British HeartJournal, 1975, 37, 69I-699. Echocardiographic assessment of severity of aortic regurgitation K. E. Gray' and D. W. Barritt From the Cardiac Department, Bristol General Hospital, Guinea Street, Bristol An echocardiographic study of left ventricular diameter was made in 27 patients with aortic regurgitation. Comparison was made with a group of 2I nomal subjects and a group of 6 patients with large left ventricles without valvar regurgitation. Total stroke volume, total left ventricular output, and ejection fraction were derived by the method of cubing the left ventricular diameter to give approximate left ventricular volumes at end-diastole and end-systole. The patients were assessed independently and placed into three grades of severity. The echocardiographic dimensions of patients with mild aortic regurgitation were not significantly different from those of the normal subjects. With increasing severity of aortic regurgitation, there were increases in group values for left ventricular diameter, total stroke volume, and total left ventricular output. The ejection fraction was depressed below the normal range in only one patient with aortic regurgitation. It is concluded that echocardiographic measurement of left ventricular dimensions is of value in assessing the severity of aortic regurgitation. In many patients it is difficult to assess accurately the severity of aortic regurgitation by clinical and non-invasive radiological methods. Cine-aorto- graphy offers a method of classification of the severity of regurgitation into one of three or four grades (Cohn et al., I967), but this requires arterial catheterization which limits how often the study may be repeated. More detailed information may be gained by quantitative angiography (Miller, Kirklin, and Swan, I965), but this is also invasive and the calculations involved are time consuming. It has been demonstrated that the diameter of the left ventricle and shortening of that diameter with systole may be measured by echocardiography (Feigenbaum, Zaky, and Nasser, I967; Chapelle and Mensch, I969). An estimate of left ventricular volume may be obtained by cubing this diameter, and approximate values for stroke volume and ejection fraction may be obtained from measure- ments at end-diastole and end-systole (Pombo, Troy, and Russell, I971; Gibson, I973; ten Cate et al., I974). When stroke volume is derived by this means in patients with valvar regurgitation the total stroke volume is estimated, being the sum of the forward stroke volume and the regurgitant fraction. Popp Received 30 January 1975. 'Present address: Barnet General Hospital, Wellhouse Lane, Barnet, Herts EN5 3DJ. and Harrison (I970) estimated the regurgitant frac- tion in patients with mitral regurgitation and patients with aortic regurgitation by subtracting the forward stroke volume measured by the Fick technique from the stroke volume measured by echocardiography. Danford et al. (I973) estimated, aortic regurgitant flow in I2 patients with mild or moderate aortic regurgitation by subtracting the mitral valve flow from the aortic valve flow, having estimated the mitral valve flow from the opening velocity of the anterior cusp. In the present study the left ventricular diameter was measured by echocardiography and the total stroke volume estimated in patients with aortic regurgitation of varying degrees of severity. The results were compared with an independent assess- ment of the severity by clinical and radiological methods. Patients and methods Echocardiographic studies were made in three groups of subjects. I. Patients with aortic regurgitation Technically satisfactory recordings were obtained in 27 patients. Patients with mitral regurgitation or dominant aortic stenosis were excluded. Patients with left bundle- branch block were excluded as this lesion may cause on 22 May 2018 by guest. Protected by copyright. http://heart.bmj.com/ Br Heart J: first published as 10.1136/hrt.37.7.691 on 1 July 1975. Downloaded from
Transcript
British HeartJournal, 1975, 37, 69I-699.
Echocardiographic assessment of severity ofaortic regurgitation
K. E. Gray' and D. W. BarrittFrom the Cardiac Department, Bristol General Hospital, Guinea Street, Bristol
An echocardiographic study of left ventricular diameter was made in 27 patients with aortic regurgitation.Comparison was made with a group of 2I nomal subjects and a group of 6 patients with large left ventricleswithout valvar regurgitation. Total stroke volume, total left ventricular output, and ejection fraction werederived by the method of cubing the left ventricular diameter to give approximate left ventricular volumes atend-diastole and end-systole. The patients were assessed independently andplaced into three grades of severity.The echocardiographic dimensions of patients with mild aortic regurgitation were not significantly differentfrom those of the normal subjects. With increasing severity of aortic regurgitation, there were increases ingroup values for left ventricular diameter, total stroke volume, and total left ventricular output. The ejectionfraction was depressed below the normal range in only one patient with aortic regurgitation.
It is concluded that echocardiographic measurement of left ventricular dimensions is of value in assessingthe severity of aortic regurgitation.
In many patients it is difficult to assess accuratelythe severity of aortic regurgitation by clinical andnon-invasive radiological methods. Cine-aorto-graphy offers a method of classification of theseverity of regurgitation into one of three or fourgrades (Cohn et al., I967), but this requires arterialcatheterization which limits how often the studymay be repeated. More detailed information maybe gained by quantitative angiography (Miller,Kirklin, and Swan, I965), but this is also invasiveand the calculations involved are time consuming.
It has been demonstrated that the diameter of theleft ventricle and shortening of that diameter withsystole may be measured by echocardiography(Feigenbaum, Zaky, and Nasser, I967; Chapelleand Mensch, I969). An estimate of left ventricularvolume may be obtained by cubing this diameter,and approximate values for stroke volume andejection fraction may be obtained from measure-ments at end-diastole and end-systole (Pombo, Troy,and Russell, I971; Gibson, I973; ten Cate et al.,I974). When stroke volume is derived by this meansin patients with valvar regurgitation the total strokevolume is estimated, being the sum of the forwardstroke volume and the regurgitant fraction. Popp
Received 30 January 1975.'Present address: Barnet General Hospital, Wellhouse Lane,Barnet, Herts EN5 3DJ.
and Harrison (I970) estimated the regurgitant frac-tion in patients with mitral regurgitation andpatients with aortic regurgitation by subtractingthe forward stroke volume measured by the Ficktechnique from the stroke volume measured byechocardiography. Danford et al. (I973) estimated,aortic regurgitant flow in I2 patients with mild ormoderate aortic regurgitation by subtracting themitral valve flow from the aortic valve flow, havingestimated the mitral valve flow from the openingvelocity of the anterior cusp.
In the present study the left ventricular diameterwas measured by echocardiography and the totalstroke volume estimated in patients with aorticregurgitation of varying degrees of severity. Theresults were compared with an independent assess-ment of the severity by clinical and radiologicalmethods.
Patients and methodsEchocardiographic studies were made in three groups ofsubjects.
I. Patients with aortic regurgitationTechnically satisfactory recordings were obtained in 27patients. Patients with mitral regurgitation or dominantaortic stenosis were excluded. Patients with left bundle-branch block were excluded as this lesion may cause
on 22 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.7.691 on 1 July 1975. Dow
asymmetrical left ventricular contraction and may in-validate estimates of stroke volume (McDonald, I973).The 27 patients were all in sinus rhythm. Six of thepatients (Cases 8, I2, I5, I9, 20, and 23) had relativelyacute aortic regurgitation, having had subacute bacterialendocarditis in the year before study. Among the 27patients were 5 who, at some stage of their illness, hadhad radiological evidence of pulmonary oedema, but inonly 2 patients (Cases i8 and I9) had raised jugularvenous pressure ever been noted and only in Case I9was this raised at the time of the echocardiographicexamination. Both Cases i8 and I9 had relatively acuteaortic regurgitation caused by a leak of sudden onsetaround the seat of a Starr valve. Six of the patients(Cases I2, I5, 17, i8, I9, and 23) were referred for aorticvalve replacement shortly after the echocardiographicexamination. An echocardiographic study was attemptedin 4 other patients with aortic regurgitation but satis-factory recordings were not obtained.
2. Normal subjectsTwenty-one healthy subjects, mainly medical students,were studied as one control group. Their ages rangedfrom 20 tO 29; i8 were men and 3 were women.
3. Patients with cardiomyopathyEchocardiographic studies were made in 6 subjects whohad large left ventricles but no evidence of valvar re-gurgitation, as a second control group. The diagnosis inthese subjects was congestive cardiomyopathy and all hadhad evidence of left ventricular failure. Patients withclinical or electrocardiographic evidence of coronaryartery disease were excluded as the left ventricles ofsuch patients may show asymmetrical contraction. Fiveof these patients were in sinus rhythm and one was inatrial fibrillation.
Subjects were studied supine or lying inclined to theleft and echocardiographic recordings were obtainedwith an Ekoline 20 ultrasonoscopel using a 2.25 MHzI.5 cm transducer, with a pulse repetition frequency ofIooo/s. The transducer was positioned at the left sternaledge and angled to identify the mitral valve echo andthen pointed more laterally and inferiorly until the leftside of the interventricular septum and the endocardiumof the posterior wall of the left ventricle could be clearlyidentified. During the early part of the study recordingswere obtained on Polaroid film, but subsequently re-cordings were made on direct print recording paperusing a Kent Cambridge fibre-optic strip chart recorder.2The diastolic diameter (Dd) of the left ventricle wasmeasured at the time of inscription of the main peak ofthe QRS complex of the electrocardiogram and thesystolic diameter (Ds) was taken as the minimum dia-meter of the left ventricle following ventricular con-traction (Fig. i). Total stroke volume was calculatedfrom (Dd3- DsO) and total left ventricular output as(stroke volume x heart rate). Ejection fraction was
'Smith Kline Instrument Co. Ltd.2Kent Cambridge Medical Ltd.
FIG. i Echocardiographic trace, recorded on Pola-roid film, showing diastolic (Dd) and systolic (Ds)diameters of the left ventricle.
calculated as (Dd3 DS3) Measurements were usuallymade from recordings of 2 to 4 cardiac cycles, and whenmeasurements varied between cycles the mean wastaken. In the patient with atrial fibrillation the mean of 8cycles was taken.
ReproducibilityIn 22 subjects a second echocardiographic recordingwas made at an interval of not less than 5 minutes afterthe first recording, and both first and second recordingswere subsequently read 'blind', with no knowledge ofthe identity of the subjects.
Independent assessment of severity of aorticregurgitationTo provide a comparison with the echocardiographicdata, an assessment of the severity of aortic regurgita-tion was made by one of us (D.W.B.) who had no know-ledge of the echocardiographic findings. This assessmentwas based on the clinical, radiographic, and electro-cardiographic findings. Particular emphasis was placedon the pulse pressure, cardiothoracic ratio on the chestradiograph, and signs of left ventricular hypertrophy onthe electrocardiogram. Haemodynamic data from cardiaccatheterization and cine-aortographic studies were avail-able in 13 of the 27 patients. From this information thepatients were placed in one of three grades of severity;mild (grade I), 5 patients; moderate (grade II), 6patients; severe (grade III), I6 patients. All 6 patientswho were subsequently referred for aortic valve replace-ment were placed in grade III.
Postoperative studyEchocardiographic studies were made postoperatively in
on 22 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.7.691 on 1 July 1975. Dow
Echocardiographic assessment of aortic regurgitation 693
3 of the patients and in 2 additional subjects, one ofwhom was originally excluded from the study because ofleft bundle-branch block and, therefore, only his leftventricular diastolic diameter was measured. Thesecond subject became available after the original serieswas completed.
Statistical methodStatistical significances between group values were cal-culated by analysis of the variance ratio.
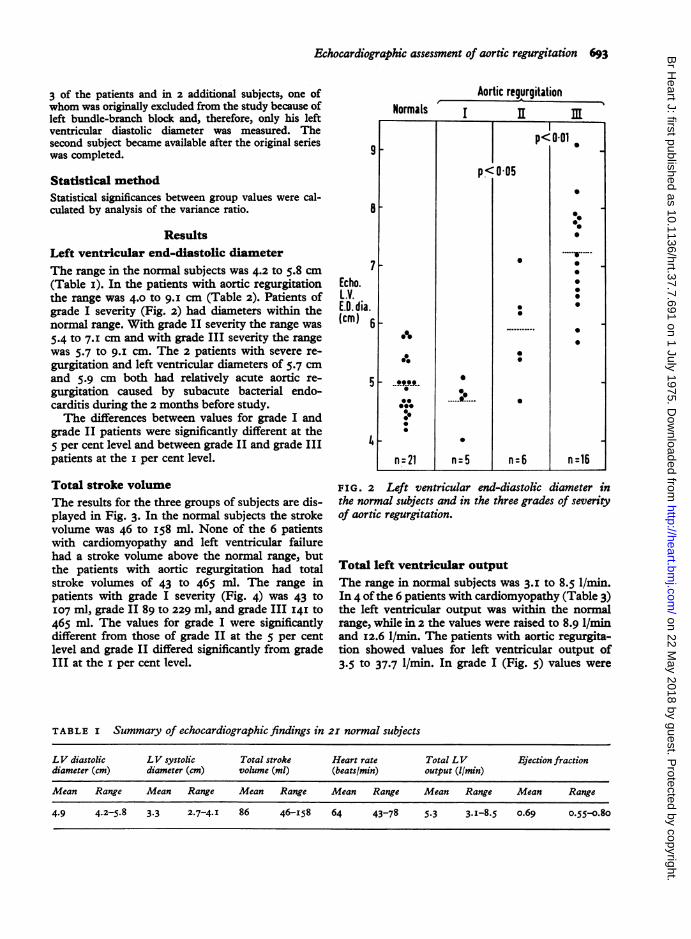
ResultsLeft ventricular end-diastolic diameterThe range in the normal subjects was 4.2 to 5.8 cm(Table I). In the patients with aortic regurgitationthe range was 4.0 tO 9.I cm (Table 2). Patients ofgrade I severity (Fig. 2) had diameters within thenormal range. With grade II severity the range was5.4 tO 7.1 cm and with grade III severity the rangewas 5.7 tO 9.I cm. The 2 patients with severe re-gurgitation and left ventricular diameters of 5.7 cmand 5.9 cm both had relatively acute aortic re-gurgitation caused by subacute bacterial endo-carditis during the 2 months before study.The differences between values for grade I and
grade II patients were significantly different at the5 per cent level and between grade II and grade IIIpatients at the i per cent level.
Total stroke volumeThe results for the three groups of subjects are dis-played in Fig. 3. In the normal subjects the strokevolume was 46 to I58 ml. None of the 6 patientswith cardiomyopathy and left ventricular failurehad a stroke volume above the normal range, butthe patients with aortic regurgitation had totalstroke volumes of 43 tO 465 ml. The range inpatients with grade I severity (Fig. 4) was 43 tOI07 ml, grade II 89 to 229 ml, and grade III 141 tO465 ml. The values for grade I were significantlydifferent from those of grade II at the 5 per centlevel and grade II differed significantly from gradeIII at the i per cent level.
Aortic regurgitation
91F
7Echo.L.V.E.D. dia.(cm) 6
5
q1
Ip<OO1I
p<O0os
n-21n-5 n-6 n~~Pc'-016
0
0~00
0%~~~~~~~~~~0
000
=01n=5n 1
FIG. 2 Left ventricular end-diastolic diameter inthe normal subjects and in the three grades of severityof aortic regurgitation.
Total left ventricular output
The range in normal subjects was 3.I to 8.5 1/min.In 4 of the 6 patients with cardiomyopathy (Table 3)the left ventricular output was within the normalrange, while in 2 the values were raised to 8.9 1/minand I2.6 1/min. The patients with aortic regurgita-tion showed values for left ventricular output of3.5 to 37.7 1/min. In grade I (Fig. 5) values were
TABLE I Summary of echocardiographic findings in 21 normal subjects
LV diastolic LV systolic Total stroke Heart rate Total LV Ejection fractiondiameter (cm) diameter (cm) volume (ml) (beats/min) output (I/min)
Mean Range Mean Range Mean Range Mean Range Mean Range Mean Range
TABLE 2 Diagnoses and echocardiographic findings in patients with aortic regurgitation
Severity of Case Age (yr) Diagnosis LV diastolic LV systolic Total stroke Heart Total LV Ejectionaortic regur- No. and diam. (cm) diam. (cm) vol. (ml) rate output fractiongitation sex (Ilmin)
I
Grade I 4
l1~6
78
Grade II 9IOII
31 F32 M49 F29 F
43 F
49 M
i6 M36 M39 MI3 M33 M
CHD, AR (AS)RHD, ARRHD, AR, MS3 valve replace-
ment, ARCHD, AR (AS)RangeMean
4.95.'4-7
4.04.84.0-5.I4.7
2.13.42.7
2.72.22.1-3.42.6
RHD, AR, (AS),SBE 5.4 2.7
AR 5.5 3.IRHD, AR, SBE 6.3 4.5AR 7.1 5.0CHD, AR 6.2 3.9AR 4.7 2.3Range 4.7-7.1 2.3-5.0Mean 5.9 3.6
12 35 M RHD, AR, SBEI3 42 M RHD, AR14 60 M AR, dissecting
aneurysmI5 44 M AR, SBEi6 27 M CHD, AR, PS17 57 F RHD, ARi8 43 M Leak around
ao. Starrvalve
I9 31 F Leak aroundao. Starrvalve,SBE
20 31 M AR, SBE2I 50 M AR, Reiter's
syndrome22 39 M AR, SBE23 52 M RHD, AR, SBE24 56 M AR, SBE25 57 F AR, dissecting
FIG. 3 Total stroke volume, estimated by echo-cardiography, in the three groups of subjects.
3.5 tO IO.O 1/min, in grade II 5.5 tO I4.8 1/min, andin grade III I2.2 tO 37.7 I/min. Grade I differedsignificantly from grade II at the 5 per cent leveland grade II from grade III at the 2 per cent level.
Ejection fractionFig. 6 shows the relation between left ventricularend-diastolic diameter and derived total strokevolume in the three groups of subjects. The linejoins theoretical points having an ejection fractionof o.s. The patients with cardiomyopathy and leftventricular failure had inappropriately large leftventricles for stroke volumes within the normalrange. They were clearly separated from thosepatients with aortic regurgitation who had a similar
FIG. 4 Total stroke volume in the nornnal subjects,and in the three grades of severity of aortic regurgita-tion.
left ventricular diameter but much larger strokevolume. These relations between left ventriculardiameter and stroke volume are summarized in theejection fractions shown in Fig. 7.The range of ejection fraction in the normal sub-
jects was 0.55 to o.80. In the patients with cardio-myopathy and left ventricular failure the range was0.10 tO 0.39. The patients with aortic regurgitationshowed a wider range of values than the normal sub-jects but only one patient showed an ejection frac-tion below the normal range. This patient (Case I3)
TABLE 3 Echocardiographic findings in patients with cardiomyopathy and left ventricular failure
Case No. Age (yr) and LV diastolic LV systolic Total stroke Heart rate Total LV Ejectionsex diameter (cm) diameter (cm) volume (ml) output fraction
I 5I M 7.2 6.3 II5 110 I2.6 0.3I2 48 M 6.7 6.i 68 88 6.o 0.233 57M 7.4 6.6 117 76 8.9 0.294 49 M 6.3 5.7 67 97 6.5 0.275 20 M 6.6 6.4 29 103 3.0 0.106 57 M 6.8 5.8 126 57 7.I 0.39
with an ejection fraction of o.44 was a man of 42with severe aortic regurgitation but very mildbreathlessness on exertion. At cardiac catheteriza-tion two days previously he had shown a mild in-crease in left ventricular end-diastolic pressure atI4 mmHg (i.9 kPa) and his pulmonary wedge
Aortic regurgitation
L40
30
Echo.L.V.output(L/min.)
20
10
FIG.subjects atregurgitat2
FIG. 6 2diastolic dithree groupoints havi
Ejectionfraction
FIG. 7subjects.
AorticNormals regurgitation L.VF.
Ejection fraction in the three groups of
" I[ I pressure on exercise rose to 30 mmHg (4.0 kPa).0 n=21 n=5 n=6 n=16 There were 6 other patients (Cases I2, I4, 15, I7,
22, and 23) who had had cardiac catheterizationTotal left ventricular output in the normal within 4 weeks of the echocardiographic study andid in the three grades of severity of aortic had shown left ventricular end-diastolic pressures or
ion. pulmonary wedge pressures raised at levels betweeni8 and 50 mmHg (2.4 and 6.7 kPa) and none ofthese patients had an ejection fraction depressedbelow the normal range. None of the 6 patients who
0,, were referred for aortic valve replacement shortly
* Normals (n :21) after the echocardiographic study showed a de-o Aortic regurgitation In :27) pressed ejection fraction.A,LV.F. (n=6)
Reproducibility study0 The second measurement of left ventricular end-
00 / diastolic diameter was within I0 per cent of the first
0 °000 / ° measurement in all 22 pairs of recordings, and° 00/(0 5 ejectionfratti - agreement was within 5 per cent for 20 of the 22
000/ pairs of recordings. The paired measurements of
0 stroke volume agreed within I5 per cent for i8 of00.. A A the 22 pairs, and for left ventricular output the4%* , , readings were within I5 per cent for I9 of the 22
~~~~~~~pairs.A
5 6 7 a 9 Postoperative studyEcho.LV E.D.dia.(cm) In all 5 patients who were studied at intervals of I3
rhe relation between left ventricular end- days to i i weeks after operation, the left ventricularsameter and estimated stroke volume in the diastolic diameter had decreased to within the normallps of subjects. The line joins theoretical range (Table 4). In the 4 patients without left bundle-ing an ejection fraction of 0.5. branch block, the total stroke volume and total left
Normals I IL l
<02I P0-020
p<0 050#,...v....
00q
. : ~~~~~~~~~......---0 ~~~~0 0
0 ....._v s .
on 22 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.7.691 on 1 July 1975. Dow
ventricular output had also fallen to within thenormal range.
DiscussionIn dominant aortic regurgitation, total stroke vol-umes of up to 390 ml/min and left ventricular out-puts of up to 28 I/min have been recorded by quanti-tative angiography and stroke volumes of up to4IO ml and left ventricular outputs of up to 36 I/minby dye dilution methods (Miller et al., I965; Franket al., I966). Such greatly increased stroke volumescan be obtained only by an increased diastolicvolume. Echocardiography by measuring left ven-tricular diameter appears to be a particularly suit-able method of assessing the increased diastolicsize.The chest radiograph is probably a poor method
of accurately assessing left ventricular size in aorticregurgitation. When compared with angiography thechest radiograph has been shown to be a poor pre-dictor of left ventricular size after myocardial in-farction (Feild et al., I974). In our series of patientswith aortic regurgitation, left ventricular diameterwas significantly larger with increasing clinicalseverity in the three grades into which the patientswere subdivided.The single beam pulse echocardiographic tech-
nique used measures only one diameter of the leftventricle and derivation of left ventricular volumefrom the single measurement relies on the assump-tion that the shape of the left ventricle is that of aprolate ellipse. Derivation of stroke volume alsoassumes symmetrical contraction. All the informa-tion obtained regarding left ventricular dimensionsis contained in the values recorded from the leftventricular diastolic diameter and systolic diameter,and the only attraction of expressing these values as
volumes is to put the information in a familiar andmeaningful form, as a unit of contraction of dia-meter in a large ventricle results in a greater volumechange than it does in a small ventricle. It has beensuggested that the cube formula for deriving leftventricular volumes from the left ventricular dia-meter exaggerates the volume in larger ventricles,and Fortuin et al. (I97I) used a regression equationinstead of a cube formula to obtain left ventricularvolume. However, other workers have found that thecube formula remains reasonably accurate over awide range of left ventricular size (Pombo et al.,I971; ten Cate et al., I974). From the examinationof our data for patients with cardiomyopathy andleft ventricular failure, it appears likely that thestroke volume and left ventricular outputs areexaggerated in some of these patients though wehave no other measurement of output for compari-son. However, there is a striking difference in strokevolume between these patients and the patients withaortic regurgitation who have left ventricles ofsimilar size. While accepting that the stroke volumesand left ventricular outputs are approximate, theydo show significantly increased values with in-creasing severity of aortic regurgitation in the threegroups. It is noteworthy that the 2 patients (CasesI5 and 23) with severe regurgitation yet high normalor modestly raised values for left ventricular end-diastolic diameter, stroke volume, and total left ven-tricular output, are the 2 patients with relatively acuteaortic regurgitation because of a recent subacutebacterial endocarditis. It is likely that in such patientsthe severity of the clinical picture is caused by thehigh left ventricular end-diastolic pressure and leftatrial pressure which results from a relatively smallvolume of blood regurgitating into a chamber whichis less compliant than that associated with long-standing regurgitation. This raised left ventricular
on 22 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.7.691 on 1 July 1975. Dow
end-diastolic pressure does not imply myocardialfailure (Braunwald and Ross, I963).
Miller et al. (i965), Tyrrell et al. (I970), andChatterjee et al. (I97I) have shown that the ejectionfraction is frequently well maintained even in theface of severe aortic regurgitation. Chatterjee et al.reported that left ventricular end-diastolic pressure,unlike ejection fraction, was a poor index of leftventricular dysfunction. Only one of our patientsshowed a depressed ejec-tion fraction, but, as indi-cated above, there was a high proportion of patientsin the series who had relatively acute aortic regurgi-tation in which the symptoms and haemodynamicdisturbance may not necessarily reflect myocardialdysfunction.Our assessment of the value of echocardiography
in aortic regurgitation has been limited to a correla-tion with three grades of severity assessed by othermeans. To define further the sensitivity of themethod, it would be necessary to compare echo-cardiographic findings with a continuously variablemethod of assessment of regurgitation such asquantitative angiography.Our small group of preoperative and postopera-
tive recordings showed that in all 5 patients theleft ventricular diameter was reduced to within thenormal range, and similar changes in stroke volumeand total left ventricular output occurred in thosepatients in whom these parameters could be esti-mated. These findings are in accordance with thefindings of Kennedy et al. (I968) who reported thatin dominant aortic regurgitation the left ventricularend-diastolic volumes and left ventricular strokevolumes decreased towards normal in the absence ofpostoperative aortic regurgitation.
ConclusionsThe main value of echocardiographic study of theleft ventricle in aortic regurgitation is that it offersa more accurate measurement of left ventricularchamber size in diastole than is possible from theplain chest radiograph. This information is of value,as in chronic and severe aortic regurgitation leftventricular size must increase if forward output isto be maintained. Further information may beobtained from the degree of shortening of the leftventricular diameter in systole and this may beconveniently expressed as a volume and an ejectionfraction. By detecting a depressed ejection fractionthe method may be of diagnostic value in a patientwith aortic regurgitation and myocardial failurecaused by the regurgitation or some other factor. Itis possible that repeated studies in the long termfollow-up of patients with aortic regurgitation maygive early warning ofmyocardial failure by detecting
an ejection fraction which is falling while still re-maining within the normal range.
We thank Dr. F. G. M. Ross and the staff of the De-partment of Ultrasonics, for allowing us to use thefacilities of the department, and for criticism, and Dr.J. Russell Rees and Dr. S. C. Jordan for permitting usto study their patients.
References
Braunwald, E., and Ross, J., Jr. (I963). Editorial. The ven-tricular end-diastolic pressure. American Journal of Medi-cine, 34, I47.
Cate, F. J. ten., Kloster, F. E., van Dorp, W. G., Meester,G. T., and Roelandt, J. (I974). Dimensions and volumesof left atrium and ventricle determined by single beamechocardiography. British Heart_Journal, 36, 737.
Chapelle, M., and Mensch, B. (I969). etude des variations dudiametre ventriculaire gauche chez l'homme par echo-cardiographie transthoracique. Archives des Maladies duCoeur et des Vaisseaux, 62, I505.
Chatterjee, K., Sacoor, M., Sutton, G. C., and Miller,G. A. H. (I97I). Assessment of left ventricular functionby single plane cineangiographic volume analysis. BritishHeart Journal, 33, 565.
Cohn, L. H., Mason, D. T., Ross, J., Jr., Morrow, A. G., andBraunwald, E. (I967). Preoperative assessment of aorticregurgitation in patients with mitral valve disease. Ameri-can Journal of Cardiology, I9, I77.
Danford, H. G., Danford, D. A., Mielke, J. E., and Peterson,L. F. (I973). Echocardiographic evaluation of the hemo-dynamic effects of chronic aortic insufficiency withobservations on left ventricular performance. Circulation,48, 253.
Feigenbaum, H., Zaky, A., and Nasser, W. K. (I967). Use ofultrasound to measure left ventricular stroke volume.Circulation, 35, 1092.
Feild, B. J., Russell, R. 0., Jr., Moraski, R. E., Soto, B., Hood,W. P., Jr., Burdeshaw, J. A., Smith, M., Maurer, B. J.,and Rackley, C. E. (I974). Left ventricular size and func-tion and heart size in the year following myocardial in-farction. Circulation, 50, 331.
Fortuin, N. J., Hood, W. P., Sherman, M. E., and Craige, E.(I97I). Determination of left ventricular volumes by ultra-sound. Circulation, 44, 575.
Frank, M. J., Casanegra, P., Nadimi, M., Migliori, A. J., andLevinson, G. E. (1966). Measurement of aortic regurgita-tion by upstream sampling with continuous infusion ofindicator. Circulation, 33, 545.
Gibson, D. G. (1973). Estimation of left ventricular size byechocardiography. British Heart Journal, 35, I28.
Kennedy, J. W., Twiss, R. D., Blackmon, J. R., and Meren-dino, K. A. (I968). Hemodynamic studies one year afterhomograft aortic valve replacement. Circulation, 37 and38, Suppl. II, I Io.
McDonald, I. G. (1973). Echocardiographic demonstration ofabnormal motion of the interventricular septum in leftbundle branch block. Circulation, 48, 272.
Miller, G. A. H., Kirklin, J. W., and Swan, H. J. C. (I965).Myocardial function and left ventricular volumes inacquired valvular insufficiency. Circulation, 31, 374.
on 22 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.7.691 on 1 July 1975. Dow
Echocardiographic assessment of aortic regurgitation 6g
Pombo, J. F., Troy, B. L., and Russell, R. O., Jr. (I97i). Leftventricular volumes and ejection fraction by echocardio-graphy. Circulation, 43, 480.
Popp, R. L., and Harrison, D. C. (1970). Ultrasonic cardiacechography for determining stroke volume and valvularregurgitation. Circulation, 41, 493.
Tyrrell, M. J., Ellison, R. C., Hugenholtz, P. G., and Nadas,
A. S. (I970). Correlation of degree of left ventricularvolume overload with clinical course in aortic and mitralregurgitation. British Heart journal, 32, 683.
Requests for reprints to Dr. K. E. Gray, Barnet GeneralHospital, Wellhouse Lane, Barnet, Herts EN5 3DJ.
on 22 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.7.691 on 1 July 1975. Dow