“ eCare” ‐ A new era in Patient Safety eCare A new era in Patient Safety and Quality of Care at North York General Hospital Central LHIN Quality Series Knowledge f bi / l f at North York General Hospital Transfer Webinar/Teleconference January 13 th 2010
Transcript
“eCare” ‐ A new era in Patient SafetyeCare A new era in Patient Safety and Quality of Care
at North York General HospitalCentral LHIN Quality Series Knowledge
f bi / l f
at North York General Hospital
Transfer Webinar/Teleconference
January 13th 2010
Agendag
• North York General Hospital profilep p• Why do we need advanced
Electronic Medical Record (EMR) systems in hospitals?S f t d ti f d t– Safety and prevention of adverse events
– Evidence-based care for improved patient outcomes– Stages of EMR development and patient outcomes
• North York General’s eCare Project:– Definitions and Scope
K f t f S– Key factors for Success– Development Methodology
• Communication and Change Managementg g• Lessons Learned and Outcomes to Date
North York General Hospital
3 Sites:1. General Site – 413 Acute Care Beds2. Branson Site – Ambulatory Care3. Seniors’ Health Centre – 200 Long Term Care Beds
Serving 400,000 residents within North Central Toronto and Southern York Region
3
Adverse Event Rates in CanadaThe Canadian Adverse Events Study
Baker R, Norton P Can Med Assoc J 2004;170(11)
Study of 3745 hospital admissions in 20 different Canadian hospitals in the year 200020 different Canadian hospitals in the year 2000
• 7.5% of acute care admissions had adverse event(s):• 37% of adverse events were preventable• 21% resulted in death• Patients at risk: age ≥ 65; LOS > 6 daysPatients at risk: age 65; LOS 6 days• Drug-related adverse events: second most common
Bridging the Evidence Gap:P t P tiPaper to Practice
Cognitive:Cognitive:
200 MB 6 000200 MB capacity
6,000 articles/dayGAP
Temporal: Average of 17 years for published clinicalAverage of 17 years for published clinical
guidelines to reach the patient bedsidePersistence of existing practices (Brazilian fishing village)Persistence of existing practices (Brazilian fishing village)
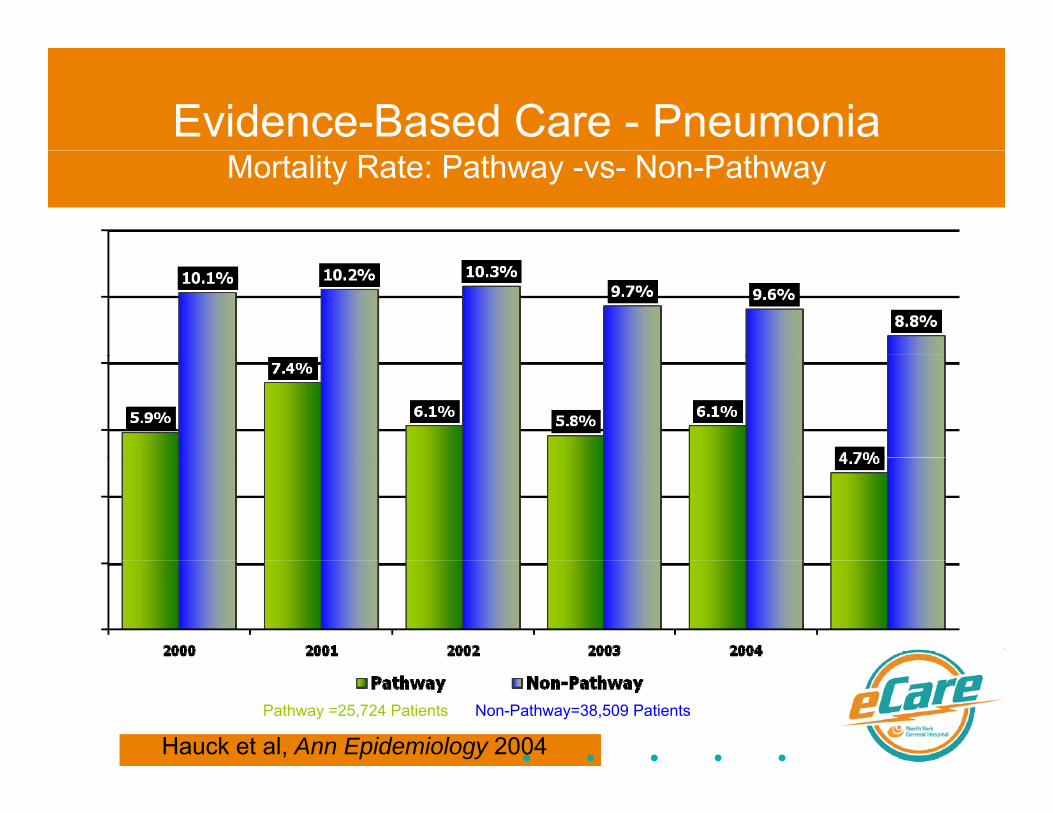
Evidence-Based Care - PneumoniaMortality Rate: Pathway -vs- Non-Pathway
– “Excellent Care for All” legislation – McGuinty gov’t
United States:• United States:– Joint Commission – performance requirements based on
condition-specific evidencecondition specific evidence – Hospitals: Pay for performance,
penalty for preventable complications– ARRA HITECH Act: Hospitals paid/penalized to implement
“meaningful use” of sophisticated electronic medical record systems with evidence-based decision supportrecord systems with evidence-based decision support
Stages of EMR Development are R l t t P ti t O tRelevant to Patient Outcomes
StatisticalStatistical correlation
between the level of
sophistication of EMRof EMR
technology and improved patientpatient
outcomes
Examples: VA VistA System Davies Award Winning HospitalsSource for EMR stage correlation data: 2006 HIMSS EMR Sophistication Correlates to Hospital Quality Data.
Examples: VA VistA System, Davies Award Winning Hospitals
CPOE (Computerized Provider Order Entry)V diff t f b d d !Very different from paper-based orders!
• Always legible• No transcription required• “Order sets” based on common diagnoses
• Active links to current evidence
• Easily updatable• Decision support with alerts and rules
• Auditable for quality improvement and research
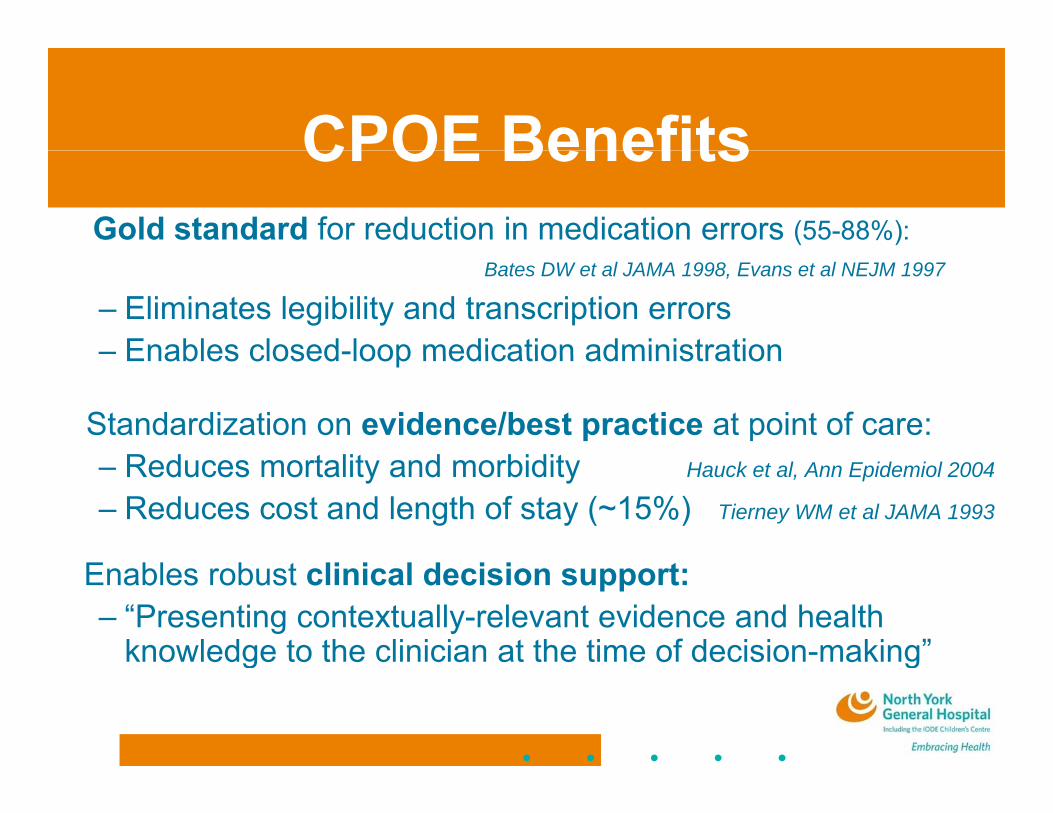
CPOE BenefitsGold standard for reduction in medication errors (55-88%):
• Standardization on evidence/best practice at point of care:R d t lit d bidit– Reduces mortality and morbidity Hauck et al, Ann Epidemiol 2004
– Reduces cost and length of stay (~15%) Tierney WM et al JAMA 1993
Enables robust clinical decision support:– “Presenting contextually-relevant evidence and health
knowledge to the clinician at the time of decision-making”g g
Effect of Adding Cli i l D i i S t t CPOEClinical Decision Support to CPOE
Evidence-based order sets with clinical decision support:Evidence based order sets with clinical decision support:– Single-hospital study – sepsis order set:
• 15.5% absolute mortality reduction (p<0.01)• Length of stay reduced by 6.3 days (p=0.02)
Thiel SW et al. Crit Care Med 2009 37(3):819-24
– 41-hospital study – care for pneumonia:• Significant 21% mortality reduction with clinical decision
support (no significant change with CPOE alone)pp ( g g )• $538 saved per patient with clinical decision support
($132 saved per patient with CPOE alone)Amarasingham R et al. Arch Intern Med 2009 169(2):108-14g ( )
What is eCare?What is eCare?
Advanced ElectronicAdvanced ElectronicMedical Record (EMR)
+Standardization on
Evidence-Based Care++
Safe Prescribing andMedication Administration
A new era in patient careusing EMR technologyed cat o d st at o
+Clinical Decision Support
g gy
Goals:Improved patient safetyImproved quality of carepp
(Rules, Alerts)Improved quality of care Improved patient outcomes
Kickoff date: January 1, 2007
Scope: Inpatient Medicine and Surgery UnitsScope: Inpatient Medicine and Surgery Units,CrCU and PACU
• Electronic Physician Message CenterCPOE Computerized Provider Order Entry
SE IPH
HIMSS Stage 4• CPOE - Computerized Provider Order Entry• eMAR – with Closed Loop Medication Admin• Medication Reconciliation, eDischarge with ePrescriptions
ASE II
HIMSS Stage 4HIMSS Stage 5
Phase I – live June 17, 2008 Phase II – live Oct 26, 2010
eCare FirstseCare Firsts
The NYGH eCare Project is unique in Canada:– First Canadian deployment of CPOE with
l l d t d id b d d t t tregularly-updated evidence-based order set content integrated into the physician decision-making workflow
– First Canadian medium to large size hospital with– First Canadian medium to large size hospital with closed-loop barcode medication administration and first in Canada to implement GS1 industry standard medication barcodingmedication barcoding
– First HIMSS Stage 5 hospital in Ontario, second hospital to reach this milestone in Canadaseco d osp a o eac s es o e Ca ada
Project Implementation StructureStructure
Clinical Adoption of CPOE: th “A id T t”the “Acid Test”
“U t 50% f CPOE i l t ti tt t f il”
health IT project = difficulty ofcomplexity clinical adoption
• “Up to 50% of CPOE implementation attempts fail”National Health Information Network Co-ordinator David Brailer Washington Post, 2005
• Example: Cedars Sinai Medical Center 2002:• Physician dissatisfaction forced the administration
to scrap a proprietary $34 million CPOE systemp p p y y
Three Key Success Factors f C I l t tifor eCare Implementation
1 Vision – full support from senior hospital management in alignment1. Vision full support from senior hospital management in alignment with organizational mission: improve quality and safety of patient care
2. Engagement of front-line clinicians:g g• Respected clinician champions for peer-driven change• Communicate impetus for change – resonate with clinicians
Di t i t i t d i f t t i b i • Direct input into design of system to increase buy-in clinician driven process = clinician adoption
• Workflow mapping and usability testing
3. Clinical Integration:• Interprofessional Team – remove traditional silos
I t t id i t i ti li i d d• Integrate evidence into existing policies and procedures
eCare Development M th d lMethodology
• Clinician-driven care transformation projectClinician-driven care transformation project with interprofessional approach:– Physicians, nurses, allied health
Pharmacy– Pharmacy– Lab, medical imaging– Clinical Informatics, Information Services
• Re-engineer care processes around evidence:– Not automation for automation’s sake!– Examine and align NYGH processes to integrateg p g
best evidence from the medical literature into standard workflows
– Examples: stroke care, psmoking cessation, vaccination
Bringing the evidence t th b d idto the bedside
Sources of Evidence:– Zynx Health Evidence-Based Order Sets
• Installed base of over 1,600 hospitals• Highest-quality evidence distilled from the literature, by staff
trained in evidence-based medicine• Updated quarterly by clinicians, for clinicians• Built-in tools for online review• Close integration with EMR for build and maintenance
– Canadian/International Guidelines/key articles– NYGH paper order sets, protocols, directives
Order Set DevelopmentOrder Set Development• Goal: 300 Evidence-Based Order Sets• Development process overseen by
centralized build team (meets weekly):( y)– 1.0 FTE physicians (4 MD’s, different specialties)– 1.2 FTE pharmacists (3 part-time)
2 0 FTE IS application specialists (3 individuals)– 2.0 FTE IS application specialists (3 individuals)• Order set design:
– Standardized layout and format (style guide)– Order sets modularized, cross-referenced, evidence integrated– All content available on Intranet – “linked evidence documents”,
interactive PDF of order sets for downtimeinteractive PDF of order sets for downtime
Order Set Life Cycle:B ildi Q lit d CBuilding Quality and Consensus
• Order Set Prototyping (Zynx guidelines NYGH documents)1
• Order Set Prototyping (Zynx, guidelines, NYGH documents)
2• Online Order Set Interprofessional Review
Nursing Allied Health Lab Radiology Medical Imaging2 Nursing, Allied Health, Lab, Radiology, Medical Imaging
3• Online Order Set MD Review – individuals, groups
3
4• Comment review and consolidation, evidence updates,
consensus meetings as needed
5• Order Set Final Approval (MAC Committee - monthly)
Interprofessional Order Set R iReview
Pneumonia: Evidence Link
Clinical Decision Support: VTE P h l iVTE Prophylaxis
Intervention ComplianceNo intervention no VTE protocol 10 40%No intervention – no VTE protocol 10-40%Simple-to-follow VTE protocol, paper (3-level risk stratification, not score-based)
50%
Standardized evidence based VTE order 65 85%Standardized, evidence-based VTE ordermodule, embedded into CPOE order sets
65-85%
Real-time electronic clinical decision support
95%+
Dr. Greg Maynard, Director, Center for Improvement Science, UCSD
clinical decision support
Medication IntegrationMedication Integration
• Clinical Decision Support:Clinical Decision Support:– CPOE Order Sets for safe prescribing
(drug selection, dose adjustment and monitoring)(drug selection, dose adjustment and monitoring)– Adverse Drug Event prevention– Dose Range CheckingDose Range Checking
Use for patient Use for patient specific dosesspecific dosesLiquidLiquid by bubble packaging
systembottle bottle dispensingdispensing
specific dosesspecific doses
InjectableInjectable Use for injectables without UPC by bar
Commercially Commercially available fromavailable from
Use for TPN & Use for TPN & patient specificpatient specificwithout UPC by bar
coding stationavailable from available from manufacturermanufacturer
patient specific patient specific IV bagsIV bags
OthersOthers Use for items without UPC by bar coding
Commercially Commercially available fromavailable from
Use for patient Use for patient specific itemsspecific itemsUPC by bar coding
stationavailable from available from manufacturermanufacturer
specific items specific items i.e. inhalersi.e. inhalers
Professional PracticeProfessional Practice
• 20 Policy updates• 20 Policy updates• Integration work
W kfl i• Workflow mapping –nursing, physicians, allied healthEd ti f t d t d t ff• Education for students and agency staff
• FMEA for Medication Administration• Dedicated project resources
Professional PracticeProfessional Practice
Benefits• Enhances safety• Supports best practices• Supportive links to the literature • Enhanced and integrated communication• Standardized workflow processesp
Nursingg
The NYGH Leadership Culture TransformationCulture Transformation
Story TellingCulture TransformationIndividuals →Teams
IHI
Collaboratives Safer HealthcareNow!
Ss
C w!
CULTURE TRANSFORMATION
& LEAN
Command & Control→Steward
Bosses→Coaches
Process TransformaPro
& L→wardship
ED-GIMlkit
C
rmationProjectsBlaming→
Account Silos→Systems
EToolkit
→untabilitySilos→
Change Managementg g
• NYGH on a journey of leadership development and• NYGH on a journey of leadership development and change management. Culture ripe for change
• Proactive involvement of front-line clinicians in system ydesign– 75 “Super Users” identified from each scope of practice– Involvement = familiarity, endorsement, adoption
• Consistent communication of benefits:– For patients– For clinicians (providing tools for quality care)
• Anticipation and minimization of “friction points”
Communication
• Communication plan with dedicated resource staffCommunication plan with dedicated resource staff• Focus on engagement of over 2300 clinical staff• Major themes:j
– Clinician-driven: “built by clinicians, for clinicians”– Improved patient safety– Integration of evidence to improve quality of care– Interprofessional Integration and Collaboration
O i it t t H lth t NYGH– Ongoing commitment to eHealth at NYGH• Fun “Super Hero” theme depicting hospital physicians,
O 2 200 li i l t ff t i d i l• Over 2,200 clinical staff trained in class• 7 additional Trainers hired plus “super users”• Online training modules created for physicians• Online training modules created for physicians• Training between 1 and 7.5 hours (depending on user)
– Physicians – 4 hours in classroom or 3 hours online with 1 hr class– Nurses – 7.5 hours in classroom– Super Users and Nurse Managers – 15 hr in classroom– “View only” users – 1 hour inserviceView only users 1 hour inservice
• Additional practice:– Practice and simulation rooms– Online practice domain
Devices and Technical
• Devices – assessed and met need for greater access:Devices assessed and met need for greater access:– “Device Fair” for clinicians to select handheld and portable devices
• Handheld “CareMobile” scanners for closed-loop medication admin“W k t ti Wh l ” t bl di ti t f h• “Workstations on Wheels” portable medication carts for each nurse
– Portable devices and stationary PC’s added to all clinical units based on unit-by-unit assessment by interprofessional team
• Performance - monitoring and adjustment of:– Electronic Medical Record software (Cerner)– PC’s, network, storage systemsC s, et o , sto age syste s– Wireless network and devices
• Tweaked interfaces to other systems
Senior Leadership TeamSenior Leadership Team• Strong Board and Senior Leadership TeamStrong Board and Senior Leadership Team
Support was crucial to the success of eCare:eCare:– Focused organization on goal of improved
quality and safety of patient care using technology– Prioritized eCare project and allocated adequate
financial resources, despite funding challengesVisible and supportive during– Visible and supportive during design, implementation and go-live
– Interaction with front-line staff during gkey project milestones and go-live
Go-Live!
• October 26 2010• October 26, 2010• All Hands On Deck!
– 24/7 Control Centre for 6 weeks– SuperUsers on all clinical units
“At th Elb ” t f h i i– “At the Elbow” support for physicians– Additional support staff from TEGH, Mt Sinai
S i T i ibl d i l ti it– Senior Team visible and circulating on units– Daily status meetings with outcome metrics
Change Req est and Appro al process in place– Change Request and Approval process in place
Lessons Learned
• Key success factors:y– Vision communicated and supported by Senior Team– Engagement and involvement of front-line clinicians– Integration of interprofessional groups, workflow, policy
and procedureI l t ti f CPOE/ MAR ifi fl i• Implementation of CPOE/eMAR magnifies flaws in existing processes (anticipate and refine proactively!)
• Adequate training and support is essential• Adequate training and support is essential• Must continue to audit, measure, learn and
improve in order to achieve full benefit for patientsimprove in order to achieve full benefit for patients
Outcomes to Date
• >95% of orders being entered by physicians in CPOE in first week of implementation
• >65% of medications being administered using closed• >65% of medications being administered using closed-loop process
• Over 300 evidence-based order sets in use, with more being built
• Clinician satisfaction survey planned for mid-JanuaryO t t i (HSMR l th f t t ) t 3 th• Outcome metrics (HSMR, length of stay, etc) at 3 months and 6 months post go-live
AchievementsJeremy wins CHIA award
NYGH Presenter Contacts
Thomas ChanInterim Director, Pharmacy Services
Dr. Jeremy ThealDirector, Medical InformaticsPharmacy Services