Dually enacted stigma among young people and their caregivers living with HIV: Challenges and opportunities to reaching 90-90-90 in Zambia Joseph G. Rosen , Edith S. Namukonda Mwelwa Chibuye, Lyson Phiri, Bwalya Mushiki, Michael T. Mbizvo, Nkomba Kayeyi 13 th INTEREST Conference – Accra, Ghana 14 May 2019
Transcript
Dually enacted stigma among young people and
their caregivers living with HIV:
Challenges and opportunities to reaching
90-90-90 in Zambia
Joseph G. Rosen, Edith S. Namukonda Mwelwa Chibuye,
Lyson Phiri, Bwalya Mushiki, Michael T. Mbizvo, Nkomba Kayeyi
13th INTEREST Conference – Accra, Ghana 14 May 2019
Disclosures
The authors confirm they have no personal or
financial conflicts of interest to disclose.
2
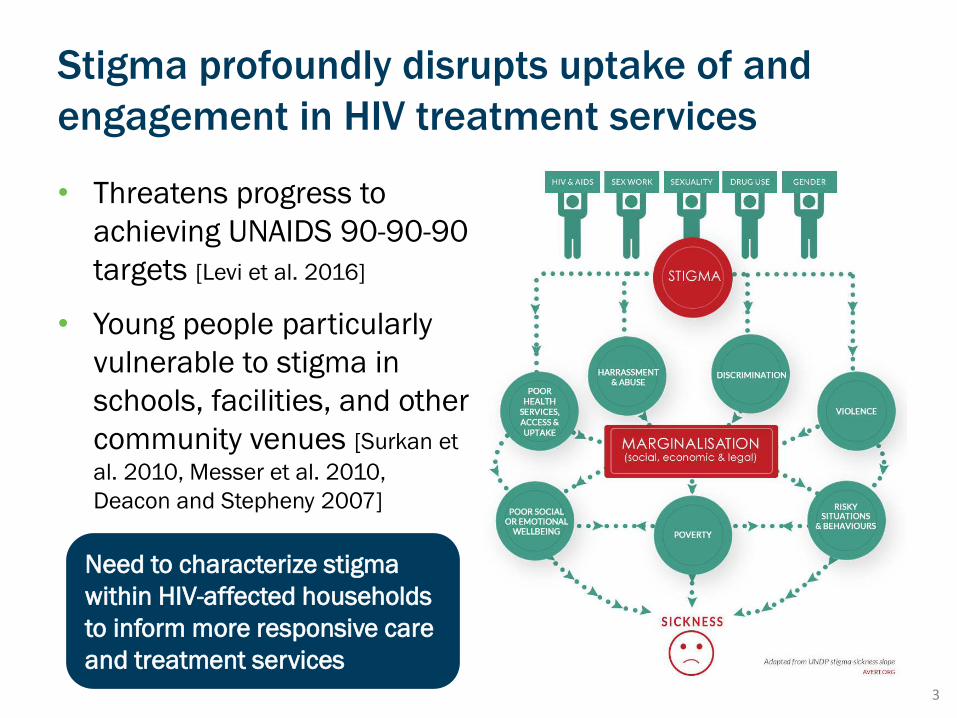
Stigma profoundly disrupts uptake of and
engagement in HIV treatment services
• Threatens progress to
achieving UNAIDS 90-90-90
targets [Levi et al. 2016]
• Young people particularly
vulnerable to stigma in
schools, facilities, and other
community venues [Surkan et
al. 2010, Messer et al. 2010,
Deacon and Stepheny 2007]
3
Need to characterize stigma
within HIV-affected households
to inform more responsive care
and treatment services
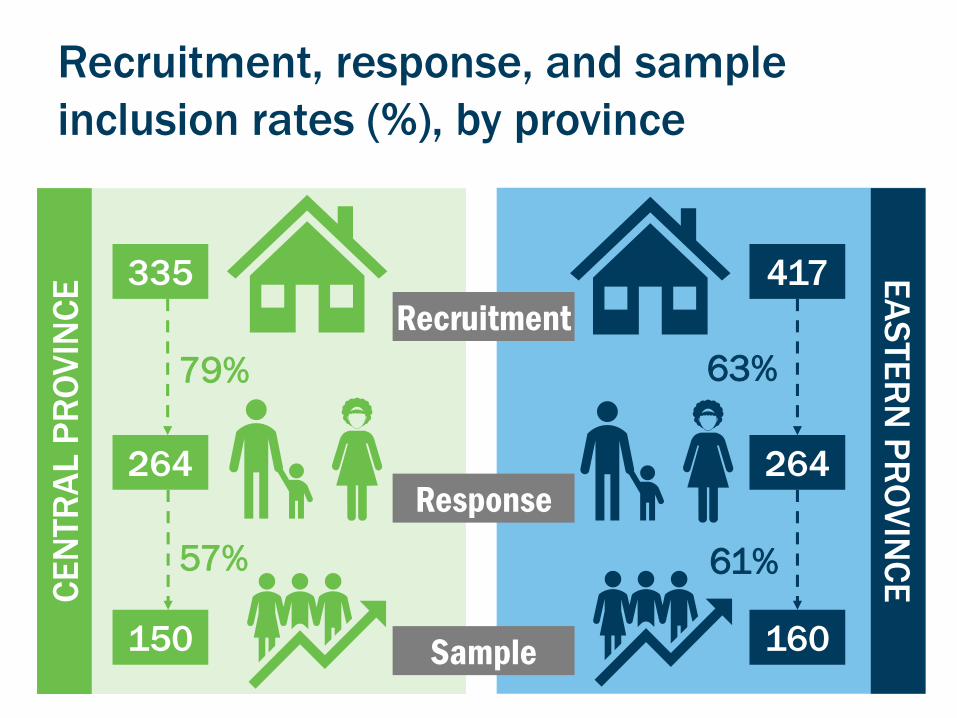
Study design
• Analysis of baseline data from 2-year prospective cohort study
▪ ZAMFAM beneficiaries (Central Province)
▪ Non-beneficiary comparison (Eastern Province)
• Assess changes in socioeconomic well-being, health, and HIV service use
4
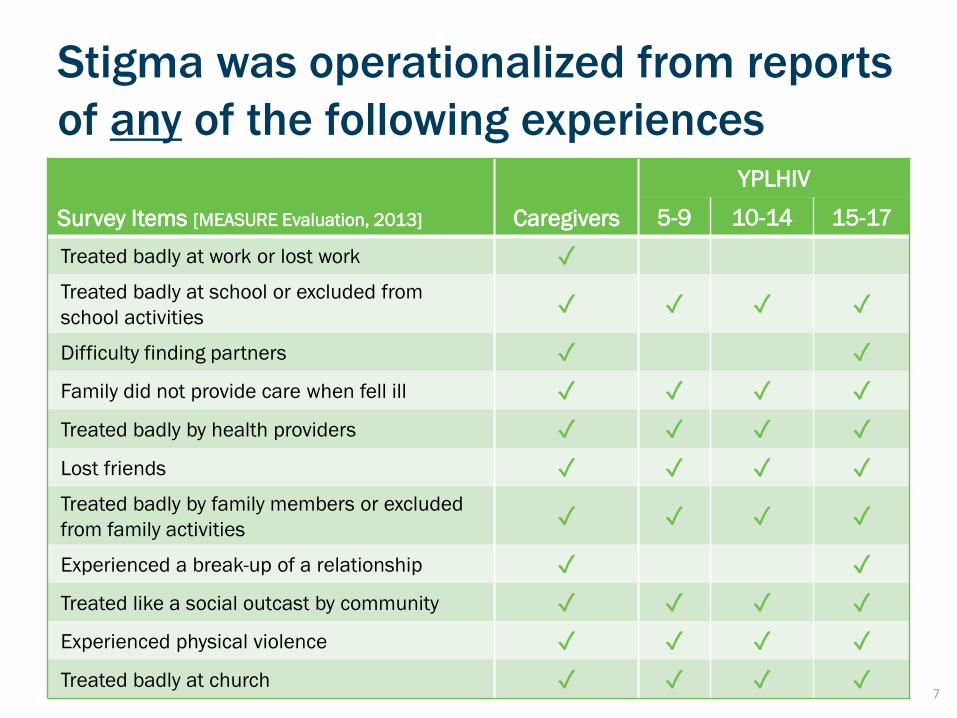
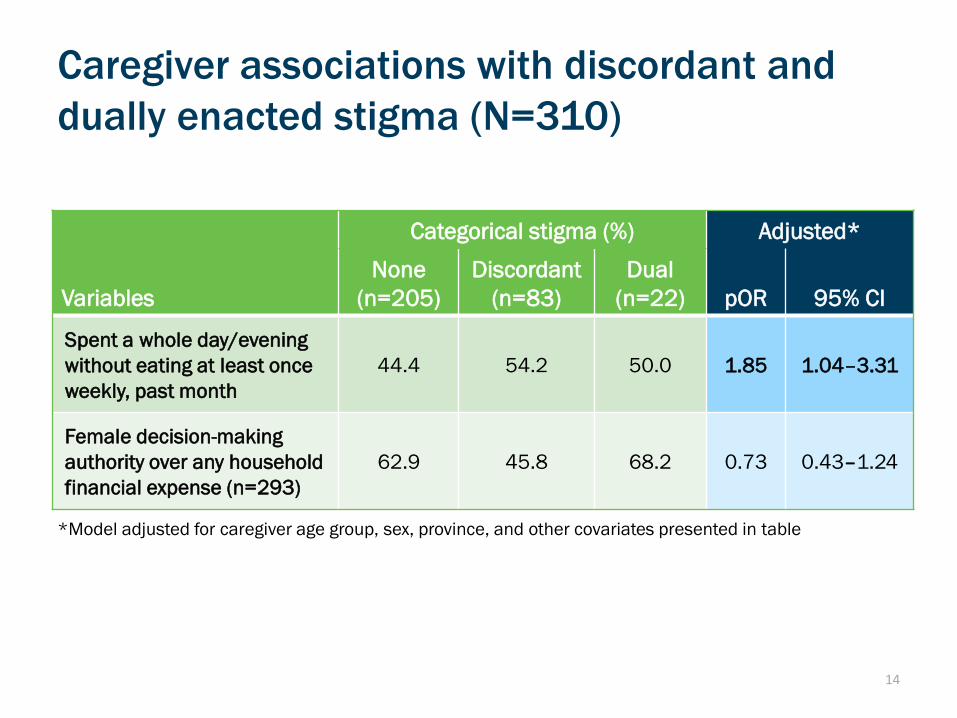
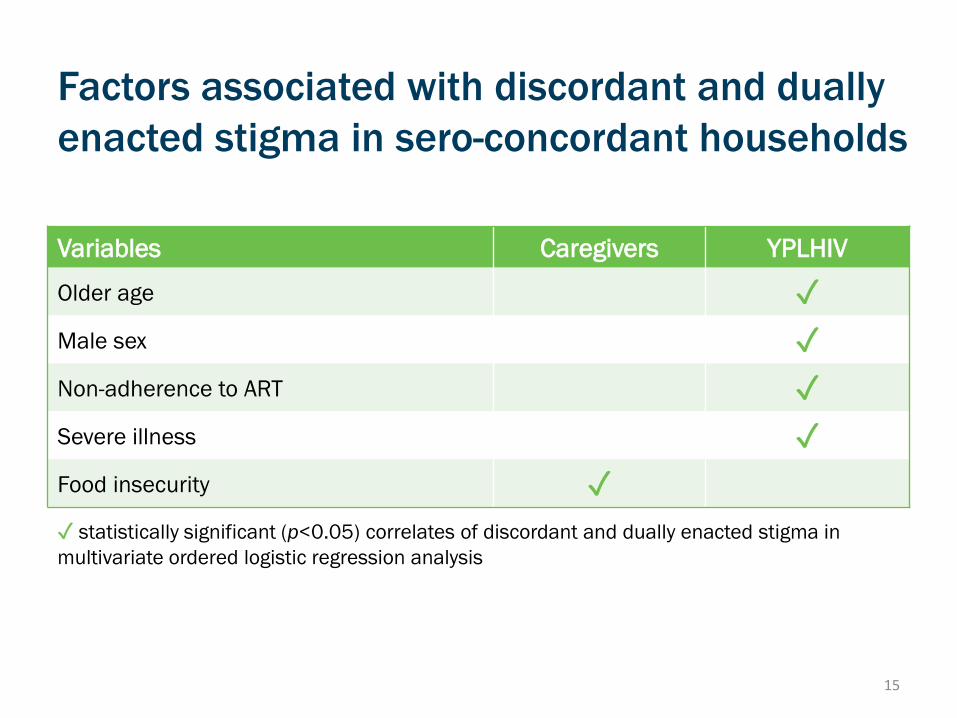
Measure prevalence and factors
associated with stigma among
YPLHIV and their HIV+ caregivers
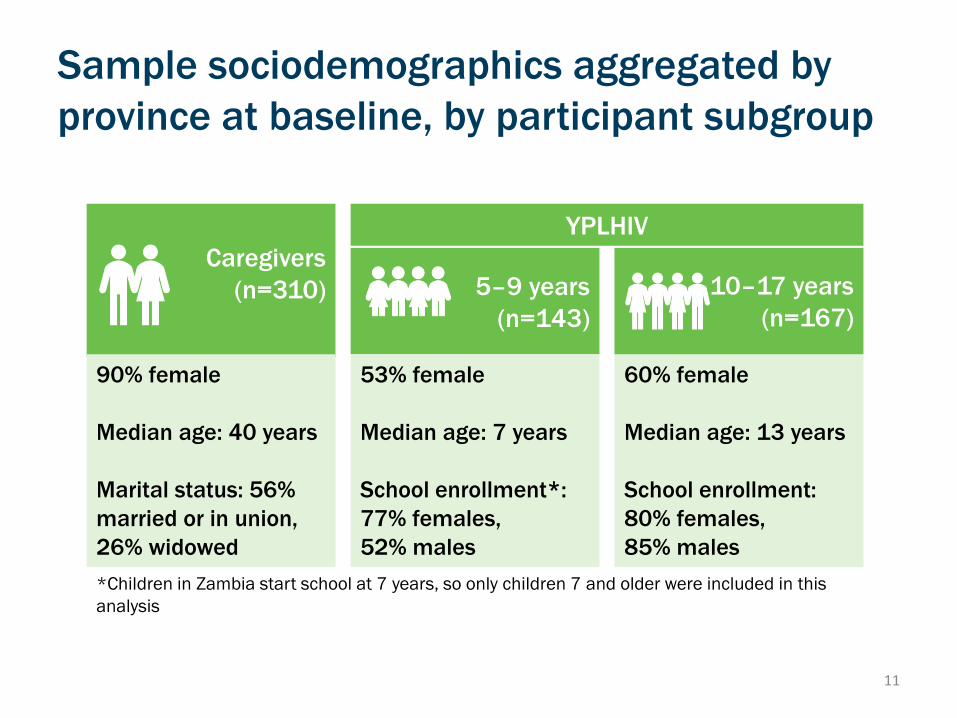
Study population from HIV-affected households
5
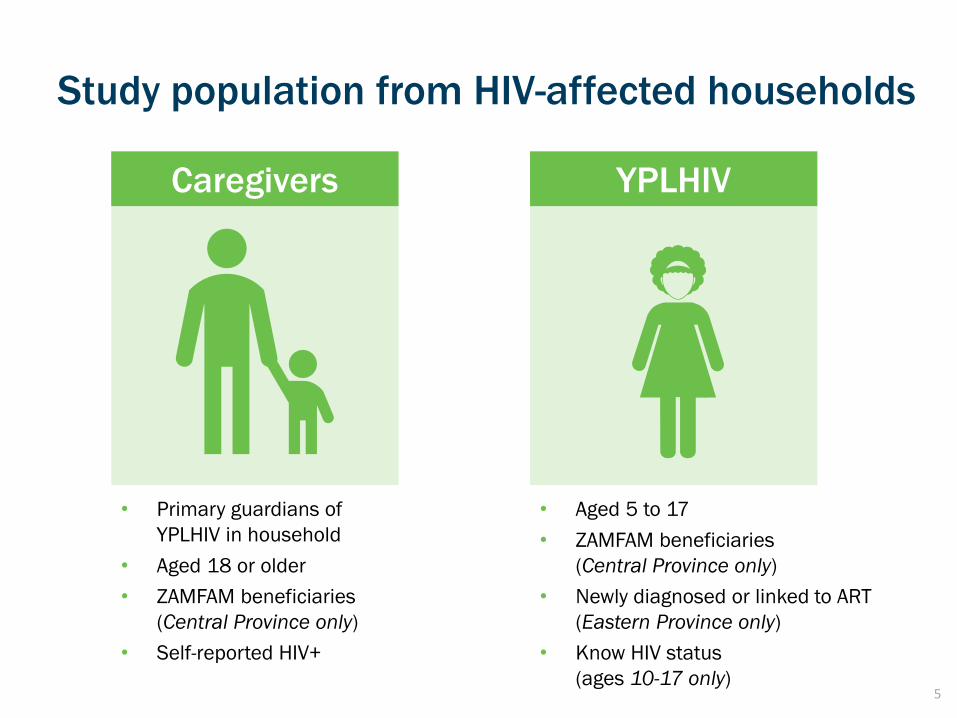
Caregivers YPLHIV
• Primary guardians of
YPLHIV in household
• Aged 18 or older
• ZAMFAM beneficiaries
(Central Province only)
• Self-reported HIV+
• Aged 5 to 17
• ZAMFAM beneficiaries
(Central Province only)
• Newly diagnosed or linked to ART
(Eastern Province only)
• Know HIV status
(ages 10-17 only)
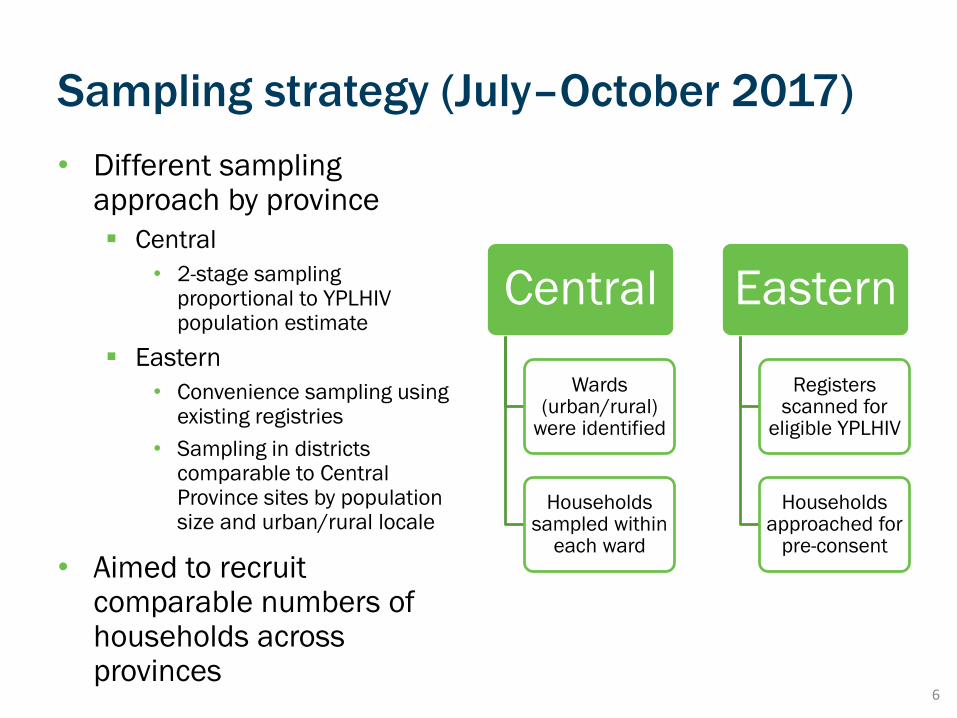
Sampling strategy (July–October 2017)
• Different sampling approach by province
▪ Central
• 2-stage sampling proportional to YPLHIV population estimate
▪ Eastern
• Convenience sampling using existing registries
• Sampling in districts comparable to Central Province sites by population size and urban/rural locale
• Aimed to recruit comparable numbers of households across provinces










![Theory of Planned Behavior, Self‑Stigma, and Perceived ...file.qums.ac.ir/repository/sdh/Theory of Planned...self-stigma (also known as internalized stigma).[5,6] Self-stigma was](https://static.documents.pub/doc/80x56/5f59324ffcada40fd01f4b2a/theory-of-planned-behavior-selfastigma-and-perceived-filequmsacirrepositorysdhtheory.jpg)








