356 | Healio.com/Pediatrics PEDIATRIC ANNALS 41:9 | SEPTEMBER 2012 Healthy Baby Practical advice for treating newborns and toddlers. Put Some ‘Teeth’ into Your Pediatric Preventive Counseling Stan L. Block, MD, FAAP A ccording to Pediatrics, the ca- pacity of dentists capable or willing to see Medicaid-insured children younger than 3 years of age is significantly limited. However, dental caries caused by Streptococcus mutans are among the most common chronic bacterial infections found in early child- hood. 1 Consider the following: only 14 of 39 states had more than 50% of dentists who treat Medicaid-insured children, 33.3 million children live in an area with a shortage of dental care professionals, and about 10% of all children, regardless of insurance coverage, never see a den- tist. 1 Pediatric dental surgery is now the most common outpatient procedure in many Canadian pediatric hospitals. 2 Early childhood dental caries (ECC) also create a tremendous demand on our nation’s resources for pediatric re- storative and dental surgical care. In addition, the costs of ECC, such as for general anesthesia, a dental surgeon, out- patient services, etc., and the months or even years of horrendous daily oral pain (see Figure 1 [above] and Figure 2, page 357) are considerable. 2 OUR ROLE IN PREVENTIVE DENTAL CARE From 1999 to 2002, as many as 11% of children in the United States ages 1 to 3 years, 3 and 41% of children ages 2 to 11 years, had ECC in their primary teeth. 4 The two best predictors of ECC in a child’s primary teeth were parents with lower educational achievement and lower socioeconomic status. 3 However, in the last few years, I have seen the lo- cal rate of patients on Medicaid soar from 30% to nearly 55% as a result of recent economic hardships; thus, socio- economic status may not be as relevant a risk factor. In pediatric offices, most children between the ages of 9 months and 36 months are seen an average of five to six times annually for their well-visits and a multitude of other complaints. These patients all have or will soon have teeth. These visits provide an opportunity to Figure 1. A 5-year-old girl was seen in our office by the nurse practitioner who was unsure whether this was a mucocele. The child alleged the lesion was not painful. Further inspection of the teeth provide clues to the diagnosis (see Figure 2, page 357). All images courtesy of Stan L. Block , MD, FAAP. Reprinted with permission. Stan L. Block, MD, FAAP, is Professor of Clinical Pediatrics, University of Louisville, and University of Kentucky, Lexington, KY; President, Kentucky Pedi- atric and Adult Research Inc.; and general pediatri- cian, Bardstown, KY. Address correspondence to Stan L. Block, MD, FAAP, via email: [email protected]. Disclosure: Dr. Block has disclosed no relevant financial relationships. doi: 10.3928/00904481-20120827-05
Transcript
356 | Healio.com/Pediatrics PEDIATRIC ANNALS 41:9 | SEPTEMBER 2012
Healthy BabyPractical advice for treating newborns and toddlers.
Put Some ‘Teeth’ into Your Pediatric Preventive Counseling Stan L. Block, MD, FAAP
According to Pediatrics, the ca-pacity of dentists capable or willing to see Medicaid-insured
children younger than 3 years of age is significantly limited. However, dental caries caused by Streptococcus mutans are among the most common chronic bacterial infections found in early child-hood.1
Consider the following: only 14 of 39 states had more than 50% of dentists who treat Medicaid-insured children, 33.3 million children live in an area with a shortage of dental care professionals, and about 10% of all children, regardless of insurance coverage, never see a den-tist.1 Pediatric dental surgery is now the most common outpatient procedure in many Canadian pediatric hospitals.2
Early childhood dental caries (ECC) also create a tremendous demand on our nation’s resources for pediatric re-storative and dental surgical care. In addition, the costs of ECC, such as for general anesthesia, a dental surgeon, out-
patient services, etc., and the months or even years of horrendous daily oral pain (see Figure 1 [above] and Figure 2, page 357) are considerable.2
OUR ROLE IN PREVENTIVE DENTAL CARE
From 1999 to 2002, as many as 11% of children in the United States ages 1 to 3 years,3 and 41% of children ages 2 to 11 years, had ECC in their primary teeth.4 The two best predictors of ECC in a child’s primary teeth were parents with lower educational achievement and
lower socioeconomic status.3 However, in the last few years, I have seen the lo-cal rate of patients on Medicaid soar from 30% to nearly 55% as a result of recent economic hardships; thus, socio-economic status may not be as relevant a risk factor.
In pediatric offices, most children between the ages of 9 months and 36 months are seen an average of five to six times annually for their well-visits and a multitude of other complaints. These patients all have or will soon have teeth. These visits provide an opportunity to
Figure 1. A 5-year-old girl was seen in our office by the nurse practitioner who was unsure whether this was a mucocele. The child alleged the lesion was not painful. Further inspection of the teeth provide clues to the diagnosis (see Figure 2, page 357).
All i
mag
es c
ourte
sy o
f Sta
n L.
Blo
ck ,
MD,
FAA
P. R
eprin
ted
with
per
mis
sion
.
Stan L. Block, MD, FAAP, is Professor of Clinical
Pediatrics, University of Louisville, and University of
PEDIATRIC ANNALS 41:9 | SEPTEMBER 2012 Healio.com/Pediatrics | 357
start our patients on the road to a lifetime of good dental hygiene, and habits they will likely teach their own children.
To do this, we need to add routine dental counseling to most well-visits af-ter age 6 months (see Sidebar, page 358).
THE ‘ROOT’ OF DENTAL CARIESECC is a consequence of the interac-
tion between normal bacterial oral flora, and dietary fermentable sugars. The oral flora create a sticky biofilm, known as dental plaque, that ferments sugar into an acidic substance that erodes the den-tal enamel over time (see Figure 3 and Figure 4). Although only a few oral bacterial species are highly associated with dental plaque, the major culprit is S. mutans. Chronic consumption of sug-ary foods and liquids will continually recharge the plaque matrix.4
ECC PREVENTION Based upon the latest recommenda-
tions from the American Academy of Pediatrics (AAP),2,4,5 and 30 years of my own pediatric practice, the following are my cardinal rules of pediatric (and ado-lescent) dental care once primary teeth have fully erupted.
Limit Caregiver Disease OriginsOne method of primary prevention is
to reduce infant exposure to the caregiv-er’s adverse dental flora during the time of the infant’s first dental eruptions. We could ask the caregiver to refrain from sharing cups and utensils, premasticat-ing the child’s food, and from cleaning the pacifier with his or her own mouth.
Modification of DietThe following three practices will
greatly reduce the incidence of ECC in children: 1) avoid all juices and sugary beverages, except for on special oc-casions; 2) avoid day-long “grazing” on starchy cereals and first foods; and
3) always have the child sit at the kitch-en table to eat or drink; this reduces the
temptation to over-indulge on sweet drinks and foods.
Healthy Baby
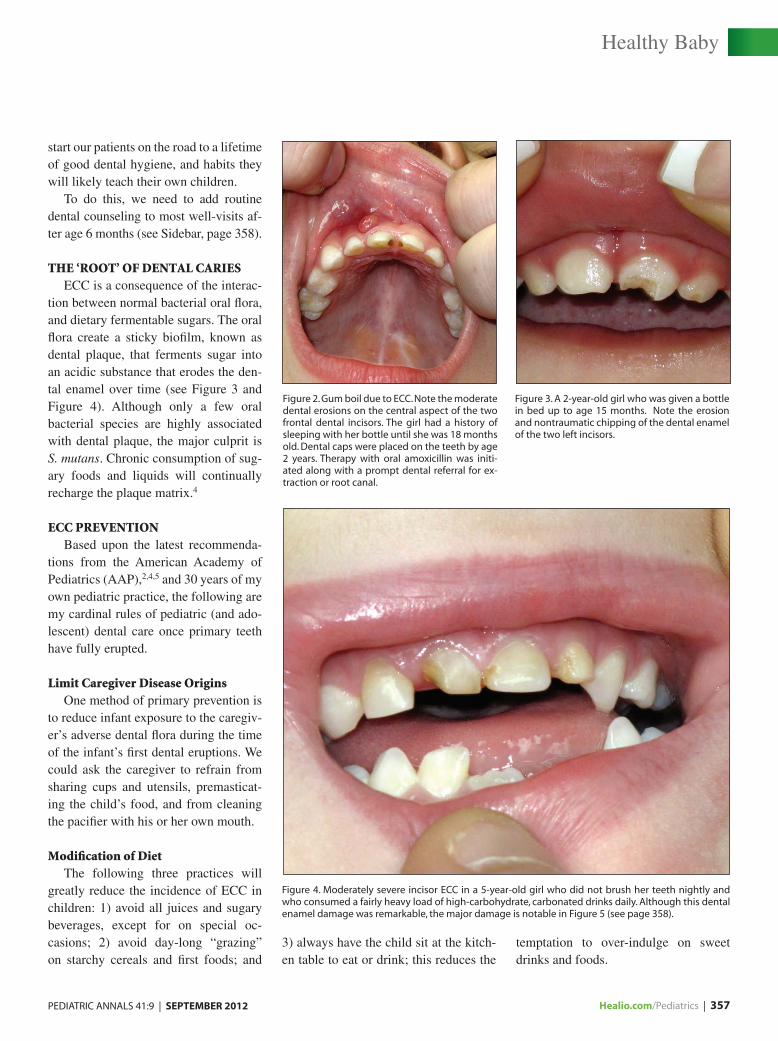
Figure 2. Gum boil due to ECC. Note the moderate dental erosions on the central aspect of the two frontal dental incisors. The girl had a history of sleeping with her bottle until she was 18 months old. Dental caps were placed on the teeth by age 2 years. Therapy with oral amoxicillin was initi-ated along with a prompt dental referral for ex-traction or root canal.
Figure 3. A 2-year-old girl who was given a bottle in bed up to age 15 months. Note the erosion and nontraumatic chipping of the dental enamel of the two left incisors.
Figure 4. Moderately severe incisor ECC in a 5-year-old girl who did not brush her teeth nightly and who consumed a fairly heavy load of high-carbohydrate, carbonated drinks daily. Although this dental enamel damage was remarkable, the major damage is notable in Figure 5 (see page 358).
358 | Healio.com/Pediatrics PEDIATRIC ANNALS 41:9 | SEPTEMBER 2012
Good Oral Hygiene AdherenceA child’s teeth should be brushed
twice daily, particularly at night before bed time. Beginning this ritual before the child is 12 months old will spare most parents a nightly battle. Using an electric tooth brush confers distinct advantages over manual brushing because it more thoroughly covers all dental surfaces,5 even if the child does not cooperate. An electric tooth brush is also an interesting “toy” and a good distraction for the tod-dler. I recommend an electric toothbrush that has a distinct on/off switch. I also recommend that immediately before or
after the child brushes his or her own teeth, an adult should brush the teeth until the child is at least 6 years old. Den-tal flossing of children’s teeth is advised, but I pick my “battles” with young chil-dren, and flossing is less important than nightly and morning brushing of teeth.
Once the teeth are brushed at night, never allow the child anything to eat or drink, except water, until the next morn-ing (see Figure 3 and Figure 4, page 257). This applies to breast milk as well, because “it may become cariogenic when combined with other carbohydrate sources.”4 If the child ingests anything besides water at night, the teeth must be brushed again. If the child sneaks food at night after everyone else has gone to bed, the parent should lock the refrigera-tor and/or cabinets at nights.
Remember that saliva, which is highly protective for teeth, is minimally produced during sleep. A morning teeth brushing is optimal, too, according to the American Academy of Pediatric Dentists (APDA).5,6
Fluoride AdministrationAt home: I advocate the supervised
use of fluoride toothpaste for all chil-dren older than 12 months. For those
children between 12 and 24 months, I suggest using merely a small smear or rice-sized grain of toothpaste on a soft (electric) toothbrush. For children older than 24 months, use a pea-sized amount of toothpaste.4-6 These are the current recommendations by the AADP and the AAP for children on Medicaid and for “high-risk” children.
Although this advice may seem somewhat controversial for toddlers (because of concerns over ingestion of too much fluoride), in my opinion, the “high-risk” dental state is nearly univer-sal.7 Most toddlers consume fruit drinks, soda pop, and sugared and nonsugared high-carbohydrate cereals more than three times a day, and many also have parents or siblings with cavities.5
This “grazing” on food during the day is now the apparent norm. Just look at the sweet-drink “sippy cup” spills and the crumbs that accumulate on your of-fice’s waiting room floor by the end of the day.
In the office: Fluoride varnishes should be applied twice annually in the office by the pediatrician’s staff for all children who have teeth who are 9 months to 3 years old and covered by Medicaid. These applications are asso-
Healthy Baby
Figure 6. This 3-year-old boy had severe ECC of the upper frontal incisors, characteristic of his re-ceiving a bottle or a “sippy cup” nightly, despite brushing his teeth. Also note the white chalky appearance on the enamel of the right front inci-sor, which is indicative of ECC.
Figure 5. Severe erosion of the two posterior molars in this 5-year-old girl (described in Figure 4, see page 357). She required extensive caps and dental restoration, along with prolonged general anesthe-sia for the dental procedure.
SIDEBAR.
Quick Q&A for Dental Screening
Does your child:
• Brush his or her teeth every night?
• Ingest any food or drinks (other than
water) after the night-time brushing?
• Take a bottle or cup to bed (or breast-
feed during the night)?
• Drink more than 4 ounces of sweetened
drinks, including juice, daily?
• Eat starchy snacks more than three times
a day?
Source: Block SL
PEDIATRIC ANNALS 41:9 | SEPTEMBER 2012 Healio.com/Pediatrics | 359
ciated with a 17% to 49% reduction in ECC, are easy for office staffs to per-form, and the Medicaid payments are worthwhile.2,4,8 However, commercial insurance does not reimburse medical offices for this procedure.
A primer on fluoride varnish proce-dure for the pediatrician’s office was written by Close and colleagues8 in 2010, but we have been performing these applications successfully and eas-ily in our office for years.
Role of NutritionReducing both the amount of sugar a
child consumes and the frequency of its intake is critical for better dentition. For that reason, I also recommend that chil-dren have no juice, but if they do, then no more than 4 ounces of juice daily.4,5,9
Instead, children should have 16 to 32 ounces of milk daily and all the fluo-ridated tap (not bottled) water they want. If parents balk at being told not to give their kids juice, you can also inform them that juice is a notable culprit in the obesity struggle, even if the label says “fruit” juice, which parents often think means it is “healthy.”
For instance, ingestion of 32 ounces of juice daily may comprise nearly 400 calories — or about 40% of a younger child’s recommended daily caloric in-take. Thus, depending on his or her me-tabolism, these extra sugar calories can increase the child’s risk of obesity if the child still consumes a typical caloric diet, or may create a finicky eater, as the child might forgo other essential calories and nutrients.
According to the AAP, sucrose is the most cariogenic sugar because it can form glucan, which enables bacte-rial adhesion.4 Cereals and starchy chips are also cariogenic. The child who fre-quently eats carbohydrate-laden snacks is definitely at increased risk for ECC.
I have parents check the cereal labels carefully for percentage of calories due to added sucrose.
THE PEDIATRIC DENTAL HOME The general dentists in my local area
usually prefer to see children only after age 3 years. By contrast, the AAP den-tal consortium recommends dental visits for all children as early as 12 months. This may be because of a study conduct-ed in the 1990s that associated early pre-ventive dental visits with reduced dental costs.10
However, this recommendation is currently quite impractical in light of the limited number of dentists nationally who will: see Medicaid patients; be able to perform any restorative procedures for ECC; or routinely and frequently dis-cuss with families many of the necessary preventive dental issues mentioned here.
More recent data have indicted that, in light of the limited number of dentists available to biannually assess children younger than 3 years, implementing a pediatrician-first screening policy “will decrease untreated decay under most plausible circumstances” more than a dentist-only policy does.3
A pediatrician-first screening/referral policy consists of an ECC risk assess-ment using patient and family history; physical screening of toddler’s dentition; and referring at-risk children. If the pedi-atric office incorporates bi-annual dental varnishes into their approach, the rate of ECC can be reduced in high-risk chil-dren on Medicaid by 17% to 49%.2,4,8
CONCLUSIONIn most states, each child must see a
dentist to enter school. However, here in rural Kentucky, my patients who are 9 to 36 months old have minimal access to a full-time pediatric dentist, as the clos-est one is at least 25 miles away. Thus,
our practice uses the pediatrician-first screening approach.
Consequently, we refer any child younger than age 4 years who adheres poorly to any one of my cardinal rules of primary dentition, or has any hint of ECC — from chalky white spots to small brown erosions (see Figure 5 and Figure 6, page 358) to overt cavitations.
In my opinion, most ECC could be prevented if general pediatricians would routinely stress the vital importance of early routine teeth brushing and avoid-ance of sugary drinks and “grazing” on carbohydrates.1
REFERENCES 1. Hakim RB, Babish JD, Davis AC. State
of dental care among Medicaid-enrolled children in the United States. Pediatrics. 2012;130(1):5-14.
2. American Academy of Pediatrics. Early childhood caries in indigenous communities. Pediatrics June 20, 2012 pp. 1190-1199.
3. Jones K, Tomar SL. Estimated impact of com-peting policy recommendations for age of first dental visit. Pediatrics. 2005;115(4):906-914.
4. American Academy of Pediatrics. Preventive oral health interventions for pediatricians. Pe-diatrics. 2008;22(6):1387-1394.
5. American Academy of Pediatrics. A Pediatric Guide to Children’s Oral Health. Elk Grove Village, IL: American Academy of Pediatrics; 2009.
6. Ameican Academy of Pediatric Dentistry. Guideline on Fluoride Therapy. Avail-able at: www.aapd.org/media/Policies_Guidelines/G_FluorideTherapy.pdf. Accessed Aug. 15, 2012.
7. Heifetz SB, Horowitz HS. Amounts of fluo-ride in self-administered dental products: safety considerations for children. Pediatrics. 1986;77(6):876.
8. Close K, Rozier RG, Zeldin LP, Gilbert AR. Barriers to the adoption and implementation of preventive dental services in primary medi-cal care. Pediatrics. 2010;125(3):509-517.
9. Marshall TA, Levy SM, Broffitt B, et al. Den-tal caries and beverage consumption in young children. Pediatrics. 2003;112(3):e184-e191.
10. Savage MF, Lee JY, Kotch JB, Vann WF. Early preventive dental visits: effects on subsequent utilization and costs. Pediatrics. 2004;114(4):e418-e423.
Healthy Baby
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.