DEAR FRIEND, Five years ago, Global Health Corps was just an idea ruminating in the heads of six passionate twentysomethings. When Peter Piot challenged the audience at the aids 2031 Conference hosted by UNAIDS and Google in 2008 to engage our generation in solving the world’s health problems, we decided to take that challenge on as our own. After a weekend retreat in Baltimore, the rough business plan for Global Health Corps was born. Our idea was to create opportunities for passionate young leaders with diverse skillsets to serve in health organizations, and to equip these young people with the tools, skills, and network to be changemakers in global health throughout their careers. This, we believed, was the way to make a lasting, widespread, and sustainable impact in global health now, while seeding the field with talent to solve future problems. In fact, we were so convinced by our idea we were sure another organiza- tion was already doing it! As we spoke with various friends and mentors, people like Wendy Kopp, Larry Brilliant, and Paul Farmer, and met with leading organiza- tions like Partners In Health and Clinton Health Access Initiative, it became increasingly clear that not only was no one doing this in the health sector, but also we were going to be the ones to pioneer it. 5 years later, GHC has grown from a big idea to an even bigger reality. Since 2009, we have grown nearly 500%: increasing from 22 fellows in our first class to 106 fellows currently. We have worked in 7 countries, placed fellows at more than 50 leading health organi- zations, and supported 216 alumni spread across x countries who continue to address social justice issues everyday. As we look back on the past 5 years, we’re inspired by the positive impact our fellows have had in the communities in which they serve. We’ve seen fellows like Isaac Mugumbule and Ann Marie Brouillette work with CHAI Uganda to develop and implement a system that reduces HIV test turn-around time from 25 days to 3 days, ensuring early access to treatment and the prevention of transmission of HIV from mothers to their children. We’ve also seen the power of the GHC network in action; After continued stockouts of blood throughout Malawi, Global Health Corps fellows and alums organized a blood drive to ensure local clinics and hospitals were stocked, directly reducing maternal and child deaths in rural areas. Our work is far from over. When the leading causes of under-5 mortality in low-income countries include preventable illnesses like pneumonia and diarrhea, when more than one-third of U.S. adults are obese, and when 800 women a day are still dying in childbirth – almost all from preventable causes, we know we have our work cut out for us. We also know that the more young leaders we bring into the field of global health, the possibilities for continued impact and solutions grows exponentially, and that is what drives us. We are immensely grateful for those who have offered their generosity, their advice, their encouragement, and their partnership over these past five years. We consider each of you collaborators in our work and are more energized than ever to continue building this movement with you to make health equity a reality. As Temie Giwa, GHC fellow ’12 says, “Thank you for being part of our tribe.” In gratitude, Barbara A mother and daughter recieving materials from ACODEV in Uganda.
Transcript
DEAR FRIEND,Five years ago, Global Health Corps was just an idea ruminating in the heads of six passionate twentysomethings. When Peter Piot challenged the audience at the aids 2031 Conference hosted by UNAIDS and Google in 2008 to engage our generation in solving the world’s health problems, we decided to take that challenge on as our own. After a weekend retreat in Baltimore, the rough business plan for Global Health Corps was born. Our idea was to create opportunities for passionate young leaders with diverse skillsets to serve in health organizations, and to equip these young people with the tools, skills, and network to be changemakers in global health throughout their careers. This, we believed, was the way to make a lasting, widespread, and sustainable impact in global health now, while seeding the field with talent to solve future problems. In fact, we were so convinced by our idea we were sure another organiza-tion was already doing it!
As we spoke with various friends and mentors, people like Wendy Kopp, Larry Brilliant, and Paul Farmer, and met with leading organiza-tions like Partners In Health and Clinton Health Access Initiative, it became increasingly clear that not only was no one doing this in the health sector, but also we were going to be the ones to pioneer it.
5 years later, GHC has grown from a big idea to an even bigger reality. Since 2009, we have grown nearly 500%: increasing from 22 fellows in our first class to 106 fellows currently. We have worked in 7 countries, placed fellows at more than 50 leading health organi-zations, and supported 216 alumni spread across x countries who continue to address social justice issues everyday.
As we look back on the past 5 years, we’re inspired by the positive impact our fellows have had in the communities in which they serve. We’ve seen fellows like Isaac Mugumbule and Ann Marie Brouillette work with CHAI Uganda to develop and implement a system that reduces HIV test turn-around time from 25 days to 3 days, ensuring early access to treatment and the prevention of transmission of HIV from mothers to their children. We’ve also seen the power of the GHC network in action; After continued stockouts of blood throughout Malawi, Global Health Corps fellows and alums organized a blood drive to ensure local clinics and hospitals were stocked, directly reducing maternal and child deaths in rural areas.
Our work is far from over. When the leading causes of under-5 mortality in low-income countries include preventable illnesses like pneumonia and diarrhea, when more than one-third of U.S. adults are obese, and when 800 women a day are still dying in childbirth – almost all from preventable causes, we know we have our work cut out for us. We also know that the more young leaders we bring into the field of global health, the possibilities for continued impact and solutions grows exponentially, and that is what drives us. We are immensely grateful for those who have offered their generosity, their advice, their encouragement, and their partnership over these past five years. We consider each of you collaborators in our work and are more energized than ever to continue building this movement with you to make health equity a reality. As Temie Giwa, GHC fellow ’12 says, “Thank you for being part of our tribe.”
In gratitude, Barbara
A mother and daughter recieving materials from ACODEV in Uganda.
OUR MISSIONOur mission is to mobilize a global community of emerging leaders to build the movement for health equity. We are building a community of changemakers who share a common belief:
Health is a human right.
We believe that everyone has a role to play in advanc-ing social justice through the health equity movement.
We embrace a philosophy of active problem solving and partnership that is designed to bring about real and sustainable progress. We are committed to creating a new breed of health sector leaders that develop innovative solutions to the most challenging health problems all over the world.
OUR VISION
GHC fellows Latifah Kiribedda and Lisa Grossman at the 2012 GHC End of Year retreat.
“It’s been incredibly inspiring to see how the GHC community has grown over the past 5 years. We told our first class that they were all co-founders with us and this organization would only be as successful as the impact they had on their organizations and work.
Charlie Hale, GHC Co-founder
Those fellows and every class since have had an impact we never could have anticipated.
It’s been a great privilege to be a part of the GHC family.”
GHC fellows at the East Africa first quarter GHC retreat in Uganda.
THE PROBLEMGlobal Health Corps believes that the unacceptable status quo of extreme health inequity cannot be solved by a single organization, institution, or individual.
We also believe that the traditional models of global health development are not working: When innovation flows only from the North to the South, when local actors are not involved in implementing social change in their communities, and when organizations with common goals are not communicating, large-scale change cannot be achieved.
adolescents between 10and 19 are living with HIV
2 million
a child dies from malaria in Africa
Every 60 seconds
of maternal deaths occur in developing countries
99%
deaths from tuberculosis in 20121.3 million
people pushed into poverty annuallyas result of health care expenditure
100 million
Source: World Health Organization
Step 2: Recruit and select exceptional young leaders with diverse skills.
Step 3: Pair them up.
Step 1: Identify high-impact health organizations with a gap that needs filling.
Step 4: Match them to an organization.
Step 6: Create a global network of fellows and alumni impacting health equity.
Step 5: Train them.
OUR APPROACHWe partner with existing non-profit organizations and government agencies in East and Southern Africa and the US whose impact would be increased by having 2 of our fellows.
We open the door for passionate young people with backgrounds in fields as varied as finance, IT, and architecture to apply those skills to the global health movement.
Fellows work in pairs – a local fellow and an international fellow – because we know that sustainable change can only be made when local voices are included and cross-cultural collaboration takes place.
During a paid year of service, fellows strengthen and learn from their placement organizations, working on a variety of health issues from HIV/AIDS to maternal and child health.
Throughout the year, fellows participate in trainings, workshops, and conferences aimed at increasing their effectiveness as practitioners and their development as global health leaders.
Through retreats, networking events, and mentorship, we facilitate communication and collaboration amongst our fellows and alumni, enabling stronger collective action to move the needle on global health issues.
Our fellows are fighting for global health equity today and together will lead the movement in the coming decades.
Midwives and nurses at Iwemba Health Center III in Bugiri district, Eastern Uganda
"We founded GHC on the idea that a global community of talented young leaders dedicated to health equity can achieve it. This global community is growing, its impact is real, and my belief in its power is stronger than ever."David Ryan, GHC Co-founder
GHC fellow Eliza Ramos at End of Year Retreat in Jinja, Uganda.
Since 2009, we’ve expanded our network 500% to
OUR REACH
22
106
4441
68
3036
158placement
orgs
fellows
include 322 alums and 44 placement organizations from Ministries of Health and small, grassroots nonprofits to large NGOS in six countries in the US and East and Southern Africa.
placement orgs
fellows placement orgs
fellows
placement orgs
fellows
90fellows
placement orgs
Our 2012 - 2013 fellows worked with 41 high-impact health organizations in Burundi, Malawi, Rwanda, Uganda, the US and Zambia.
PLACEMENT ORGANIZATIONSSince 2012, our fellows have worked with the following high-impact health organizations.
For the 2012-2013 fellowship year, our fourth class had
90 fellows from 12 countries.
Over 45 fields of expertise are represented including:
public health,architecture, computer science international relations economics, finance,
community health medicine, political science, epidemiology, agriculture, pharmacy, health
policy, global health, evaluation, program management, education, civil, biomedical and
environmental engineering.
"I cannot stress this enough -- at least 60% of my total learn-ing came directly from my co-fellow. The co fellow model is one of the absolute best parts of GHC." 2012-2013 fellow
They speak XX languages.
They worked with 34 organizations in 6
countries in the US and East and Southern Africa.
have graduate degrees including Master of Public Health, MA in Architecture, Master of Policy Administration, Master of Social Work, and Master of Education
XX%
average age 26
undergraduateprograms
graduateprograms
nonprofitsector
government/public sector
corporate/private sector
Selected from over
4100 applicants.
12%
20%
38%
12%
18%
GHC fellows come from a wide range of sectors and professional backgrounds.
"This experience forever changed my career trajectory and set me on a path where I can continue to work towards realizing a world where health equity is a reality."
2012-2013 fellow
Midwives and nurses at Iwemba Health Center III in Bugiri district, Eastern Uganda
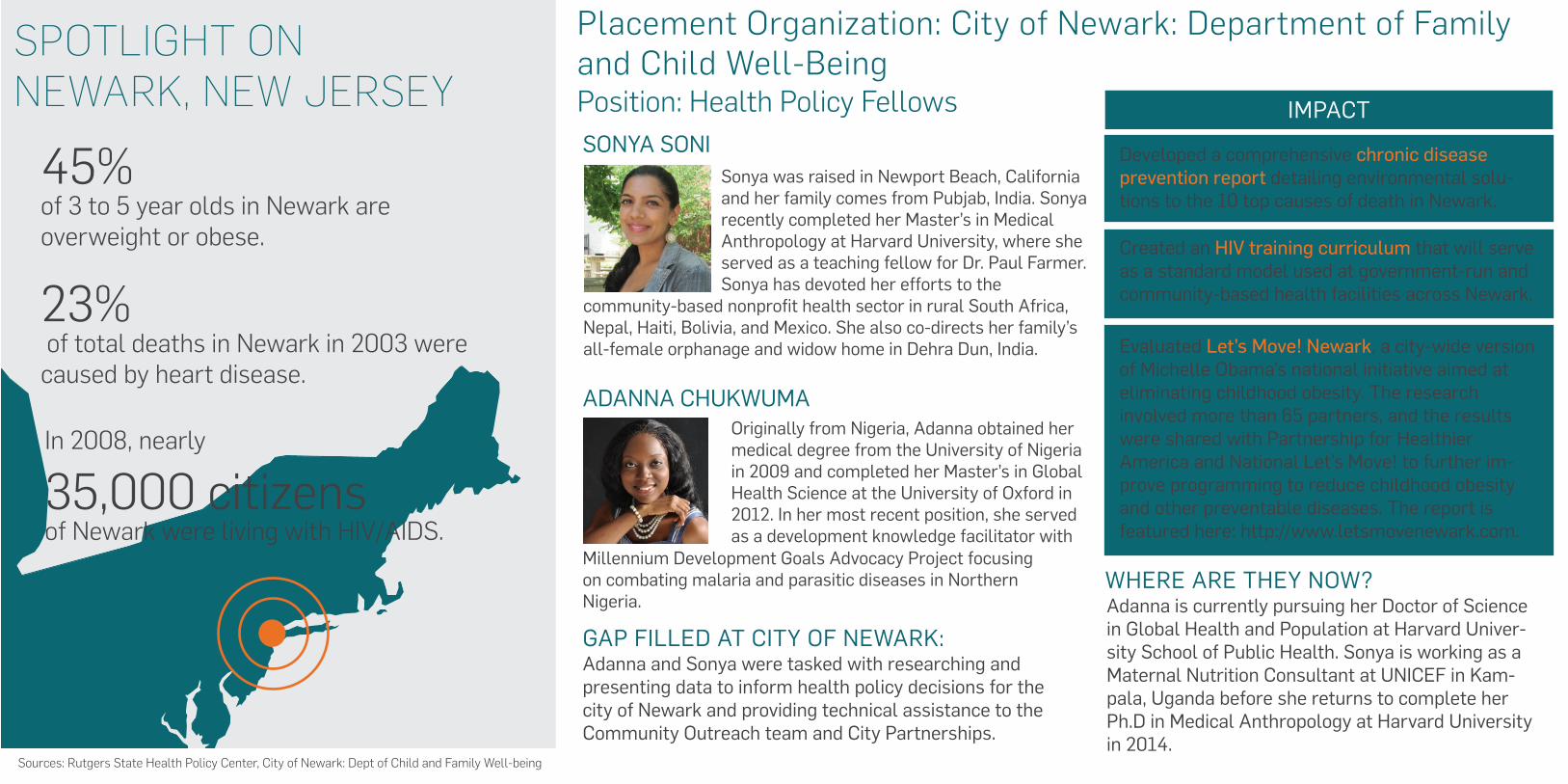
SPOTLIGHT ON NEWARK, NEW JERSEY
ADANNA CHUKWUMAOriginally from Nigeria, Adanna obtained her medical degree from the University of Nigeria in 2009 and completed her Master’s in Global Health Science at the University of Oxford in 2012. In her most recent position, she served as a development knowledge facilitator with
Adanna and Sonya were tasked with researching and presenting data to inform health policy decisions for the city of Newark and providing technical assistance to the Community Outreach team and City Partnerships.
Adanna is currently pursuing her Doctor of Science in Global Health and Population at Harvard Univer-sity School of Public Health. Sonya is working as a Maternal Nutrition Consultant at UNICEF in Kam-pala, Uganda before she returns to complete her Ph.D in Medical Anthropology at Harvard University in 2014.
Developed a comprehensive chronic disease prevention report detailing environmental solu-tions to the 10 top causes of death in Newark.
Created an HIV training curriculum that will serve as a standard model used at government-run and community-based health facilities across Newark.
Evaluated Let’s Move! Newark, a city-wide version of Michelle Obama’s national initiative aimed at eliminating childhood obesity. The research involved more than 65 partners, and the results were shared with Partnership for Healthier America and National Let’s Move! to further im-prove programming to reduce childhood obesity and other preventable diseases. The report is featured here: http://www.letsmovenewark.com.
IMPACT
Millennium Development Goals Advocacy Project focusing on combating malaria and parasitic diseases in Northern Nigeria.
WHERE ARE THEY NOW?
GAP FILLED AT CITY OF NEWARK:
SONYA SONISonya was raised in Newport Beach, California and her family comes from Pubjab, India. Sonya recently completed her Master’s in Medical Anthropology at Harvard University, where she served as a teaching fellow for Dr. Paul Farmer. Sonya has devoted her efforts to the
community-based nonprofit health sector in rural South Africa, Nepal, Haiti, Bolivia, and Mexico. She also co-directs her family’s all-female orphanage and widow home in Dehra Dun, India.
45% of 3 to 5 year olds in Newark are overweight or obese.
Sources: Rutgers State Health Policy Center, City of Newark: Dept of Child and Family Well-being
In 2008, nearly
35,000 citizens of Newark were living with HIV/AIDS.
23% of total deaths in Newark in 2003 were caused by heart disease.
Placement Organization: City of Newark: Department of Family and Child Well-BeingPosition: Health Policy Fellows
Sonya Soni, 2012-2013 GHC fellow
“Working as a health policy fellow for the City of Newark provided me with the opportunity of bringing best practices from my ancestral lands of rural India to Newark. Striving to adapt India's national community health worker model to one of America's most marginalized cities truly taught me the definition of global health equity."
SPOTLIGHT ON KAMPALA, UGANDA
CJ SCHELLACKOriginally from New Jersey and Vermont, CJ was a policy director in the National Security Council in the White House prior to her GHC fellowship. In this position she advised senior White House staff, managed the U.S. Govern-ment policymaking process, and authored
Brian and CJ were tasked with providing technical assistance and oversight to the Ugandan Ministry of Health in areas including HIV, malaria and commodities management.
Both CJ and Brian remained with CHAI Uganda after their fellow-ships. CJ is an HIV Systems and Drug Access Coordinator and Brian is a Country Support Technical Associate.
Placement Organization: Clinton Health Acess Initiative, Uganda
Introduced and pioneered HP-developed GSM printer technology that will provide near-immediate Early Infant Diagnosis HIV tests, significantly reducing the turnaround time of test results between satellite health facilities and the central testing laboratory. This reduced time will allow for early the early initia-tion of anti-retroviral therapy in infants, which is criti-cal for reducing reduce HIV-related morbidity and mortality in HIV-infected infants.
Forecasted Uganda’s entire demand for pediatric drugs and Early Infant Diagnosis commodities, ultimately procuring $2 million worth of these commodities with UNITAID funds.
Wrote the national training manual on Option B+, used across the country at public sector facilities. Option B+ provides treatment life-long treatment for all HIV-positive pregnant women, preventing mother-to-child transmission of the virus.
IMPACT
WHERE ARE THEY NOW?
GAP FILLED AT CITY OF NEWARK:
BRIAN NGWATUOriginally from Uganda, Brian is a medical doctor by training with a degree in medicine and surgery from Mbarara University of Science and Technology. Most recently, he worked as a care and treatment specialist at Baylor-Uganda in a health-systems-strengthening project in the West Nile region of Uganda.
Position: Access to Medicines Analysts
20,000 infants in Uganda are infected with HIV through transmission from their mother each year.
Sources: World Health Organization, Clinton Health Access Initiative.
64% of households reported that essential medicines were unaffordable in 2008.
reports for the President and National Security Advisor.
Supported national scale up of intravenous Artesunate for severe malaria, a drug with lower side effect profile and proven better clinical outcomes in the treatment of severe malaria in children than the previously preferred Quinine.
Malaria prevalence in Uganda is over
6x higher than the global average.
“You need a pot to cook, but you need firm stones to hold the pot in place. We've seen CHAI take a committed position amongst stake-holders in backing the local health ministry's efforts to positively trans-form health service delivery in Uganda."
Brian Ngwatu, 2012-2013 GHC fellow
{xxxxxxx} Burundi.
Sources: International Fund for Agricultural Development, World Health Organization, UNICEF
SPOTLIGHT ON NENO, MALAWI
JEFFREY TILLUSBorn in Haiti, Jeff graduated with a degree in Economics, Health Care Policy, and Manage-ment and Legal Studies from University of Pennsylvania’s Wharton School of Business. Before joining GHC, he interned in health care investment banking at Jefferies & Company.
Fatsani and Jeffrey were responsible for a $500,000+ budget for the purchase and delivery of clinical items as well as the construc-tion of new surgical wards at PIH Malawi. The fellows used their private sector experience to help develop cost-effective and effi-cient processes for the Operations Department.
Fatsani remained with PIH Malawi as a Clinical Adminis-trator after the fellowship. Jeffrey is currently working with another GHC placement organization, CHAI Malawi, on the Health Financing and Drug Access teams handling malaria initiatives.
Achieved at least 10%+ discount on each purchase, which resulted in cost savings of more than $50,000.
Implemented an electronic stock management system for tracking drugs and essential commodities. This ensured no stock-outs of essential medicines, palliative care, and chronic care between November 2012 and March 2013.This is a particularly impressive achievement because the national stock out level was 75% for essential medicines. The team, in partnership with the Ministry of Health and UNICEF, were able to ensure that patients receive the necessary care they deserved.
Spearheaded construction of a cell tower which doubled network coverage and improved communi-cations with Lower Neno, one of the poorest regions in Africa where half of PIH Malawi’s patients are located. The improved communication allowed for PIH to increase and improve the services provided and the number of supplies and drugs delivered to Lower Neno.
IMPACT
WHERE ARE THEY NOW?
GAP FILLED AT CITY OF NEWARK:
FATSANI BANDAOriginally from Malawi, Fatsani worked as a bank teller at the Standard Bank of Malawi before joining GHC. Prior to that she worked for the National Audit and the Tobacco Control Commission where she audited all the procured pharmaceuticals at one of the central hospitals in Malawi.
10% of adults in Malawi are living with HIV/AIDS
In 2009,
90% of Malawians lived on less than $2/day.
Almost 30% of poor children in Malawi did not attend primary school in 2009
Placement Organization: Partners in Health, MalawiPosition: Procurement & Logistics Coordinators-
Fellows at HIPS distributed 104,899 sterile needles throughout Washington, D.C., help-ing to curtail the spread of HIV, Hepatitis C, bacterial infections, and other infections common in intravenous drug users and sex workers. This year, the grade for syringe access services in DC increased to an A- from a B, and work at HIPS is specifically cited as one of the reasons for this progress.*
Fellows at Health Builders in Rwanda over-saw the national scale-up of community health worker training in SMS-based track-ing system for pregnant women, resulting in the training of over 20,000 CHWs (46% of the CHWs in the country) who will now be able to more easily track and deliver health-care to pregnant women.
Fellows at EGPAF Malawi developed stan-dardized M&E tools for the organization and trained 152 EGPAF sites on the tools, improving the implementation and impact of the organization’s projects. Fellows also supported 6 community based organizations in monitoring and implementing Prevention of Mother-to-Child Transmission services, which reached over 2,200 HIV-positive women last year.
Fellows at IDI in Uganda designed and imple-mented 5 eLearning courses for health care workers on comprehensive HIV prevention, pediatric ART management, online data man-agement, and computer training. Fellows trained over 80 health workers on the eLearn-ing materials.
Fellows at Last Mile Health in Boston, MA raised over $1 million to fund the organization's rural health programs in Liberia, more than doubling revenue totals from the previous year.
Fellows at MASS Design Group in Rwanda helped design a new health center and high-quality doctors’ housing with the aim of attracting and retaining skilled physicians in rural Rwanda.
Fellows at LifeNet International in Burundi established and managed relationships with the Ministry of Health, Ministry of Foreign Affairs, Medical Chiefs of Provinces, and church partners to facilitate LifeNet’s expan-sion into new clinics, where it provides nurse and management training, pharmaceutical distribution, and growth financing.
Fellows at ZCAHRD in Zambia served as Junior Survey Coordinators to implement the first National Tuberculosis Prevalence Survey to assess number of people suffering from TB. Zambia is now the first and only country to have a fully electronic survey, the results of which will help accurately distribute health resources and prevent the spread of the dis-ease.
of fellows worked onfinancial systems
of fellows addressedsupply chains
of fellows advocated for smarter health policies
of fellows strengthenedpartnerships
provided direct services to patients in need
provided training to the health workforce
strengthened commun-ications strategies
strengthened monitoring and evaluation systems
FELLOW IMPACTOur fellows work with high-impact health organizations to address a variety of pressing global health issues. Our 2012-2013 fellows made impact in the following areas:
26%
28%
47%
42%
12%
32%
49%
67%
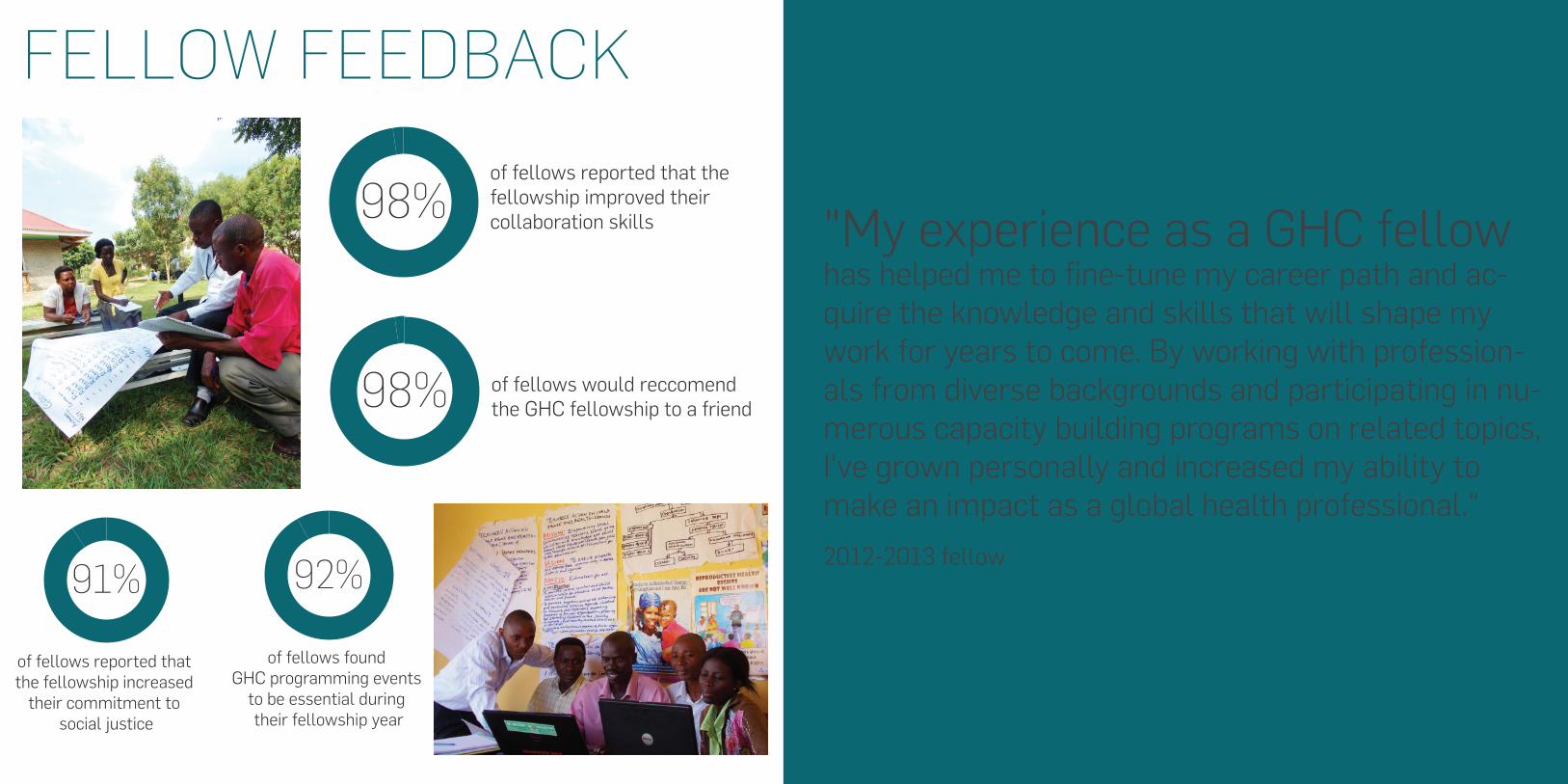
FELLOW FEEDBACK
of fellows found GHC programming events
to be essential during their fellowship year
of fellows reported that the fellowship increased
their commitment to social justice
of fellows would reccomend the GHC fellowship to a friend
of fellows reported that the fellowship improved their collaboration skills "My experience as a GHC fellow
has helped me to fine-tune my career path and ac-quire the knowledge and skills that will shape my work for years to come. By working with profession-als from diverse backgrounds and participating in nu-merous capacity building programs on related topics, I've grown personally and increased my ability to make an impact as a global health professional." 2012-2013 fellow
98%
91% 92%
98%
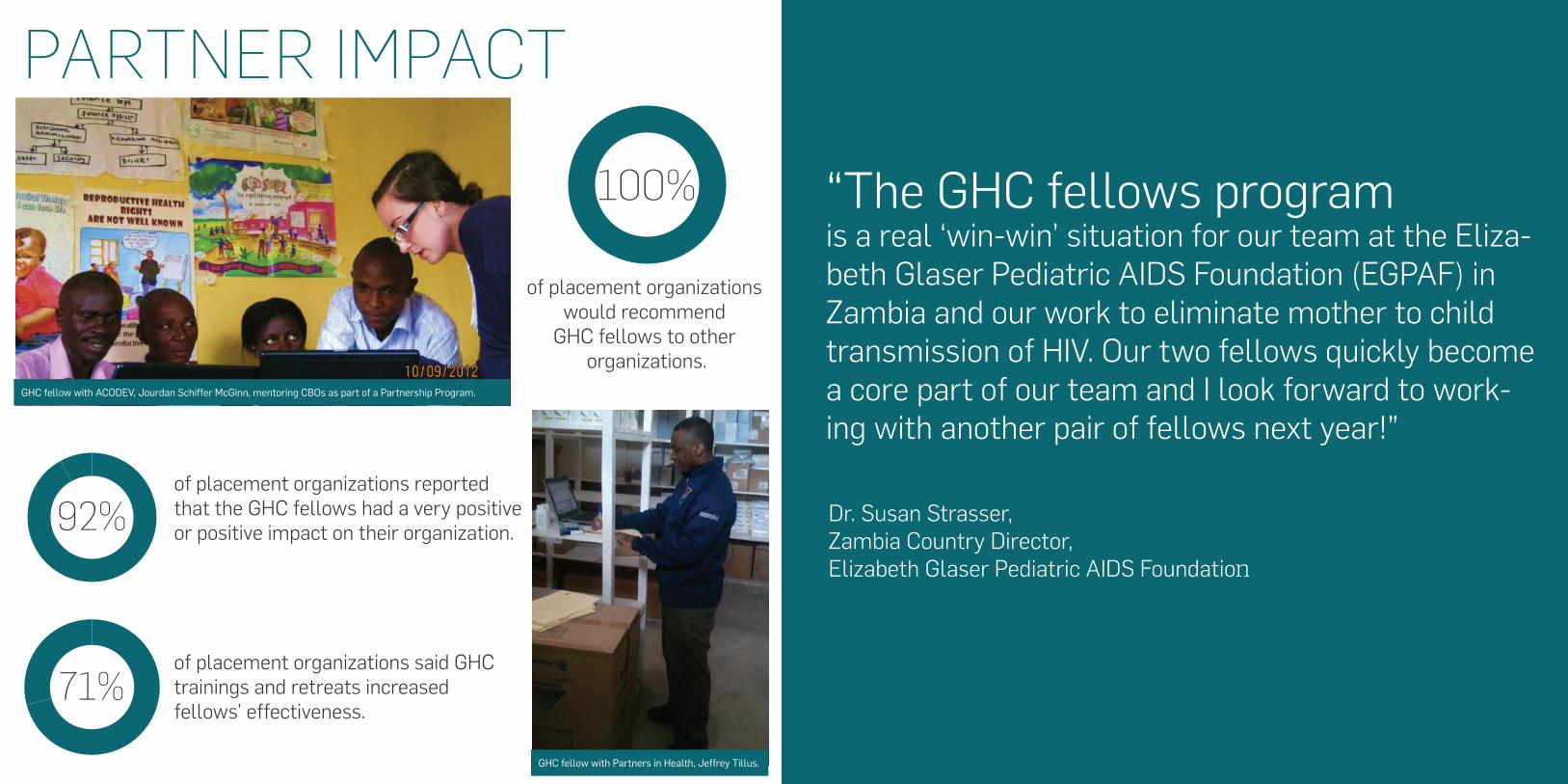
PARTNER IMPACT
“The GHC fellows program is a real ‘win-win’ situation for our team at the Eliza-beth Glaser Pediatric AIDS Foundation (EGPAF) in Zambia and our work to eliminate mother to child transmission of HIV. Our two fellows quickly become a core part of our team and I look forward to work-ing with another pair of fellows next year!”
Dr. Susan Strasser, Zambia Country Director, Elizabeth Glaser Pediatric AIDS Foundation
of placement organizations would recommend
GHC fellows to other organizations.
100%
of placement organizations reported that the GHC fellows had a very positive or positive impact on their organization.
of placement organizations said GHC trainings and retreats increased fellows’ effectiveness.
92%
71%
GHC fellow with ACODEV, Jourdan Schiffer McGinn, mentoring CBOs as part of a Partnership Program.
GHC fellow with Partners in Health, Jeffrey Tillus.
PROPELLING THE MOVEMENT
216 alums 106 fellows 24 citizenships44 organizations 6 countries
CHANGINGTHE CONVERSATIONOur fellows write op-eds, post blogs, present at TedX, and participate in conferences, making sure their voices are heard in the dialogue about improving health outcomes and access.
GHC fellow Mine Metitiri presents at Eat. See. Speak.
GHC fellow Adanna Chukwuma speaks at the 2013 Social Innovation Summit.
52%
of fellows are offered full-time positions with their
host organizations
37%
are employed at non-profit organizations such as
UNICEF, World Vision, IntraHealth, and UN Foundation
23%
are employed at GHC partner organizations including Partners in Health, MASS Design Group, CHAI and Millennium Villages
Project
are employed in government, including the US Dept. of
State, USAID, CDC andMinistries of Health
6%23%
of GHC alums pursued graduate degrees such as
MDs, PhDs, MPHs andother Masters
GHC alum Nargis Shirazi addresses Women Deliver 2013.
LOOKING FORWARD
0.0
0.2
0.4
0.6
0.8
1.0
This year, our fifth class has
106 fellows from 16 countries.
They speak 29 languages.
They will be working with over 45 partner organizations in
6 countries in the US and East and Southern Africa.
Over 45 fields of expertise are represented including:
Public Health, Architecture, Computer Science, International Relations, Economics, Finance, Community Health, Medicine,
Political Science, Epidemiology, Agriculture, Pharmacy, Policy, Global Health, Monitoring and Evaluation, Program
Management, Civil, Biomedical and Environmental Engineering.
average age 26.6
13%
undergraduateprograms
graduateprograms
20% 29%
nonprofitsector
government/public sector
20%
corporate/private sector
9%
Selected from almost 4000 applicants.
have graduate degrees includingMaster of Public Health, MA in Architecture, Master of Policy Administration, Master of Social Work, and Master of Education
45%
You take it with you. Being a fellow and having the support and mentorship of the GHC community, I further developed and matured my personal career mission and philosophy - one where health is a human right and we all have something to contribute in making our world more just and equitable.”
Emily Bearse, 2010-2011 fellow with CHAI Malawi
“Once you are a GHC fellow, you are always a fellow.
"The diverse experiences and skills of our fellows are a constant source of inspiration within the GHC community. Due to this our network of fellows has grown quicker, closer and stronger than we ever imagined." Andrew Bentley, GHC Co-founder
[xxxxxxxxxxxxx]
As we embark on our 6th year at Global Health Corps, the demand for growth is motivating: nearly 4,000 applicants applied for our 106 current fellowship positions (that’s a 2.6% acceptance rate!) and a record 120 organizations applied to host fellows next year (we currently work with 44 organizations!). We intend to recruit, select, and train 130 fellows in our next class – a 122% increase from our current class.
While we have no intention of slowing down, our current focus is on deepening and strengthening our program in the regions where we work before embarking on larger scale expansion.
In particular, GHC alums are on the top of our mind these days, as we’re beginning to reach a critical mass of GHC alums and fellows in our 6 placement countries. It has been well-documented that connecting people from different perspectives, knowledge, and backgrounds is necessary in order to solve complex problems. We agree, and it is central to our mission and impact to harness the energy, diversity, skills, and passion of our community after they have completed the fellowship in order to positively impact today’s most pressing health issues. We are focused on creating opportunities for alumni to collaborate, network, and help one another succeed. We’ve already seen our network in action, with alums serving as advisors to our current fellows, and country-established alumni committees drafting collective impact strategies.
In 15 years, our dream is to have GHC fellows represented at all major global health decision-making tables. As one of our fellows only half-joked, “It will be great when I’m the Minister of Health in Malawi, Soline is the Minister of Health in Rwanda, and Diego is running the Gates Foundation.” We couldn’t agree more!
Our fellows and alumni are equipped to change the health landscape today AND tomorrow and you’re our partner in helping them do it.
Thank You.
WHAT’S NEXT FOR GHC
FINANCIALS
Financial information based on audited financials statements.
Statement of Financial Position
AssetsCashReceivables Corporate and foundation grants Prepaid expensesProperty and equipment, netOther assets
1, 426,685
207, 56527, 67984,10720,089
688, 300
- 8,400
93,5215,550
1, 766,125 795,771Total Assets
2012 2011
Statement of Activities
Corporate and foundation grantsIndividual contributionsFundraisingIn-kind contributionsInterest
2,298,029488,474256,390150,734
673
1,292,020307,131
-210,332
58
3,194,300 1,809,541Total Revenue and Support
Liabilities and Net Assets Accounts payable and accrued expenses
Payroll withholdings Total liabilities
81, 78710, 25992,046
1, 766,125 795,771Total Liabilities and Net Assets
UnrestrictedTemporarily Restricted Total net assets
119,9766398
126,074
1,227,079447,000
1,674,079
669,697 -
669,697
Liabilities
Net Assets
Revenue and Support
Program Services Fellows and partners support Training and developmentManagement and generalFundraising Total Expenses
998,937441,358707,62042,003
2,189,918
2,189,918 1,190,562Net Assets, End of Year
Expenses435,209342,004413,349
-1,190,562
Increase in Net AssetsNet assets, beginning of yearPrior period adjustment