34
DRAFT DY7-8 Program Funding & Mechanics (PFM) Protocol Webinar Ardas Khalsa, John Scott, Noelle Gaughen, Emily Sentilles February 9, 2017 1

DRAFT DY7-8 Program Funding &
Mechanics (PFM) Protocol WebinarArdas Khalsa, John Scott, Noelle Gaughen, Emily Sentilles
February 9, 2017
1
DY7-8 Proposal
HHSC has requested CMS approval of an additional 21 months of level funding for the UC and DSRIP pools and a continuation of the managed care provisions of the 1115 Waiver, through September 30, 2019.
The implementation of the DSRIP structure is dependent on CMS approval of the additional 21 months and DSRIP protocols.
HHSC has posted a survey for feedback on the waiver website.
2

DSRIP DY7-8 Proposal The DY7-8 draft program structure evolves from project-
level reporting to targeted Measure Bundles that are reported by DSRIP Performing Providers as a provider system.
DY7-8 serves as an opportunity for Performing Providers to move further towards sustainability of their transformed systems, including development of alternative payment models to continue services for Medicaid and low-income or uninsured individuals after the waiver ends.
3

Current DY2-6 DSRIP Structure
Provider A
Category 1 or 2 Project 1 – MLIU QPI
Category 4 – P4R(only hospitals)
Category 3 Outcome 1a
Category 1 or 2 Project 2 – MLIU QPI
Category 1 or 2 Project 3 – MLIU QPI
Category 3 - Outcome 1b
Category 3 Outcome 2a
Category 3 Outcome 3a
Category 3 Outcome 3b
Category 3 Outcome 3c
Total Performing Provider Valuation per DY - $5 million4

Category C - Measure Bundle 2
Category C - Measure Bundle 1
Proposed DY7-8 DSRIP Structure
Note that any DY6 QPI and Category 3 milestones/metrics carried forward to DY7 will follow the DY6 structure and requirements.
Provider A
Category D – P4R (all Performing Providers)
Measure 1a
Category B – MLIU PPP for Performing Provider “system”
Measure 1b
Measure 2a Measure 2b
Measure 2c
Category A - Core ActivitiesAlternative Payment Methodology, Costs & Savings, Collaborative Activities
5
Measure 2d
Total Performing Provider Valuation per DY - $5 million

What about replacement projects?
Providers will have the funds planned for replacement projects allocated to use for the proposed new structure.
Existing DY2-6 Category 1 or 2 projects can continue under the new structure.
The planned replacement projects, existing projects, and new activities would represent “core activities”.
The “core activities” should be initiatives that assist providers to meet measures that are included in the selected measure bundles.
Providers may adjust core activities throughout DY7-8 without plan modifications.
6
DSRIP Pool Funding
The DSRIP pool allocation for DY7-8 would be $3.1 billion per DY. The $775 million allocated to DY6B would be combined
with the $2.325 billion for DY7.
HHSC is seeking proposals for uses of the remaining DSRIP funds, estimated at $25M available per DY.
7
DSRIP Provider Funding
A Performing Provider's total valuation for DY7 and DY8 would be equal to its total valuation for DY6A with the following exceptions: If HHSC determined that a DSRIP project was ineligible
to continue in DY6A, then the Performing Provider may use the funds associated with the DSRIP project beginning in DY7.
If a Performing Provider withdrew a DSRIP project between June 30, 2014 and June 30, 2016, then the Performing Provider may use the funds associated with the DSRIP project beginning in DY7.
8
Categories A-DCategories 1-4 in DY2-6 would be transitioned to the following Categories in DY7-8: Category A - Required reporting that includes progress on core
activities, alternative payment model arrangements, costs and savings, and collaborative activities.
Category B - Medicaid and Low-income or Uninsured (MLIU) Patient Population by Provider (PPP)
Category C - Measure Bundles
Category D - Statewide Reporting Measure Bundle, similar to the previous hospital Category 4 reporting expanded to include all Performing Providers.
9

Category Funding Distribution
*If private hospital participation minimums in the region are met, then Performing Providers may increase the Statewide Reporting Measure Bundle funding distribution to 10%.
DY 7 DY 8
Category A - required reporting 0% 0%
Category B - MLIU PPP 10% 10%
Category C- Measure Bundles 80 or 85% 80 or 85%
Category D - Statewide Reporting
Measure Bundle5 or 10% 5 or 10%
10
Category A: Required ReportingEach Performing Provider would be required to report the following during the second reporting period of each DY to be eligible for payment of Categories B-D.
Core Activities - Each Performing Provider would report on progress and updates to core activities.
Alternative Payment Methodology (APM) - Each Performing Provider would report on any progress toward or implementation of APM arrangements with Medicaid managed care organizations or other payors.
Costs and Savings - Each Performing Provider would submit costs of the core activities and forecasted/generated savings in a template approved by HHSC or a comparable template.
Collaborative Activities - Each Performing Provider would be required to attend at least one learning collaborative , stakeholder forum, or other stakeholder meeting each DY. 11

Category B: MLIU PPP
Each Performing Provider would be required to report the total number of individuals and number of MLIU individuals served by their system each DY.
HHSC is seeking stakeholder feedback on how to define “system”.
Each Performing Provider would be required to submit the baseline total number of individuals and the baseline number of MLIU individuals served by their system in the RHP Plan Update, based on the averages of DY5 and DY6. The baseline serves as the maintenance goal for DY7-8.
The baseline may be used to determine valuation in DY9-10. 12

Category B: MLIU PPP (cont.) To earn payment for Category B, each Performing Provider must
maintain the number of MLIU individuals served and the ratio of MLIU individuals served to total individuals served in DY7-8, within allowed variation thresholds.
The allowable variation would be determined by HHSC once Performing Providers have submitted their baselines, based on provider size and types.
MLIU PPP reporting would occur in the first round of the following DY, e.g. DY7 MLIU PPP would be reported in DY8 Round 1 – April 2019.
Partial payment would be available for MLIU PPP.
Although reporting would be streamlined, all reported MLIU PPP information may be audited.
13
Category C: Measure Bundles
Measure Bundles would consist of measures that share a unified theme, apply to a similar population, and are impacted by similar activities.
Bundling measures:
Allows for ease in measure selection and approval.
Increases standardization of measures across the state for providers with similar activities.
Facilitates the use of regional networks to identify best practices and share innovative ideas.
Continues to build on the foundation set in the initial waiver period while providing additional opportunities for transforming the healthcare system and bending the cost curve. 14

Measure Bundle Connections to
Previous Categories 1 and 2 The Measure Bundle Menu will be developed so that each
bundle will connect to one or more DSRIP Category 1 or 2 project areas on the Transformational Extension Menu (TEM).
Most DSRIP Category 1 and 2 project areas could be connected to one or more Measure Bundles.
The most common Category 1 and 2 project areas could connect to multiple bundles because they are broad activities.
Performing Providers would be required to describe the transition from DY2-6 projects to the selected Measure Bundles in the RHP Plan Update.
15

Measure Bundles Menu HHSC will work with stakeholders to finalize a menu of Measure Bundles.
The final menu may include measures taken from common existing Category 3 outcome measures, new or updated measures from authoritative sources, and innovative measures developed for DSRIP by participating entities to fill gaps in current standardized measures.
Innovative measures may be developed--pending interest--by a Texas entity functioning as a measure steward.
Bundles would include a mix of related process measures (currently designated as non-standalone [NSA]) and patient clinical outcomes (currently designated as standalone [SA]).
16

Measure Bundles Menu (cont.)
The following requirements will also be finalized in the Measure Bundles Menu and are not defined in the PFM Protocol:
Point values assigned to each Measure Bundle
Standard point valuation to calculate minimum point thresholds
Minimum point threshold cap
17
Measure Bundle Point ValueEach Measure Bundle would be assigned a point value based on one or more of the following factors:
The number of measures in the bundle and the difficulty of the measures in the bundle. (Ex: Current Category 3 stand-alone [SA] measures are worth 3 points, and current Category 3 non stand-alone [NSA] measures are worth 1 point).
Whether the measure is pay-for-performance (P4P) or pay-for-reporting (P4R).
Whether the bundle is considered a state priority. (Ex: If the bundle is considered a state priority, one point could be added to its value).
18

Measure Bundle Selection Criteria Each Performing Provider would be assigned a minimum point
threshold for Measure Bundle selection based on DY7 valuation and its size and role in serving the Medicaid and uninsured population.
HHSC is considering using factors such as Medicaid and uninsured costs and inpatient days as reported in the Uncompensated Care (UC) Tool, UC payments, and Disproportionate Share Hospital (DSH) payments.
There will be a cap on the minimum point threshold for providers with very high valuations.
Performing Providers would select one or more bundles to meet or exceed their minimum point threshold.
19

Example: Minimum Point Threshold Standard point valuation: $200,000
Minimum point value cap: 100
Minimum points increased for providers with a statewide ratio greater than 2
Hospital A Hospital B Hospital C Hospital D
DY7 Valuation $2,000,000 $2,000,000 $2,000,000 $100,000,000
% of Statewide DY6 valuation .05% .05% .05% 4.5%
% of Medicaid/UCFactors
.04% 0.02% .01% 4.2%
Statewide Ratio 1.25 2.5 5 1.07
Minimum Points 10 13 25 100 (not 268)20

Example (cont.) Hospital B selects the following Measure Bundles to total
at least 13 points.
Primary Care Prevention - Healthy Texans TOTAL: 4
PointsMeasure Type
IT-1.21 Adult Body Mass Index (BMI) Assessment Process +1
IT-1.23 Tobacco Use: Screening & Cessation Process +1
IT-12.4 Pneumonia vaccination status for older adults Process +1
IT-12.6 Influenza Immunization -- Ambulatory Process +1
New HIE Review for Opioid Prescribing (Innovative - P4R) Process +0
Cancer Screening TOTAL: 9
PointsMeasure Type
IT-12.1 Breast Cancer Screening Process +1
IT-12.13 Mammography follow-up rate Clinical +3
IT-12.15 Abnormal Pap test follow-up rate Clinical +3
IT-12.2 Cervical Cancer Screening Process +1
IT-12.3 Colorectal Cancer Screening Process +121
Measure Bundles for
CMHCs and LHDs
HHSC is proposing that each Community Mental Health Center (CMHC) be required to select a combination of measures to create one or more Measure Bundles.
HHSC is seeking proposals from Local Health Departments (LHDs) for their Measure Bundle requirements.
HHSC anticipates flexibility in measure selection for CMHCs and LHDs.
22

Measurement Periods
P4P Baseline: Calendar Year (CY) 2017
P4P Performance Year (PY) 1: CY 2018
P4R Reporting Year (RY) 1: DY7
P4P PY2: CY 2019
P4R RY2: DY8
23
DY7:
DY8:

Measure Bundle MilestonesThe milestone structure and valuation for DY7-8 would be as follows:
24
P4P Measure P4R MeasureDY7 25% baseline reporting
milestone100% Reporting Year (RY) 1 reporting milestone
25% Performance Year (PY) 1 reporting milestone50% PY1 goal achievement milestone
DY8 25% PY2 reporting milestone 100% RY2 reporting milestone
75% PY2 goal achievement milestone
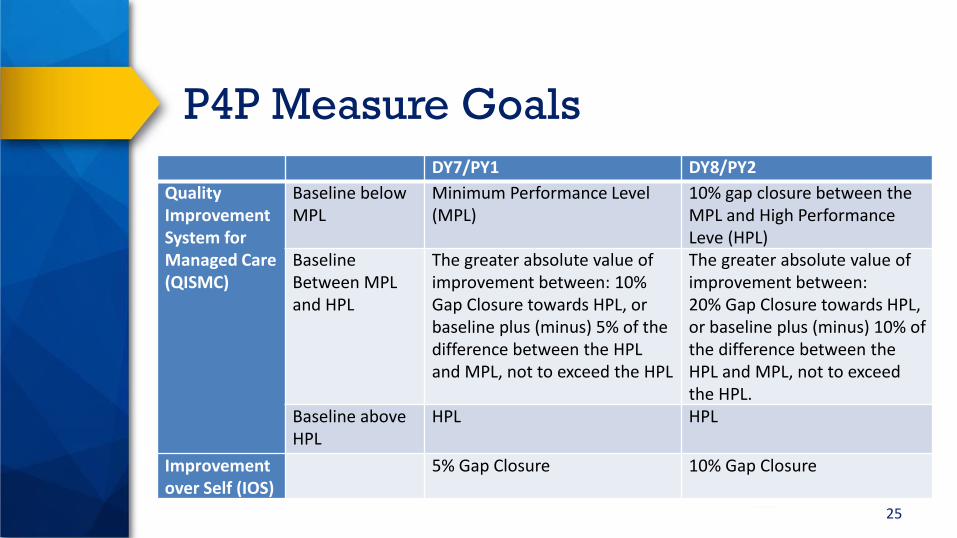
DY7/PY1 DY8/PY2
Quality Improvement System for Managed Care (QISMC)
Baseline below MPL
Minimum Performance Level (MPL)
10% gap closure between the MPL and High PerformanceLeve (HPL)
Baseline Between MPL and HPL
The greater absolute value of improvement between: 10% Gap Closure towards HPL, or baseline plus (minus) 5% of the difference between the HPL and MPL, not to exceed the HPL
The greater absolute value of improvement between: 20% Gap Closure towards HPL, or baseline plus (minus) 10% of the difference between the HPL and MPL, not to exceed the HPL.
Baseline above HPL
HPL HPL
Improvement over Self (IOS)
5% Gap Closure 10% Gap Closure
P4P Measure Goals
25

Measure Bundle Reporting
Each measure’s denominator population includes all individuals served by the Performing Provider system.
For P4P measure goal achievement milestones, each Performing Provider would be paid for achievement of the MLIU rate (with some exceptions due to data limitations) .
For P4P and P4R measure reporting milestones, each Performing Provider would be required to report the rate for All-Payer, Medicaid, and LIU payer types (with some exceptions due to data limitations) to be eligible for payment of the reporting milestone for the measure.
26

Measure Bundle Reporting (cont.)
Partial payment would be available for P4P measure milestones.
DY7 partial achievement = (PY1 Achieved -Baseline)/(PY1 Goal - Baseline)
DY8 partial achievement = (PY2 Achieved -Baseline)/(PY2 Goal - Baseline)
Carryforward of reporting (i.e., delayed reporting), not carryforward of achievement, would be allowed for all goal achievement milestones.
27

Category D: Statewide Reporting
Measure Bundle
Each Performing Provider would be required to report on the Statewide Reporting Measure Bundle according to the type of Performing Provider.
The measures would be similar to the previous Category 4 population-focused measures with additional measures developed for non-hospital Performing Providers with stakeholder involvement and feedback.
28

If a region maintains its current (DY6) level of private hospital participation, each Performing Provider in the region would be allowed to shift 5 percent of their total valuation from Category C (P4P) to Category D (P4R).
A region would demonstrate maintenance of private hospital participation at submission of the RHP Plan DY7-8 update.
A 3 percent decrease may be allowed in each region and considered maintenance.
The current statewide private hospital DY6 valuation is $868 million. With the allowable 3 percent decrease, there would be a statewide minimum total private hospital valuation of $842 million in DY7-8.
Private Hospital Participation
Regional Incentive
29
Estimated Timeline February 2017 – Gather stakeholder feedback on the draft PFM
Protocol using the survey posted on the waiver website. HHSC is particularly interested in feedback on:
Definition of provider “system”
Factors and weights to determine minimum point thresholds for hospitals and physician practices
Requirements for LHDs
Uses for remaining DSRIP funds – estimated $25M available per DY
March 31, 2017 – Submit PFM Protocol to CMS for approval.
30
Estimated Timeline (cont.) February – May 2017 – Gather stakeholder feedback on the Measure
Bundles.
Clinical Champions subgroups
CMHCs workgroup, in collaboration with the Texas Council
LHDs workgroup
Anchor workgroup
June/July 2017 – DY7-8 proposed rules posted for public comment.
June 30, 2017 – Submit Measure Bundle Protocol to CMS for approval.
August 2017 – Targeted CMS approval of protocols.
31

Estimated Timeline (cont.)
November 30, 2017 – Anchors submit RHP Plan Updates, including:
Updated community needs assessment
MLIU PPP - baseline total number of individuals and baseline number of MLIU individuals served by each Performing Provider’s system
Measure Bundle selections
New activities or ongoing activities from Performing Providers’ initial Category 1 or 2 projects to improve performance on the measures in their selected bundles
32

Proposed Reporting Timeline
33
Category A Category B Category C Category D
DY7 Apr DY7 P4P Measure Baseline
DY7 Category D
DY7 Oct DY7Category A
DY7 P4R Measure
DY8 Apr DY7 MLIU PPP
DY7 P4P Measure
Achievement
DY8 Category D
DY8 Oct DY8Category A DY8 P4R
MeasureDY9 Apr DY8 MLIUPPP
DY8 P4P Measure
AchievementDY9 Oct

Waiver Communications
Find updated materials and outreach details:
https://hhs.texas.gov/laws-regulations/policies-rules/waivers/medicaid-1115-waiver
Submit questions to:
34

















