39
Dysphagia in Pseudobulbar palsy PHINOJ K ABRAHAM II nd MOTh Student All India Institute of Physical Medicine & Rehabilitation, (AIIPM&R) Mumbai
| Date post: | 07-May-2015 |
| Category: |
Education |
| Upload: | phinoj-k-abraham |
| View: | 2,023 times |
| Download: | 6 times |

Dysphagiain
Pseudobulbar palsy
PHINOJ K ABRAHAMIInd MOTh Student
All India Institute of Physical Medicine & Rehabilitation, (AIIPM&R) Mumbai

Dysphagia in Pseudobulbar Palsy
◦ Bulbar and Pseudo bulbar Palsy
◦ Dysphagia- Definition
◦ Anatomy of Pharynx
◦ Swallowing Process
◦ Types of dysphagia
◦ Causes of dysphagia
◦ Clinical assessment of dysphagia
◦ Treatment of Dysphagia
Overview
2

Bulbar Palsy◦ Is caused by bilateral lower motor neuron lesion
affecting the nerves supplying the bulbar muscles of the jaw, face, palate, pharynx & larynx.
C/F◦ Impaired speech and swallowing◦ Speech develops a nasal quality due to escape of
air through nose.◦ Paralysis of affected muscles, and tongue appears
wasted.
Bulbar & Pseudobulbar palsy
3

Pseudo bulbar palsy (Supra nuclear bulbar palsy)◦ Pseudo bulbar palsy results from damage to cortico motor
neuron pathways innervating the bulbar musculature◦ It is resulting from an upper motor neuron lesion.
Pattern of involvement 1. Unilateral upper motor neuron lesion
This produce only transient weakness of many of muscles supplied by the cranial nerves. E.g., in stroke hemiplegia
2. Bilateral damage to the corticobulbar tracts This causes persistent weakness and spasticity of the
muscles supplied by the bulbar nuclei.
Bulbar & Pseudo bulbar palsy cont..
4

Presentation
◦ Tongue - paralysed, no wasting initially and no fasciculations; "Donald duck" speech; unable to protrude
◦ Palatal movements absent◦ Dribbling persistently◦ Facial muscles - may also be paralysed◦ Reflexes - exaggerated e.g. jaw jerk◦ Nasal regurgitation may be present◦ Dysphonic◦ Dysphagic◦ Emotional lability may also be present◦ There may also be neurological deficits in the limbs e.g.
increased tone, enhanced reflexes and weakness.
Pseudo bulbar palsy cont…
5

Causes◦ Cerebrovascular events e.g. bilateral internal capsule infarcts
◦ Demyelinating disorders e.g. multiple sclerosis
◦ Motor neurone disease◦ High brainstem tumours◦ Head injury◦ Neurosyphilis
Complications◦ Poor nutrition◦ Psychological dysfunction◦ Progression of underlying disease
Prognosis◦ This depends on the underlying cause.
Pseudo bulbar palsy cont…
6

Dysphagia, a Greek word that means disordered eating, is difficulty in eating as a result of disruption of the swallowing process. (Braddom p535)
Dysphagia is defined as a condition in which an individual has had an interruption in either eating function or the maintenance of nutrition and hydration (Buchholz, D)
Difficulty with eating which may include one or more of the following Chewing food swallowing solids and/or liquids coughing or chocking when eating food sticking in the throat or chest
(ASHA)
Dysphagia-definition
7
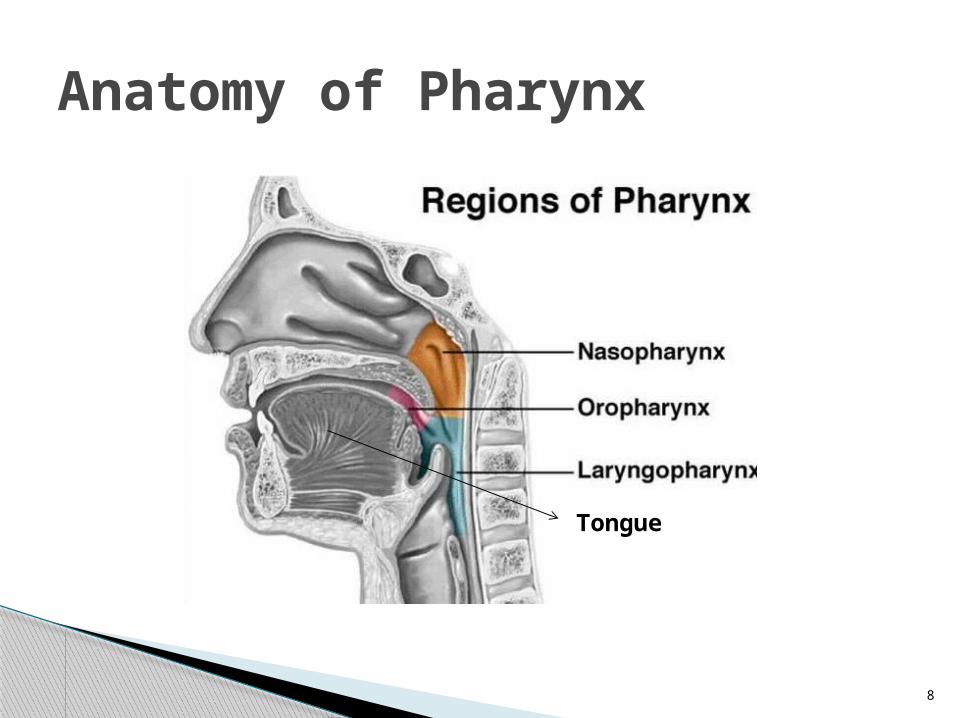
Anatomy of Pharynx
Tongue
8

Anatomy of Pharynx cont…
9

The Four phases of Swallowing
Oral Preparatory Phase Oral Phase Pharyngeal Phase Esophageal Phase
These 4 phases are dynamic and overlapping.
In general, they allowed food and liquid to
move from the mouth into the stomach
smoothly & Safely. (ASHA)
The Swallowing Process
10

Eating is anticipated
Food is brought to the mouth
◦ Bitten off
◦ Taken from the utensil
Food is chewed and mixed with saliva
Liquids are sipped or sucked through a
straw
Oral Preparatory Phase
11
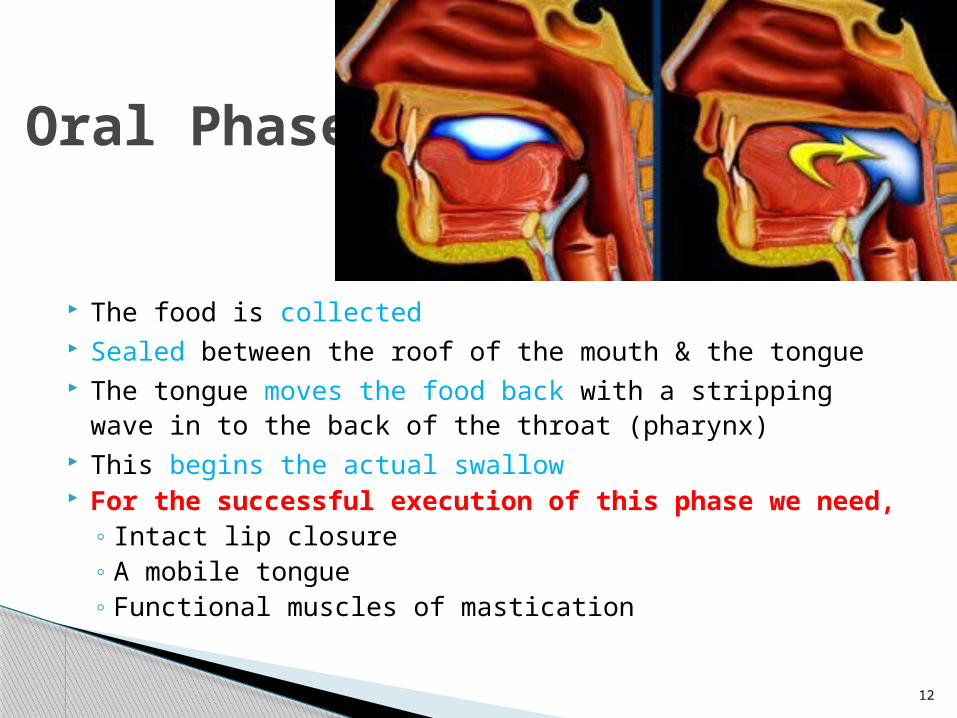
The food is collected Sealed between the roof of the mouth & the tongue The tongue moves the food back with a stripping wave in
to the back of the throat (pharynx) This begins the actual swallow For the successful execution of this phase we need,
◦ Intact lip closure◦ A mobile tongue◦ Functional muscles of mastication
Oral Phase
12

Soft palate elevates◦ Preventing food from escaping into the nose
Tongue base moves back to contact pharyngeal wall
Larynx (voice box) moves up and forward Epiglottis (top part of larynx) is tilted down
and back to guide the food past the airway.
Pharyngeal Phase
13

Breathing momentarily stops
Vocal cord comes together to further protect
airway
Muscles of the pharynx contract
◦ Moves the food towards the esophagus
◦ Upper esophageal sphincter relaxes
Food passes in to the esophagus.
Pharyngeal Phase cont…
14

Duration : 0.6 sec Aspiration is most likely to occur in this
phase Protection from laryngeal penetration and
aspiration is afforded in several ways;
◦ By folding of the epiglottis over the laryngeal opening
◦ By closure of vocal cords◦ By elevation and anterior displacement of larynx
Pharyngeal Phase cont…
15

Esophageal Phase• Peristalsis moves the
food through the esophagus
• The lower esophageal sphincter relaxes to allow the food to passes into the stomach• Duration: 6-10 sec
16

FLUROSCOPIC IMAGING OF NORMAL SWALLOWING
17

The most important images of the swallowing study are those taken of the lateral view.
1. The base of the tongue and the soft palate close the oral cavity posteriorly (arrow) to prevent spill of food into the open larynx.
2. Hyoid bone and base of the tongue move in a cranial direction and lift the larynx (arrow).
3. Soft palate elevates to prevent spill into the nasopharynx (thin arrow) and the larynx closes by contraction of the aryepiglottic folds (broad arrow)
4. Contraction of the upper pharyngeal constrictor (arrow)5. Contraction of the middle pharyngeal constrictor (arrow)6. Contraction of the lower pharyngeal constrictor and relaxation
of the cricopharyngeal muscle (arrow)7. Epiglottis elevates to regain its resting position and the larynx
opens.8. Epiglottis in resting position and larynx is open (arrow).
www.radiologyassistant.nl/en/440bca82f1b77
Fluoroscopic imaging cont…
18

The swallowing process requires the following elements:◦ Sensory input from the peripheral and central
nervous system Through V, VII, IX & X cranial nerves
◦ A coordinating center or centers Exact role of cerebral cortex is unknown The brain stem swallowing centers receive the input,
organize it in to programmed response and transmit the response.
◦ A subsequent motor response sent back through these systems. Through V, VII, IX, X & XII cranial nerves
Neurological control of swallowing
19

20

There are three types of swallowing disorder, divided on the basis of where the problem is occurring: ◦ Oral Dysphagia◦ Pharyngeal Dysphagia◦ Esophageal Dysphagia
Dysphagia Types
Oral or pharyngeal dysphagia Esophageal dysphagia
• Coughing or choking with swallowing
• Difficulty initiating swallowing• Food sticking in the throat• Drooling• Unexplained weight loss• Change in dietary habits• Recurrent pneumonia• Change in voice or speech• Nasal regurgitation
• Sensation of food sticking in the chest
• Oral or pharyngeal regurgitation
• Food sticking in the throat• Drooling• Unexplained weight loss• Change in dietary habits• Recurrent pneumonia
21

Based up on the cause there are 2 types;1. Mechanical Dysphagia
Dysphagia caused by a large bolus or luminal narrowing is called mechanical Dysphagia
2. Motor (Neuro muscular) Dysphagia Dysphagia due to weakness of peristaltic
contractions or to impaired deglutitive inhibition** causing nonperistaltic contractions and impaired sphincter relaxation is called motor dysphagia.
◦ ** Deglutitive inhibition: The inhibition that precedes the peristaltic contractions.
Causes of Dysphagia
22

MECHANICAL DYSPHAGIA◦ Luminal (Large bolus, foreign body etc...)◦ Intrinsic narrowing (Malignant/ Benign tumors, Webs
and rings etc…)◦ Extrinsic compression (Cervical spondylitis, Enlarged
thyroid gland etc…)
MOTOR (NEUROMUSCULAR) DYSPHAGIA◦ Difficulty in initiating swallowing reflex (Paralysis of the
tongue, Lack of saliva)◦ Disorders of pharyngeal and esophageal striated
muscle◦ Upper motor neuron lesions (pseudobulbar paralysis)◦ Disorders of esophageal smooth muscle
Causes of Dysphagia cont…
23

History◦ h/o dental disorders, recurrent pneumonia, cardio
pulmonary disease or cervicle ankylosis or spondylosis.
Examination◦ Cranial nerve testing (V, VII, IX, X & XII) & direct
observation of lip closure, jaw closure, tongue mobility and strength, palatal elevation & oral sensitivity.
◦ Level of alertness & cognitive status◦ Gag reflex [but an absent gag doesn’t implay the
inability to swallow safely (Logemann JA 1989)]◦ Chest Auscultation.
Clinical assessment
24

Examination◦ Diagnostic feeding assessment with various food texture.◦ “3-ounce Water Swallow Test”
This test has compared favorably with the video swallow in identifying aspiration
The 3-oz water swallow test is a sensitive screening tool for
identifying patients at risk for clinically significant aspiration
who need referral for more definitive modified barium swallow evaluation. (DePippo KL et al)
it has been shown that if the 3-ounce water swallow test is passed, diet recommendations can be made without further objective dysphagia testing. (Debra M. Suiter &
Steven B. Leder, 2008) CRITIQUE : The 3-oz water screen utilizing the cough reflex
as the sole indica tor of aspiration is not a replacement for
the precision and accuracy of a videofluoro scopic evaluation. (Bernard R. Garon)
Clinical assessment cont..
25

Laboratory Data◦ Routine lab tests◦ Pulse oximetry
Technical Assessment of Dysphagia◦ Videofluroscopy
Easy to use Less expensive Risk of Radiation-present
◦ Ultrasonography◦ CT and MRI◦ Endoscopy
Clinical assessment cont..
26

Videofluroscopy of Aspiration before swallowing
27

1. Notice that contrast enters the pharynx, but does not trigger a swallowing reflex.
2. No swallowing reflex3. Contrast reaches the hypopharynx, but still no swallowing
reflex.4. Contrast enters the larynx, which is still open and not yet
elevated 5. At this moment the swallowing reflex starts and the larynx
elevates6. Contrast is transported to the esophagus and the larynx
closes, but there is already contrast in the trachea.7. Proper relaxation of the cricopharyngeus and finally there is
good closure of the larynx.8. Notice that there is no stasis at the end of the swallow .
www.radiologyassistant.nl/en/440bca82f1b77
Videofluroscopy of Aspiration before swallowing
28

CLINICAL EVALUATION
29

Treatment of Dysphagia Dysphagia treatment rests on 5 principles
1. Amelioration of the underlying disease process2. Prevention of complications3. Improvement of swallowing via therapy4. Compensations to improve swallowing safety and
efficiency &5. Environmental modification
(Braddom 3ird edn)
Occupational Therapist: Evaluates and treats sensory and motor impairments and assesses prosthetic needs related to self-feeding and swallowing. (ASHA)
30
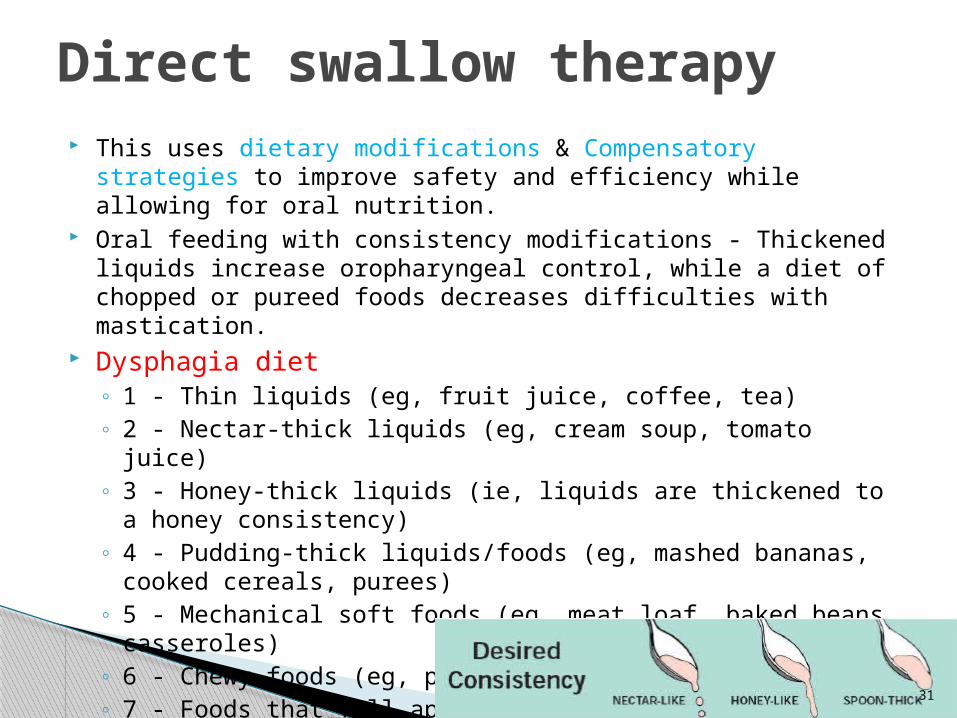
This uses dietary modifications & Compensatory strategies to improve safety and efficiency while allowing for oral nutrition.
Oral feeding with consistency modifications - Thickened liquids increase oropharyngeal control, while a diet of chopped or pureed foods decreases difficulties with mastication.
Dysphagia diet◦ 1 - Thin liquids (eg, fruit juice, coffee, tea) ◦ 2 - Nectar-thick liquids (eg, cream soup, tomato juice) ◦ 3 - Honey-thick liquids (ie, liquids are thickened to a honey
consistency) ◦ 4 - Pudding-thick liquids/foods (eg, mashed bananas, cooked
cereals, purees) ◦ 5 - Mechanical soft foods (eg, meat loaf, baked beans,
casseroles) ◦ 6 - Chewy foods (eg, pizza, cheese, bagels) ◦ 7 - Foods that fall apart (eg, bread, rice, muffins) ◦ 8 - Mixed textures
Direct swallow therapy
31

Compensatory strategies to reduce the risk of aspiration include the following: ◦ Chin tuck - The patient holds his/her chin down, increasing the
epiglottic angles, and pushes the anterior laryngeal wall backward, thereby decreasing the airway diameter.
◦ Head rotation - The ipsilateral pharynx is closed, forcing the food bolus to the contralateral pharynx while cricopharyngeal pressure is decreased.
◦ Head tilt - This technique uses gravity to guide the bolus to the ipsilateral pharynx.
◦ Supraglottic swallow - This technique involves simultaneous swallowing and breath-holding, closing the vocal cords and protecting the airway. The patient thereafter can cough to expel any residue in the laryngeal vestibule. The Valsalva maneuver may be used to maximize vocal cord closing.
◦ Mendelsohn maneuver - This maneuver is a form of supraglottic swallow in which the patient mimics the upward movement of the larynx by voluntarily holding the larynx at its maximum height to increase the duration of the cricopharyngeal opening.
Direct swallow therapy cont..
32

Common postural techniques & some indications for use
Compensatory technique
Indication
Chin tuck Reduced oral bolus control with aspiration before or during the swallow
Neck extension Impaired oral bolus propulsion
Head turn to weak side
Unilat. Pharyngeal weakness with retention after swallowing
Head tilt to weak side
Unilat. Oral & pharyngeal weakness
Reclining position Pharyngeal weakness with retention & overflow after swallowing
Supraglottic swallow In adequate or delayed closure of laryngeal aditus (entrance)
Effortful swallow Poor tongue based retraction
Mendoelsohn maneuver
Inadequate upper esophageal sphincter opening
Syringe feeding Impaired oral bolus propulsion
Alterating solids & liquids
Retention in the pharynx after swallowing
33

It involve the use of oral, pharyngeal, laryngeal, and respiratory exercises to improve flexibility, strength and co-ordination.◦ Biofeedback techniques are used to reeducate
muscles affected in facial palsy and disorders of articulation. Such techniques include EMG feedback, with surface electrodes placed over the anterior neck. Visual feedback is obtained in VFSS while experimentation with head positions and swallowing maneuvers is conducted.
◦ Thermal stimulations in the form of icing of the anterior faucial arches can be performed; this may help to decrease the delay of pharyngeal swallow
Indirect therapy technique
34

Common indirect therapy techniques
Therapy technique Description ORAL CAVITYOral motor control exercises (jaw, tongue, lip)
Jaw opening & closing. Tounge rotation, lateralization, protrusion, retraction. Lip protrusion, lateralization & opening-closing
Relaxation & ROM exs (jaw, tongue, lip)
Stretching & increasing ROM
Resistance exercise (jaw, tongue, lip)
Opening closing jaw against resistance. Pushing the tongue against resistance
PHARYNXLaryngeal elevation exs
Volitional laryngeal elevation by saying a high pitched ‘ee’
Vocal cord adduction exs By uttering ‘ah’ simultaneously
Masako maneuver Swallowing with the tongue tip held anteriorly outside the mouth
Sensory stimulation Tactile stimulation of the faucial arches with cold or sour stimuli
UPPER ESOPHAGEAL SPHINCTER OPENINGShaker exs
Active head rising (neck flexion) in the supine position
Upper esophageal sphincter dialatation
Expansion of balloon catheter in the upper esophageal sphincter
35

Botulinum toxin type A is injected endoscopically into the gastroesophageal sphincter and upper esophagus to decrease tone. This could be very useful in cricopharyngeal spasms causing dysphagia.13,15
Diltiazem can aid in esophageal contractions and motility, especially in the disorder known as the nutcracker esophagus.
Glucagon is used in disimpacting esophageal bodies; diazepam also is sometimes used. No major study has proven their effectiveness.
Cystine-depleting therapy with cysteamine is the treatment of choice for patients with dysphagia due to pretransplantation or posttransplantation cystinosis.16
Nitrates can be recommended, especially isosorbide dinitrate in achalasia.
Medical interventions
36

◦ Esophageal dilatation in achalasia, strictures, and webs
◦ Cervical osteophyte resection ◦ Cricopharyngeal myotomy for upper esophageal
spasm◦ Esophageal resection and reanastomosis ◦ For paralyzed vocal cords, Teflon injection or
reversible vocal cord medialization can be performed.
◦ In recurrent pneumonia, cuffed tracheostomy sometimes is performed to protect the airway.
◦ Laryngectomy or laryngotracheal diversion also may be indicated, as for tracheostomy, and often is performed as a permanent palliative measure when all else has failed.
Endoscopic and surgical interventions
37
Psychological factors
Environmental factors
Hygienic considerations
Other considerations
38

THANK YOU…
39

















