Drug Addiction, 1st Brain Report Monday, 27 March 1961 00:00 MINISTRY OF HEALTH DEPARTMENT OF HEALTH FOR SCOTLAND DRUG ADDICTION Report of the Interdepartmental Committee LONDON HER MAJESTY'S STATIONERY OFFICE 1961 INTERDEPARTMENTAL COMMITTEE ON DRUG ADDICTION Minute of Appointment of the Committee I hereby appoint: Sir Russell Brain, Bart., M.A., D.M., F.R.C.P. A. Lawrence Abel, Esq., M.S., F.R.C.S. *D. M. Dunlop, Esq., M.D., F.R.C.P.Ed., F.R.C.P., F.R.S.E. Donald W. Hudson, Esq., M.P.S. A. D. Macdonald, Esq., M.Sc., M.D. A. H. Macklin, Esq., O.B.E., M.C., T.D., M.D. S. Noy Scott, Esq., M.R.C.S., L.R.C.P. M. A. Partridge, Esq., M.A., D.M., D.P.M. tobe a committee to review, in the light of more recent developments, theadvice given by the Departmental Committee on Morphine and HeroinAddiction in 1926; to consider whether any revised advice should alsocover other drugs liable to produce addiction or to be habit-forming;to consider whether there is a medical need to provide special,including institutional, treatment outside the resources alreadyavailable, for persons addicted to drugs; and to make recommendations,including proposals for any administrative measures that seemexpedient, to the Minister of Health and the Secretary of State forScotland. I hereby further appoint Sir Russell Brain to be Chairman,and Roy Goulding, Esq., M.D., B.Sc., and W. G. Honnor, Esq., I.S.O., tobe Secretaries of the Committee.DEREK WALKER-SMITH, Minister of Health. 3rd June, 1958. *Now Sir Derrick Dunlop INTERDEPARTMENTAL COMMITTEE ON DRUG ADDICTION REPORT To The Rt. Hon. J. Enoch Powell, M.B.E., M.P., Minister of Health. 1 / 14
Transcript
Drug Addiction, 1st Brain ReportMonday, 27 March 1961 00:00
MINISTRY OF HEALTH
DEPARTMENT OF HEALTH FOR SCOTLAND
DRUG ADDICTION
Report of the
Interdepartmental Committee
LONDON
HER MAJESTY'S STATIONERY OFFICE
1961
INTERDEPARTMENTAL COMMITTEE ON DRUG ADDICTION Minute of Appointment of the Committee I hereby appoint: Sir Russell Brain, Bart., M.A., D.M., F.R.C.P. A. Lawrence Abel, Esq., M.S., F.R.C.S. *D. M. Dunlop, Esq., M.D., F.R.C.P.Ed., F.R.C.P., F.R.S.E. Donald W. Hudson, Esq., M.P.S. A. D. Macdonald, Esq., M.Sc., M.D. A. H. Macklin, Esq., O.B.E., M.C., T.D., M.D. S. Noy Scott, Esq., M.R.C.S., L.R.C.P. M. A. Partridge, Esq., M.A., D.M., D.P.M. tobe a committee to review, in the light of more recent developments, theadvice given by the DepartmentalCommittee on Morphine and HeroinAddiction in 1926; to consider whether any revised advice should alsocoverother drugs liable to produce addiction or to be habit-forming;to consider whether there is a medical need toprovide special,including institutional, treatment outside the resources alreadyavailable, for persons addicted todrugs; and to make recommendations,including proposals for any administrative measures that seemexpedient, tothe Minister of Health and the Secretary of State forScotland. I hereby further appoint Sir Russell Brain to be Chairman,and Roy Goulding, Esq., M.D., B.Sc., and W. G.Honnor, Esq., I.S.O., tobe Secretaries of the Committee.DEREK WALKER-SMITH, Minister of Health. 3rd June, 1958. *Now Sir Derrick Dunlop INTERDEPARTMENTAL COMMITTEE ON DRUG ADDICTION REPORT To The Rt. Hon. J. Enoch Powell, M.B.E., M.P., Minister of Health.
1 / 14
Drug Addiction, 1st Brain ReportMonday, 27 March 1961 00:00
The Rt. Hon. John Maclay, C.M.G., M.P., Secretary of State for Scotland. Appointment 1. We were appointed on 3rd June, 1958, with the following terms of reference: "toreview, in the light of more recent developments, the advice given bythe Departmental Committee onMorphine and Heroin Addiction in 1926; toconsider whether any revised advice should also cover other drugsliableto produce addiction or to be habit-forming; to consider whetherthere is a medical need to provide special, includinginstitutional,treatment outside the resources already available, for persons addictedto drugs; and to makerecommendations, including proposals for anyadministrative measures that may seem expedient, to the MinisterofHealth and the Secretary of State for Scotland ". Procedure 2.We have held eleven meetings. We decided as a first step to seekinformation from a number of organisationsand persons having aninterest in the questions before us and at a later stage we arrangedfor publication of a pressnotice inviting anybody interested to submitrepresentations. We compiled a list of the points which we thoughtwereof importance, but we made it clear that the replies need not beconfined to these particular items. As ageneral rule we did not askfor oral evidence, though we found it an advantage in certaininstances. Appendix I givesa list of the bodies and persons consulted.The Department of Health for Scotland, the Home Office and theMinistryof Health submitted evidence to us; officers of these Departmentsattended our meetings and have given usvaluable assistance. Interim Report 3.On 23rd November, 1959, we submitted an Interim Report. This dealt withtwo questions which arose from ourterms of reference and which hadbeen brought specially to our notice. First, we were asked to examinethe risksattending the abuse of carbromal and bromvaletone andpreparations containing these substances. The PoisonsBoard had alreadyconsidered this problem but, in the absence of sufficient evidence thatthese compounds werewidely abused, had not recommended them forcontrol as "poisons" under the Pharmacy and PoisonsAct, 1933. 4. Onexamination of the evidence it became clear to us that carbromal andbromvaletone were examples of anumber of drugs on sale to the publicwhich were not appropriate for restriction to supply on prescriptionunder theDangerous Drugs Act, 1951, or the Therapeutic Substances Act,1956, and had not so far been recommended forcontrol as poisons. 5.We recommended that, in general, any drug or pharmaceutical preparationwhich has an action on the centralnervous system and is liable toproduce physical or psychological deterioration should be confined tosupply onprescription and that an independent expert body should beresponsible for advising which substances should be socontrolled. 6.As an interim and urgent measure, the Secretary of State for the HomeDepartment, on the recommendation ofthe Poisons Board, has madeRules(1) under which certain substances having an action on the centralnervoussystem are included in a new list of substances which may besold by retail only on the prescription of a dulyqualified medicalpractitioner, registered dentist, registered veterinary surgeon orregistered veterinary practitioner. 7. We are glad to note theaction that has been taken and we hope that arrangements will be madeto ensure that,as other preparations affecting the central nervoussystem become available, they too will be brought to the noticeof thePoisons Board, or such other advisory body as may in due course beappointed for the purpose, to considerwhether there are sufficientgrounds for restricting any of them also to supply on prescription. 8.The second part of our Interim Report was devoted to anaesthetists whobecome addicted to the gases andvapours which they use in the courseof their professional duties. We ascertained that the incidence ofthisirregularity was very small indeed. However, over a period of elevenyears, patients' lives had been endangeredin two known instances. 9.We were assured by our expert witnesses on this subject that, with theapparatus at present to hand, thepreliminary sniffing of the gasesimmediately before administering them to a patient was a recognisedandindispensable precaution. We accepted this. 10. In view of the heavyand direct responsibility carried by every anaesthetist we wereconvinced that anyoneaddicted to the inhalation of gases and vapoursshould never be entrusted with their administration. Interventioninthe first instance, we thought, should be by the anaesthetist'sprofessional colleagues. The ethical questionsarising have beendiscussed between Ministers and representatives of the medicalprofession and we are glad tosee that a memorandum embodying theagreed arrangements was sent to hospital authorities in England andWaleson 27th May, 1960, and that one was sent to hospital authoritiesin Scotland on 18th August, 1960.
2 / 14
Drug Addiction, 1st Brain ReportMonday, 27 March 1961 00:00
Report of the Departmental Committee on Morphine and Heroin Addiction (the "Rolleston Committee")1926 11. The main tasks of the Rolleston Committee, whose advice we were invited to review, were to advise on: (a)the circumstances, if any, in which the supply of morphine and heroin,and preparations containing thesesubstances, to persons addicted tothose drugs might be regarded as medically advisable; (b) theprecautions which medical practitioners administering or prescribingmorphine or heroin should adopt toavoid abuse and any administrativemeasures that seemed expedient to secure observance of thoseprecautions. 12. Through the system of records and inspectionthen in operation cases were brought to the notice of the HomeOfficeat that time in which exceptionally large quantities of morphine andheroin had been supplied to particularpractitioners or prescribed forindividual cases. On further enquiry it was ascertained that sometimesthe doctor hadordered these drugs simply to satisfy the craving of theaddict; in some instances there was a doubt whether thesupply was forbona fide medical treatment; in other cases the drugs had beenprescribed in large quantities eitherto persons previously unknown tothe practitioner or to a patient receiving supplies elsewhere;occasionally, largesupplies had been used by practitioners forself-administration. 13. It appeared then that in somecircumstances dangerous drugs were being supplied in contravention oftheintention of Parliament that a doctor should be authorised tosupply drugs only so far as was necessary for thepractice of hisprofession. Before deciding on measures to secure proper observance ofthe law, it was feltnecessary to have some authoritative medicaladvice on various aspects of the treatment of addiction, the useofdangerous drugs in medical treatment, and the action which might betaken where a doctor appeared to havemisused his authority to possessand supply them. 14. The Rolleston Committee's recommendationsin 1926 on the supply of morphine and heroin to addicts to thesedrugsand on the use of drugs in treatment are discussed later in thisReport. They have, up to now, been includedin the Memorandum on theDangerous Drugs Act and Regulations which is prepared by the HomeOffice for theinformation of doctors and dentists. 15. As aresult of the Rolleston Committee's proposals for administrativemeasures, amendments were made to theDangerous Drugs Regulations in1926 to the following effect : (i)Provision was made for theconstitution of a tribunal to which the Secretary of State could refercases in which, inhis opinion, there was reason to think that a dulyqualified practitioner might be supplying, administering orprescribingdrugs either for himself or other persons otherwise than as requiredfor purposes of medical treatment. (ii) The Secretary of State wasempowered, on the recommendation of a tribunal, to withdraw a doctor'sauthority topossess and supply dangerous drugs and to direct that sucha doctor, or a doctor convicted of an offence under theAct, should notissue prescriptions for dangerous drugs. (iii) It was made clearthat prescriptions should only be given by a duly qualified medicalpractitioner when requiredfor purposes of medical treatment. (iv)It was made an offence for a person who was receiving treatment fromone doctor to obtain a supply ofdangerous drugs from a second doctorwithout disclosing that he was being supplied by the first doctor. (v) All doctors, dentists and veterinary surgeons were required to keep appropriate records of all dangerous drugsobtained. Withthe exception of the provisions relating to tribunals, which we discusslater, all these amendments remain in thecurrent regulations. The changed situation 16.In the thirty-four years since the Rolleston Committee reported therehave been developments in two directionswhich are of interest to ourown Committee. On the one hand pharmaceutical research has produced anumber ofnew analgesic drugs, many of which are capable of producingaddiction. Some of these have been derived fromopium and others havebeen produced synthetically. It is possible that many moreaddiction-producing drugs will beproduced. A potent analgesic which isnot addiction-producing has so far not been forthcoming. We have had
3 / 14
Drug Addiction, 1st Brain ReportMonday, 27 March 1961 00:00
todirect our attention to the question whether these drugs should be usedwith the same precautions and subjectedto the same control as themorphine and heroin considered by the Rolleston Committee. 17.The second development has been in the methods of treatment of drugaddiction. The withdrawal from addictsof the drug to which they areaddicted has been the subject of experiment in several countries andparticularly in theUnited States of America. These experiments haveincluded the substitution of newer addiction-producing drugsand theirsubsequent gradual withdrawal, and also the use of other new drugs,such as tranquillizers, for thealleviation of the withdrawal symptoms.It has therefore been necessary to consider whether there arestillcircumstances in which the continued administration of dangerous drugs,even under the conditions strictlydefined by the RollestonCommittee(2), can be justified. 18. We therefore had to consider: (i) whether any new advice could be brought effectively to the notice of doctors and dentists; (ii) whether the principles underlying the advice could be emphasised clearly to avoid misinterpretation; (iii) whether any action was necessary to prevent the unjustifiable prescribing of dangerous drugs by somedoctors; (iv)whether there was any way of preventing the unjustified use ofdangerous drugs by any doctor for himself orfor members of his family ; (v)the suggestion made in certain international organizations thatGovernments might set up special institutionsfor the treatment, careand rehabilitation of addicts on a compulsory basis. 19. In additionthere has been an increase in the use by doctors and by the generalpublic of drugs liable to causehabituation. Because they do not giverise to ill-effects substantially the same as, or analogous to, thoseproducedby morphine or cocaine they are not within the scope ofinternational agreements. We have considered thisdevelopment. Definitions adopted 20.From the outset we felt it necessary to have a clear and consistentidea of the phenomena confronting us. Wetherefore adopted thefollowing definitions, realising that they are somewhat arbitrary andmay need to be revised inthe light of increasing knowledge. Drug Addictionis a state of periodic or chronic intoxication produced by the repeatedconsumption of a drug(natural or synthetic); its characteristicsinclude: (1) an overpowering desire or need (compulsion) to continue taking the drug and to obtain it by any means, (2) a tendency to increase the dose, though some patients may remain indefinitely on a stationary dose, (3) a psychological and physical dependence on the effects of the drug, (4) the appearance of a characteristic abstinence syndrome in a subject from whom the drug is withdrawn, (5) an effect detrimental to the individual and to society. Drug Habituation (habit) is a condition resulting from the repeated consumption of a drug. Its characteristicsinclude: (1) a desire (but not a compulsion) to continue taking the drug for the sense of improved well-being which itengenders, (2) little or no tendency to increase the dose, (3)some degree of psychological dependence on the effect of the drug, butabsence of physical dependence andhence of an abstinence syndrome, (4) detrimental effects, if any, primarily on the individual. Sedative.A drug which depresses the central nervous system, especially at higherlevels, so as to allaynervousness, anxiety, fear and excitement, butnot normally to the extent of inducing sleep. Hypnotic(or soporific). A drug used to induce sleep, which does so bydepression of the central nervous system,more profoundly than asedative but with a restricted duration of effect. Tranquillizer(or Ataractic). A drug which promotes a sense of calmness andwell-being without that degree ofdepression of the central nervoussystem commonly associated with the action of sedatives or hypnotics. Stimulant.A drug which, by its action on the central nervous system, temporarilyenhances wakefulness andalertness, improves mood and lessens the senseof fatigue. 21. In terms of physiology and pharmacology anarcotic is any agent which brings about a reversible depressionofcellular metabolism and activity in the central nervous system.Substances included in any of the groups
4 / 14
Drug Addiction, 1st Brain ReportMonday, 27 March 1961 00:00
mentioned above, with theexception of the stimulants, may therefore be regarded as narcotics. 22.In more common parlance and in the proceedings of internationalagencies and control organisations the word"narcotic" is often limitedto drugs like opium, morphine, heroin, pethidine, cocaine, etc., whicharesubject to measures of international control. 23. Alcoholwas excluded from our considerations for the purpose of this report. Weregard addiction to it as aserious problem which needs separateattention. Extent of the problem in Great Britain 24.After careful examination of all the data put before us we are of theopinion that in Great Britain the incidenceof addiction to dangerousdrugs—which today comprise not only morphine and heroin but also suchothersubstances coming within the provisions of the Dangerous DrugsAct, 1951, as pethidine, methadone, levorphanol,etc.—is still verysmall. The figures provided by the Home Office (see Appendix II) whichmight suggest an extensionof addiction in Great Britain reflect, wethink, an intensified activity for its detection and recognition overthe post warperiod. At the same time the choice of drugs has altered,the new synthetics taken orally being now more popular.There isnevertheless in our opinion no cause to fear that any real increase isat present occurring. The number ofdoctors and nurses involved—theso-called "professional addicts"—though small in total,remainsdisproportionately high. 25. According to the Home Office and thepolice, supported by such independent evidence as we have been abletoobtain, the purveying of illicit supplies of manufactured dangerousdrugs for addicts in this country is so small asto be almostnegligible. The cause for this seems to lie largely in social attitudesto the observance of the law ingeneral and to the taking of dangerousdrugs in particular, coupled with the systematic enforcement oftheDangerous Drugs Act, 1951 and its Regulations. 26. We wouldemphasise that there is, in Great Britain, no system of registration ofaddicts, nor any scheme bywhich the authorities allocate to themregular supplies of the drugs they are taking. We are, however,satisfied thatthe arrangements for recording manufacture and supply,and for inspection, continue to ensure that nearly alladdicts ateknown to the Home Office, to the Ministry of Health and to theDepartment of Health for Scotland. Treatment 27.Like the Rolleston Committee, we believe that addiction should beregarded as an expression of mentaldisorder rather than a form ofcriminal behaviour. 28. We believe that every addict should betreated energetically as a medical and psychiatric problem.Theevidence presented to us indicates that the satisfactory management ofthese cases is not possible except insuitable institutions. We are notconvinced that compulsory committal to such institutions is desirable.Good resultsare more likely to be obtained with co-operative ratherthan with coerced patients. At a time when the compulsorytreatment ofthe mentally sick is being steadily diminished we see no grounds forseeking new powers of compulsionfor the treatment of drug addicts. 29.Judging by the expert advice offered to us we can see no advantage inabrupt withdrawal. Sudden andcomplete denial of the drug to the addictis a distressing and occasionally dangerous experience which it is bestnotto provoke. We do not think that we need draw up a plan oftreatment, still less would we suggest that there is anideal regimenwhich should be generally adopted. Yet, as this is a subject on whichonly a few doctors in GreatBritain have any great personal experience,we have set out, in Appendix III, some notes that may serve as aguide. Provision of institutions 30.Because the overall problem is so small it is doubtful whether there isscope for establishing specialisedinstitutions in Great Britainexclusively for the treatment of drug addiction. We realise that atcentres of this kind bothmedical and nursing staff would have anopportunity for training and research in the management of addicts,butvery few patients would qualify for admission at any one time. 31.The best unit for the initial treatment of the established addict is,we consider, the psychiatric ward of a generalhospital. Long-term supervision and rehabilitation 32.Whereas withdrawal of the drug may be a fairly simple undertaking,long-term management, adequate
5 / 14
Drug Addiction, 1st Brain ReportMonday, 27 March 1961 00:00
rehabilitation and permanent curepresent greater difficulties. Selected centres might undertake thislong-termsupervision and, at one or more of these, facilities forresearch might be provided, possibly by the MedicalResearch Council. 33.There remains the stage at which the addict returns to everyday lifeand consequently to the stresses which areliable to provoke a relapse.Social services are then required to offer all the help they can.Before the patient leaveshospital the general practitioner and,whenever appropriate, the local health authority as well, should beconsultedabout the provision of continued guidance and support. Werecommend, too, that in every case the generalpractitioner should benotified immediately the patient leaves the hospital. Prognosis 34.Information about the ultimate prognosis for drug addicts is extremelyscanty and, so far as we can ascertain,the long-term results havehitherto been disappointing. This may reflect boththe intractability of the condition and the inadequacy of thetreatment. Prevention, obviously, is to be preferred to cure and thisleads us to acknowledgethe prevailing healthy attitude of the publicto this problem and the efficacy of the measures in Great Britainwhichkeep the incidence of drug addiction to such small dimensions. Administration of drugs to persons already addicted 35.The Rolleston Committee defined "circumstances in which morphine orheroin may be legitimatelyadministered to addicts". These included"Persons for whom, after every effort has been made for thecure ofaddiction, the drug cannot be completely withdrawn, either because: (i)Complete withdrawal produces serious symptoms which cannot besatisfactorily treated under the ordinaryconditions of private(3)practice; or (ii) The patient, while capable of leading a useful andfairly normal life so long as he takes a certainnon-progressivequantity, usually small, of the drug of addiction, ceases to be able todo so when the regularallowance is withdrawn". On the first ofthese points we have already stated (paragraph 28) that we believe onlyinstitutional treatment islikely to be satisfactory. With the secondof these points we entirely agree, though the expression`regularallowance' has led to unfortunate and persistent misunderstanding. Ithas been taken in error to mean thataddicts in Great Britain areentitled to receive supplies of dangerous drugs on prescription andthat this involves theregistration of the addict with some centralauthority. We think that the Rolleston Committee never meanttoencourage a system of registration and from the evidence we havereceived it is clear that the Home Office havenever acted in thatbelief and have never put such a system into force. The continuedprovision of supplies topatient addicts depends solely on theindividual decision made by the medical practitioner professionallyresponsiblefor each case. We are strongly opposed to any suggestionthat "registration" would be either desirableor helpful. 36.Arising also out of sub-paragraph (ii) quoted above is the conceptionof a "stabilised addict". Theauthenticity of this has been widelyquestioned. Many of those authorities and experienced persons whogaveevidence to us nevertheless agree that this type of patient does exist.Moreover, a careful scrutiny of thehistories of more than a hundredpersons classsified as addicts reveals that many of them who have beentakingsmall and regular doses for years show little evidence oftolerance and are often leading reasonably satisfactorylives. (SeeAppendix IV). Consequently we see no reason to reject the idea of a"stabilised addict".Indeed, to group together all "drug addicts" onthe basis of a pharmacological definition may convey anover-simplifiedand misleading impression. There are drug addicts who have beenintroduced to the practice whenphysically healthy with drugs procuredby illicit means or in the course of their professional work. Thisgroup is avery small one in Great Britain. There are those who, havingbeen given a drug of addiction as the appropriatetreatment for apainful illness, continue to be dependent on it when the originalnecessity for its use hasdisappeared. And there is a third group ofthose who are unable to abandon a drug rightly or wrongly prescribedforsome physical or mental ailment which itself persists. Opinions maywell differ as to whether those in the last groupshould be regarded asaddicts, except in a technical sense, and where the line should bedrawn between addictionto a drug and its appropriate medical use.Furthermore, we are impressed that the right of doctors in GreatBritain tocontinue at their own professional discretion the provisionof dangerous drugs to known addicts has not contributedto any increasein the total number of patients receiving regular supplies in this way. Unjustifiable prescribing 37.Despite the generally satisfactory state of affairs we have beeninformed that from time to time there have been
6 / 14
Drug Addiction, 1st Brain ReportMonday, 27 March 1961 00:00
doctors who wereprepared to issue prescriptions to addicts without providing adequatemedical supervision,without making any determined effort at withdrawaland, notably, without seeking another medical opinion. Suchactioncannot be too strongly condemned. Only two such habitual offendersduring the past twenty years have beenbrought to our notice and it issatisfactory to note that, in spite of widespread enquiry, no doctor isknown to befollowing this practice at present. Professional addicts 38.Among the known addicts are doctors who obtain and administer dangerousdrugs to themselves. They takeadvantage of their privileged positionto maintain their own addiction. Our enquiries reveal that only a fewdoctors inGreat Britain are at present involved. Small though theirnumbers may be they present special problems. Disciplinary measures 39.Under the Dangerous Drugs Regulations, 1953, as at present in force,the Home Secretary may withdraw froma doctor the authority which theRegulations give to all doctors to possess and supply dangerous drugs,if thatdoctor has been convicted of an offence against the DangerousDrugs Act, 1951, or of certain Customs offences inrespect of dangerousdrugs and if the Home Secretary is of the opinion that that doctor maynot properly be allowedto possess and supply them; he may also direct,if he withdraws the authority, that it shall not be lawful forthatdoctor to give a prescription for a dangerous drug. 40. A doctor whoappears to be prescribing excessively for a particular patient mayclaim that he is doing so foradequate medical reasons. Withoutinterfering with his professional freedom it would be difficult tocontest such anassertion. 41. A doctor who decides that medicallyhe requires the regular administration of dangerous drugs maylawfullyobtain them for his own use by giving a prescription for that purpose,but he thereby attracts the attention ofthe authorities. Whether suchself-administration or excessive prescribing, or the disorders ofprofessional conductto which it may lead constitutes infamous conductin a professional respect is, in our opinion, a matter for theGeneralMedical Council. 42. In 1926 the Rolleston Committee recommendedthat a tribunal should be established to investigate anddecidewhether, in particular cases, there were sufficient medical grounds forthe administration of dangerous drugsby the doctor concerned either toa patient or himself. If a tribunal were to find to the contrary itwould be able toadvise the Home Secretary accordingly, and he wouldhave power to withdraw the doctor's authority to possess andsupplydangerous drugs without a previous conviction in the Courts. Althoughprovision for these tribunals was madein the Dangerous DrugsRegulations, 1926, they never came into being, and when the newRegulations werepromulgated in 1953 under the consolidated DangerousDrugs Act of 1951, this provision was deferred pendingcompletion ofthe negotiations which were then proceeding with the professionalorganisations. 43. The need for these tribunals has been urged uponus by some of our witnesses. We have been told that theyhave worked toadvantage in Northern Ireland, but that they have now been discontinuedin that country. 44. We are impressed by the difficulties ofestablishing a special tribunal for this purpose. There would be aneedfor powers to take evidence on oath, witnesses who are themselvesaddicts are notoriously unreliable and itmight prove extremely hard toassess "sufficient medical grounds" in the face, possibly, ofopposingmedical opinions. Accordingly, after the most careful examination ofthis proposal, we have concluded thatsuch special tribunals should notbe set up in this country. 45. In general, we think that theinfrequency of these irregularities fails to justify the introductionof further statutorypowers to correct them. We strongly recommend,however, that every doctor should obtain a second medicalopinion inwriting before embarking on the regular prescribing of a dangerousdrug, either to a patient, to a relativeor to himself, for a lengthyperiod, say, in excess of three months. This would not interfere withthe management ofchronic cases, for example of inoperable carcinoma,as it must be very exceptional for such patients not to be seenby aconsultant at some stage. To have, moreover, the support of anotherpractitioner when dealing with an addictwould, we feel, be welcomedrather than resented by the vast majority of doctors. 46. Further,we support the advice of the British Medical Association that a generalpractitioner should prescribeonly a limited supply of a dangerous drugto a patient temporarily under his care in the absence of a letter fromthepatient's own doctor. Distinctive prescription forms for Dangerous Drugs 47.We found little support for the suggestion that specially coloured orotherwise distinctive forms should beintroduced for prescribingdangerous drugs. We see no advantage in this device, because in thiscountry the problem
7 / 14
Drug Addiction, 1st Brain ReportMonday, 27 March 1961 00:00
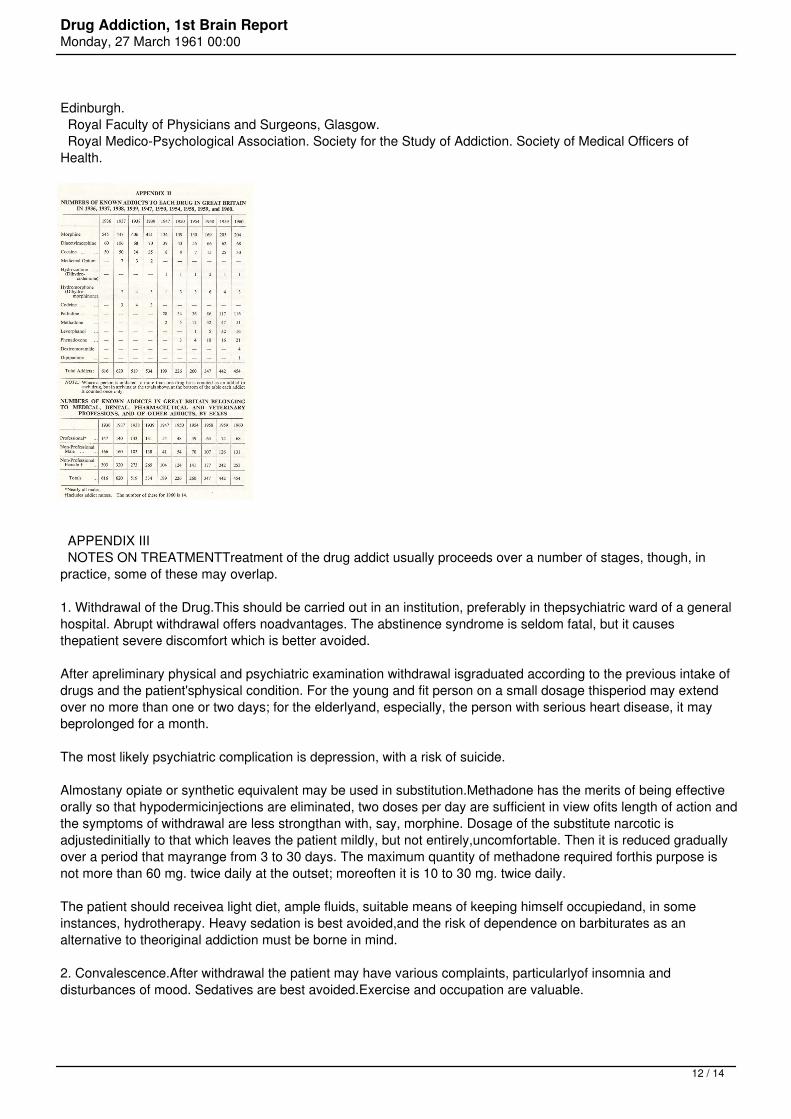
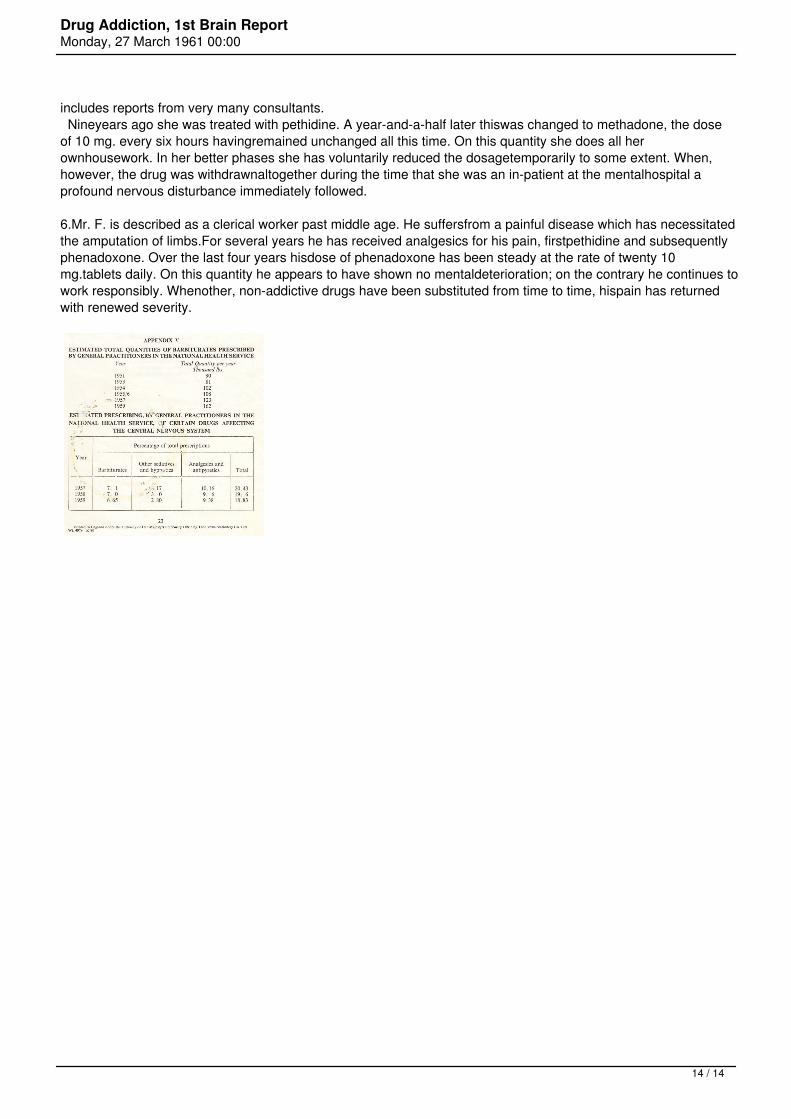
of addiction is a small one, our present system ofcontrol works very efficiently and the additional work involved,bothfor doctors and for the Government, in the use and checking of specialprescription forms, could not bejustified. Moreover the use of suchspecial forms might disclose to a patient that he was receivingdangerous drugsand it might be better for him not to know this. Student instruction 48.In general we have come to the conclusion that students, during theirundergraduate training, are adequatelytaught in most medical schoolsabout the pharmacology and therapeutics of dangerous drugs and therisks ofaddiction to them, though the level of teaching variesconsiderably from one school to another. The note onaddiction andhabit-forming drugs which appears in the British National Formulary,1960, is quite informative, but itsscope could usefully be extended. 49.While not forgetting the need for medical students to be warned aboutthe possibilities of addiction arising fromthe prescribing ofdangerous drugs for medical reasons we are also aware thatover-emphasis of this risk maysometimes lead to the withholding ofpowerful analgesics where the doctor's paramount duty is to relievepain, andthe possibility of addiction is virtually of no importance,e.g. in carcinoma. Advice to the medical profession 50.The Home Office Memorandum(4) is accepted as fully comprehensive but itis thought that the essentialfeatures could be presented in a morereadable form. It should be distributed, moreover, to all doctors inpracticeand not limited to general practitioners in the NationalHealth Service. Other drugs, beside morphine and heroin, likely to cause addiction 51.In 1926 the Rolleston Committee addressed itself solely to morphine andheroin. Today there is a whole rangeof analgesic drugs which may leadto addiction. These are readily brought within the purview of theDangerousDrugs Act, 1951, and its Regulations and the arrangements bywhich this legislation is amended from time to time inaccordance withInternational Conventions give rise to no difficulty. Moreover, thepharmaceutical organisationshandling such drugs in this countryco-operate so fully with the Home Office that there is at present noneed forfurther statutory powers in this connection. The situation,however, should be kept under constant review. 52. There is somefeeling that new potent analgesics should not be advertised or marketedto the medicalprofession until they have been subjected to anofficially sponsored clinical trial and granted formal approval bysomecentral authority. This proposal has received by no means universalsupport and we are not persuaded that itwould be workable or whollyadvantageous. We nevertheless think that no drug likely to be addictiveshould bereleased by the manufacturers until they have made sure thatit has been carefully tested for this possibility. 53. So far as wecan see at the moment all potent analgesics are likely to be addictive,whether they beold-established like morphine and heroin or new onesderived synthetically. Administratively they require the samecontroland medically they have the same indications and demand similarprecautions in use to those outlined by theRolleston Committee formorphine and heroin. Cannabis 54.In our view cannabis is not a drug of addiction: it is an intoxicant.Nevertheless it comes within the scope of theDangerous Drugs Act,1951. But having virtually no place in therapeutics it is obtainedalmost solely through illicitchannels and there has been some rise inthe annual amount seized by the Customs authorities. We havenotreceived evidence that its use constitutes a medical problem. Even ifits social consequences should give rise toconcern, which we wouldshare with the authorities who are responsible for the suppression oftraffic in this drug, wesee no indication for further administrativemeasures within our own terms of reference. Habit-forming drugs 55.Over recent years an intensive interest has developed, bothexperimentally and clinically, in drugs affecting thecentral nervoussystem. These include sedatives, hypnotics, tranquillizers andstimulants. The impression has beenformed that medically they are nowused on a very large scale. 56. Most of our witnesses affirmed that,today, drugs acting on the central nervous system are beingusedexcessively, but they were unable to furnish records in support of thiscontention. We have thereforeendeavoured to obtain some evidence. Froma sample of the prescriptions issued under the National HealthServicewe have been provided with an estimate of the total quantity ofbarbiturates prescribed annually in Englandand Wales over the past fewyears (Appendix V). It is obvious that usage has expanded bothprogressively andsubstantially so that in 1959 it was almost twicewhat it was in 1951. Total production figures, though they of
8 / 14
Drug Addiction, 1st Brain ReportMonday, 27 March 1961 00:00
courseinclude exports as well, confirm this trend. Secondly, by an analysisof National Health Service prescriptionsaccording to therapeuticclassification it can be seen that barbiturates, other sedatives andhypnotics, together withanalgesics and antipyretics (excludingdangerous drugs) account for no less than about nineteen per cent ofall theprescriptions issued (Appendix V). 57. For thetranquillizers we have no corresponding figures. There is reason tobelieve, however, that theirprescription has also increased. Certainlythe amount spent on one particular tranquillizer by nine selectedmentalhospitals has increased about ten-fold over a course of fiveyears. The scale of use of tranquillizers in generalpractice we havenot been able to ascertain. One reason for this has been that as suchdrugs are not readily subjectto therapeutic classification theirhandling in a sample analysis is difficult. 58. Less still have weany definite information about the volume of purchases withoutprescription. We believe,however, that the action which followed ourInterim Report will have reduced this self-medication, at least so farasthe more potent drugs acting on the central nervous system areconcerned. 59. The abuse of stimulant drugs such as the amphetaminesand phenmetrazine has led to some publicity andconcern. We know thatcases of habituation and addiction occur. Although at least forty-eightcases of amphetamineaddiction and a few of phenmetrazine addictionhave been reported in the medical literature because of theirhavingpresented with severe (though transient) mental disorder, there are nofigures available to indicate the actualextent to which suchhabituation or addiction may occur, with or without overt mentalsymptoms. 60. An analysis of some 214,000,000 National HealthService prescriptions in 1959 indicated that some5,600,000, orapproximately 21 per cent, were for preparations of the amphetaminesand phenmetrazine. Since theindications for the use of thesesubstances are not clear cut, it may be that such prescribing isexcessive, thoughhardly to an extent that could give rise to concern.We have formed the impression that, while serious cases ofaddictionarise from time to time, such abuse is not widespread. Precautions havealready been taken to preventthose intent on abuse from having accesswithout prescription to preparations of the amphetaminesandphenmetrazine and to what was formerly a ready source of supply, namelythe inhalers containing paperimpregnated with amphetamine inconcentrated form. 61. It is clear that there is scope and a needfor operational research into the prescribing pattern in thiscountry,with particular reference to habit-forming drugs. The results of such astudy could be enlightening to thepublic. 62. To explain this trendin medication directed at the central nervous system we have found nosingle answer. Inpart it must be due to the vigorous advertising ofthese drugs and their preparations by the pharmaceutical industry,bothto the medical profession and to the public. To some extent theaccelerated tempo and heightened anxieties ofmodern life have beenheld to blame, but this is an assertion based on assumption more thanfact. Thirdly, andpossibly of considerable consequence, there is thematerialistic attitude adopted nowadays to therapeutics ingeneral Thisis one feature of an age which owes so much to science. For everydeviation from health, great orsmall, a specific, chemical correctiveis sought and, if possible, applied, and it is also widely believedthat health maybe positively enhanced by the use of drugs. Whendealing with mental disease psychotherapy may still be invoked.Often,however, a prescription is given for a drug when the patient's realneed is a discussion of his psychologicaldifficulties with the doctor.An obvious danger arises when the drugs so employed, far from beingplacebos, areundeniably potent, frequently toxic and sometimeshabit-forming as well. On the other hand the newer drugs areproving ofgreat value in psychiatry where they are to some extent replacing othermethods of treatment. 63. This increasing use of sedatives,stimulants and tranquillizers raises issues upon which we do not asaCommittee feel competent to pronounce. In particular, it is not for usto decide whether their occasional or evenregular use is justified ifit enables a person to lead a happier and more useful life. In anycase, if recourse topotentially habit-forming drugs is sometimes to beregarded as a symptom of psychological maladjustment, it shouldbetreated as a symptom, and its cause sought, perhaps as much in socialconditions as in the mind of theindividual. These are questions whichshould be considered not only by doctors, but by all concerned withsocialwelfare. 64. The argument has been advanced that theavailability of these drugs to so many people nowadays leads totheirfrequent use for suicide. Over recent years, certainly, thebarbiturates have figured more prominently in thisconnection. At thesame time the total suicide rate has remained almost unchanged. Itlooks, therefore, as thoughsuicide itself has not become more popular,even if the means of achieving it have altered, and it must be bornein.mind that the therapeutic use of barbiturates and tranquillizersmay well have saved many people from suicide. 65. The management ofmental disorder generally has also been brought to our notice. Thepattern seems to havechanged considerably over recent years. Communitycare is taking the place of institutional confinement. Morepatientscan be treated at home and many of them enabled to take an active anduseful part in life. If the prescribing
9 / 14
Drug Addiction, 1st Brain ReportMonday, 27 March 1961 00:00
of even habit-forming drugs hascontributed to this state of affairs it is to be condoned rather thancondemned 66. We think that the position may require carefulwatching as time goes on but, at the moment, we see nogrounds forsuggesting further statutory control over habit-forming drugs, otherthan that recommended in our InterimReport. Summary of conclusions and recommendations 67. The following is a summary of our conclusions and recommendations. (1)In Great Britain the incidence of addiction to drugs controlled underthe Dangerous Drugs Act, 1951, is still verysmall and traffic inillicit supplies is almost negligible, cannabis excepted. This ismainly due to the attitude of thepublic and to the systematicenforcement of the Dangerous Drugs legislation. (Paragraphs 24, 25 and54). (2) While there is no registration of addicts, nor any officialallocation of drugs to them on that basis, theDepartmentalarrangements ensure that nearly all addicts to dangerous drugs areknown. (Paragraph 26). (3) Addiction should be regarded as an expression of mental disorder, rather than a form of criminal behaviour.(Paragraph 27). (4)Satisfactory treatment of addiction is possible only in suitableinstitutions, but compulsory committal of anaddict to such aninstitution is not desirable. (Paragraph 28). (5)There is noadvantage in abrupt withdrawal of a drug from a patient. Notes ontreatment are given as a guide.(Paragraph 29 and Appendix III). (6)As the problem is small, the establishment of specialised institutionsexclusively for the treatment of drugaddiction is not practicable.Initial treatment of an established addict is best undertaken in thepsychiatric ward of ageneral hospital. (Paragraphs 30 and 31). (7)Longterm supervision would best be undertaken at selected centres, at whichfacilities for research might beprovided. (Paragraph 32). (8) Continued support and guidance should be available locally when a patient leaves hospital. (Paragraph. 33). (9) Longterm results of treatment of addiction appear to be disappointing, butthe information available is limited.(Paragraph 34). (10) A system of registration of addicts would not be desirable or helpful. (Paragraph 35). (11)It is doubtful whether a person who is unable to abandon a drugoriginally prescribed for a condition which stillpersists should bedescribed as an addict. It is accepted that such a person may be ableto lead a reasonablysatisfactory life on a small and regular dose of anarcotic drug but may be unable to do so if it be withdrawn.(Paragraph36). (12) The Home Secretary should not establish medical tribunalsto investigate the grounds for recommending himto withdraw a doctor'sauthority to possess and supply dangerous drugs. (Paragraph 44). (13)Irregularities in prescribing of dangerous drugs are infrequent andwould not justify further statutory controls.(Paragraph 45). (14) Adoctor should obtain a second medical opinion before deciding toprescribe a dangerous drug for a lengthyperiod; and should give only alimited supply of a dangerous drug to a patient temporarily under hiscare in theabsence of a letter from the patient's own doctor.(Paragraphs 45 and 46). (15) No advantage would arise from the use of distinctive prescription forms for dangerous drugs. (Paragraph47). (16)Student instruction on dangerous drugs is generally adequate; butover-emphasis on the dangers of addictionmay discourage the use ofsuch drugs in cases where their need is paramount. (Paragraph 49). (17)The essential features of the Home Office Memorandum on Dangerous Drugscould be presented in a morereadable form. It should be sent to alldoctors in practice. (Paragraph 50). (18) Further statutory powersto control new analgesic drugs are not needed at present. There isinsufficientjustification for withholding them from distribution untilthey have been approved by some central authority, but anydrug likelyto be addictive should be tested for this possibility at the instanceof the manufacturers before release.(Paragraphs 51 and 52). (19)Cannabis has practically no therapeutic use and its control is not amedical matter within the Committee'sterms of reference. (Paragraph54). (20) There has been a substantial increase in the use of drugsaffecting the central nervous system, which arepotentially habitforming. While the position requires careful watching, no furtherstatutory control, beyond thatrecommended in our Interim Report, isneeded at present. (Paragraphs 55-66). 8. We wish to record ourdebt to our Secretariat and others who have attended our meetings. OurSecretaries, Mr.
10 / 14
Drug Addiction, 1st Brain ReportMonday, 27 March 1961 00:00
W. G. Honnor and Dr. Roy Goulding have done invaluablework in preparing the material for our discussions anddrafting ourreport. Mrs. J. Hauff, and later Mr. H. N. Roffey, of the Ministry ofHealth have also given us muchassistance, and we are grateful to Dr.J. M. Johnston, of the Department of Health for Scotland, for giving usthebenefit of his special knowledge of drug addiction. Mr. T. C. Greenand later Mr. S. H. E. Burley, and Mr. A. L.Dyke, of the Home Office,have been a great help to us in dealing with the administrative aspectsof the question. (1) The Poisons Rules 1960 (S.I. 1960, No. 699). (2) See paragraph 35 (3) In this context " private practice" may be read as " general practice." (4) See Paragraph 14 of this Report. (Signed) W. RUSSELL BRAIN A. LAWRENCE ABEL D. M. DUNLOP DONALD W. HUDSON A. D. MACDONALD A. H. MACKLIN S. NOY SCOTT MAURICE PARTRIDGE ROY GOULDING - W. G. HONNOR Joint Secretaries 29th November, 1960 APPENDIX I ALPHABETICAL LIST OF WITNESSESAssociation of Anaesthetists of Great Britain and Ireland. Association of British Pharmaceutical Industry. Association for the Study of Medical Education. A. A. Baker, Esq.,M.D., D.P.M. J. C. Batt, Esq., M.D., D.P.M. C. C. Beresford, Esq., M.B., D.P.M. British Dental Association. British Medical Association. British Pharmacological Society British Psychological Society. Central Midwives Board. College of General Practitioners. Faculty of Anaesthetists, Royal College of Surgeons of England. General Medical Council. General Nursing Council. Guild of Public Pharmacists. Harris Isbell, Esq., M.D. Denis Leigh, Esq., M.D., F.R.C.P. Roderick Macdonald, Esq., M.B., D.P.M. Medical Defence Union, Ltd. Medical and Dental Defence Union of Scotland, Ltd. Medico-Legal Society. Medical Protection Society, Ltd. T. M. Moylett, Esq., M.B., D.P.M. National Pharmaceutical Union. Dennis Parr, Esq., M.D., D.P.M. Pharmaceutical Society of Great Britain. Prison Commission. Proprietary Association of Great Britain. Regional Hospital Boards and Boards of Governors of Teaching Hospitals in England and Wales, and Scotland. Royal College of Midwives. Royal College of Nursing. Royal College of Physicians. Royal College of Physicians of Edinburgh. Royal College of Surgeons of England. Royal College of Surgeons,
11 / 14
Drug Addiction, 1st Brain ReportMonday, 27 March 1961 00:00
Edinburgh. Royal Faculty of Physicians and Surgeons, Glasgow. Royal Medico-Psychological Association. Society for the Study of Addiction. Society of Medical Officers ofHealth.
APPENDIX III NOTES ON TREATMENTTreatment of the drug addict usually proceeds over a number of stages, though, inpractice, some of these may overlap. 1. Withdrawal of the Drug.This should be carried out in an institution, preferably in thepsychiatric ward of a generalhospital. Abrupt withdrawal offers noadvantages. The abstinence syndrome is seldom fatal, but it causesthepatient severe discomfort which is better avoided. After apreliminary physical and psychiatric examination withdrawal isgraduated according to the previous intake ofdrugs and the patient'sphysical condition. For the young and fit person on a small dosage thisperiod may extendover no more than one or two days; for the elderlyand, especially, the person with serious heart disease, it maybeprolonged for a month. The most likely psychiatric complication is depression, with a risk of suicide. Almostany opiate or synthetic equivalent may be used in substitution.Methadone has the merits of being effectiveorally so that hypodermicinjections are eliminated, two doses per day are sufficient in view ofits length of action andthe symptoms of withdrawal are less strongthan with, say, morphine. Dosage of the substitute narcotic isadjustedinitially to that which leaves the patient mildly, but not entirely,uncomfortable. Then it is reduced graduallyover a period that mayrange from 3 to 30 days. The maximum quantity of methadone required forthis purpose isnot more than 60 mg. twice daily at the outset; moreoften it is 10 to 30 mg. twice daily. The patient should receivea light diet, ample fluids, suitable means of keeping himself occupiedand, in someinstances, hydrotherapy. Heavy sedation is best avoided,and the risk of dependence on barbiturates as analternative to theoriginal addiction must be borne in mind. 2. Convalescence.After withdrawal the patient may have various complaints, particularlyof insomnia anddisturbances of mood. Sedatives are best avoided.Exercise and occupation are valuable.
12 / 14
Drug Addiction, 1st Brain ReportMonday, 27 March 1961 00:00
3. Physical Rehabilitation.Any physical disease from which the patient is suffering should betreated from thebeginning. Chronic causes of pain should be eliminatedif at all possible, surgical measures being taken whereindicated. 4. Psychotherapy. Supportive psychotherapy is essential. It may be conducted as a group procedure. 5. Occupational Therapy. As far as possible this should take the form of useful work with increasing responsibilityand need for application. 6. Recreational Therapy.Library services, cinema, games and television should be provided tokeep the patientconstantly interested and his mind exercised. 7. Length of Treatment.No arbitrary figure can be set for this, which depends on theindividual patient's personalityand character, the length and severityof his addiction, and the possible arrangements which can be made forhisfuture. 8. After-care.The stage at which the patient returns to the community and, perhaps,to his old surroundings andacquaintances, is a crucial one.Employment, unpaid or otherwise is almost always indicated andregularconsultations are likely to be essential. In drawing up thesenotes on treatment the Committee gratefully acknowledges its debt toDr. Harris Isbell of theNational Institute of Health AddictionResearch Centre, Lexington, Kentucky, U.S.A., who gave his evidenceandadvice from the very extensive experience which he has had in thissubject. APPENDIX IV SUMMARIES OF THE CASE HISTORIES OF KNOWN STABILISED ADDICTS1.Mrs. A., a housewife, well past middle age, had a radical amputation ofthe breast forcarcinoma ten years ago. Severe pain at the site of theoperation and elsewhere in associated areas has persistedever since.For the greater part of this period she has been taking pethidine,prescribed by her general practitioner,at the steady rate of 3 to 4tablets, each of 50 mg., daily. On this dosage she is relatively freefrom symptoms and isable to undertake her own housework. There is noindication that the dose requires to be increased, butnumerousattempts at withdrawal, or substitution by codeine, aspirinpreparations, etc. have met with a return of herpain and incapacity.No personality changes have been detected. 2. Mrs. B., also ahousewife, and well past middle age, has been troubled for over tenyears with very severevaricose ulceration of the leg. This has notbeen improved by conventional treatment. The pain has notbeenmitigated by antipyretic analgesics. For about five years she hasreceived 5 tablets of pethidine, each of 50mg., daily. This enablesher to carry out her duties as a housewife and to look after members ofher family sufferingfrom severe disease and psychoneuroses. There hasbeen no need to increase the dose, but when the drug iswithheld thepatient pleads that she cannot carry on because of the pain. 3.Mrs. C., a housewife, is an old lady, and a life-long neurotic person.Suspected of a crush-fracture in themid-thoracic region after a fallshe has complained of constant pain despite a spinal support. With fourmethadonetablets, each of 5 mg., per day she manages her householdduties. There has been no plea to increase the dose.On the other handwithdrawals have led to such a reaction that the home and family havesuffered. 4. Mr. D. is past middle age; he is employed in theoffice of a large manufacturing firm. For many years he hassufferedfrom generalised osteoarthritis. He has had advice and treatment fromseveral consultants. Some year agolevorphanol was prescribed. At firstthere was a tendency for the dose to rise but, for about five years nowit hasremained at 3 tablets, each of 1. 5 mg., daily. Attempts havebeen made at withdrawal on several occasions. Therehas been noabstinence syndrome, but the patient's pain has returned with aseverity sufficient to stop him working.So long as he is given histablets he seems to be capable of a hard responsible full day's work. 5.Mrs. E. is a manic-depressive of middle age. Her persistent symptom islow back pain for which she has hadoperations. In addition she hasexhibited pseudo-cyesis and has been an in-patient in a mentalhospital. Her record
13 / 14
Drug Addiction, 1st Brain ReportMonday, 27 March 1961 00:00
includes reports from very many consultants. Nineyears ago she was treated with pethidine. A year-and-a-half later thiswas changed to methadone, the doseof 10 mg. every six hours havingremained unchanged all this time. On this quantity she does all herownhousework. In her better phases she has voluntarily reduced the dosagetemporarily to some extent. When,however, the drug was withdrawnaltogether during the time that she was an in-patient at the mentalhospital aprofound nervous disturbance immediately followed. 6.Mr. F. is described as a clerical worker past middle age. He suffersfrom a painful disease which has necessitatedthe amputation of limbs.For several years he has received analgesics for his pain, firstpethidine and subsequentlyphenadoxone. Over the last four years hisdose of phenadoxone has been steady at the rate of twenty 10mg.tablets daily. On this quantity he appears to have shown no mentaldeterioration; on the contrary he continues towork responsibly. Whenother, non-addictive drugs have been substituted from time to time, hispain has returnedwith renewed severity.