quality of gingival maturation (Simonpieri et al 2009)
1 week
• The strength of PRF membranes enables a biomaterial to be maintained and protected
Ridge Augmentation
Composite Grafts
• PRF fragments serve as a biological connector between bone particles facilitating cellular migration, particularly for endothelial cells necessary for neo-angiogenesis (Simonpieri et al 2009; Kobayashi 2011)
Complex Reconstructive Surgery
• Platelet cytokines are gradually released as the fibrin matrix is resorbed, thus creating a perpetual process of healing
PRF is a welcomed addition for all my SFE procedures, but it is especially helpful in high risk membrane perf/sinus communication cases!
FAILED LWO SINGLE TOOTH SITESOAF EXT/OAC SINUS SEPTA




























































































](https://static.documents.pub/doc/80x56/545eed83af795935708b4b26/ilya-prigogine-isabelle-stengers-alvin-tofflerbook4meorg.jpg)






