68
Dr. Ahmad AlHadi Assistant Professor, Consultant of Psychiatry and Psychotherapy Department of Psychiatry, College of Medicine King Saud University Riyadh, Saudi Arabia

Dr. Ahmad AlHadi Assistant Professor, Consultant of Psychiatry and Psychotherapy
Department of Psychiatry, College of Medicine King Saud University Riyadh, Saudi Arabia

Agenda
• IntroducCon • Depression • CBT • CBT for Depression • Behavioral acCvaCon • Summary & feedback

Needs Assessment
• What do you want from this workshop (CBT for Depression)?
Objec0ves:
• AMendants of this workshop will: 1. Know the basic concept of CBT. 2. Know the CBT techniques. 3. Learn how CBT can be used in treatment of
Depression.

Why Depression?
• The 2nd leading cause for disability now • The 1st in 2020
• Chronic
• Common

Exercise
• Write down as much as you can of Depression symptoms and signs in one minute.

Major Depressive Disorder DSM5 Diagnos0c Criteria
A. Five (or more)of the following symptoms have been present during the same 2-‐week period and represent a change from previous func0oning: at least one of the symptoms is either (1) depressed mood or (2) loss of interest or pleasure. Note: Do not include symptoms that are clearly aNributable to another medical condi0on. 1. Depressed mood most of the day, nearly every day, as indicated by
either subjec0ve report (e.g., feels sad, empty, hopeless) or observa0on made by others (e.g., appears tearful). (Note: In children and adolescents, can be irritable mood.)
2. Markedly diminished interest or pleasure in all, or almost all, ac0vi0es most of the day, nearly every day (as indicated by either subjec0ve account or observa0on).
3. Significant weight loss when not die0ng or weight gain (e.g., a change of more than 5% of body weight in a month), or decrease or increase in appe0te nearly every day. (Note: In children, consider failure to make expected weight gain.)
4. Insomnia or hypersomnia nearly every day.

Major Depressive Disorder DSM5 Diagnos0c Criteria
5. Psychomotor agita0on or retarda0on nearly every day (observable by others, not merely subjec0ve feelings of restlessness or being slowed down).
6. Fa0gue or loss of energy nearly every day. 7. Feelings of worthlessness or excessive or inappropriate guilt (which may be
delusional) nearly every day (not merely self-‐reproach or guilt about being sick).
8. Diminished ability to think or concentrate, or indecisiveness, nearly every day (either by subjec0ve account or as observed by others).
9. Recurrent thoughts of death (not just fear of dying), recurrent suicidal idea0on with-‐ out a specific plan, or a suicide aNempt or a specific plan for commi[ng suicide.
B. The symptoms cause clinically significant distress or impairment in social, occupa0onal, or other important areas of func0oning. C. The episode is not aNributable to the physiological effects of a substance or to another medical condi0on.

Major Depressive Disorder DSM5 Diagnos0c Criteria
Note: Criteria A-‐C represent a major depressive episode. D. The occurrence of the major depressive episode is not beMer explained by schizoaffecCve disorder, schizophrenia, schizophreniform disorder, delusional disorder, or other specified and unspecified schizophrenia spectrum and other psychoCc disorders. E. There has never been a manic episode or a hypomanic episode. Note: This exclusion does not apply if all of the manic-‐like or hypomanic-‐like episodes are substance-‐induced or are aMributable to the physiological effects of another medical condiCon.

Diagnosis
• one or more Major Depressive Episode. DSM-‐IV-‐TR diagnosCc criteria: A. At least 5 of the following, during the same 2-‐week period, represenCng
a change from previous funcConing; must include either (a) or (b): 1. Depressed mood 2. Diminished interest or pleasure 3. Significant weight loss or gain (AppeCte) 4. Insomnia or hypersomnia (sleep) 5. Psychomotor agitaCon or retardaCon (acCvity) 6. FaCgue or loss of energy 7. Feelings of worthlessness (guilt) 8. Diminished ability to think or concentrate; indecisiveness 9. Recurrent thoughts of death, suicidal ideaCon, suicide aMempt, or specific
plan for suicide

Diagnosis DSM-‐IV-‐TR diagnosCc criteria:
B. Symptoms do not meet criteria for a mixed episode
C. Symptoms cause clinically significant distress or impairment of funcConing.
D. Symptoms are not due to the direct physiologic effects of a substance or a general medical condiCon.
E. Symptoms are not beMer accounted for by bereavement

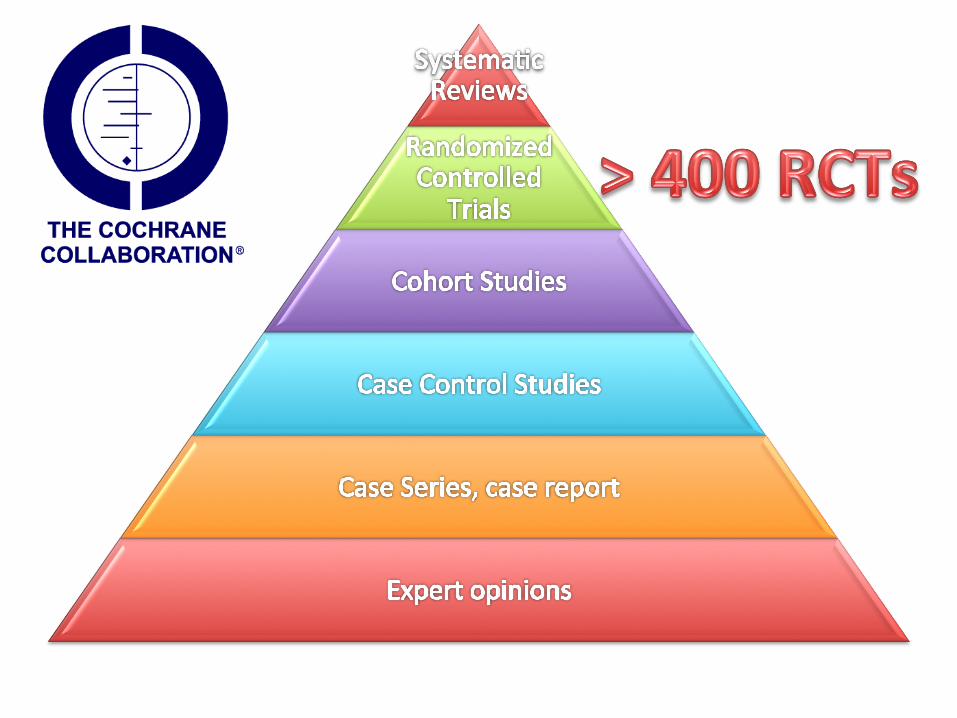
SCIENTIFIC EVIDENCES CBT for Depression

CBT for Major Depression • Bledsoe, S. E., & Grote, N. K. (2006). TreaCng depression during pregnancy and the
postpartum: A preliminary meta-‐analysis. Research on Social Work PracCce, 16, 109–120.
• Feldman, G. (2007). CogniCve and behavioral therapies for depression: Overview, new direcCons, and pracCcal recommendaCons for disseminaCon. Psychiatric Clinics of North America, 30, 39–50.
• Hollon, S. D., Thase, M. E., & Markowitz, J. C. (2005). Treatment and prevenCon of depression. Psychological Science in the Public Interest, 3, 39–77.
• Paykel, E. S. (2007). CogniCve therapy in relapse prevenCon in depression. InternaConal Journal of Neuropsychopharmacology, 10, 131–136.
• Wampold, B. E., Minami, T., Baskin, T. W., & Tierney, S. C. (2002). A meta-‐ (re)analysis of the effects of cogniCve therapy versus “other therapies” fordepression. Journal of AffecCve Disorders, 68, 159–165.
Guidelines
• (APA) • (NICE) • (CPA)

• NICE guidelines – mild to moderate • NIMH: – ‘By teaching new ways of thinking and
behaving, CBT helps people change negative styles of thinking and behaving that may contribute to their depression’.
• NIMH also recommends IPT • NIMH suggests that ‘for mild to
moderate depression psychotherapy may be the best treatment option’
Evidence base



THE MODEL CBT for Depression

Basic Cogni0ve Model
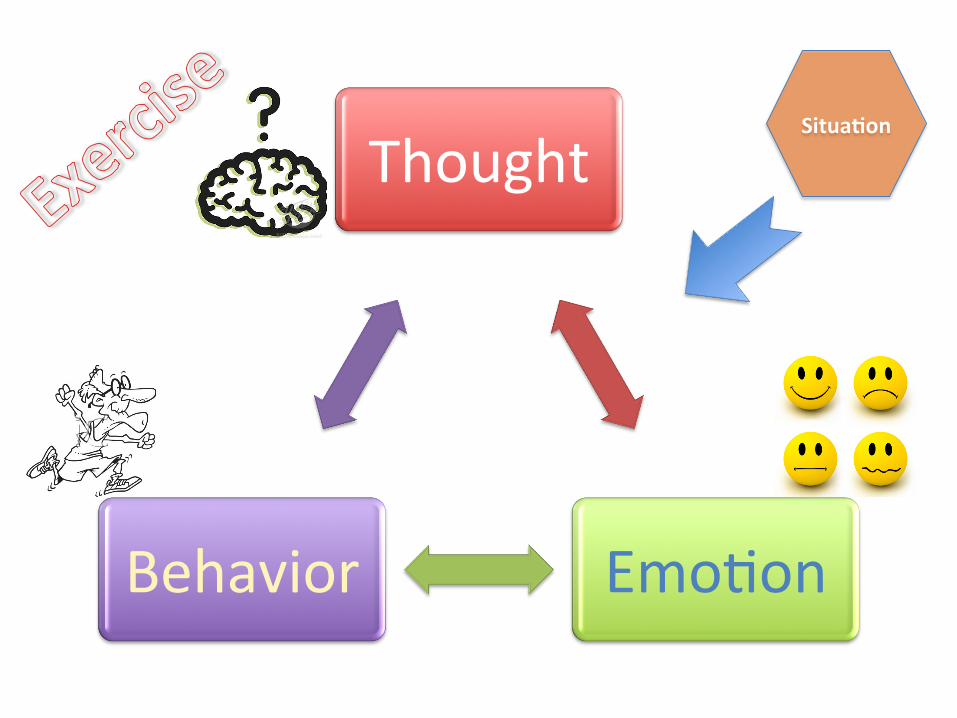
Thought
EmoCon Behavior
Situa0on

CBT Model
• Thoughts influence emoCon and behavior • Behavior influences thought and emoCons
• in CBT, paCents are taught to detect and modify inner thoughts and change behavior to reduce distress and promote well-‐being

Exercise
• Role play vs Video


Thinking of depressed people: – negaCve triad (negaCve view of self, future, the world)
– AMribuCon العزو (internal, global, fixed) – logical errors
Behavior of depressed people: – reduced acCvity level – increased unrewarding behaviors (eg. TV) – unrewarding interpersonal interacCons
CBT Model Depression

CogniCve: – restructuring of negaCve triad – idenCficaCon of faulty processing – alter underlying assumpCons, core beliefs
Behavioural: – increase pleasurable, saCsfying acCvity – change interpersonal behaviour
CBT of Depression

CBT for Depression
Assessment and
educa0on Techniques
Relapse preven0on
and termina0on

General Plan of Treatment for Depression
• Assessment – CogniCve, behavioral, and interpersonal assessment – Tests and other evaluaCons – EvaluaCon of suicidal risk – ConsideraCon of medicaCon
• SocializaCon to treatment • Establishment of goals • Behavioral acCvaCon and other behavioral intervenCons • CogniCve intervenCons • Relapse PrevenCon • Phasing out therapy

Behavioral Techniques for Depression
• Behavioral acCvaCon السلوكي التنشيط • Scheduling pleasure and mastery acCviCes
والتمكن املتعة جدول • Seeking social support االجتماعي الدعم • Graded task assignments اBزّئة املهام واجبات • Behavioral experiments السلوكية التجارب • Credit lists االجنازات قائمة • PracCcing social skills االجتماعية املهارات

Who is suitable for CBT?

Suitability for Short Term CT Ra0ng Scales (SRS) (Safran, Segal, Shaw & Vallis,1990)
1. Accessibility of automaCc thoughts 2. Awareness & differenCaCon of emoCon 3. Acceptance of personal responsibility for change 4. CompaCbility with cogniCve raConale 5. Alliance potenCal (in-‐session evidence) 6. Alliance potenCal (out-‐of-‐session evidence) 7. Chronicity 8. Security operaCons 9. Focality 10. General opCmism/pessimism about therapy

What do we need to look for in CBT assessment for depression
• Symptoms and signs for depression • Possible causes for depression • Support • Factors of CBT suitability

Formula0on • Called also ConceptualizaCon
• Stem from a thorough CBT assessment
• Incorporates consideraCon of the following: – Predisposing Factors – PrecipitaCng Factors – PerpetuaCng Factors – ProtecCve Factors
• will incorporate a consideraCon of these factors in therapy, also guide any therapeuCc intervenCons.

Use Scales
• BDI • PHQ9 • HAM-‐D • HAM-‐D-‐7

Session-‐by-‐Session Treatment Op0ons for Major Depression *
Session 1 • Assessment
– Ascertain presenCng problems Inquire regarding all symptoms – Assess for cogniCve, behavioral, and interpersonal deficits – Assess impairment in social, educaConal and occupaConal funcConing
Administer standard baMery of intake measures – Evaluate for comorbid condiCons (e.g., anxiety disorders) – Evaluate for suicidal risk – Evaluate substance use; evaluate need for counseling or detoxificaCon
if paCent has substance abuse or dependence – Assess need for medicaCon
• Homework – Have the paCent begin reading David Burns’s Feeling Good or The
Feeling Good Handbook
* From treatment plans for depression and anxiety, Robert Leahy, 2000

Session 2 • SocializaCon to Treatment • Inform paCent of diagnosis • Develop list of treatment goals • Provide paCent with informaCon handouts on depression and on
cogniCve-‐behavioral therapy in general • Evaluate homework • Behavioral IntervenCons
– IdenCfy behavioral targets (behavioral deficits and excesses) – Instruct paCent in reward planning and acCvity scheduling – Encourage paCent to increase self-‐reward – Encourage paCent to decrease ruminaCon Cme and passive/asocial behavior – Evaluate need for paCent to modify personal hygiene, grooming, diet,
bingeing, etc. – Evaluate/treat insomnia.

Session 2 • CogniCve IntervenCons
– Train paCent in relaConship between automaCc thoughts and feelings – Train paCent in categorizing distorted automaCc thoughts – Elicit and challenge automaCc thoughts in session – Evaluate reasons for and challenge hopelessness – Establish no-‐suicide contract – Challenge anC-‐pleasure thoughts
• MedicaCon – Consider medicaCon (if paCent is not already using it) Evaluate side
effects Evaluate need to increase dosage • Homework
– Have paCent record thoughts and moods, categorize automaCc thoughts, begin self-‐directed reward planning and acCvity scheduling, increase self-‐reward, and use graded task assignment

Socializa0on to treatment
• How to do it?
• Video
• Exercise

Goals
• Problems list • Behavioral • SMART • Magic wind technique

Goals
• Give me examples of good goals in Depression?
1. . 2. . 3. . 4. .

Prac0ce
• In Pairs: – Therapist and PaCent
– Put the problem list (2 items), and Therapy goals.

Behavioral ac0va0on
• It includes many techniques. – Scheduling pleasure and mastery acCviCes – Graded task assignments – PracCcing social skills – Seeking social support

Weekly Ac0vity Schedule
Saturday Sunday Monday Tuesday Wednesday Thursday Friday
8-‐9
9-‐10
10-‐11
11-‐12
12-‐1
1-‐2
2-‐3
3-‐4
4-‐5
5-‐6
6-‐7
InstrucCons: Write down your acCviCes for each hour and then rate them on a scale of 0–10 for mastery (m) or degree of accomplishment and for pleasure (p) or amount of enjoyment you experienced. A raCng of 0 would mean that you had no sense of mastery or pleasure. A raCng of 10 would mean that you experienced maximum mastery or pleasure.

Exercise
• Fill out the form about last two days.

Tips for behavioral ac0va0on *
1. Develop a collaboraCve relaConship before trying it.
2. Let the Pt decide. 3. Judge the Pt readiness to change. 4. Prepare the Pt for it (SocraCc quesConing,
MoCvaConal interview) 5. Design assignments that are manageable
* Learning CBT, Wright et al, 2007

Weekly Ac0vity Schedule
• Video
• Exercise: in pairs of two – Pt has depression – Therapist who will explain to the pt the acCvity scheduling.

Sessions 3–4 • Assessment
– Evaluate homework – Evaluate depression (BDI) and anxiety (BAI) – Evaluate suicidality – Evaluate any side effects from medicaCon
• Behavioral IntervenCons – Teach and pracCce asserCon skills in session – Increase rewarding behavior toward others – Increase posiCve social contacts—iniCaCng contact, building support network
– Evaluate self-‐reward – Introduce problem-‐solving skills
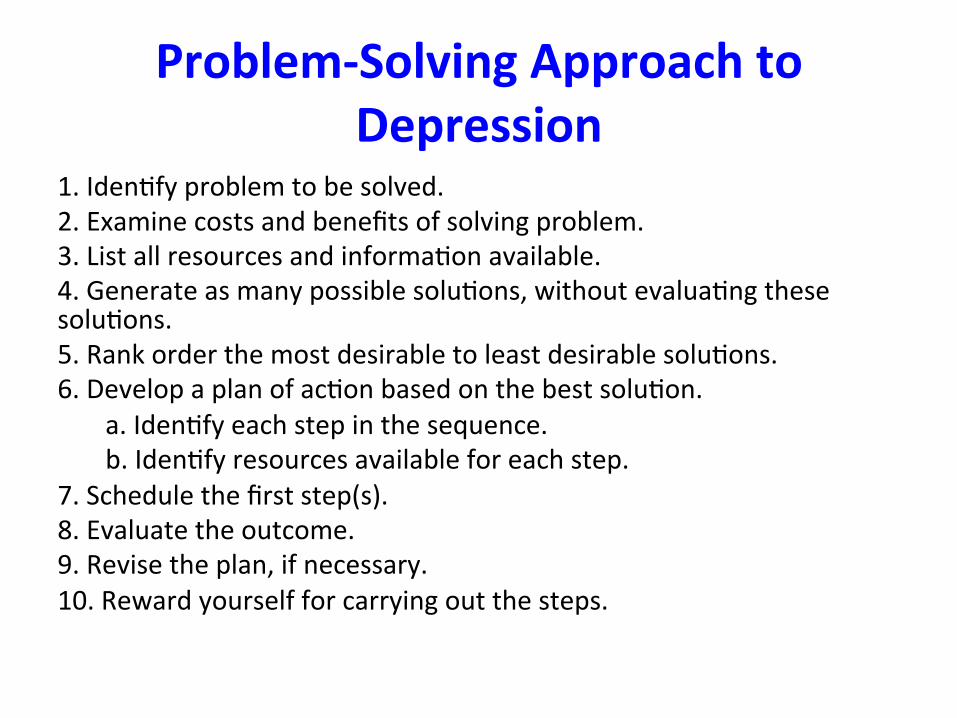
Problem-‐Solving Approach to Depression
1. IdenCfy problem to be solved. 2. Examine costs and benefits of solving problem. 3. List all resources and informaCon available. 4. Generate as many possible soluCons, without evaluaCng these soluCons. 5. Rank order the most desirable to least desirable soluCons. 6. Develop a plan of acCon based on the best soluCon.
a. IdenCfy each step in the sequence. b. IdenCfy resources available for each step.
7. Schedule the first step(s). 8. Evaluate the outcome. 9. Revise the plan, if necessary. 10. Reward yourself for carrying out the steps.

Sessions 3–4 • CogniCve IntervenCons
– Teach use of PaCent’s Daily Record of DysfuncConal AutomaCc Thoughts (TR) – Use specific cogniCve techniques to help paCent challenge negaCve automaCc
thoughts – IdenCfy and challenge underlying maladapCve assumpCons
• MedicaCon – Evaluate side effects, Evaluate need to increase dosage If no improvement,
either increase dosage, add another medicaCon, or change class of medicaCon (consider the need to taper or disconCnue one class of medicaCon when adding another class)
• Homework – Have paCent use PaCent’s Daily Record of DysfuncConal AutomaCc Thoughts – assign specific cogniCve techniques for challenging automaCc thoughts and
assumpCons – have paCent conCnue with graded task assignment, social skills training,
reward planning, acCvity scheduling, problem solving

Sessions 5–7 • Assessment – Evaluate homework – Evaluate depression (BDI) and anxiety (BAI) Evaluate suicidality
• Behavioral IntervenCons – ConCnue to teach and pracCce problem-‐solving skills – Train paCent in communicaCon skills (acCve listening, ediCng communicaCon, empathy)
– ConCnue graded task assignment – ConCnue asserCon and social skills training

Sessions 5–7 • CogniCve IntervenCons
– IdenCfy and challenge automaCc thoughts that are parCcularly difficult for paCent
– ConCnue idenCfying and challenging maladapCve assumpCons – Begin to idenCfy and challenge negaCve schemas
• MedicaCon – Evaluate side effects, Evaluate need to increase dosage If no
improvement, either increase dosage, add another medicaCon, or change medicaCon class
• Homework – Have paCent pracCce using various techniques to challenge
assumpCons and schemas; – conCnue graded task assignment, asserCveness, self-‐reward; and
conCnue pracCcing communicaCon and problem-‐solving skills

Catch
Check
Correct Problem Solving

Cogni0ve Interven0ons
• Monitor automaCc thoughts • Teach imagery techniques • Promote cogniCve restructuring • Examine alternaCve evidence • Modify core beliefs • Generate raConal alternaCves

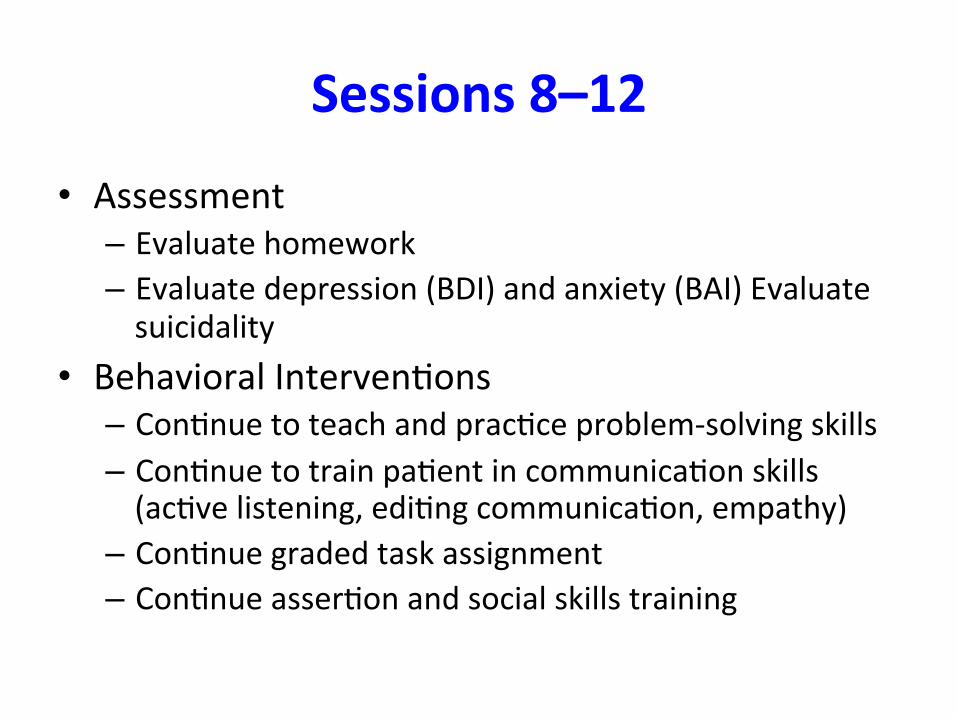
Sessions 8–12
• Assessment – Evaluate homework – Evaluate depression (BDI) and anxiety (BAI) Evaluate suicidality
• Behavioral IntervenCons – ConCnue to teach and pracCce problem-‐solving skills – ConCnue to train paCent in communicaCon skills (acCve listening, ediCng communicaCon, empathy)
– ConCnue graded task assignment – ConCnue asserCon and social skills training
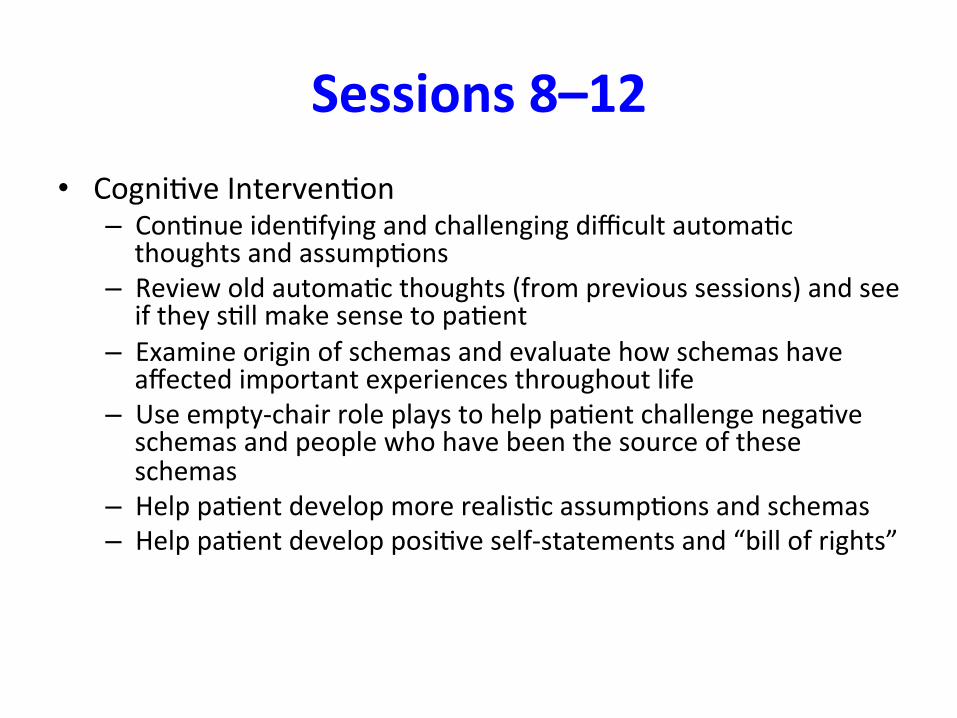
Sessions 8–12 • CogniCve IntervenCon
– ConCnue idenCfying and challenging difficult automaCc thoughts and assumpCons
– Review old automaCc thoughts (from previous sessions) and see if they sCll make sense to paCent
– Examine origin of schemas and evaluate how schemas have affected important experiences throughout life
– Use empty-‐chair role plays to help paCent challenge negaCve schemas and people who have been the source of these schemas
– Help paCent develop more realisCc assumpCons and schemas – Help paCent develop posiCve self-‐statements and “bill of rights”
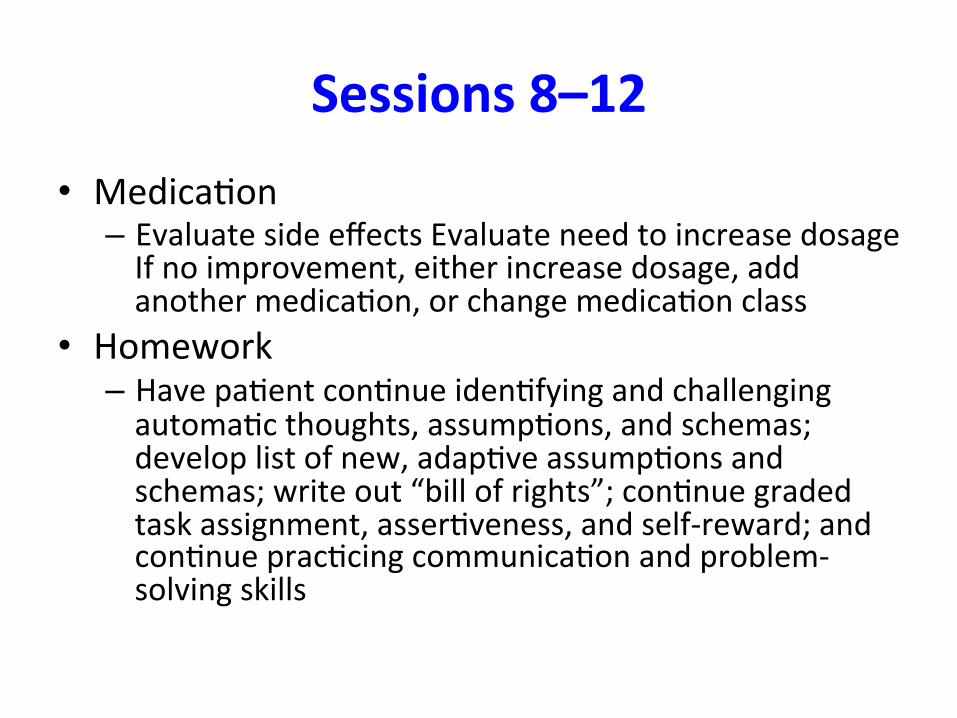
Sessions 8–12 • MedicaCon – Evaluate side effects Evaluate need to increase dosage If no improvement, either increase dosage, add another medicaCon, or change medicaCon class
• Homework – Have paCent conCnue idenCfying and challenging automaCc thoughts, assumpCons, and schemas; develop list of new, adapCve assumpCons and schemas; write out “bill of rights”; conCnue graded task assignment, asserCveness, and self-‐reward; and conCnue pracCcing communicaCon and problem-‐solving skills

Session 13–16 (Scheduled Biweekly or Monthly)
• Assessment – Evaluate homework Evaluate depression (BDI) and anxiety (BAI) Evaluate suicidality Evaluate any side effects from medicaCon
• Behavioral IntervenCons – ConCnue to teach and pracCce problem-‐solving skills – ConCnue graded task assignment – ConCnue asserCon and social skills training
From Treatment Plans and IntervenCons for Depression and Anxiety Disorders by Robert L. Leahy and Stephen J. Holland. Copyright 2000 by Robert L. Leahy and Stephen J. Holland.

Session 13–16 (Scheduled Biweekly or Monthly)
• CogniCve IntervenCons – Help paCent to conCnue developing more realisCc assumpCons and schemas – Have paCent conCnue work on posiCve self-‐statements and “bill of rights” – Review old automaCc thoughts (from previous sessions and from homework
assignments) and conCnue challenging them – Plan phase-‐out of therapy – Have paCent idenCfy which intervenCons were helpful and which were not – Have paCent examine previous episodes of depression and describe how he or
she will handle depression in the future
• Homework – Develop plans for how problems can be handled in future – Have paCent assign own homework – Have paCent indicate which problems he or she will work on once therapy
ends.
From Treatment Plans and IntervenCons for Depression and Anxiety Disorders by Robert L. Leahy and Stephen J. Holland. Copyright 2000 by Robert L. Leahy and Stephen J. Holland.

Relapse Preven0on
• Most useful techniques • Future difficulCes • Plans for Possible soluCons

ADVANCED THERAPIES CBT for Depression

CBASP • CogniCve Behavioral Analysis System of Psychotherapy
• a research-‐based psychotherapeuCc approach
• designed to moCvate chronically depressed paCents to change and help them to develop needed problem-‐solving and relaConship skills.
• Use CBT and IPT techniques.
James P. McCullough, Jr. PhD

CBASP
• To help Pt overcomes avoidance of interpersonal situaCons.
• Techniques: – specific situaConal analyses – training of interpersonal skills

MBCT
• MBCT: Mindfulness Based CogniCve Therapy
– by Zindel Segal, Mark Williams and John Teasdale, based on MBSR, 1995 .
– Recurrent depression. – Mindfulness + CT. – 8 weekly 2-‐hour classes + one full day. – evidence from two RCTs of MBCT è êrelapse by 50% among paCents who suffer from recurrent depression.

MBCT
• MBCT: Mindfulness Based CogniCve Therapy
– Class 1: AutomaCc Pilot, – Class 2: Dealing with Barriers, – Class 3: Mindfulness of the Breath, – Class 4: Staying Present, – Class 5: Allowing and Levng Be, – Class 6: Thoughts are Not Facts, – Class 7: How Can I Best Take Care of Myself, – Class 8: Using What’s Been Learned to Deal with Future Moods.

What about Bipolar Disorder?

Feedback

Thank you

















