75
DYSPNEA Muhammad Fachri
| Date post: | 13-Dec-2015 |
| Category: |
Documents |
| Upload: | zulfa-n-fath |
| View: | 235 times |
| Download: | 0 times |

DYSPNEADYSPNEA
Muhammad Fachri

Dyspnea:
• Discomfort feeling in breathing
• Subjective and difficult to measure
• Etiology : lung, heart, endocrine, kidney, neurology, hematology, rheumatology and psichology
• Prevalens of dispnea → no accurate data
INTODUCTION
1

DEFINITION OF DYSPNEA
The American Thoracic Society (ATS):
the term of discomfort perception subjective in breathing that consist of sensation with different intensity as a results of interaction of various physiologic, social and environtmental factors.
3

MECHANISM OF DYSPNEA
• Interaction between signal and receptor in otonomic nerve system, motoric cortex,airway receptor, lung and thoracic cage →dyspnea
4


MECHANISM OF DYSPNEA

MECHANISM OF DYSPNEA
Dyspnea
Complex of breathing
Lung and thoracic cage
CognitiveBehavior
Emotion
Chemoreceptor stimulation
Exercise
Primary motoric cortex
Primary sensoric cortex

AIRWAY SYSTEM

AIRWAY SYSTEM

MEASURE OF DYSPNEA• Aim : to differentiate the severity and to
evaluate the nature of dyspnea • Technique of measuring :
– visual analogue scale– Borg scale– Medical research council (MRC) dyspnea scale– American thoracic sosiety (ATS) dyspnea scale – baseline dyspnea index (BDI) – transitional dyspn index (TDI)

ATS dyspnea index• Grade 1 : No dyspnea except severe exercise activity • Grade 2 : Dyspnea when climb the step in hurry or climb a small hill • Grade 3 : Walk slower compared to common people• Grade 4 : Must stop for breathing after 100 yard walk• Grade 5 : Dyspnea while puput on / off the clothes

Dyspnea
pulmonary non-pulmonary
(cardiac)
*pulm edema *arrhythmias
*asthma/COPD *acute MI
*Pleural effusion
*myocardial ishemia
*pneumonia
*pneumothorax

DYSPNEA IN PULMONARY DISEASE
• Abnormality of breathing mechanism, lung become more stiff, weakness of ventilation muscles.
• Restrictive lung diseases.
• Obstructive lung diseases.
• Disturbance of lung diffusion.
• Disturbance of lung perfusion.

RESCTIVE LUNG DISEASE
• Lung : - atelectasis - fibrosis - lung tumour - bulla - lung abscess - pulmonary edema
• Mediastinum : - mediastinal tumour - cardiomegali - pericardial effusion
RESCTIVE LUNG DISEASE
• Pleura : - pleural effusion - pleural tumour - pneumothorax • Diaphragm : - hernia of diaphragm - paralize of diaphragm• Bone : - rib fracture - pectus excavatum - scoliosis, kyphosis• Muscle : - miasthenia gravis

ARDS

PNEUMONIA

ATELECTASIS

DESTROYED LOBE

LUNG ABSCES

BULLA

BULLA

MILIARY TB

NODUL IN THE LUNG
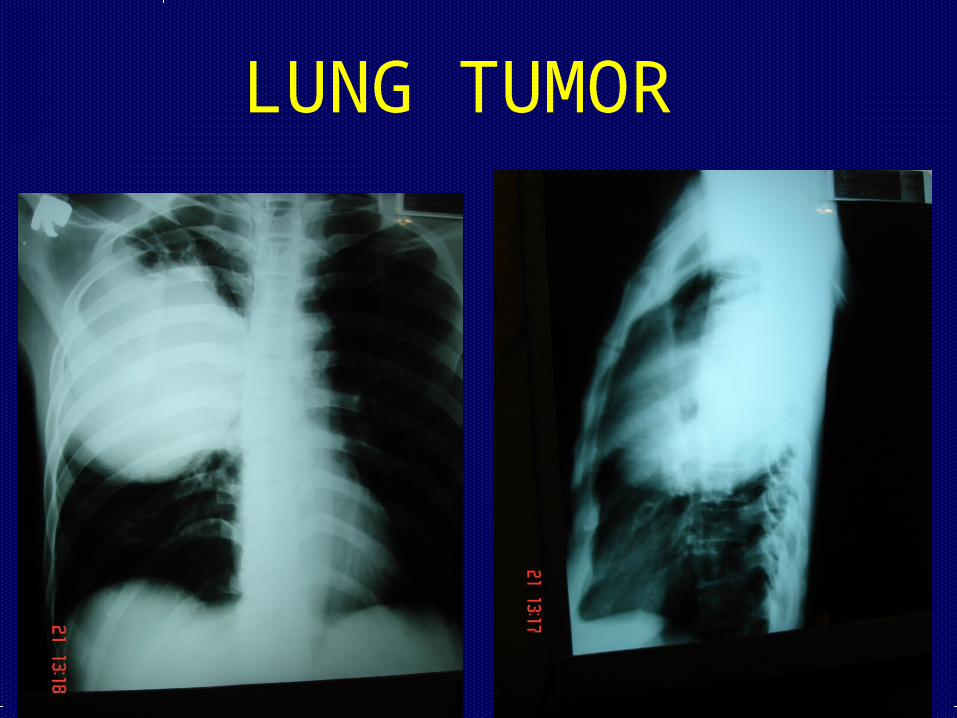
LUNG TUMOR

PANCOAST TUMOR
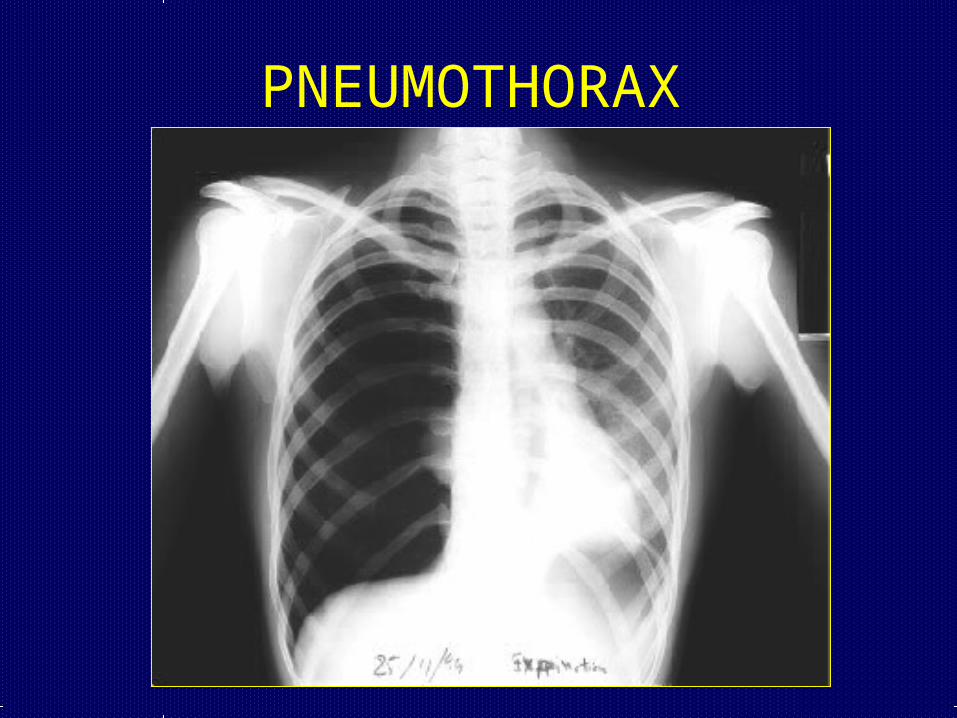
PNEUMOTHORAX

HYDROPNEUMOTHORAX

OBSTRUCTIVE LUNG DISEASE
• Asthma
• COPD : - chronic bronchitis
- emphysema
• Bronchiectasis
• Lung tumour
• Foreign body

EMPHYSEMA

NormalNormal HyperinflationHyperinflation
Air trappingAir trapping

BRONCHIECTASIS

BRONCHIECTASIS

BRONCHIECTASIS

BRONCHIECTASIS

BRONCHIECTASIS

BRONCHIECTASIS

BRONCHIECTASIS

Lung Cancer

TUMOR IN THE AIRWAY

LUNG CANCER

DISTURBANCE OF DIFFUSION
• Alveolar wall
• Interstitial space
• Arterial wall
• Plasma
• Red blood cell wall

DISTURBANCE OF PERFUSSION
• Pulmonary emboli
• Congestive heart failure

Dyspnea
• Subjective sensation of: – Difficult, labored breathing or– Shortness of breath

Hyperventilation Syndrome
• Response to stress, anxiety
• Patient exhales CO2 faster than metabolism produces it
• Blood vessels in brain constrict
• Anxiety, dizziness, lightheadedness
• Seizures, unconsciousness

Hyperventilation Syndrome
• Chest pains, dyspnea
• Numbness, tingling of fingers, toes, area around mouth, nose
• Carpopedal spasms of hands, feet

Hyperventilation Syndrome
• Treatment– Obtain thorough history– Avoiding misdiagnosis is critical– Try to “talk patient down”
– Re-breathe CO2 from face mask with oxygen flowing at 1 to 2 liters/minute

Upper Airway
• Foreign Body Obstruction
• Pharyngeal Edema
• Croup
• Epiglottitis

Foreign Body Obstruction
• Partial or complete
• Most common cause of pediatric airway obstruction

Foreign Body Obstruction
• Suspect in any child with – Sudden onset of dyspnea– Decreased LOC
• Suspect in any adult who develops dyspnea or loses consciousness while eating

Foreign Body Obstruction
• Management– Partial with good air exchange– Partial with poor air exchange– Complete

Lower Airway
• Asthma
• Chronic Obstructive Pulmonary Disease– Chronic bronchitis– Emphysema

Asthma
• Reversible obstructive pulmonary disease
• Episodic, family history, trigger factor
• Younger person’s disease (80% have first episode before age 30)
• Lower airway hypersensitive to allergens, emotional stress, irritants, infection

Asthma
• Bronchospasm
• Bronchial edema
• Increased mucus production, plugging
Resistance to airflow, work of breathing increase

Asthma
• Airway narrowing interferes with exhalation
• Air trapped in chest interferes with gas exchange
• Wheezing, coughing, respiratory distress

Asthma
• All that wheezes is not asthma
• Other possibilities– Pulmonary edema– Pulmonary embolism– Anaphalaxis (severe allergic reaction)– Foreign body aspiration– Pneumonia

Asthma
• Treatment– High concentration O2, humidified
– Position of comfort– Assist ventilation as needed– Bronchodilators via small volume nebulizer– Antiinflammatory drugs (e.g. Corticosteroid)– Calm patient, reassure

Chronic Obstructive Pulmonary Disease
• Chronic Bronchitis
• Emphysema

Chronic Bronchitis
• Chronic lower airway inflammation– Increased bronchial mucus production– Productive cough
• Urban male smokers > 30 years old

Chronic Bronchitis
• Mucus, swelling interfere with ventilation
• Increased CO2, decreased 02
• Cyanosis occurs early in disease• Lung disease overworks right ventricle• Right heart failure occurs• Right Heart Failure produces peripheral edema
Blue Bloater

Emphysema
• Loss of elasticity in small airways
• Destruction of alveolar walls
• Urban male smokers > 40-50 years old

Emphysema
• Lungs lose elastic recoil
• Retain CO2, maintain near normal O2
• Cyanosis occurs late in disease• Barrel chest (increased AP diameter) • Thin, wasted• Prolonged exhalation through pursed lips
Pink Puffer

COPD
• Prone to periods of “decompensation”• Triggered by respiratory infections, chest trauma• Signs/Symptoms
– Respiratory distress– Tachypnea– Cough productive of green, yellow sputum

COPD Management
• Oxygen– Monitor carefully– Some COPD patients may experience
respiratory depression on high concentration oxygen
• Assist ventilations as needed

COPD Management
• If wheezing present, aerosol bronchodilators via nebulizer

Alveolar Function Problems

Pulmonary Edema
• Fluid in/around alveoli, small airways
• Causes– Left heart failure– Toxic inhalants– Aspiration– Drowning– Trauma

Pulmonary Edema
• Signs/Symptoms– Labored breathing– Coughing– Rales, rhonchi– Wheezes– Pink, frothy sputum

Pulmonary Edema
• Signs/Symptoms– Sit up
– High concentration O2
– Assist ventilation

Pulmonary Embolism
• Clot from venous circulation
• Passes through right heart
• Lodges in pulmonary circulation
• Shuts off blood flow past part of alveoli

Pulmonary Embolism
• Associated with:– Prolonged bed rest or immobilization– Casts or orthopedic traction– Pelvic or lower extremity surgery– Phlebitis– Use of BCPs

Pulmonary Embolism
• Signs/Symptoms– Dyspnea– Chest pain– Tachycardia– Tachypnea– Hemoptysis
Sudden Dyspnea + No Readily Identifiable Cause = Pulmonary Embolism

Pulmonary Embolism
• Management– Oxygen– Assisted ventilation– Transport

CONCLUSION
• Dyspnea is subjective symptom
• Various abnormalities may cause dyspnea
• Diagnosis should be establisherd properly
• Severity of dyspnea can be measured
• Oxygen may be administered initially
• Definitive treatment based on the etiology


















