Early Decrease in Minimal Luminal Diameter After Successful Percutaneous Transluminal Cwonary A $ia&y te stenosis Alfredo Rodriguez, MD, Omar Santaera, MD, Miguel Larribeau, MD, Maria I. Sosa, MD, and lgor F. Palacios, MD Eightyeight patients underwent serial coronary ar- teriography before, immediately after, 24 hours after and 7 * 2 months after successful percuta- neous transluminal coronary angioplasty (PTCA) of 102 lesions. Severity of coronary obstruction was measured using quantitative digital angiom phy. Three groups of lesions were defined when comparing angiograms recorded immediately after and 24 hours after PTCA: #oup I - lesions with either no change or 510% increase in arterial di- ameter stenosis after PTCA (n = 71); group II - le- sions with ~20% increase in diameter stenosis after PTCA (n q 19); and group Ill - patients with total occlusion (n q 12). There were no significant differences in the severity of stenosis before or immediately after PTCA among the 3 groups of k+ sions. Twenty-four hours after PTCA the diameter stenosis was 14.2 + 6.3% in group I, 34.7 f 6.1% in group II and 100 in group Ill (p <O.OOOl). At 7.1 & 2 months after PTCA the diameter stenosis was 21.2 -+ 16.6% in group I, 61.3 -I- 1.1% in group II, and 96.5 -t 1.3% in group Ill (p <O.OOOl). Resten* sis (250% stenosis diameter) at follow-up per k+ sion was significantly greater in group II than in group I (73.6 vs 9.8%) (p <O.OOOl). Thus, early an- giographic study after successful PTCA stratifies lesions into angiographic subsets with low (group I) and high (group II) risk of coronary restenosis. (Am J Cardiol1993;71:1391-1395) From the Division of Cardiology, Anchorena Hospital, Buenos Aires, Argentina; Massachusetts General Hospital, and Harvard Medical School, Boston, Massachusetts. Manuscript received October 1.5,19Y2; revised manuscript received January 15, 1993, and accepted January 17. Address for reprints: Igor F. Palacios, MD, Cardiac Unit, Massa- chusetts General Hospital, Fntit Street, Boston, Massachusetts 02114. P ercutaneous transluminal coronary angioplasty (PTCA) is a widely accepted alternative method for treating patients with coronary artery disease. Although PTCA results in a good immediate angio- graphic and clinical outcome in most patients, the long- term success of this procedure is limited by the resteno- sis of the treated artery. lil Restenosis occurs more fre- quently between the second and sixth months after PTCA. Radionuclide”-s and angiographic studies have showngp-‘2 that a significant number of patients have re- stenosis early -before the end of the tist month and even on the first week after PTCA. Little is known about the role of early coronary angiography as a guideline to determine the early and late outcome in patients after successful PTCA. We addressed this issue by per- forming a prospective study in 88 patients who under- went early (24 hours) and late (7 I!I 2 months) coronary angiography after successful PTCA. METHODS Between November 1, 1988 and May 15, 1989, 111 consecutive patients underwent PTCA of 145 lesions at the Anchorena Hospital, Buenos Aires, Argentina. PTCA was successfulin 98 patients (88.2%). A successfulout- come was defined as >20% change in the percentageof stenosis and a residual stenosis of <50% of the vessel lumen after PTCA, with no major complication occur- ring during hospitalization. Patients were examined angiographically before, immediately after, 24 hours after and at 7 f 2 months after PTCA. Coronary stenoses were determined using digital quantitative analysis. Sequential high-quality angiograms adequate for dig- ital quantitative analysis were obtained in only 88 of the 98 patients. They are the subject of this study. There were 13 women and ‘7.5 men, mean age 54 1: 3 years (range 38 to 78) (Table I). Forty-five (51.1%) had stable angina, 36 (40.9%) had unstable angina and 7 (8%) had acute myocardial infarction. Angioplasty procedure: All patients received aspirin and dipyridamole starting at least 1 day before PTCA. After arterial access, systemic heparinizationwas achieved by the intravenous administration of a bolus dose of 10,000 IU of heparin. Patients received a continuous in- fusion of intravenous nitroglycerin and heparin during PTCA. PTCA was performed using the standard tech- nique. Final angiographic outcome after PTCA was ob- tained by orthogonal angiographic views of the dilated vessel recorded immediately after the last balloon i&la- tion. After PTCA, medical treatment up to the 24-hour repeat study consisted of systemic heparinization, calci- PERCUTANEOUS TRANSLUMINAL CORONARY ANGIOPLASTY 1391
Transcript
Early Decrease in Minimal Luminal Diameter After Successful Percutaneous Transluminal
Cwonary A $ia&y te stenosis Alfredo Rodriguez, MD, Omar Santaera, MD, Miguel Larribeau, MD,
Maria I. Sosa, MD, and lgor F. Palacios, MD
Eightyeight patients underwent serial coronary ar- teriography before, immediately after, 24 hours after and 7 * 2 months after successful percuta- neous transluminal coronary angioplasty (PTCA) of 102 lesions. Severity of coronary obstruction was measured using quantitative digital angiom phy. Three groups of lesions were defined when comparing angiograms recorded immediately after and 24 hours after PTCA: #oup I - lesions with either no change or 510% increase in arterial di- ameter stenosis after PTCA (n = 71); group II - le- sions with ~20% increase in diameter stenosis after PTCA (n q 19); and group Ill - patients with total occlusion (n q 12). There were no significant differences in the severity of stenosis before or immediately after PTCA among the 3 groups of k+ sions. Twenty-four hours after PTCA the diameter stenosis was 14.2 + 6.3% in group I, 34.7 f 6.1% in group II and 100 in group Ill (p <O.OOOl). At 7.1 & 2 months after PTCA the diameter stenosis was 21.2 -+ 16.6% in group I, 61.3 -I- 1.1% in group II, and 96.5 -t 1.3% in group Ill (p <O.OOOl). Resten* sis (250% stenosis diameter) at follow-up per k+ sion was significantly greater in group II than in group I (73.6 vs 9.8%) (p <O.OOOl). Thus, early an- giographic study after successful PTCA stratifies lesions into angiographic subsets with low (group I) and high (group II) risk of coronary restenosis.
(Am J Cardiol1993;71:1391-1395)
From the Division of Cardiology, Anchorena Hospital, Buenos Aires, Argentina; Massachusetts General Hospital, and Harvard Medical School, Boston, Massachusetts. Manuscript received October 1.5, 19Y2; revised manuscript received January 15, 1993, and accepted January 17.
Address for reprints: Igor F. Palacios, MD, Cardiac Unit, Massa- chusetts General Hospital, Fntit Street, Boston, Massachusetts 02114.
P ercutaneous transluminal coronary angioplasty (PTCA) is a widely accepted alternative method for treating patients with coronary artery disease.
Although PTCA results in a good immediate angio- graphic and clinical outcome in most patients, the long- term success of this procedure is limited by the resteno- sis of the treated artery. lil Restenosis occurs more fre- quently between the second and sixth months after PTCA. Radionuclide”-s and angiographic studies have showngp-‘2 that a significant number of patients have re- stenosis early -before the end of the tist month and even on the first week after PTCA. Little is known about the role of early coronary angiography as a guideline to determine the early and late outcome in patients after successful PTCA. We addressed this issue by per- forming a prospective study in 88 patients who under- went early (24 hours) and late (7 I!I 2 months) coronary angiography after successful PTCA.
METHODS Between November 1, 1988 and May 15, 1989, 111
consecutive patients underwent PTCA of 145 lesions at the Anchorena Hospital, Buenos Aires, Argentina. PTCA was successful in 98 patients (88.2%). A successful out- come was defined as >20% change in the percentage of stenosis and a residual stenosis of <50% of the vessel lumen after PTCA, with no major complication occur- ring during hospitalization. Patients were examined angiographically before, immediately after, 24 hours after and at 7 f 2 months after PTCA. Coronary stenoses were determined using digital quantitative analysis.
Sequential high-quality angiograms adequate for dig- ital quantitative analysis were obtained in only 88 of the 98 patients. They are the subject of this study. There were 13 women and ‘7.5 men, mean age 54 1: 3 years (range 38 to 78) (Table I). Forty-five (51.1%) had stable angina, 36 (40.9%) had unstable angina and 7 (8%) had acute myocardial infarction.
Angioplasty procedure: All patients received aspirin and dipyridamole starting at least 1 day before PTCA. After arterial access, systemic heparinization was achieved by the intravenous administration of a bolus dose of 10,000 IU of heparin. Patients received a continuous in- fusion of intravenous nitroglycerin and heparin during PTCA. PTCA was performed using the standard tech- nique. Final angiographic outcome after PTCA was ob- tained by orthogonal angiographic views of the dilated vessel recorded immediately after the last balloon i&la- tion.
After PTCA, medical treatment up to the 24-hour repeat study consisted of systemic heparinization, calci-
urn antagonists, intravenous nitroglycerin and aspirin. All patients were receiving a continuous intravenous in- fusion of nitroglycerin during PTCA and at the repeat 24-hour angiogram. All patients were followed chnical- ly. Coronary angiography was repeated in the 88 patients (102 dilated lesions) at 7 IL 2 months (range 4 to 11)
after PTCA. At follow-up, ah patients were receiving aspirin and calcium antagonists”
CorolwyawiwPmY~ nteasuremelitofeors naty stenoses: AU patients underwent conventional and digital coronary angiography before, immediately after and 24 hours after PTCA and at follow-up. Similar or- thogonal projections were used at each procedure.13-l7
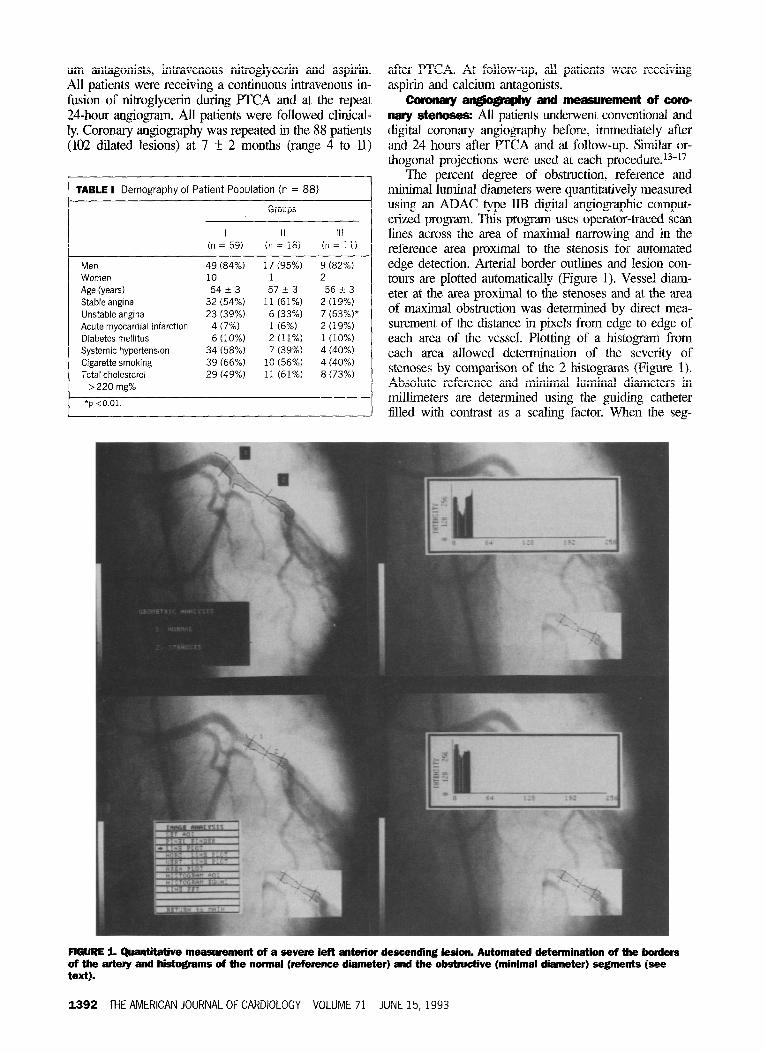
The percent degree of obstruction, reference and minimal luminal diameters were quantitatively measured using an ADAC type JIB digital angiographic comput- erized program. This program uses operator-traced scan lines across the area of maximal narrowing and in the reference area proximal to the stenosis for automated edge detection. Arterial border outlines and lesion con- tours are plotted automatically (Figure 1). Vessel diam- eter at the area proximal to the stenoses and at the area of maximal obstruction was determined by direct mea- surement of the distance in pixels from edge to edge of each area of the vessel. Plotting of a histogram from each area allowed determination of the severity of stenoses by comparison of the 2 histograms (Figure 1). Absolute reference and minimal luminal diameters in millimeters are determined using the guiding catheter filled with contrast as a scaling factor. When the seg-
AWRE 1. Quantiiive measurement of a severe left anterior descending lesion. Automated determination of the borders of the artery and histograms of the normal (reference diameter) and the obstructive (minimal diameter) segments (see text).
1392 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 71 JUNE 15, 1993
ment of the artery proximal to the stenoses was abnor- mal, the segment of the vessel distal to the obstruction TABLE II Angiographic Findings of the 102 Lesions Treated
was used as normal luminal diameter. Absolute dimen- sions are measured with an accuracy of 0.08 mm and a high reproducible intraobserver variability (r = 0.90). For each lesion, 2 orthogonal views were analyzed and averaged. To minimize the foreshortening effect, only end-diastolic tine frames were analyzed. The distance between the patient and the x-ray system was the same in the initial study and in each of the following studies. When there was radiologic evidence of dissection after PTCA, the dissection was included in the Gnal diameter calculation.
The lesion was considered to have restenosed when the diameter stenosis at follow-up was 250%.12 In addi- tion, the incidence of restenoses was also determined by using the criteria of absolute loss 20.7 of the initial gain in minimal luminal diameter.9
Statistkal analysis: Parametric, nonparametric, Student’s t and &i-squared tests were used in compar- ing pre- and postangioplasty degree of obstruction, min- imal luminal diameter and in determining the incidence of restenosis. Comparisons among the 3 groups of patients were performed using l-way analysis of vari- ance. The results are expressed as mean + SD. A p value co.05 was considered significant. Actuarial freedoms for restenosis curve were constructed using the log-rank test.
RESULTS 24-hour angiography: Patients were classiiied into 3
groups by comparing the results of the coronary arterio- grams 24 hours after and immediately after PTCA: group I- lesions with no changes or 110% increase in the post-PTCA arterial diameter stenosis (71 lesions, 69.6%); group II - lesions with >lO% increase in the post-PTCA arterial diameter (19 lesions, 18.6%); and group lTl- lesions with total occlusion (12 lesions, 11.8%).
Groups
I II Ill 0-i = 71) (n = 19) (n = 12)
Coronary arteries Left anterior descending 41 (58%) Right 18 (25%) Left circumflex 12(17%)
Total occlusion 3(4%) Type A lesion 48 (67.6%) Type B lesion 19 (26.7%) Type C lesion 4 (5.7%) Type B and C 23 (32.3%)
Patients in whom multiple lesions were dilated could be included in >1 group. For example, 1 PTCA lesion could be the same as the day before (group I) and an- other lesion dilated in the same patients could exhibit either a more severe obstruction (group II) or total oc- clusion (group III). Regardless of the 24-hour angio- graphic iindings, no patient underwent reintervention. Thirty percent of the lesions showed worsening obstruc- tion (either total occlusions or more severe obstruction) at 24-hour follow-up angiography than immediately af- ter PTCA. However, the standard criteria for restenosis (250% diameter stenosis at follow-up) was present in only 15 of the 102 lesions studied (14.7%) at 24-hour follow-up.
There were no significant differences in the severity of stenosis before and immediately after PTCA in groups I, II and III. However, group III had a higher incidence of patients with prior total occlusion than groups I and II (p ~0.01) (Table lI). In addition, group IIl had a higher percentage of acute closure syndrome during dilatation (p <0.005) (Table IfI). Complex lesions
(eccentric, tortuous, tandem, filling defects, total occlu- sion) were more frequent in groups III (91.6%) and II (68.4%) than in group I (32.3%) (p ~0.01) (Table II). The percentage of patients having a residual stenosis immediately after PTCA ~20% was greater in groups I and IIl than in group II. However, the minimal luminal diameter after PTCA was >2.4 mm in all 3 groups (Table III).
Clinical findings: Demographic and basal clinical characteristics were similar in the 3 groups (Table I); however, group IIl had a higher proportion of patients with unstable angina and acute myocardial infarction than the other 2 groups.
Late angiogiaphic findings and incidence of rest* nosis: At late follow-up angiography, the mean degree of obstruction in group I was 21.2 f 16.8%, in group II 60.6 + 21.9% and in group III 98.5 + 1.3% (Table III). Although there were no significant differences among these 3 groups immediately after PTCA, at 24 hours after PTCA and at late follow-up, lesions in groups II and III had a greater decrease in minimal luminal di- ameter and diameter stenosis than those in group I (p <O.OOOl) (Table III). The degree of residual obstruction immediately after PTCA was associated with an in- creased incidence of late restenosis (37.7%) when it was 220% than when it was ~20% (22.8%) (p <O.OOl), but this variable alone was insufficient in predicting the inci- dence of late restenosis for groups I and II. Restenosis occurred in 9% of the 22 lesions in group I with post- PTCA residual stenosis 220% and in 10% of the 49 lesions with post-PTCA residual stenosis ~20%; in con- trast, restenosis occurred in 70.5% of the 17 lesions in group II with post-PTCA residual stenosis 220% and iu the 2 lesions (100%) with post-PTCA residual stenosis <20%.
Angiography at 24 hours identified those lesions that were more likely to have late restenosis. Using the Na- tional Heart, Lung, and Blood Institute Registry defini- tion of restenosis of 250% diameter at follow-up, the overall incidence of late restenosis per lesion was 32% (33 of 102). Restenosis (per lesion) was significantly greater in group II than in group I (73.6% [14 of 191 vs
LATE RESTENOSIS Lesions
GROUP I GROUP JI
FIGURE 2. Difference in late restenosis per lesion among groups I and II (p ~0.0001).
9.8% [7 of 711, p <O.OOOOl) (Figure 2). When the 12 lesions with total occlusion identified at 24 hours are excluded, late restenosis occurred in 21 (23%) of the other 90 lesions. From this later cohort of 90 lesions, the 21 lesions with late restenosis had a significantly greater decrease in minimal luminal diameter at 24 hours than the 69 lesions without restenosis (-0.3 + 0.06 mm vs -0.05 + 0.03 mm, p <O.OOOl). The correspond- ing decrease in diameter stenosis at 24 hours was also significantly greater in lesions with restenosis (-9.8 + 1.8% vs -1.9 + 0.78%, p <0.00005).
A similar relation between late restenosis and diame- ter stenosis at 24 hours was present when the detinition of restenosis of loss of 20.7 mm of the initial gain in minimal huninal diameter at follow-up was used. With this definition, 33 of the 102 lesions (32%) had late re- stenosis. Restenosis occurred in 73.6% (14 of 19) of the lesions in group II compared with 9.8% (7 of 71) of the lesions in group I (p <O.OOl). Lesions with restenosis had a signikantly greater decrease in minimal luminal diameter at 24 hours than lesions without restenosis (-0.27 + 0.06 mm vs -0.06 f 0.03 mm, p <0.0016). The corresponding decrease in diameter stenosis at 24 hours was also signilicantly greater in the lesions with late restenosis (-8.7 + 1.8% vs -2.44 + 0.8%, p ~0.003).
LilSCUSSlON The present study demonstrates that early decreases
in minimal luminal diameter detected by coronary angi- ography performed 24 hours after successful PTCA are present in lesions that are more likely to develop reste- nosis at follow-up. Lesions exhibiting a decrease in minimal luminal diameter >0.3 mm or showing an increase in diameter stenosis of >lO% 24 hours after PTCA (group II) were more likely to develop resteno- sis at late follow-up. In contrast, lesions with either no changes or improved arterial luminal diameter at early repeated angiography (group I) have a lower incidence of restenosis at follow-up. Patients in group III (with total occlusion at 24 hours after PICA) had 2 important baseline differences compared with the other 2 groups: (1) a greater proportion of patients with previous total occlusion, and (2) a higher incidence of unstable angi- na and acute myocardial infarction. However, unstable clinical syndromes by themselves do not seem to be the only factor responsible for restenosis. There were no sign&ant clinical differences between groups I and II before PTCA; specilically, they had a similar incidence of previous unstable clinical conditions. On the other hand, plaque morphology seems to be an important fac- tor for restenosis. Complex lesions (types B and C) were more frequently identifted by angiography in group II than in group I.
In the immediate period after PTCA, the degree of residual obstruction has been previously described to be an important predictor for late restenosis.1,2,12,181 In agreement with those studies, our data show that patients with residual lesions of >20% immediately after PTCA have a greater incidence of restenosis at late follow-up than those with lesser degree of residual stenosis (39.6 vs 22.8%, p ~0.01). However, repeat coronary an- giography 24 hours after PTCA can further identify a
1394 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 71 JUNE 15,1993
subset of patients at a higher risk of restenosis from those with obstruction ~20% immediately after PICA.
Our study supports the high predictive value for late restenosis in positive thallium stress test resu1ts5,8%22-24 and exercise-gated blood pool scan7 performed between 1, day gll;;ci 2 .+,z& .Jici- ~giopiasry.S,7,ZCLG
Nobuyoshi et allo suggested that angiographic find- ings on the lirst day after FTCA are not predictive of late restenosis. However, although the result was not sta- tistically significant, patients having restenoses 24 hours after PTCA had a greater tendency to have restenoses at 3-month follow-up. Furthermore, in Nobuyoshi’s study the incidence of plaque morphology before PICA and its 24-hour correlation after PICA was not ana- lyzed. As shown in our study, plaque morphology appears to be an important factor in determining early decreases in minimal luminal diameter 24 hours after INCA.
The underlying mechanism for the decrease in mini- mal luminal diameter, which occurs in some patients at 24-hour follow-up angiography, cannot be determined by this study. Although early arterial wall elastic recoil9 seems to be an attractive explanation for some lesions such as those with eccentric plaques, thrombus forma- tion could also play an important role, particularly in lesions with unstable plaques. The use of techniques to study coronary intraarterial lumen such as angioscopy and intracoronary ultrasound may help to further clarify the findings of this study. It is possible that the use of other interventional coronary artery techniques that de- bulk the atherosclerotic plaque (atherectomy and laser) or decrease arterial elastic recoil @tents) could have a favorable impact in the results obtained with PICA in this study. FinaIly, the patients included in groups II and IIl represent a therapeutic challenge and their manage- ment could be controversial. Controlled studies are needed to determine the role of mechanical (laser, stents, atherectomy, repeat PTCA) and/or biological (antiplatelet agents, antithrombin drugs, chemotherapy) forms of therapy in the prevention of restenosis in these high-risk patients.
.I. Kaltembach M, Kober G, Schwa D, Vallbracht C. Recui-ence rate after suc- cessful coronay angioplasty. Eur Hearf .I 1985;6:276-281. 2. Leimgmber PP, Roubin GS, Hollman J, Cotsonis G, M&r B, Douglas J, King S, Gruentzig A. Restenosis after successful coronluy angioplasty in patients with single vessel disease. Circulation 1986;73:7 10-717. 3. Levine S, Ewels CJ, Rosing DR, Kent KM. Coronary angioplasty: clinical and angiographic follow-up. Am .I Cardiol 1985;55:673+576. 4. Rosing DR, Cannon RO, Watson RM, Bonow R, Mincemoyer R, Ewels C, Leon M, Lakatos E, Epstein S, Kent K. Three year anatomic functional and clinical fol-
low-up after successful percutaneous transluminal coronary angioplasty. J Am Cull Cmdiol 1987;9:1-7. 5. Breinblatt W, Weiland F, Sapaccavento L. Stress Thallium-201 imaging after coronary angioplasty predicts restenosis and recurrent symptoms. J Am CON Car- dial 1988;12:1199-1204. 6. DePuey EG, Leatherman LL, Leachman RD, Dear W, Massin E, Mathur V, Rllrrlinp r !+nq+e”,G” nh-- c^-..l...-:.--il 1, : ._i ~~.... _.._. __-..” _-._. . . ;;r.h,LJ ‘“,&“+dr uardleu w,ut cxer- cise-gated rxdionuctidc ventic:~logwphy. d Am C& Cwdioi 1984,4:1103-l 113. 7. O’Keefe J, Lapeyre A, Holmes D, Gibbons R. Usefulness of early radionuclide angiogmphy for identifying low-risk patients for late restenosis after PICA. Am J Cardiol 19X8:61:51-54. 8. Stokey T, Burwell L, Nygaxd TH, Gibson R, Wetson D, Bella G. Quantita- tive exercise Thallium-201 scintigmphy for predicting angina recurrence after PICA. Am .I Cardiol 1989;63:517-521, 9. Sermys PW, Luyten HE, Beat KJ, Geuskens R, De Feyter P, Vander Brand M, Reiber J, Ten Kate” H, Vanes A, Hugenholtz PG. incidence of restenosis after suc- cessful coronary angioplasty: a time-related phenomenon. Circulation 1988;77: 361-371. 10. Nobuyoshi M, Kimura T, Nosaka H, Mioka S, Veno K, Yokoi H, Hamasaki N, Horiuchi H, Ohishi H. Restenosis after successful percutaneous tmnsluminal coronary angioplasty: serial angiographic follow-up of 229 patients. J Am Coil Car- dial 1988;12:616-623. 11. Sanders M. Angiographic changes thirty minutes following percutaneous trans- luminal coronary angioplasty. Angiopkzsty 1985;36:419-424. 12. Holmes DR, Vliestra RE, Smith HC, Vetrovec G, Kent K, Cowley M, Faxon D, Gruentzig A, Kclsey S, Dctre K, Van Raden M, Mock M. Restenosis after per- cutaneous transluminal coronary angioplasty (RCA): a repoti from the pI%A Reg- ishy oftheNationalHeti,Lung andBloodInstitute.AmJCardioll984;53:77C-81C’. 13. Htison DG, White CW, Hiratza LF, Doty DB, Barnes DH, Eastham CL, Marcus ML. The value of lesion cross-sectional area dcterminated by quantitative coronary angiography in assessing the physiologic significance of proximal left ante- rior descendiig coronary arterial stenosis. Circulation 1984;69: 1 I1 1-I 119. 14. Nichols AB, Gabrieli CFO, Fenoglio JJ, Esser PD. Quantification of relative coronay arterial stenosis by cinevideodensitometc analysis of coronary at&o- grams. Circulation 1984;69:512-522, 15. Siver KH, Buczek JA, Esser PD, Nichols AB. Quantitative analysis of coro- nay arteriograms by microprocessor cinevideodensitometry. C&et Cardiovasc Diagn 1987;13:291-300. 16. White CW, Wright CB, Doty DB, Hiratza L, Eastham C, Harrison D, Marcus M. Does visual interpretation of the coronary arteriogran predict the physiologic importance of a cog-onaty stenosis? N Engl .I Med 1984;310:819-824. 17. Sermys RW, Reiber JHC, Wijns W, Brand MV, Kooijman C, Kate” H, Hugen- holtz PG. Assessment of percutaneous transluminal coronary angioplasty by qua.“- tit&e coronary angiography: diameter versus densitomehic area measurements. Am .I Curdiol 1984;54:482488. 18. Mabin TA, Holmes DR, Smith HC, Vliestra R, Reeder G, Bresnaham J, Bow. A, Hammes L, Elvebeck L, Orszulek T. Restenosis after percutaneous translumi- nal coronary angioplasty. Circulation 1985;71:75&760. 19. McBride W, Lange R, Hillis D. Restenosis after successful coronary angio- plasty. N Engl J Med 1,988;26:1734-1736. 20. Essed CE, Van denBraId M, Becker AE. Transluminal coronary angioplasty and early restenosis: fibrocellular occlusion after wall laceration. Or Heart J 1983;49: 393-396. 21. Blackshan JL, O’Callagham W, Califf R. Medical approaches to prevention ,after coronary angioplasty. J Am Co11 Cardiol 1987;9:83&848. 22. Wijns W, Sermys PW, Reiber JHC, De Feyter P, Van denBrand M, Smoons M, Hugenholtz P. Early detection of restenosis after successful percutaneous rrans- luminal coronruy angioplasty by exercise-redis~ibution thallium scintigraphy. Am J Cardiol 1985;55:357-361. 23. El Tamini H, Davies G, Hackett D, Fragasso G, Crea F, Mzxn A, O’Sulli- van C. Very early prediction of restenosis after successful coronary angioplascy: anatomic and functional assessment. I Am Co11 Cardiol 1990;15:259-264. 24. Hardoft’ R, Shefer A, Gips S, Mcrdler A, Flugelman M, Halon D, Lewis B. Predicting late restenosis after coronary angiopla%y by very early (12 to 24 hs.) Thallium-201 scintigraphy: implications with regard to mechanisms of late core- nay restenosis. .I Am Co11 Cardiol 1990;15:1486-1492.