51
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | marcus-short |
| View: | 219 times |
| Download: | 1 times |
Neurotransmitters-101
• Dopamine pathway – learning, pleasure• Serotonin pathway – regulates mood• Opioid pathway – antinociceptive• Noradrenergic – alertness, decision-making• Glutamate – excitation• GABA, acetylcholine – inhibition

Neural Reward Circuits Important in the Reinforcing Effects of Drugs of Abuse.
Camí J, Farré M. N Engl J Med 2003;349:975-986.

“The Substance” and the Brain:Neuroadaptation
• Yin-Yang – homeostasis (activating/inhibiting)• Intoxication – temporary dominance• Tolerance – activating opposition, down-
regulating receptors• Withdrawal – removing the drug; biological
effects much longer-lasting (days to years)• Tx of WD – substance mimetics (long-acting,
taper); antagonizing opposition

Universal Withdrawal Symptoms
• Drug craving• Irritability• Dysphoria• Anxiety• Insomnia• + specific Sx of whatever agonist/antagonist
receptor systems involved• Immediate phase: starts w/i hours, lasts days• Protracted phase: 6-18 mo (malaise, cravings)

General Assessment Principles
• Primary substance – type, route, frequency, amount, time of last use
• Complications of use and withdrawal• History of medication-assisted detox• Concurrent substances use/co-morbidities• Vital signs• Mental status• Pupils• Ability to ambulate• Urine toxicology
General Approach to O/D
• Airway• Breathing• Circulation
Coma cocktail– Thiamine 100 mg– 1 amp of D50– Naloxone 2 mg

Alcohol: the Most Common and Lethal
• GABA-A vs. glutamate/NMDA• Indirect release of β-endorphins and dopamine• In and Out: consider Pruno, hand-sanitizers• Intoxication: slurred speech, confusion, ataxia, ↓HR;
assess ability to protect airway• Withdrawal
– Early symptoms 6-24 hrs– Seizures 12-48 hrs– Isolated hallucinosis 12-48 hrs– Delirium Tremens 48-96 hrs

Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-Ar)
• Most commonly used instrument, validated• Measures 10 subscales
– Nausea/vomiting Tactile disturbances– Tremor Auditory
disturbances– Diaphoresis Visual disturbances– Anxiety Headache– Agitation Orientation
• Max score 67, prophylaxis if >8, hospitalization if >15-20, ICU if > 35

EtOH: Cornerstones of Treatment
• Monitor – CIWA-Ar, VS; close observation• EtOH substitutes – benzodiazepines• Supportive treatment
– Quiet, protective environment– Correct hypovolemia/electrolytes– Thiamine (before glucose), MVI, folate, MgSO4
• Adjunct treatment– Beta-blockers, antipsychotics– Anticonvulsants– α2 agonists, muscle relaxants
EtOH substitute: Benzodiazepines
• Fixed ATC vs. Sx-triggered dosing• Chlordiazepoxide (Librium)
– Longest-acting, active metabolites, auto-taper– 50-75 mg PO q 4-6 hrs, add’l doses hourly prn
• Lorazepam (Ativan)– Medium-to-short acting, no active metabolites– Preferable in patients with advanced cirrhosis or
high risk for oversedation (elderly, co-morbidities)– 1-2 mg PO q 4-6 hrs, hourly prn

EtOH Dependence
• Medication is adjunct to ψ-social intervention• Acamprosate
– NMDA partial antagonist; 666 mg tid• Disulfiram
– Blocks alcohol dehydrogenase; nausea/flushing/↑HR; 250-500 mg/d• Naltrexone
– Blocks μ-opioid receptors– Oral (50 mg/d) or injectable (380 mg/mo)
• Baclofen– GABA-B agonist; anxiolytic; 10-20 mg tid
• Topiramate– ↑GABA, ↓glutamate; slow titration to 300 mg/d

Benzodiazepines
• Most abused: short-acting alprazolam (Xanax)• Most common: clonazepam (Klonopin),
Valium (Diazepam), lorazepam (Ativan)• Intoxication: similar to EtOH• WD: beware of much longer half-life• Tx: chlordiazepoxide or clonazepam taper
– Carbamazepine as an alternative for w/d Sx

Gamma-Hydroxybutyrate
• Acts on specific GHB and GABA-B receptors• Euphoric, ↓inhibition, amnesia, hypotonia,
somnolence, ↓HR, ↓BP, clonus, resp. depression• Short-acting; acute intoxication best treated
with observation if no respiratory compromise• WD: similar to BZD/EtOH, less autonomic,
more CNS – insomnia, tremor, anxiety; 1 wk• Tx: consider BZD taper, baclofen

Z-drugs
• Zolpidem, zaleplone, (es)zopiclone• GABA-A receptor; effects similar to BZD• High doses – euphoria, exaltation, anxiolysis• Dependence, withdrawal – similar to BZD
(from sympathetic O/D to Sz)• Tx: consider diazepam or gabapentin taper

Carisoprodol (Soma)
• Metabolized into meprobamate• Acts on GABA-A; similar to barbiturates/BZD• Sedative, relaxant, euphoric; synergy w/ opiates• Abuse increasing; 2012 - schedule IV• WD: anxiety, insomnia, HA, myalgia, tremors,
hallucinations, paranoia• Tx: consider BZD taper (if 12-25 tab/day)

Gabapentin (Neurontin)
• Increased availability of endogenous GABA, +/- action on GABA-B, ↓ glutamate release
• Intranasal snorting: high similar to cocaine• Oral use: similar to EtOH, BZD• WD: depression, anxiety, insomnia,
depersonalization, paresthesias, delirium• Tx: taper for doses >1800 mg/d
Pregabalin (Lyrica)
• Similar to gabapentin– Higher potency, quicker absorption, ↑ bioavailability
• Euphoric, dissociative effects; tolerance• WD: agitation, tremor, ↑ HR, ↑ BP• Tx: 1-wk taper (for doses > 300 mg/d)

Topiramate (Topamax)
• Augments GABA action• Antagonizes AMPA/kainate glutamate receptor• Often requested for wt loss properties• Emerging usefulness in EtOH and stimulant
dependence• Literature indicates little potential for abuse• SE – somnolence, memory problems,
paresthesias

Opiate Intoxication and Tolerance
• Heroin: fine china vs. black tar• μ, δ, κ receptors• Analgesia, modulation of respiration, miosis,
↓gut motility; trigger DA release - euphoria• Tolerance: receptor desensitization, ACh
downregulation, cAMP upregulation

Opiate Overdose
• Heroin, morphine, oxycodone, hydrocodone, methadone• AMS, stupor, miosis• ↓BP, ↓HR, slow shallow breaths, pulmonary edema• Motionless in a cold environment:
– ↓temp, rhabdomyolysis, renal failure• Meperidine (Demerol), propoxyphene (Darvon), tramadol (Ultram)
– mydriasis, Sz• Assess responsiveness, airway protection• Look for fentanyl patches• Tx: naloxone (Narcan) 0.04-0.5-1-2-4-10 mg IV q 2 min• Consider concurrent acetaminophen O/D (Norco, Percocet)

Opiate Withdrawal• Morphine, heroin – 6-12 hrs, methadone 36-48 hrs; last ≈ 2 wks• Activation of cholinergic and noradrenergic systems• Symptoms and signs – COWS
– Nausea, diarrhea, cramping, lacrimation, rhinorrhea, diaphoresis, chills– Irritability, anxiety, insomnia, yawning, ↑HR, ↑BP
• Opiate substitution– Methadone taper – daily, 20-30 d; most Sx at the end; few SE– Buprenorphine – few studies, varying doses/duration– Tramadol – limited literature, similar effectiveness to buprenorphine
• α-2 agonists – modulate noradrenergic hyperactivity– Clonidine 0.1-0.3 mg tid x 2-4 days, taper over 7 days– Reduces WD Sx; increases # who completed WD (vs. placebo)– SE: drowsiness, dizziness, hypotension, dry mouth
• Sx tx: acetaminophen, donnatal, loperamide, hydroxyzine, melatonin

Tx of Opiate Dependence
• Substitute therapy– Methadone; 60-100 mg/d; QTc monitoring– Buprenorphine; 8-24 mg/d
• Pure (Subutex) or combo with naloxone (Suboxone)
• Antagonist therapy– Oral naltrexone; 50 mg/d– Injectable naltrexone; 380 mg/d
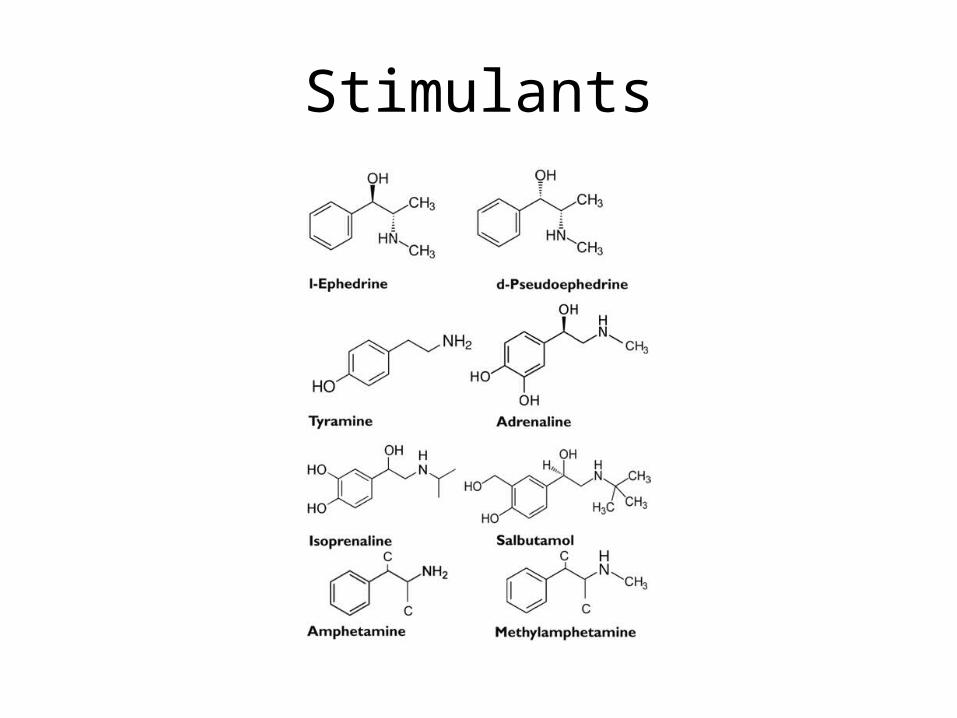
Stimulants
Classic Stimulants
Cocaine• Hydrochloride salt vs. free-base
(crack)• DA, NE, serotonin uptake
transporter inhibition• Lasts 30-60 min• Beware of combos:
“speedball”, cocoethylene
Amphetamines• Speed/crack/crystal meth, Rx
(Adderal, Dexedrine)• Besides transporter inhibition,
↑DA, NE>serotonin release, MAOI• Effects last hours• Related stimulant:
methylphenidate (Ritalin)
Euphoria, ↑ libido, ↓ appetite, ↑ concentrationSleeplessness, anxiety, paranoia, aggression

Classic Stimulants: Intoxication
• Adrenergic stimulation (α,β), DA, serotonin (release, ↓re-uptake)
• ↑BP, ↑HR, ↑temp, mydriasis• Dry mucous membranes and diaphoresis• Agitation, delirium, hypertonia, seizures • Vasospasm (myocardial, cerebral), arrhythmia• Rhabdomyolysis, renal/hepatic toxicity• Tx: lorazepam, haloperidol, labetalol for HTN;
nitrates/CCB for chest pain; cooling

Stimulant O/D: Tx Considerations
• Avoid 3Ps– Physical restraints– Phenothiazines in escalating doses– Psychiatric ward
• Use ART– Acceptance (explanation, reassurance)– Reduce stimuli (dark, quiet environment)– Talkdown

Stimulant Withdrawal
• Chronic use ↓ glutamate, DA, serotonin• WD (“tweaking”) w/i 24 hrs of last dose• “Crash” – acute, 1wk; subacute – 2-3 wks• Hyperarousal: craving, agitation, vivid dreams• Reversed vegetative: hypersomnia, ↓ energy, ↑appetite• Anxiety: dysphoria, anhedonia, paranoia, ψmotor slowing
Tx of Stimulant WD and Dependence
• No proven tx, but a number of research avenues• Modafinil: mild stimulant, ↑ glutamate; blocks euphoria
– May attenuate cocaine w/d– Not effective for methamphetamine dependence
• GABAergics for maintenance– Vigabatrin, topiramate
• Disulfiram– Increases cocaine/DA levels, unpleasant anxiety
• Cocaine and methamphetamine vaccines– Stimulate production of Ab which prevent stimulants’ entrance
into CNS

Ecstasy/MDMA
• 3,4-methylenedioxymethamphetamine• Serotonin > DA/NE reuptake inhibition• Onset 30 min, last 4 hrs• Intense sensual experiences, empathy, sociability,
insomnia, ↓appetite• ↑Temp, ↑BP, ↑HR, mydriasis, diaphoresis, trismus• Serotonin syndrome, hyponatremia, dehydration• No medications for tx of mild intoxication or WD• Dependence rare, largely psychological

Bath Salts
• Mephedrone, methylenedioxypyrovalerone– Mephedrone: more stimulant, onset/action 30-60 min– MDPV: more hallucinatory, onset 1 hr, lasts 2-3 hrs
• Cathinone (Khat plant) derivatives, stimulants• DA, serotonin, NE reuptake inhibition• Euphoria, hallucinations → insomnia, paranoia• Agitation, twitches, ↑HR, ↑BP, ↑ temp, mydriasis, Sz• Rhabdomyolysis, renal failure, MI, excited delirium• WD: very severe cravings, fatigue, irritability; 1-2 d• Tx: cooling, hydration, lorazepam, haloperidol

Albuterol
• Stimulant-like (ᵦ-adrenergic)• Clenbuterol – pill, abused by body-builders• Frequent canister exchange – red flag• Spray on paper, dry, inhale powder• ↑HR, ↓BP, tremor, agitation• Tx: observation; consider propranolol

Bupropion (Wellbutrin)
• DA and NE reuptake inhibitor, nicotinic antagonist• Chemically similar to stimulants• Antidepressant, no wt gain or sexual dysfunction• Abused intranasally; high similar to cocaine, but
less intense• Seizure with high doses (>600 mg/d)• WD rare; anxiety, lethargy, irritability• Tx: gradual taper

Selective Serotonin Reuptake Inhibitors
• Intoxication: serotonin syndrome (usually drug combinations)– Flushing, fever, diaphoresis– Trismus, tremor, irritability
• Tx: lorazepam, consider cyproheptadine• WD: anxiety, crying, dizziness, HA, nausea,
insomnia, vivid dreams, tremor

Quetiapine (Seroquel)
• Antihistaminic and anticholinergic effects• Sedative, anxiolytic; may ↓amphetamine craving• ↑blood methadone levels• 80% of opioid misusers exposed to quetiapine• Intranasal and intravenous use described• WD: insomnia, anxiety• Taper not needed for low dose (<200 mg/d)

Steroids
• Anabolic-androgenic; testosterone derivatives• Androstenedione, DHEA – OTC precursors• Frequent co-dependence with opioids• ↑Muscle mass, ↑strength, ↓fat; appearance,
performance, sense of well-being• Excessive dose – mania, psychosis, hepatotoxic• WD: hypogonadism, fatigue, HA, myalgia, insomnia,
depression• Tx (rarely needed): gradual tapering of injectable
testosterone, guided by trough levels
Antihistamines
• Promethazine (Phenergan),diphenhydramine (Benadryl), TCAs, baclofen
• Potentiate opiates; high dose – hallucinations• Anticholinergic properties: “Hot as hare, dry
as a bone, red as beet, mad as hatter”• Mydriasis, ↑HR, ↑BP, urinary retention, Sz• QT prolongation• Tx: tincture of time

Dissociatives - PCP
• Phencyclidine (PCP, angel dust)• NMDA agonist, anticholinergic, opioid agonist,
α-adrenergic, dopaminergic• Intoxication: violent agitation, bizarre
behavior, lethargy – fluctuating delirium• Tx: lorazepam and haloperidol

Dissociatives - Ketamine
• Onset – 5-30 min, lasts up to 3 hrs• Antagonist at NMDA, agonist at μ–opioid receptor• Anticholinergic, potentiates GABA, releases DA• Hallucinations, distortions of time/space• Dissociation, depersonalization – “K-hole”• OD: non-lethal; prone to accidents; abdominal pain,
dizziness, lower urinary tract Sx; ↑ HR• WD: anxiety, craving, +/- tremor, diaphoresis • Methoxetamine – slower onset, longer duration

Dextromethorphan
• OTC component of cough syrup or tablet• Synthetic analog of codeine; σ-opioid receptor• Dissociative in doses > 7mg/kg (metabolite
dextrophan – NMDA antagonist); serotomimetic• Stimulant, euphoria→hallucinations→sedation,
disassociation• ↑BP, ↑HR, respiratory depression, mydriasis• Utox – may cross-react with PCP assay• Effects short-lived; no dependence/withdrawal

Caffeine
• Most widely used psychoactive drug worldwide• Stimulant; adenosine receptor antagonist• ↑NE and DA levels; ↑ alertness, coordination• Intoxication: ↑HR, tremor• WD: HA, fatigue, difficulty concentrating,
depression, irritability, nausea, myalgia– start in 12-24 hrs, last 2-9 days

Tobacco
• Activation of nicotinic cholinergic receptors• DA release; also glutamate/GABA• Enhanced performance, elevated mood, ↓ wt• WD: anxiety, irritability, depression, insomnia• Nicotine substitutes: gum, patch, e-cigarette • Partial agonists: cytisine, varenicline• Bupropion SR: inhibits DA and NE reuptake• Nortriptyline: similar effects, lesser abuse
Marijuana/Cannabis
• Most widely used illicit drug worldwide• Hashish vs. sinsemilla (skunk): Δ9-THC/cannabidiol content• Cannabis receptor, NE release, dopaminergic, anticholinergic• Intoxication: euphoria, giggling, perceptual distortion, sedation
– Later: hunger, conjunctival injection, dry mouth, ↑HR; panic, psychosis– Consider propranolol for CV effects, lorazepam for anxiety
• WD: anxiety, insomnia, ↓appetite, nausea, diarrhea, abdominal pain, anger, HA, chills– Sx start w/i 24 hrs of cessation, last up to 28 d– Small studies of dronabinol, Li, buspirone, zolpidem– No medications currently recommended for tx of WD or dependence

Hallucinogens
• Lysergic acid diethylamide, psilocybin, mescaline, DMT (dimethyltryptamine)
• Serotonin agonists• Hallucinations, synesthesia, mild euphoria,
time distortions, religious experiences, anxiety• Mydriasis, hyperthermia• Tx: time, lorazepam• Withdrawal: non-existent

Salvia Divinorum
• Agonist at κ–opioid receptors; secondary effects – cannabinoid, serotonin, DA
• Onset 30 sec, lasts 20-30 min• Vivid colors/shapes, hallucinations, synesthesia• OD: dysphoria, anxiety, psychosis• WD: not well described; possible GI effects

Inhalants• Volatile solvents
– Enhance GABA-A, inhibit NMDA; ↑DA– Euphoria, “drunkenness”– Lethargy, confusion, HA, restlessness, incoordination
• Alkyl nitrites– Smooth muscle relaxants, ↑libido, euphoria– Nausea, ↓BP, HA; hemolysis, methemoglobinemia
• N2O– Euphoria, distortion of sensation/time/space, anesthesia– Oxidizes B12, resulting in deficiency
• WD: craving; no physical signs; Tx: observation/support

•Cami J, Farre M. Drug addiction. NEJM 2003; 349:975-86•Mokhesi B. et al. Adult toxicology in critical care. Chest 2003; 123:577-92, 897-921•Kosten T, O’Connor, P. Management of drug and alcohol withdrawal. NEJM 2003; 348:1786-95•Lingford-Hughes AR, et al. BAP updated guidelines: evidence-based guidelines for the pharmacological management of substance abuse, harmful use, addiction and comorbidity. J Psychopharmacology 2012; 26:899–952•Amato L. et al. Efficacy and safety of pharmacological interventions for the treatment of the alcohol withdrawal syndrome. Cochrane Library 2011, Issue 6•Loperz-Munoz F. The discovery of chlordiazepoxide and the clinical introduction of benzodiazepines. J Anxiety Disord 2011; 25:554–62•Parr JM et al. Effectiveness of current treatment approaches for benzodiazepine discontinuation: a meta-analysis. Addiction 2008; 104:13–24•Dell’osso B, Lader M. Do benzodiazepines still deserve a major role in the treatment of psychiatric disorders? European Psychiatry 2013; 28:7–20•Reeves R. Benzodiazepines and low-dose quetiapine in prison: guideline, education, and peer comparison to reduce prescriptions. J Correct Health Care 2012; 18:45-52•Snead O, Gibson K. γ-Hydroxybutyric acid. NEJM 2005; 352:2721-32•Wojtowitz JM et al. Withdrawal from gamma-hydroxybutyrate, 1,4-butanediol and gamma-butyrolactone. CJEM 2008;10:69-74
References
•Recoppa L., et al. Gabapentin abuse in inmates with prior history of cocaine dependence. American J on Addictions 2004; 13:321-3•Gabapentin and pregabalin: abuse and addiction. Rev Prescrire 2012; 340:116-8•Gahr M et al. Concerns about pregabalin: further experience with its potential of causing addictive behaviors. J Addict Med 2013;7:147–9•Reeves RR et al. Carisoprodol: update on abuse potential and legal status. Southern Medical Journal 2012; 105:619-23•Victorri-Vigneau C et al. Pharmacoepidemiological characterisation of zolpidem and zopiclone usage. Eur J Clin Pharmacol 2013; epub•Sporer, K. Acute heroin overdose. Ann Int Med 1999; 130:584-90•Boyer E. Management of opioid analgesic overdose. NEJM 2012; 367:146-55•Threlkeld M et al. Tramadol versus buprenorphine for the management of acute heroin withdrawal. American J on Addictions, 2006; 15:186–91•Gowing L et al. Alpha2-adrenergic agonists for the management of opioid withdrawal. Cochraine Library 2009, Issue 3•Lobmaier P et al. The pharmacological treatment of opioid addiction. Eur J Clin Pharmacol 2010; 66:537–45•Fareed A et al. Heroin anticraving medications. American J Drug and Alcohol Abuse, 2010; 36:332–341

•Lee MR. The history of ephedra (ma huang). R Coll Physicians Edinb 2011; 41:78–84•Snelders S, Pieters T. Speed in the Third Reich: metamphetamine (Pervitin) use and a drug history from below. Soc History Med 2011; 24:686–99•Panenka WJ et al. Methamphetamine use: a comprehensive review of molecular, preclinical and clinical findings. Drug and Alcohol Dependence 2013; 129:167–79•Freye, E. Pharmacology and abuse of cocaine, amphetamines, ecstasy, and related designer drugs. Springer Science 2009.•Shoptaw SJ, Kao U,Heinzerling K, Ling W. Treatment for amphetamine withdrawal. Cochrane Library 2009, Issue 2•Kampman KM. What’s new in the treatment of cocaine addiction? Curr Psychiatry Rep 2010; 12:441–7•Winder GS et al. Are “Bath Salts” the next generation of stimulant abuse? J Subst Abuse Treat 2013; 44:42–45•Zawilska JB, Wojcieszak J. Designer cathinones—an emerging class of novel recreational drugs. Forensic Science Internat 2013; 231:42–53 •Boucher A. et al. Salbutamol misuse or abuse with fatal outcome: A case-report. Hum Exp Toxicol 2011 30: 1869-71

•Yoon G, Westermeyer J. Intranasal bupropion abuse: case report. American J on Addictions 2013; 22:180•Reeves RR, Ladner ME. Additional evidence of the abuse potential of bupropion. J Clinical Psychopharmacology 2013; 33:584-5•Nielsen M et al. What is the difference between dependence and withdrawal reactions? A comparison of benzodiazepines and selective serotonin re-uptake inhibitors. Addiction 2011; 107:900–8•McLarnon ME et al. Characteristics of quetiapine misuse among clients of a community-based methadone maintenance program. J Clin Psychopharmacology 2012; 32:721-3•Tamburello AC et al. Successful removal of quetiapine from a correctional formulary. J Am Acad Psychiatry Law 2012; 40:502–8•Kanayama G et al. Anabolic–androgenic steroid dependence: an emerging disorder. Addiction 2009; 104:1966–78•Shapiro B et al. Promethazine misuse among methadone maintenance patients and community-based injection drug users. J Addict Med 2013;7:96–101•Corazza O et al. From “Special K” to “Special M”: the evolution of the recreational use of ketamine and methoxetamine. CNS Neuroscience & Therapeutics 2013; 19:454–60•Romanelli F, Smith KM. Dextromethorphan abuse: clinical effects and management. J Am Pharm Assoc. 2009; 49:e20–7

•Olive MF et al. Glutamatergic medications for the treatment of drug and behavioral addictions. Pharmacology, Biochemistry and Behavior 2012; 100:801–10•Juliano LM et al. Development of the Caffeine Withdrawal Symptom Questionnaire. Drug and Alcohol Dependence 2012; 124:229– 34•Cahill K et al. Pharmacological interventions for smoking cessation: an overview and network meta-analysis. Cochrane Library 2013, Issue 5•Thibodeau L et al. Prerelease intent predicts smoking behavior postrelease following a prison smoking ban. Nicotine & Tobacco Research 2010; 12:152–8•Crippa JAS et al. Pharmacological interventions in the treatment of the acute effects of cannabis. Harm Reduction Journal 2012; 9:7-12•Forti MD et al. High-potency cannabis and the risk of psychosis. British J Psychiatry 2009; 195, 488–91•Allsop DJ et al. Quantifying the clinical significance of cannabis withdrawal. PLOS One 2012; 7 (9)•Beckley JT, Woodward JJ. Volatile solvents as drugs of abuse: focus on the cortico-mesolimbic circuitry. Neuropsychopharmacology 2013; 1–13•Zawilska JB, Wojcieszak J. Salvia divinorum: from Mazatec medicinal and hallucinogenic plant to emerging recreational drug. Hum Psychopharmacol Clin Exp 2013 epub•Gibbons S. ‘ Legal Highs’ – novel and emerging psychoactive drugs. Clinical Toxicology 2012; 50:15–24

















![Cyanide Intoxication after Ingestion of Wild Cherry (Prunus Avium) · cause acute cyanide intoxication or some chronic diseases [14]. Several cyanide intoxication cases has been reported](https://static.documents.pub/doc/80x56/613b2037f8f21c0c8268d3d6/cyanide-intoxication-after-ingestion-of-wild-cherry-prunus-avium-cause-acute-cyanide.jpg)
