52
Cross Roads Dr. Raed Al-Bukhari, FACP Consultant Rheumatologest King Fahd Hospital of the University University of Dammam
| Date post: | 14-Dec-2015 |
| Category: |
Documents |
| Upload: | mustafa-maddison |
| View: | 214 times |
| Download: | 0 times |

Cross RoadsDr. Raed Al-Bukhari, FACPConsultant RheumatologestKing Fahd Hospital of the UniversityUniversity of Dammam
• Musculoskeletal complaints resulting from endocrinological diseases are common and well described.
• Every disease has its own rheumatic symptoms and signs.
• Very high prevalence rate of diabetes mellitus in our society, frequent thyroid diseases and steroid effect on adrenal function.
• Rheumatologist, internist, primary care physician and general practitioner should be well informed about endocrinological diseases effect on muscles, tendons, ligaments and joints.
• Over view and recent data on three common areas.

Diabetes Mellitus
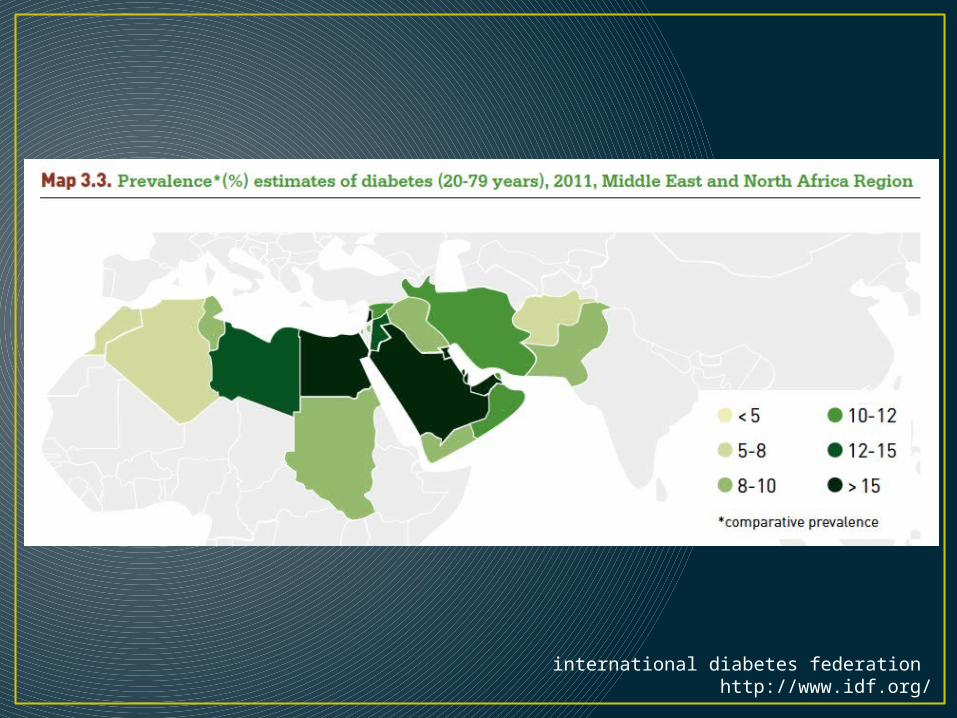
international diabetes federation http://www.idf.org/

Middle East and North Africa
• More than 34.2 million people in the MENA Region have diabetes; by 2030 this will rise to 59.7 million.
• Globally number of people with diabetes 371 million.
• Diabetes caused 356,586 deaths in the MENA Region 2012.
• 12 billion USD were spent on treating diabetes in the region.
• The region has the highest prevalence of diabetes in adults (11%) (overall).
international diabetes federation http://www.idf.org/

Diabetes in Saudi Arabia • From top of the world at a glance in 2012 • Prevalence 19.42%• Total adult population 17,582,020• Number of adults with diabetes 3,414,510• Number of adults with undiagnosed diabetes
241,710• Number of deaths due to diabetes 20,933. • Mean healthcare expenditures per person with
diabetes (USD) 953.71
international diabetes federation http://www.idf.org/

Musculoskeletal Manifestations

• Limited Joint Mobility (Diabetic Cheiroarthropathy).
• Skin changes of LJM begin around the MCP and PIP joints of the little finger and progress medially to involve other digits and distally to involve the DIP joints.
• LJM usually is painless.• Flexion contractures involving several
fingers and thickened, tight, and waxy skin.
• Physical examination, inability to oppose the palmar surfaces of the hands and fingers with the wrists dorsiflexion.
• Prayer SignRheumatic manifestations of diabetes mellitus. Rheumatic diseases clinics of
North America. 2010;36:681-699.
• The prevalence of LJM ranges between 30% and 58% among patients with type 1 DM and between 45% and 76% among those with type 2 DM, as compared with between only 4% and 20% among individuals without DM.
• Stenosing Flexor Tenosynovitis, 5% and 36% among patients with type 1 and 2 DM, as compared with 2% in the general population.
• Dupuytren’s contracture, most often involves the middle and ring fingers rather than the ring and little fingers, as in nondiabetics, prevalece between 16% and 42%

Clinical appearance of Dupuytren's disease. A, Patient showing a cord from the radial longitudinal oriented fibers of the palmar aponeurosis of the thumb. This image also shows a cord arising from the distal transverse commissural ligament of the first web space. B, A 73-year-old man who presented with DD of the ring finger worsening over 10 years. C, A 45-year-old patient who presented with new DD of the right middle finger and recurrence of DD of the little finger following surgery 4 years earlier.
Dupuytren's DiseaseThoma, Achilleas, PLASTIC SURGERY: INDICATIONS AND PRACTICE, CHAPTER 90, 1173-1179Copyright © 2009 © 2009, Elsevier Inc. All rights reserved.
• Recently, injecting the thickened palmar fascia with collagenase from Clostridium histolyticum has been developed as a nonsurgical treatment approach.
• Adhesive capsulitis of the shoulder, prevalence ranges from 10% to 29% and is about 5-fold that in the general population.
• Associated with the presence of autonomic neuropathy among individuals with either type of DM and with myocardial infarction among those with type 1 DM.
• Compared to nondiabetics its associated with an inferior outcome with more pain, restricted range of motion and poorer function.

• Carpal tunnel syndrome, described bilaterally, DM is a risk factor for CTS (large case-control study of 3391 patients).
• Impaired median nerve recovery observed after carpal tunnel release among some patients with DM suggests that intrinsic nerve pathology might contribute to its pathogenesis in DM.
• Diabetic muscle infarction, systematic review identified 116 patients, mean age at presentation was 43, the average duration of DM 14 years, and vascular complications of DM present in the majority, particularly nephropathy 71%, retinopathy 57% and neuropathy 55%.
• DISH.
Diabetic muscle infarction: an underdiagnosed complication of long-standing diabetes. Diabetes care. 2003;26:211-215.

Anteroposterior ( A ) and lateral ( B ) views of the thoracic spine in patient with DISH. Flowing ossification is noted anteriorly and on the right side of the spine. At least seven contiguous vertebral bodies are involved. The disc spaces are preserved. Radiolucency extends from the disc space into the ossification, creating a Y-shaped lucency and a bumpy bony excrescence at the disc level.
Brower, Anne C., MD, Arthritis in Black and White, 15, 275-292Copyright © 2012 Copyright © 2012, 1997, 1988 by Saunders, an imprint of Elsevier Inc.

Lateral view of the foot in patient with DISH. All joint spaces are preserved. Ossification is seen at the attachment of the plantar aponeurosis and the Achilles tendon. There is also ossification on the dorsal aspect of the navicular and the cuneiform, the base of the fifth metatarsal, and the distal tibia ( arrows ).
Diffuse Idiopathic Skeletal HyperostosisBrower, Anne C., MD, Arthritis in Black and White, 15, 275-292Copyright © 2012 Copyright © 2012, 1997, 1988 by Saunders, an imprint of Elsevier Inc.
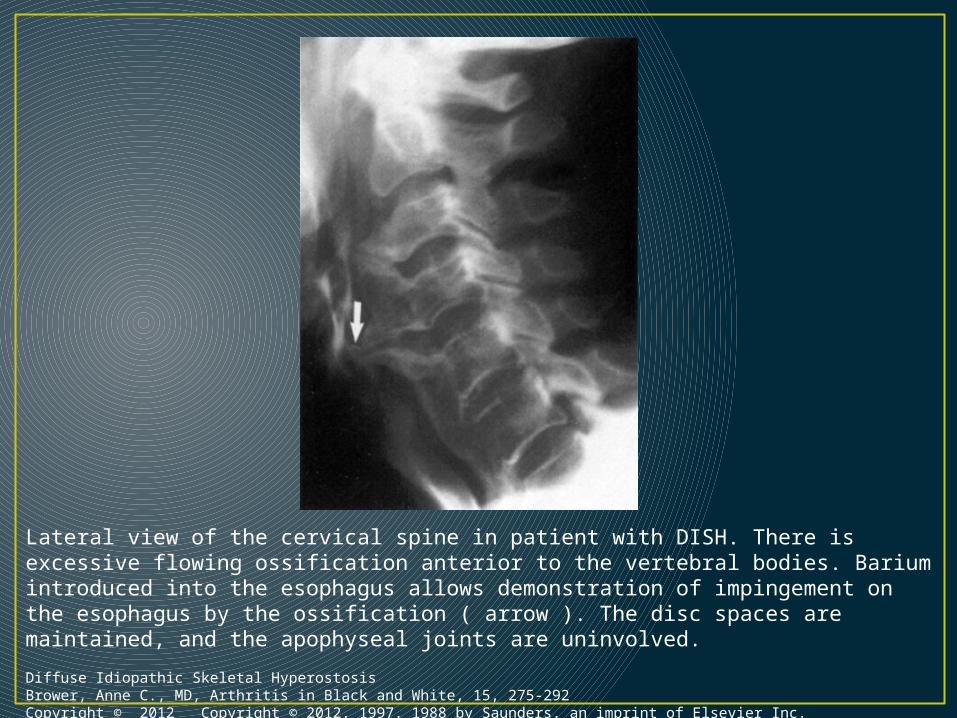
Lateral view of the cervical spine in patient with DISH. There is excessive flowing ossification anterior to the vertebral bodies. Barium introduced into the esophagus allows demonstration of impingement on the esophagus by the ossification ( arrow ). The disc spaces are maintained, and the apophyseal joints are uninvolved.
Diffuse Idiopathic Skeletal HyperostosisBrower, Anne C., MD, Arthritis in Black and White, 15, 275-292Copyright © 2012 Copyright © 2012, 1997, 1988 by Saunders, an imprint of Elsevier Inc.

• Characterized by an inflammatory process resulting in dislocation of the neuropathic joint, fracture and resorption of affected bones. Most commonly associated with DM.
• Prevalence 0.15%, most commonly true ankle, tarsometatarsal, metatarsophalangeal.
• Early immobilization is important to prevent progression hence imaging studies should be obtained early in the course of illness even with little pain.
• Early MRI show marrow edema or microfractures.• Bisphosphonates did not shorten the immobilization
time, no data were available regarding long term effects on deformities and ulcerations.
Treatment of acute Charcot foot with bisphosphonates: a systematic review of the literature. Diabetologia. 2012;55:1258-1264.
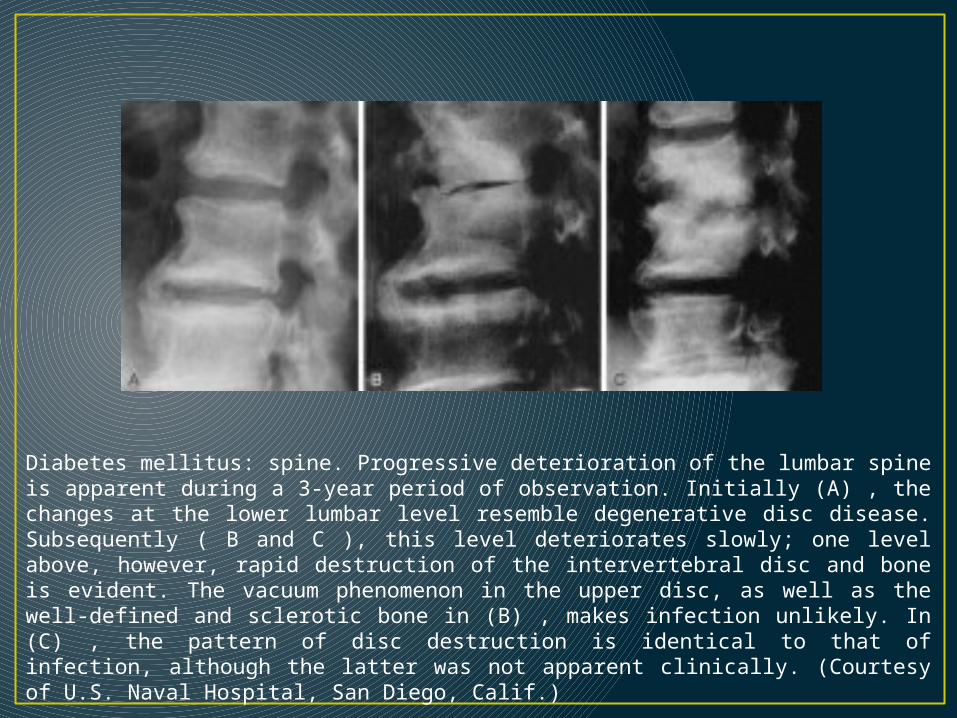
Diabetes mellitus: spine. Progressive deterioration of the lumbar spine is apparent during a 3-year period of observation. Initially (A) , the changes at the lower lumbar level resemble degenerative disc disease. Subsequently ( B and C ), this level deteriorates slowly; one level above, however, rapid destruction of the intervertebral disc and bone is evident. The vacuum phenomenon in the upper disc, as well as the well-defined and sclerotic bone in (B) , makes infection unlikely. In (C) , the pattern of disc destruction is identical to that of infection, although the latter was not apparent clinically. (Courtesy of U.S. Naval Hospital, San Diego, Calif.)
Neuropathic Osteoarthropathy, Resnick, Donald, MD, Bone and Joint Imaging, CHAPTER 66, 1056-1066Copyright © 2005 Copyright © 2005, 1996, 1989 by Elsevier Inc.
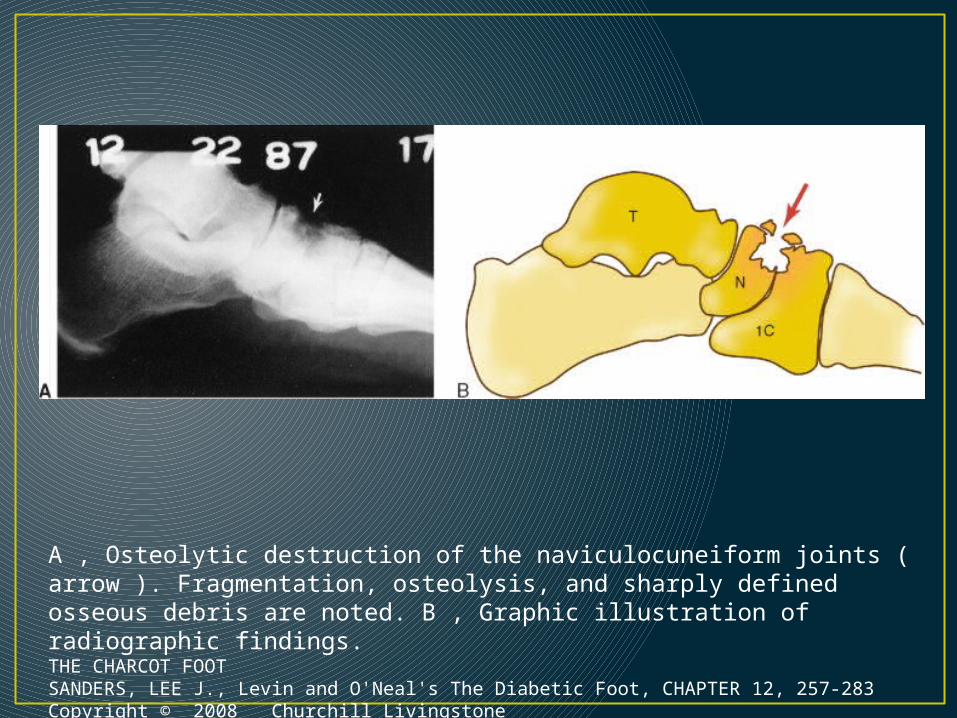
A , Osteolytic destruction of the naviculocuneiform joints ( arrow ). Fragmentation, osteolysis, and sharply defined osseous debris are noted. B , Graphic illustration of radiographic findings. THE CHARCOT FOOTSANDERS, LEE J., Levin and O'Neal's The Diabetic Foot, CHAPTER 12, 257-283Copyright © 2008 Churchill Livingstone
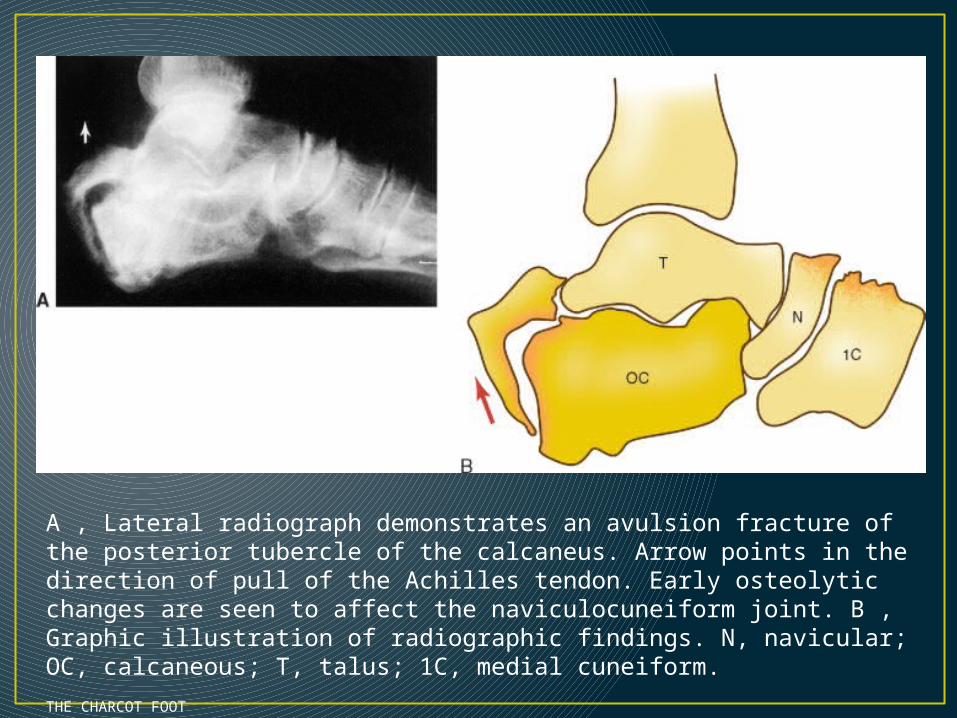
A , Lateral radiograph demonstrates an avulsion fracture of the posterior tubercle of the calcaneus. Arrow points in the direction of pull of the Achilles tendon. Early osteolytic changes are seen to affect the naviculocuneiform joint. B , Graphic illustration of radiographic findings. N, navicular; OC, calcaneous; T, talus; 1C, medial cuneiform.
THE CHARCOT FOOTSANDERS, LEE J., Levin and O'Neal's The Diabetic Foot, CHAPTER 12, 257-283Copyright © 2008 Churchill Livingstone

Musculoskeletal manifestations in diabetic patients at a tertiary center. Libyan journal of medicine. 2012;7:1-7.
Prevalence of musculoskeletal disorders among studied diabetic patients"MSK manifestations Number %Overall prevalence 45 17.8Carpal tunnel syndrome 17 6.7Shoulder adhesive capsulitis 17 6.7Diabetic amyotrophy 12 4.8Flexor tenosynovitis 11 4.4Diabetic cheiroarthropathy 8 3.2Crystal arthropathy 7 2.7Diabetic sclerodactyly 5 2Plantar fasciitis 3 1.2Dupuytren's disease 1 0.4Muscle infarction 1 0.4Charcot joint 1 0.4Diffuse idiopathic skeletal hyperosteosis 1 0.4De Quervain's tenosynovitis 1 0.4Osteomyelitis 1 0.4Diabetic osteolysis 0 0Reflex sympathetic dystrophy 0 0Septic arthritis 0 0
King Abdulaziz University Hospital,Jeddah, Saudi Arabia
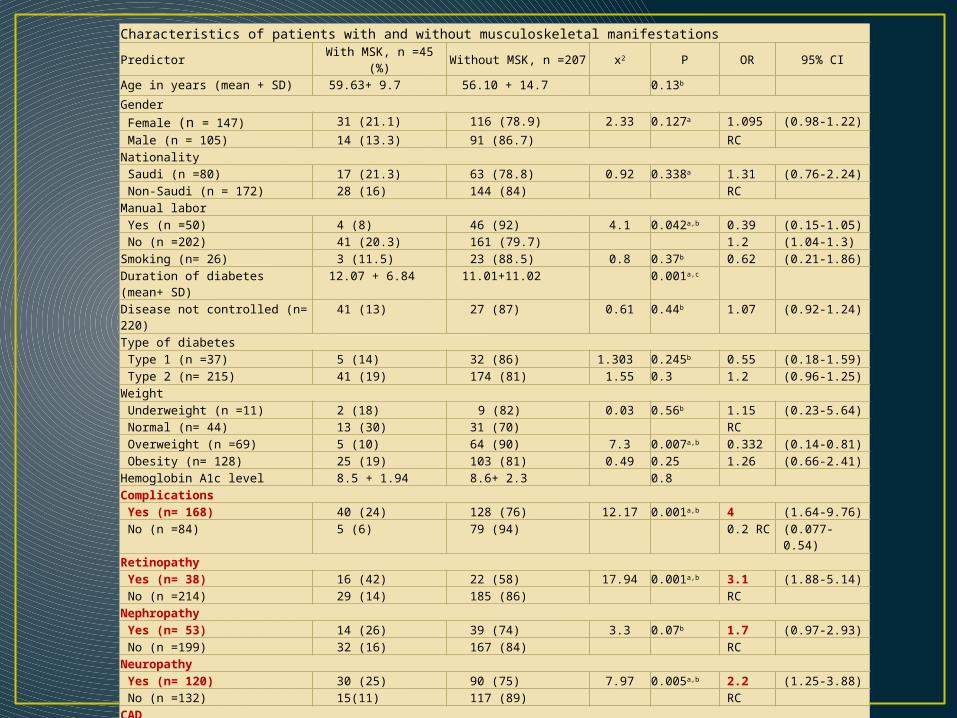
Characteristics of patients with and without musculoskeletal manifestationsPredictor With MSK, n =45 (%) Without MSK, n =207 x2 P OR 95% CIAge in years (mean + SD) 59.63+ 9.7 56.10 + 14.7 0.13b GenderFemale (n = 147) 31 (21.1) 116 (78.9) 2.33 0.127a 1.095 (0.98-1.22)Male (n = 105) 14 (13.3) 91 (86.7) RC
NationalitySaudi (n =80) 17 (21.3) 63 (78.8) 0.92 0.338a 1.31 (0.76-2.24)Non-Saudi (n = 172) 28 (16) 144 (84) RC
Manual laborYes (n =50) 4 (8) 46 (92) 4.1 0.042a,b 0.39 (0.15-1.05)No (n =202) 41 (20.3) 161 (79.7) 1.2 (1.04-1.3)
Smoking (n= 26) 3 (11.5) 23 (88.5) 0.8 0.37b 0.62 (0.21-1.86)Duration of diabetes (mean+ SD)
12.07 + 6.84 11.01+11.02 0.001a,c
Disease not controlled (n= 220) 41 (13) 27 (87) 0.61 0.44b 1.07 (0.92-1.24)Type of diabetesType 1 (n =37) 5 (14) 32 (86) 1.303 0.245b 0.55 (0.18-1.59)Type 2 (n= 215) 41 (19) 174 (81) 1.55 0.3 1.2 (0.96-1.25)
WeightUnderweight (n =11) 2 (18) 9 (82) 0.03 0.56b 1.15 (0.23-5.64)Normal (n= 44) 13 (30) 31 (70) RCOverweight (n =69) 5 (10) 64 (90) 7.3 0.007a,b 0.332 (0.14-0.81)Obesity (n= 128) 25 (19) 103 (81) 0.49 0.25 1.26 (0.66-2.41)
Hemoglobin A1c level 8.5 + 1.94 8.6+ 2.3 0.8ComplicationsYes (n= 168) 40 (24) 128 (76) 12.17 0.001a,b 4 (1.64-9.76)No (n =84) 5 (6) 79 (94) 0.2 RC (0.077-0.54)
RetinopathyYes (n= 38) 16 (42) 22 (58) 17.94 0.001a,b 3.1 (1.88-5.14)No (n =214) 29 (14) 185 (86) RC
NephropathyYes (n= 53) 14 (26) 39 (74) 3.3 0.07b 1.7 (0.97-2.93)No (n =199) 32 (16) 167 (84) RC
NeuropathyYes (n= 120) 30 (25) 90 (75) 7.97 0.005a,b 2.2 (1.25-3.88)No (n =132) 15(11) 117 (89) RC
CADYes (n= 75) 21 (28) 54 (72) 7.5 0.006a,b 2.1 (1.23-3.47)No (n =177) 24 (14) 153 (86) RC
CVAYes (n= 21) 6 (29) 19 (71) 1.79 0.181b 1.69 (0.81-3.53)No (n =231) 39 (17) 192 (83) RC

International Diabetes Federation (IDF) definition
• Central obesity (waist circumference ≥ 94cm for Europid men and ≥ 80cm for Europid women) (Arab use Europid)
• + Two of the following four factors:• Raised TG level: ≥ 150 mg/dL or specific treatment for this
lipid abnormality• Reduced HDL cholesterol: < 40 mg/dL in males and < 50
mg/dL in females, or specific treatment for this lipid abnormality
• Raised blood pressure: systolic BP ≥ 130 or diastolic BP ≥ 85 mm Hg, or treatment of previously diagnosed hypertension
• Raised fasting plasma glucose (FPG) ≥ 100 mg/dL or previously diagnosed type 2 diabetes
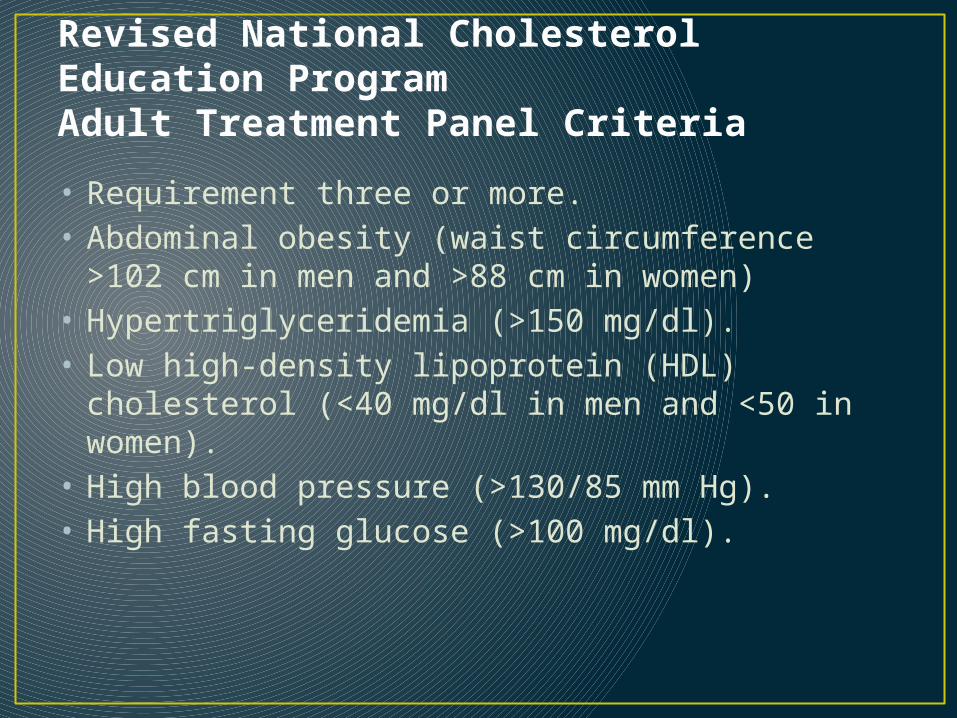
Revised National Cholesterol Education ProgramAdult Treatment Panel Criteria
• Requirement three or more.• Abdominal obesity (waist circumference >102 cm
in men and >88 cm in women)• Hypertriglyceridemia (>150 mg/dl).• Low high-density lipoprotein (HDL) cholesterol
(<40 mg/dl in men and <50 in women).• High blood pressure (>130/85 mm Hg).• High fasting glucose (>100 mg/dl).
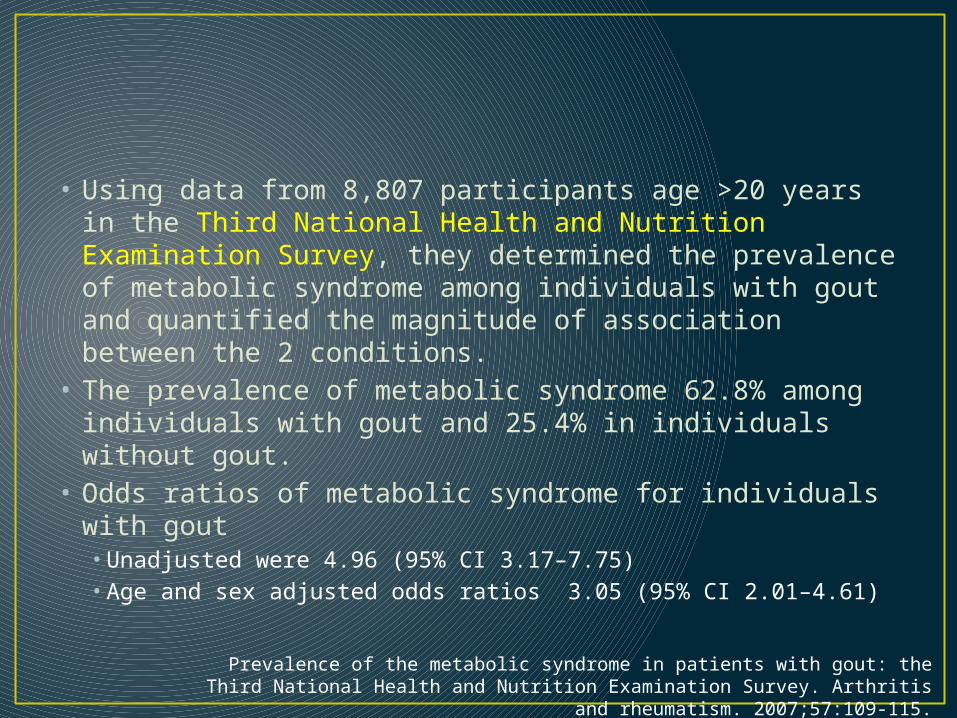
• Using data from 8,807 participants age >20 years in the Third National Health and Nutrition Examination Survey, they determined the prevalence of metabolic syndrome among individuals with gout and quantified the magnitude of association between the 2 conditions.
• The prevalence of metabolic syndrome 62.8% among individuals with gout and 25.4% in individuals without gout.
• Odds ratios of metabolic syndrome for individuals with gout • Unadjusted were 4.96 (95% CI 3.17–7.75)• Age and sex adjusted odds ratios 3.05 (95% CI 2.01–4.61)
Prevalence of the metabolic syndrome in patients with gout: the Third National Health and Nutrition Examination Survey. Arthritis and rheumatism.
2007;57:109-115.

Gout• Case control study 20 male early onset gout
patients, gout family history, without a habit of alcohol consumption or obesity before the first attack of gout, and 42 unrelated males control.
• Gout and Type 2 diabetes shared the common genetic factors.
• Type 2 diabetes was the most significantly associated disease with gout as recognized by 36 gene symbols corresponding to 334 significant SNPs.
Gout and type 2 diabetes have a mutual inter-dependent effect on genetic risk factors and higher incidences. Rheumatology. 2012;51:715.
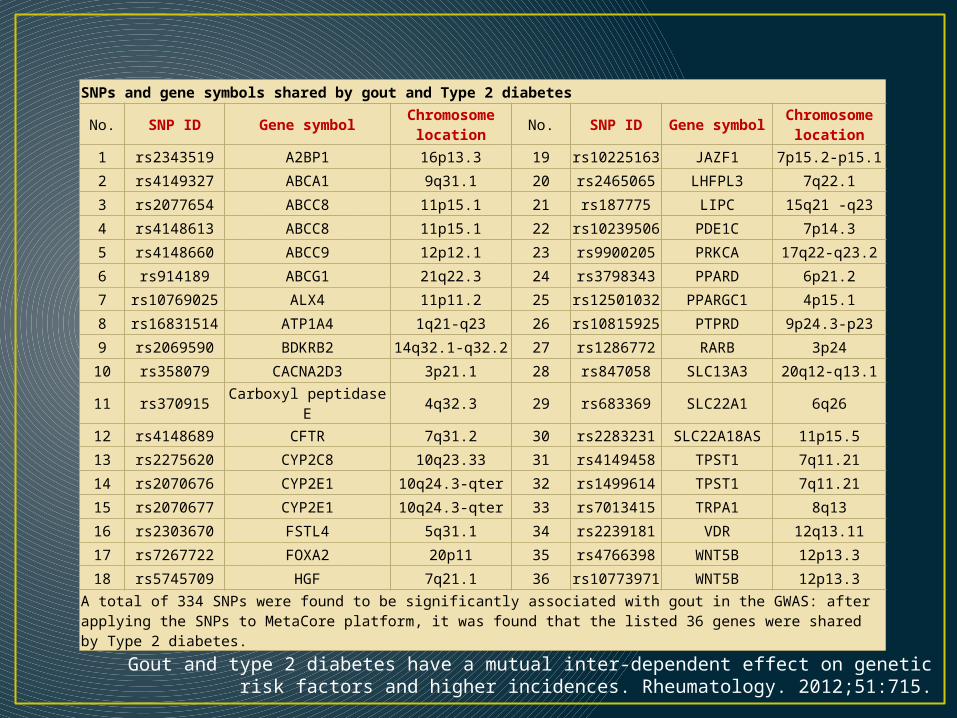
SNPs and gene symbols shared by gout and Type 2 diabetes
No. SNP ID Gene symbolChromosome
locationNo. SNP ID Gene symbol
Chromosome location
1 rs2343519 A2BP1 16p13.3 19rs1022516
3JAZF1 7p15.2-p15.1
2 rs4149327 ABCA1 9q31.1 20 rs2465065 LHFPL3 7q22.1
3 rs2077654 ABCC8 11p15.1 21 rs187775 LIPC 15q21 -q23
4 rs4148613 ABCC8 11p15.1 22rs1023950
6PDE1C 7p14.3
5 rs4148660 ABCC9 12p12.1 23 rs9900205 PRKCA 17q22-q23.2
6 rs914189 ABCG1 21q22.3 24 rs3798343 PPARD 6p21.2
7 rs10769025 ALX4 11p11.2 25rs1250103
2PPARGC1 4p15.1
8 rs16831514 ATP1A4 1q21-q23 26rs1081592
5PTPRD 9p24.3-p23
9 rs2069590 BDKRB2 14q32.1-q32.2 27 rs1286772 RARB 3p24
10 rs358079 CACNA2D3 3p21.1 28 rs847058 SLC13A3 20q12-q13.1
11 rs370915 Carboxyl peptidase E 4q32.3 29 rs683369 SLC22A1 6q26
12 rs4148689 CFTR 7q31.2 30 rs2283231 SLC22A18AS 11p15.5
13 rs2275620 CYP2C8 10q23.33 31 rs4149458 TPST1 7q11.21
14 rs2070676 CYP2E1 10q24.3-qter 32 rs1499614 TPST1 7q11.21
15 rs2070677 CYP2E1 10q24.3-qter 33 rs7013415 TRPA1 8q13
16 rs2303670 FSTL4 5q31.1 34 rs2239181 VDR 12q13.11
17 rs7267722 FOXA2 20p11 35 rs4766398 WNT5B 12p13.3
18 rs5745709 HGF 7q21.1 36rs1077397
1WNT5B 12p13.3
A total of 334 SNPs were found to be significantly associated with gout in the GWAS: after applying the SNPs to MetaCore platform, it was found that the listed 36 genes were shared by Type 2 diabetes.
Gout and type 2 diabetes have a mutual inter-dependent effect on genetic risk factors and higher incidences. Rheumatology. 2012;51:715.
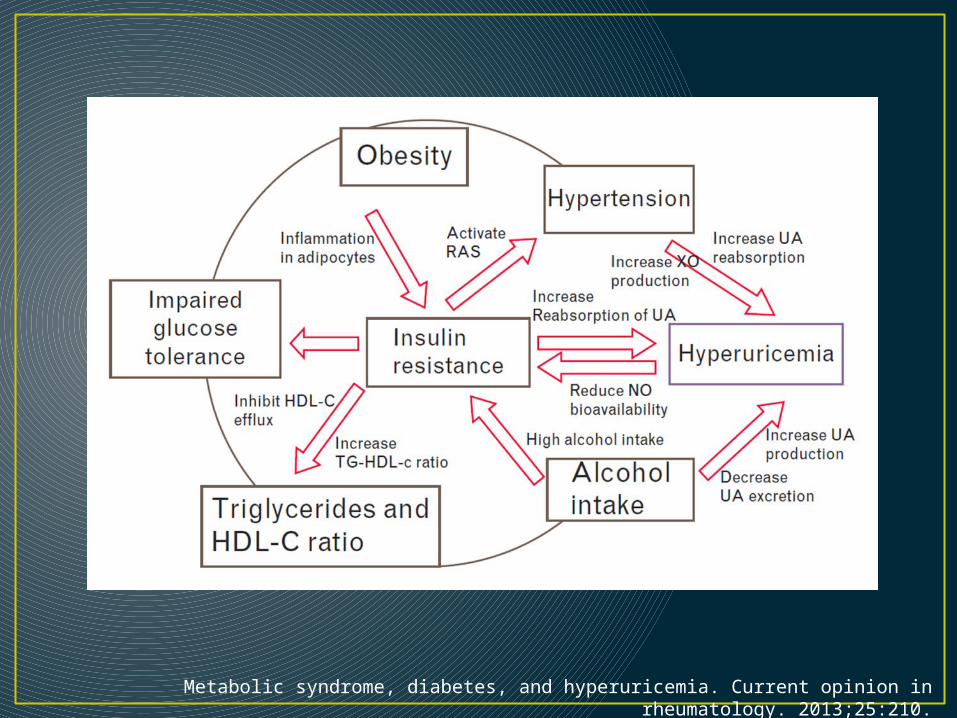
Metabolic syndrome, diabetes, and hyperuricemia. Current opinion in rheumatology. 2013;25:210.
Gout• RR for incident gout among patients with
diabetes, as compared with individuals with no diabetes was 0.67 (95% CI 0.63 to 0.71).
• Case-control all incident cases of gout 24768 and randomly sample from 50000 controls.
• The multivariate analysis of RRs with the duration of diabetes showed inverse relationship.
• Results after adjusting for age, sex, body mass index, general practitioner visits, smoking, alcohol intake, ischaemic heart disease and presence of cardiovascular risk factors.
Impact of diabetes against the future risk of developing gout. Annals of the rheumatic diseases. 2010;69:2090-2094.
Impact of diabetes against the future risk of developing gout. Annals of the rheumatic diseases. 2010;69:2090-2094.
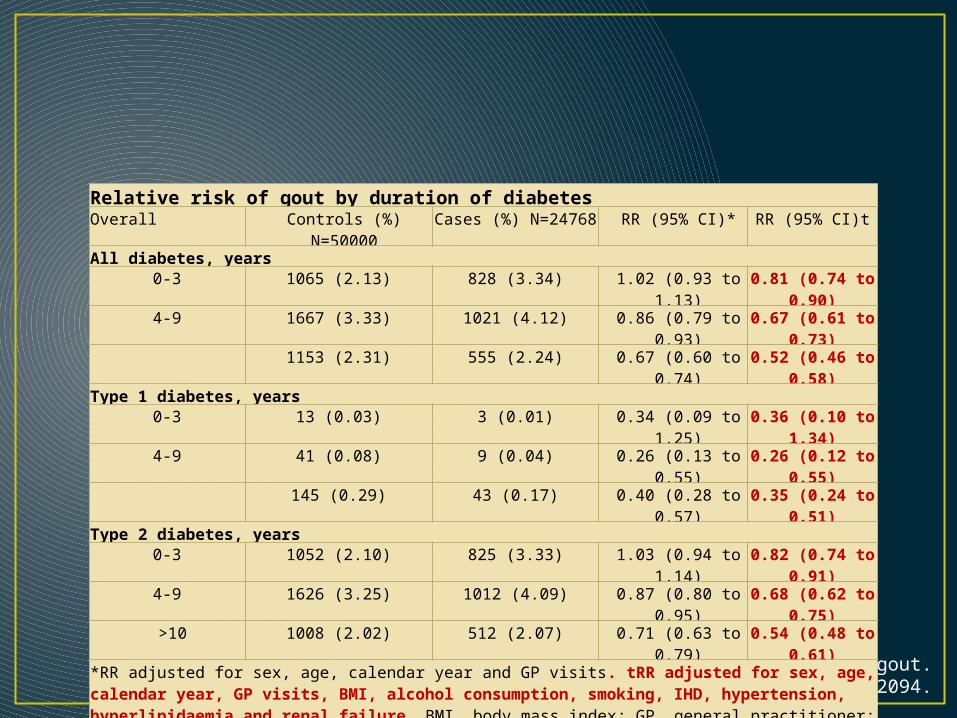
Relative risk of gout by duration of diabetesOverall Controls (%)
N=50000Cases (%) N=24768 RR (95% CI)* RR (95% CI)t
All diabetes, years0-3 1065 (2.13) 828 (3.34) 1.02 (0.93 to
1.13)0.81 (0.74 to
0.90)4-9 1667 (3.33) 1021 (4.12) 0.86 (0.79 to
0.93)0.67 (0.61 to
0.73)1153 (2.31) 555 (2.24) 0.67 (0.60 to
0.74)0.52 (0.46 to
0.58)Type 1 diabetes, years
0-3 13 (0.03) 3 (0.01) 0.34 (0.09 to 1.25)
0.36 (0.10 to 1.34)
4-9 41 (0.08) 9 (0.04) 0.26 (0.13 to 0.55)
0.26 (0.12 to 0.55)
145 (0.29) 43 (0.17) 0.40 (0.28 to 0.57)
0.35 (0.24 to 0.51)
Type 2 diabetes, years0-3 1052 (2.10) 825 (3.33) 1.03 (0.94 to
1.14)0.82 (0.74 to
0.91)4-9 1626 (3.25) 1012 (4.09) 0.87 (0.80 to
0.95)0.68 (0.62 to
0.75)>10 1008 (2.02) 512 (2.07) 0.71 (0.63 to
0.79)0.54 (0.48 to
0.61)*RR adjusted for sex, age, calendar year and GP visits. tRR adjusted for sex, age, calendar year, GP visits, BMI, alcohol consumption, smoking, IHD, hypertension, hyperlipidaemia and renal failure. BMI, body mass index; GP, general practitioner; IHD, ischaemic heart disease.

0-3 9-Apr >100
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
All diabetes, years
Type 1 dia-betes, years
Type 2 dia-betes, years
• Relative risk of gout by duration of diabetes adjusted for sex, age, calendar year, GP visits, BMI, alcohol consumption, smoking, IHD, hypertension, hyperlipidaemia and renal failure
Impact of diabetes against the future risk of developing gout. Annals of the rheumatic diseases. 2010;69:2090-2094.

Thyroid Gland
• Autoimmune thyroid disease (AITD) denotes a spectrum of immunological disorders of the thyroid gland that includes • Graves’ disease • Chronic lymphocytic thyroiditis (Hashimoto disease)
• Manifested as thyrotoxicosis, hypothyroidism and thyroid nodule or neck swelling.
• Anti-thyroid peroxidase (anti-TPO) antibodies are expressed in 90-95%, and anti-thyroglobulin (anti-TG) antibodies in about 20-50%, of patients with CLT.
• A minority of patients express thyrotropin receptor antibodies (blocking antibodies that contribute to hypothyroidism).
Hypothyroidism
Symptoms and Signs• Generalized stiffness. • Symmetrical arthropathy with stiffness of the
small joints of the hands (MCP, PIP, MTP) and knees joints without the presence of inflammatory synovitis.
• On palpation the joints feel ‘gelatinous’ and fluid is usually noninflammatory, chondrocalcinosis, and CPPD crystals disease can be seen.
• There is a significant association between the number of joints affected and anti-Thyroid peroxidase, erythrocyte sedimentation rate, and TSH levels.
Rheumatic manifestations of autoimmune thyroid disease: the other autoimmune disease. The Journal of rheumatology. 2012;39:1125-1129
Symptoms and Signs• Shoulder adhesive capsulitis. • Neck pain.• Carpal tunnel syndrome can be the 1st
manifestation of hypothyroidism, present in more than 7% of patients.
• Hypothyroidism symptom tends to overlap that of fibromyalgia symptoms.
• A myopathy has been reported presenting with proximal weakness and fatigue. Physical examination findings may include muscle hypertrophy, proximal muscle weakness, and delayed relaxation of deep tendon reflexes.
Rheumatic manifestations of autoimmune thyroid disease: the other autoimmune disease. The Journal of rheumatology. 2012;39:1125-1129

• Serum muscle enzyme levels are frequently elevated in patients with hypothyroid myopathy and are elevated in up to 90% of asymptomatic patients.
• These enzymes include CK, myoglobin, and lactate dehydrogenase.
• The increase is typically mild (CK<1000 IU/L).• Reports of a polymyositis like illness or
rhabdomyolysis with dramatic elevations in CK levels do exist in the literature
Musculoskeletal manifestations of thyroid disease. Rheumatic diseases clinics of North America. 2010;36:637-646.

Hyperthyroidism

Symptoms and Signs• The myxedma may appear as nodules varying in
size from 1 cm to large lesions covering most of the pretibial surface and colored from pink to a light purple hue. They can appear and as erythema nodosum, painless and due hyaluronic acid.
• Nail changes, onycholysis and clubbing (thyroid acropachy) may be associated with periostitis around the metacarpal joints as well as soft tissue swelling of the digits.

Symptoms and Signs• Proximal muscle weakness loss of muscle mass
and weight loss.• In contrast with hypothyroidism, serum CK levels
are typically normal and myopathic findings on EMG were rare (10% of patients). Symptoms of weakness resolve with a mean 3.6 months of therapy for hyperthyroidism.
• Shoulder adhesive capsulitis.• Decline in bone mineral density (BMD).• Serum calcium levels are increased due to
increased bone resorption.
Musculoskeletal manifestations of thyroid disease. Rheumatic diseases clinics of North America. 2010;36:637-637.
AITD &Other Diseases Associations

• Autoimmune thyroid diseases associated with well defined systemic autoimmune diseases, MCTD, Sjogren’s syndrome, SLE, RA, systemic sclerosis, and polymyositis/dermatomyositis.
• Risk of quantification study of autoimmune diseases in cohort of more than 3000 UK subjects and their parents with AITD.
• Provide novel information about disease clustering, and the presence of true disease associations.
• These risks highlight the importance of screening for other autoimmune diagnoses.
Prevalence and relative risk of other autoimmune diseases in subjects with autoimmune thyroid disease. The American journal of medicine. 2010;123:183.e1-
183.e9.
Prevalence and relative risk of other autoimmune diseases in subjects with autoimmune thyroid disease. The American journal of medicine. 2010;123:183.e1-
183.e9.
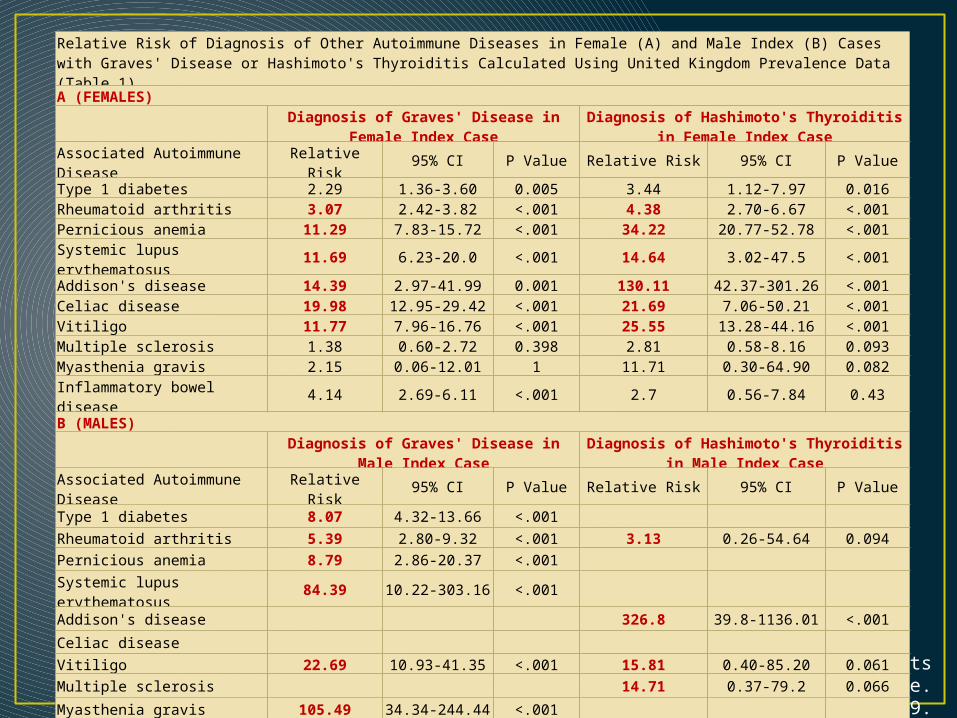
Relative Risk of Diagnosis of Other Autoimmune Diseases in Female (A) and Male Index (B) Cases with Graves' Disease or Hashimoto's Thyroiditis Calculated Using United Kingdom Prevalence Data (Table 1)A (FEMALES)
Diagnosis of Graves' Disease in Female Index Case
Diagnosis of Hashimoto's Thyroiditis in Female Index Case
Associated Autoimmune Disease
Relative Risk 95% CI P Value Relative Risk 95% CI P Value
Type 1 diabetes 2.29 1.36-3.60 0.005 3.44 1.12-7.97 0.016Rheumatoid arthritis 3.07 2.42-3.82 <.001 4.38 2.70-6.67 <.001Pernicious anemia 11.29 7.83-15.72 <.001 34.22 20.77-52.78 <.001Systemic lupus erythematosus
11.69 6.23-20.0 <.001 14.64 3.02-47.5 <.001
Addison's disease 14.39 2.97-41.99 0.001 130.11 42.37-301.26 <.001Celiac disease 19.98 12.95-29.42 <.001 21.69 7.06-50.21 <.001Vitiligo 11.77 7.96-16.76 <.001 25.55 13.28-44.16 <.001Multiple sclerosis 1.38 0.60-2.72 0.398 2.81 0.58-8.16 0.093Myasthenia gravis 2.15 0.06-12.01 1 11.71 0.30-64.90 0.082Inflammatory bowel disease 4.14 2.69-6.11 <.001 2.7 0.56-7.84 0.43B (MALES)
Diagnosis of Graves' Disease in Male Index Case
Diagnosis of Hashimoto's Thyroiditis in Male Index Case
Associated Autoimmune Disease
Relative Risk 95% CI P Value Relative Risk 95% CI P Value
Type 1 diabetes 8.07 4.32-13.66 <.001 Rheumatoid arthritis 5.39 2.80-9.32 <.001 3.13 0.26-54.64 0.094
Pernicious anemia 8.79 2.86-20.37 <.001 Systemic lupus erythematosus
84.39 10.22-303.16 <.001
Addison's disease 326.8 39.8-1136.01 <.001
Celiac disease Vitiligo 22.69 10.93-41.35 <.001 15.81 0.40-85.20 0.061
Multiple sclerosis 14.71 0.37-79.2 0.066
Myasthenia gravis 105.49 34.34-244.44 <.001 Inflammatory bowel disease 1.62 0.20-5.83 0.64 5.66 0.14-30.48 0.162

Other Disease with AITD
• Autoimmune diseases can be associated with increased prevalence's of thyroid autoimmunity include • Type 1 diabetes• Vitiligo• Addison’s disease• Multiple sclerosis
• In general studies have been hampered by small sample sizes and by the use of control populations not matched for age, gender, or geographic location.
• 1517 patients with systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), systemic sclerosis (SSc), mixed connective tissue disease (MCTD), Sjogren's syndrome (SS) and polymyositis/dermatomyositis (PM/DM) were included in the study.
• The HT and GD were diagnosed based on thorough clinical evaluation, imaging and fine-needle aspiration cytology (FNAC).
• 426 patients with autoimmune thyroid disease including 256 GD and 170 HT were also evaluated for the incidence of systemic autoimmune conditions.
Association of systemic and thyroid autoimmune diseases. Clinical rheumatology. 2006;25:240-245

Frequency of thyroid disorders in systemic autoimmune diseases
Hashimoto's thyroiditis (HT)
Graves' disease (GD)
All autoimmune thyroid (HT + GD)
Euthyroid goitre (EG)
All thyroid (HT + GD + EG)
SLE (w = 482) 11 (2.3%) 14 (2.9%) 25 (5.2%) 5 (1.0%) 30 (6.2%)RA (»= 185) 6 (3.2%) 3 (1.6%) 9 (4.9%) 11 (5.9%) 20 (10.8%)SSc (n=119) 5 (4.2%) 4 (3.4%) 9 (7.6%) 5 (4.2%) 14(11.8%)MCTD (w= 159) 34 (21.4%) 4 (2.5%) 38 (23.9%) 4 (2.5%) 42 (26.4%)SS (n = 400) 28 (7.0%) 12 (3.0%) 40 (10.0%) 15 (3.8%) 55 (13.8%)PM/DM (« = 172)
2 (1.2%) 2 (1.2%) 4 (2.3%) 4 (2.3%) 8 (4.7%)
Altogether (n= 1517)
86 (5.7%) 39 (2.6%) 125 (8.2%) 44 (2.9%) 169 (11.1%)
Association of systemic and thyroid autoimmune diseases. Clinical rheumatology. 2006;25:240-245
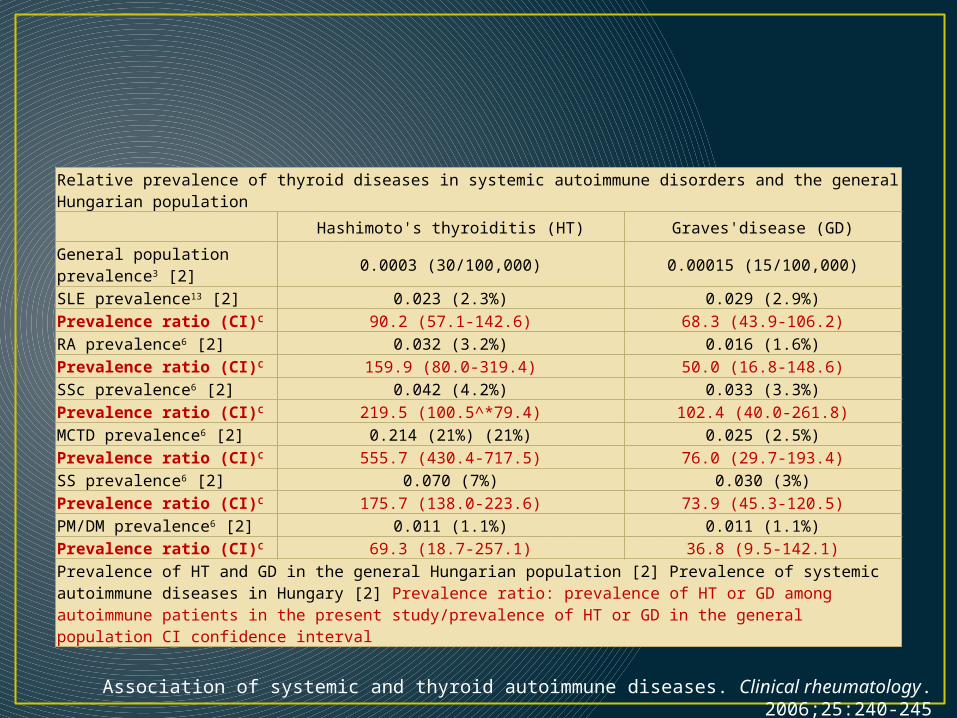
Relative prevalence of thyroid diseases in systemic autoimmune disorders and the general Hungarian population
Hashimoto's thyroiditis (HT) Graves'disease (GD)General population prevalence3 [2]
0.0003 (30/100,000) 0.00015 (15/100,000)
SLE prevalence13 [2] 0.023 (2.3%) 0.029 (2.9%)Prevalence ratio (CI)C 90.2 (57.1-142.6) 68.3 (43.9-106.2)RA prevalence6 [2] 0.032 (3.2%) 0.016 (1.6%)Prevalence ratio (CI)C 159.9 (80.0-319.4) 50.0 (16.8-148.6)SSc prevalence6 [2] 0.042 (4.2%) 0.033 (3.3%)Prevalence ratio (CI)C 219.5 (100.5^*79.4) 102.4 (40.0-261.8)MCTD prevalence6 [2] 0.214 (21%) (21%) 0.025 (2.5%)Prevalence ratio (CI)C 555.7 (430.4-717.5) 76.0 (29.7-193.4)SS prevalence6 [2] 0.070 (7%) 0.030 (3%)Prevalence ratio (CI)C 175.7 (138.0-223.6) 73.9 (45.3-120.5)PM/DM prevalence6 [2] 0.011 (1.1%) 0.011 (1.1%)Prevalence ratio (CI)C 69.3 (18.7-257.1) 36.8 (9.5-142.1)Prevalence of HT and GD in the general Hungarian population [2] Prevalence of systemic autoimmune diseases in Hungary [2] Prevalence ratio: prevalence of HT or GD among autoimmune patients in the present study/prevalence of HT or GD in the general population CI confidence interval
Association of systemic and thyroid autoimmune diseases. Clinical rheumatology. 2006;25:240-245
• They set out to quantify the risk of coexisting autoimmune diseases in an extensive cohort of more than 3000 UK subjects with well-characterized autoimmune thyroid disease, as well as in their parents, and to compare findings for Graves’ disease and Hashimoto’s thyroiditis in women and men.
• 9.67% of the 2791 subjects with Graves’ disease and 14.3% of the 495 patients with Hashimoto’s thyroiditis had another autoimmune disorder (P<.005).
• Among index cases with Graves’ disease and Hashimoto’s thyroiditis, rheumatoid arthritis was most common.
The American journal of medicine. 2010;123:183.e1-183.e9.

The American journal of medicine. 2010;123:183.e1-183.e9.
Relative Risk of Diagnosis of Other Autoimmune Diseases in Parents of Index Cases with Graves' Disease or Hashimoto's Thyroiditis Calculated Using United Kingdom Prevalence Data
Diagnosis of Graves' Disease in Index Case
Diagnosis of Hashimoto's Thyroiditis in Index Case
Associated Autoimmune Disease
Relative Risk 95% CI P Value Relative Risk 95% CI P Value
Hyperthyroidism 8.32 7.43-9.29 <.001 4.51 3.03-6.43 <.001Hypothyroidism 6.09 5.40-6.84 <.001 14.65 12.22-17.36 <.001Type 1 diabetes 3.64 2.83-4.59 <.001 7.43 4.83-10.90 <.001Rheumatoid arthritis 13.55 12.32-14.86 <.001 13.04 10.26-16.29 <.001Pernicious anemia 14.1 11.48-17.03 <.001 15.54 9.53-23.87 <.001Systemic lupus erythematosus
4.65 1.87-9.56 0.001 7.48 1.97-26.96 0.03
Addison's disease 5.97 1.23-17.44 0.015 Celiac disease 5.73 3.28-9.30 <.001 6.1 1.25-17.66 0.014Vitiligo 6.09 4.22-8.50 <.001 8.08 3.50-15.86 <.001Multiple sclerosis 3.45 2.23-5.08 <.001 3.11 1.17-7.93 0.042Myasthenia gravis 2.39 0.29-8.63 0.638 6.73 0.17-37.43 0.138Inflammatory bowel disease
2.34 1.62-3.27 <.001 1.17 0.24-3.40 1
CI = confidence interval. P values were calculated through the single exact binomial proportion test.

• The higher prevalences and relative risks of rheumatoid arthritis in parents compared with index cases suggest a strong disease association.
• For each autoimmune disease investigated, the present data provide novel information about disease clustering, strongly supporting the prese
• Low threshold for screening for these diagnoses should be used.
• This applies especially to patients with autoimmune thyroid disease who remain nonspecifically unwell or who develop new symptoms despite adequate treatment.

Association between Rheumatic and Autoimmune Thyroid Diseases
Rheumatic disease
Pathophysiological mechanism
Association with AITD
Genetic participation
Major thyroid disease
Most frequent hormone change
Sjogren syndrome
Polyclonal autoimmune response389 + 3,8,9,11
HLA-B8 and DR31,6-9 HT13
Clinical and subclinical
hypothyroidism8,12
SLEPolyclonal autoimmune response, drugs, low T3 syndrome, chance17,18,22
+17,19
HLA-B8 and DR3
Susceptibility gene in 5q14.3-
q1 520,21
HT17,22
Clinical and subclinical
hypothyroidism18,22,2
3
Rheumatoid arthritis
Polyclonal autoimmune response5
+3,5,28-31HLA-DR3 HLA-
DR4 HLA-A2424,26
HT3,5,28-31 Hypothyroidism31
JIAPolyclonal autoimmune
response+ 63-69 68 HT23,63-69
Subclinical hypothyroidism 63-69
SclerodermaPolyclonal autoimmune
response, thyroid fibrosis1,39
+ 39,42 HLA-DR1540 HT11,41 Hypothyroidism39,42-
44
PR/GCA/other vasculitides
? ? ? HT1,46 Hypothyroidism47-49
Rheumatic fever ?
? Report of patients
with CRCD53,54,56-
60
? HT60 Hyper/hypothyroidism59
Fibromyalgia ? ? ? ATA +72
Decrease in thyroid hormones after
stimulus with TRH71
SLE: systemic lupus erythematosus; JIA: juvenile idiopathic arthritis; PR: polymyalgia rheumatica; GCA: giant cell arteritis; AITD: autoimmune thyroid disease; HT: Hashimoto's thyroiditis; CRCD: chronic rheumatic cardiac disease; ATA: antithyroid antibodies; TRH: thyrotropin-releasing hormone; +: positive; ?: inconclusive
Autoimmune thyroid disease in patients with rheumatic diseases. REVISTA BRASILEIRA DE REUMATOLOGIA. 2012;52:417-430.

Thank You

















