26
Drugs affecting breast milk and lactation Prof. Hanan Hagar Dr.Abdul latif Mahesar Pharmacology Department College of Medicine
| Date post: | 28-Dec-2015 |
| Category: |
Documents |
| Upload: | giles-eaton |
| View: | 236 times |
| Download: | 2 times |
Drugs affecting breast milk and lactation
Prof. Hanan Hagar
Dr.Abdul latif Mahesar
Pharmacology Department
College of Medicine

Intended learning issues
• Relation of drugs and lactation• Factors modifying passage of drugs in
milk• Effects of drugs on milk production• Role of lactation on drugs excretion• Drug safety during lactation / use of
safe drugs• Drugs contraindicated during lactation

LACTATION
• Breast feeding is very important because mother’s milk is the best nutritious , most compatible and healthiest form of milk for babies.
• It also Provides the baby with immunoglobulins (IgA, IgM) that are essential for protection against gastroenteritis.

DRUGS AND LACTATION
• Most drugs administered to breast feeding woman are detectable in her milk.
• The concentration of drugs achieved in breast milk is usually low.
• Even small amounts however may be of significance for the suckling child because his drug metabolic and eliminating mechanisms are immature.

• Neonates have very limited rate of metabolism due to immaturity of liver enzymes that is not fully developed until 8 weeks of age.
• Renal clearance is less efficient: well developed after 3-5 months.
• Premature babies and newborn (less than 1 month of age) have much more limited capacity for metabolism and excretion.

• The epithelium of the breast alveolar cells is most permeable to drugs during the 1st week postpartum, so drug transfer to milk may be greater during the 1st week of an infants life.

Factors controlling passage of drugs into breast milk
1. Physiochemical character of the drug Lipid solubility of the drug: lipid soluble
drugs pass more freely in the breast milk
Molecular weight: low molecular weight drugs are more likely to get transferred to breast milk than high molecular weight
• e.g.• Insulin: MW > 6,000 daltons• Heparin: MW 40,000 daltons• Ethanol: MW 200

Factors controlling passage of drugs into breast milkcontinued
Degree of ionization: nonionized form of drugs are more likely to be transferred into breast milk.
pH of the plasma and milk:
Weakly alkaline drugs tend to be concentrated in milk.
Weakly acidic drugs don't enter the milk to a significant extent and tend to be concentrated in plasma.

Maternal blood circulation Milk
Alkaline drug
Nonionized acidic drug will diffuse back
Acidic drug
Ionized alkaline drug will be captured
Effect of pH of the plasma and milk
plasma pH is 7.4 Milk pH is 7.2

2. Plasma protein binding of drugs highly plasma protein-bound drugs pass less into milk.
anti diabetic
3. Drug concentration in maternal serum Transfer of drug from mother’s blood to milk is passive and is low with drugs that have
large volume of distribution (Vd). short half life (t ½).

The amount of a drug to which the babyis exposed as a result of breast feedingdepends on:
• The concentration of the drug in the milk at the time of feeding.
• The amount of milk consumed.
• The amount of drug absorbed.
• The ability of the baby to eliminate the drug.

General considerations to minimize risk to nursing infant
• The safest drug should be chosen.
e.g. Acetaminophen than aspirin for analgesia
• Route of administration (topical, local, inhalation) instead of an oral form.
• Poorest oral bioavailability
• Lowest lipid solubility.
• Shortest half-life
• Highest protein-binding ability.

General considerations to minimize risk to nursing infant
• Lactating mother should take medication just after nursing and 3-4 hours before the next feeding.
• Infants should be monitored for adverse effects e.g. feeding, sedation, irritability, rash, etc.
• Drugs with no safety data should be avoided or lactation should be discontinued.

• Cautions required in - premature infants - low birth weight - infants with impaired ability to metabolize
/excrete drugs eg. sick babies - infants with G6PD deficiency
General considerations to minimize risk to nursing infant

Drugs that should be avoided during lactation
1. Radioactive iodine
2. Anticancer drugs Doxorubicin, cyclophosphamide, methotrexate
3. CNS acting drugs Amphetamine, heroin, cocaine
4. Lithium

Drugs that can suppress lactation
• Thiazide diuretics
• Levodopa (dopamine precursor)
• Bromocriptine (dopamine agonist)
• Ergot derivatives
• Androgens
• Estrogen, oral contraceptives that contain high-dose estrogen and a progestin.

Drugs that can augment lactation
Persistent and active suckling release both prolactin and oxytocin to stimulate milk
secretion.Dopamine antagonists : they stimulate prolactin secretion e.g.
• Metoclopramide (antiemetic)• Haloperidol (antipsychotic)• Phenothiazines • Methyl dopa (antihypertensive drug)• Theophylline (used in asthma)

Penicillins
Ampicillin
amoxacillin
No significant adverse effect
allergic reactions, diarrhea
Cephalosporins No significant adverse effect
Chloramphenicol “Gray baby” syndrome
Possibility of bone marrow suppression
Sulphonamides hyperbilirubinemia -neonatal jaundice Should be avoided in premature infants or infants with G6PD deficiency
Antibiotics
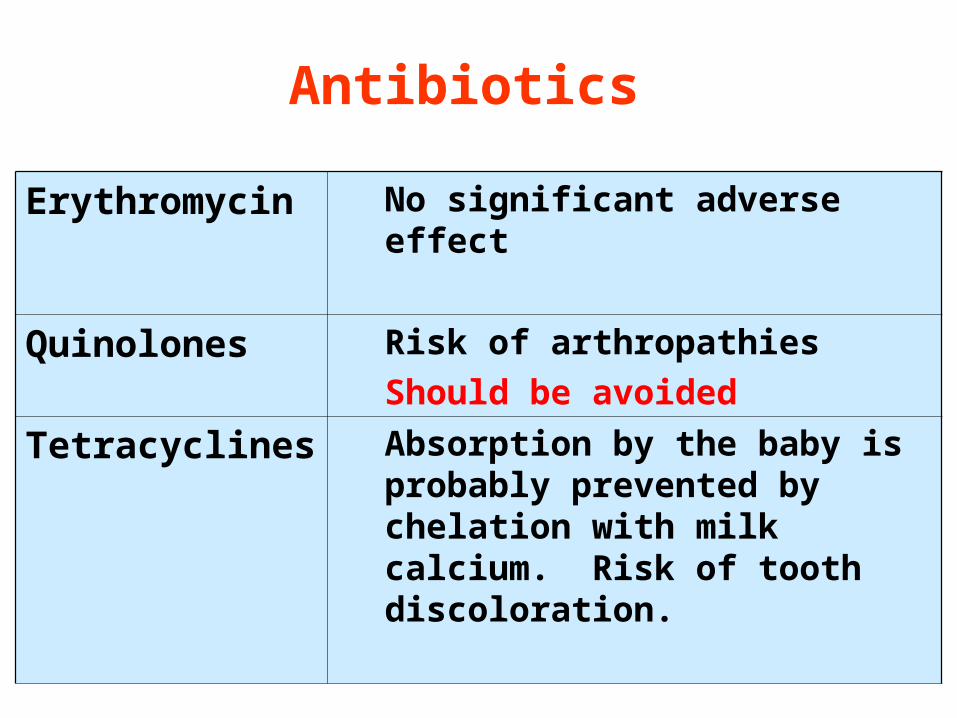
Erythromycin No significant adverse effect
Quinolones Risk of arthropathies
Should be avoided
Tetracyclines Absorption by the baby is probably prevented by chelation with milk calcium. Risk of tooth discoloration.
Antibiotics

Barbiturates
(phenobarbitone)
Lethargy, sedation, poor suck reflexes
Clinical monitoring is recommended
Benzodiazepines
(diazepam)
Lethargy, sedation in infants
Clinical monitoring is recommended
Sedative/hypnoticssingle doses are unlikely to be harmfulRegular use of high doses should be avoided

Insulin
Oral antidiabetics
safe
compatible
Antidiabetics

Non hormonal method should be used
Avoid estrogens containing pills
Estrogens milk quantity
Progestin only pills or minipill are preferred for birth control.
Oral contraceptives

Antithyroid drugs Propylthiouracil
Carbimazole Methimazole
May suppress thyroid function in infants.Propylthiouracil should be used rather than carbimazole or methimazole.
Anticonvulsants
Carbamazepine Phenytoin
Are preferable over othersAmounts entering breast milk are not sufficient to produce adverse effectsInfants must be monitored
Anticoagulants
Heparin
Warfarin
Heparin is not present in breast milk. Safe (very small quantities found in breast milk).

Iodine (radioactive)
Hypothyroidism permanent in infantBreast-feeding is contraindicated
Cytotoxic drugsBreast feeding should be avoided
LithiumLarge amounts can be detected in milk
CVS drugs
Atenolol Risk of bradycardia and hypoglycemiaavoid

Antibiotics Cephalosporins, penicillins
Avoid chloramphenicol, sulphonamides and tetracyclines
Antidiabetics Insulin – oral antidiabetics
Avoid metformin
Anticoagulants Heparin - warfarin
Analgesics Acetaminophen
Antithyroid drugs Propylthiouracil is preferable over others
Anticonvulsants Carbamazepine - phenytoin
Oral contraceptives Progestin only pills or minipills are preferred for birth control.
Antiasthmatics Inhaled corticosteroids - prednisone
Drugs of choice in lactation

Summary for choice of drug
• Short acting
• Highly protein bound
• Low lipid solubility
• High molecular weight
• No active metabolites
• Route of administration
• well-studied in infants

















