32
By P. SIVA KRISHNA M. PHARMACY GIET School of Pharmacy Andhra University
| Date post: | 15-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | sivakrishnapinnika |
| View: | 151 times |
| Download: | 3 times |

ByP. SIVA KRISHNAM. PHARMACYGIET School of PharmacyAndhra University

FIRST-PASS EFFECTS
The topics under this phenomenon are:
Theory
Systems that effect pre-systemic metabolism
of a drug
Estimation of bio-availability
Prevention
Beneficial effects

THEORY
The first-pass effect is a phenomenon of drug metabolism in which the
concentration of a drug is greatly reduced before it reaches the systemic
circulation.
eg: Imipramine, Morphine , Propranolol, Diazepam, Cemitidine etc.
The indication of first-pass effect is the diminished drug concentration
or complete absence of drug in the plasma after oral administration.
The first-pass effect may leads to inactivation or activation of a drug.

SYSTEMS AFFECTING PRE-SYSTEMICMETABOLISM
The systems included are:
Digestive enzymes
Bacterial enzymes
Gut wall enzymes/mucosal enzymes
Hepatic enzymes

DIFFERENT SITES OF PRE-SYSTEMIC METABOLISM

DIGESTIVEENZYMES
• These are present in gut fluids intestinal and pancreatic secretions
• These include hydrolases which hydrolyse ester drugs like chloramphenicol palmitate to active chloramphenicol
• And peptidases which split amide linkages and inactive protein or polypeptide drugs. In order to avoid this peptide drugs are delivered to colon which lack peptidases
BACTERIALENZYMES
• Microflora are present scantily in stomach and small intestine and are rich in colon hence most orally administered drugs are unaffected by these enzymes
• Sulfasalazine is converted to sulfapyridine and 5-aminosalicylate by the microbial enzymes of colon
• Intestinal microflora hydrolyse conjugates of drugs that are actively secreted via bile and the free drugs are reabsorbed into blood eg: glucuronides of digoxin and oral contraceptives
GUT WALLENZYMES
• They are present in stomach, small intestine and colon
• Alcohol dehydrogenase enzyme which is present in stomach mucosa inactivates ethanol
• Sulphation of ethanol oestradiol and isoprenaline by intestinal enzymes
• Colonic mucosa contains both phase-l and phase-ll enzymes but only the enzymes of proximal small intestine are most active

HEPATICENZYMES
• The liver contains both phase-l and phase-ll enzymes
• This is the major site of metabolism of most orally given drugs
• Highly metabolized drugs in this are Isoprenaline, Nitroglycerin, Diltiazem, Nefidepine, Lidocaine, Morphine etc..
ESTIMATION OF BIOAVAILABILITY
Absolute bioavailability:
• For an orally administered drug that is chemically stable in the gastrointestinal tract and is 100% systemically absorbed (F = 1), the area under the plasma drug concentration curve, AUC∞
0, oral, should be the same when the same drug dose is given intravenously, AUC∞
0, IV.
• Therefore, the absolute bioavailability (F) may reveal evidence of drug being removed by the liver due to first-pass effects as follows
oraliv
ivoral
D AUC
D AUCF
Liver extraction ratio:
• There are many other reasons for a drug to have a reduced F value, the extent of first-pass effects is not very precisely measured from the F value
• The liver extraction ratio (ER) provides a direct measurement of drug removal from the liver after oral administration of a drug.
ER=(Ca-Cv)/Cv
C a is the drug concentration in the blood entering the liver C v is the drug concentration leaving the liver

Relationship b/w F and ER
• Sampling of drug from the hepatic portal vein and artery is difficult so the following relationship between bioavailability and liver extraction enables a rough estimate of the extent of liver extraction
F=1-ER-F’’
F” is the fraction of drug removed by nonhepatic process F is the fraction of bioavailable drug
• If F” is considered negligible then the equation is as follows
F=1-ER then
ER=1-F

PREVENTION:
• We can avoid first pass effect by choosing alternative routes of administration like suppositories, I.V, I.M, inhalational aerosol and sublingual
• Because they allow drug to be absorbed directly into systemic circulation
• Prevention is taken only for drugs that are destroyed by the first-pass effect

BENIFICIAL EFFECTS:
• Prodrugs like codeine(methylmorphine) are converted from inactive form to pharmacologically active form morphine
• Aspirin a prodrug which is inactive is converted to active salicylic acid by esterase's in liver
• Sulphasalzine an inactive form converted to sulphapyridine and active 5-aminosalicylate

METHODS FOR STUDYING DRUG ABSORPTION
Classification :
In silico methods
Physicochemical methods
In vitro methods
In situ methods

IN SILICO METHODS
• In silico methods predict intestinal permeability on the basis of drug characteristics or descriptors, such as lipophilicity, H-bonding capacity, molecular size, polar surface area, and quantum properties.
• One of the most famous is the Rule of five by Lipinski et al
• This approach predicts low permeability or solubility when the following cut-offs are exceeded:

l
1. There are more than five H-bond donors (expressed as the sum of OHs and NHs).
2. The molecular weight MW is over 500.
3. The log P is over 5 (P is the drug 1-octanol/water partition coefficient).
4. There are more than 10 H-bond acceptors (expressed as the sum of Ns and Os).
5. Compound classes that are substrates for biological transporters are exceptions to the rule.
• The Rule of five has the advantages of being simple, easy to interpret, and fast to compute even if, as other similar approaches [80], it does not take into account the interactions between drug properties

PHYSICOCHEMICAL METHODS
• Dressman et al. propose to incorporate various basic drug physicochemical properties into a unique parameter, the absorption potential (AP), defined by
AP=log(PFun/D0), D0=X0/CsVL
• P is the drug 1-octanol/water partition coefficient, Fun is the fraction of drug not ionized at pH 6.5, Cs is the aqueous solubility of not ionized species at 37 C, VL is the volume of water taken with the dose (it is usually set = 250 ml), X0 is the drug dose, and D0 is dose number.
IN VITRO METHODS
• In vitro techniques when compared to vivo methods they do not account for the effect of physiological factors such as gastric emptying rate, gastrointestinal transit rate, gastrointestinal pH, etc
In vitro strategies :1.Animal tissue methods :
a)Everted gut techniqueb)Intestinal sheetsc)Isolated membrane vesicles
2.cell based methods : Caco-2 cell method

EVERTED GUTTECHNIQUE

EVERTED GUT TECHNIQUE
• It is aimed to determine intestinal wall permeability on the basis of drug transport across the membrane from the donor drug solution to the receiver environment
• This technique implies fixing the intestinal tract on the left side of a ‘‘U’’ glass capillary connected to a cylindrical glass vessel. In this disposition, intestinal mucosa faces the donor environment while the serosal side faces the receiver environment.
• This model is ideal for studying the absorption mechanism of drugs since both the passive and active transport can be studied.
l
• The whole preparation is maintained at 370C and shaken
mildly.
• At predetermined time intervals the sac is removed and the concentration of drug in the serosal liquid is determined.
• The advantage of this configuration consists in a wide donor volume and a small receiver volume so that drugs accumulate faster.
• The drawbacks of this technique are the lack of active blood and nerve supply that can lead to a rapid loss of viability and tissue damage due to intestine everting.

INTESTINAL SHEETS
• Involves the isolation of the intestinal tissues, cutting it into strips of appropriate size and clamping it on a suitable device so that the donor and receiver environments are separated by a flat intestinal membrane.
• Tissue permeability is evaluated resorting to drug concentration increase in the receiver environment (that is in contact with the intestine serosal side).
• Lack of blood and nerve supply, rapid loss of tissues viability, changes in morphology and functionality represent main drawbacks of this approach.

ISOLATED MEMBRANE VESICLES
• Membrane vesicles can be prepared from either intestinal scrapings or isolated enterocytes
• They allow studying drug and nutrient transport at the cellular level (brush border as well as basolateral side), they are ideal for mechanistic absorption studies and for the isolation and identification of transporter proteins
• One of the most important advantages of vesicles over the everted gut and intestinal sheets approaches is the very small amount of drug required.

l
• In addition, the possibility of vesicles cryopreservation permits storing them for a long time.
• Conversely, it is practically impossible to isolate pure brush border membrane vesicles (or basolateral vesicles) without the contamination with the other type of vesicles.
• Vesicles isolation process often implies transporter proteins and enzymes getting damaging.

CELL BASED METHODS
• some of the most commonly used cell models we can mention Caco-2 (human/colon; epithelial), HT-29 (human/colon; epithelial), T-84 (human/colon; epithelial), MDCK (canine/kidney; epithelial), and LLC-PK1 (porcine/kidney; epithelial).
• Caco-2, is human colon adenocarcinoma undergoing spontaneous enterocytic differentiation leading to a monolayer (on a semipermeable porous filter) where cell polarity and tight junctions are well established.
• In addition, as they do not produce mucus, permeability evaluation is altered by the absence of the diffusive resistance offered by mucus
• Finally, it is worth mentioning that Caco-2 cell model accounts only for passive drug transport
IN SITU METHODS• These methods simulates the in vivo conditions for drug absorption
and are based on perfusion of a segment of GIT by drug solution and determination of amount of drug diffused through it.
• The most important advantage of in situ methods compared to the in vitro techniques consists in intact blood and nerve supply.
• Accordingly, this methodology is highly accurate for predicting the permeability of passively transported compounds, while the use of a scaling factor is recommended for predicting permeability of carrier-mediated compounds
• Classification :1)Doluisoi method2)Single pass perfusion technique
DOLUISIOMETHOD
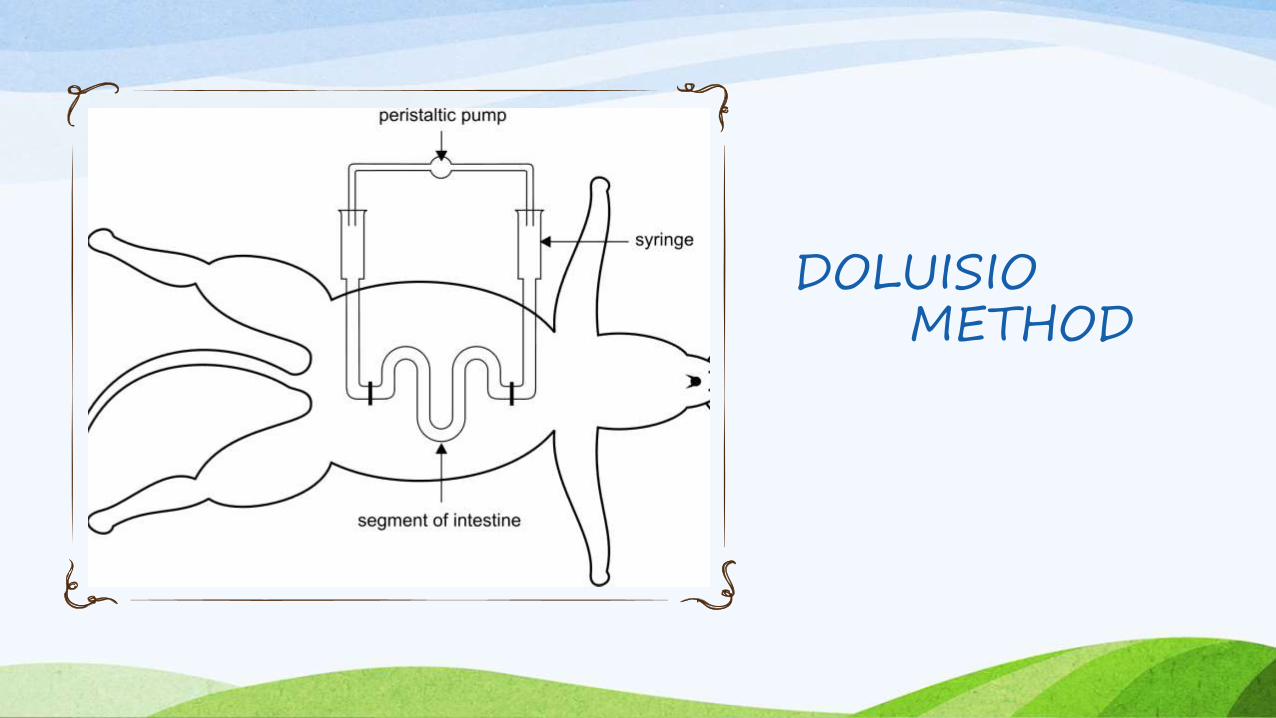
DOLUISIO METHOD
• In this method, the upper and lower parts of the small intestine of anaesthetised and dissected rat are connected by means of tubing to syringes of capacity 10 – 30 ml.
• After washing the intestinal segment with normal saline, the syringe is filled with a solution of radiolabelled drug and a non-absorbable marker which is used as an indicator of water flux during perfusion.
• Part of the content of the syringe containing drug is delivered to the intestinal segment which is then collected in the second syringe and analysed for drug.

SINGLE PASSPERFUSION
TECHNIQUE

SINGLE PASS PERFUSION TECHNIQUE
• It is generally considered superior to the Doluisio method giving better control of the hydrodynamics and increased surface area
• The drug solution is perfused continuously (via an infusion pump) down a set length of intestine through the duodenalend cannula and perfusate collected from the ileal-end cannula, at flow rates of between 0.1 and 0.3 ml/min.
• The samples collected at outflow are assayed for drug content.

L

















