23
ECMO ECMO
| Date post: | 24-Dec-2015 |
| Category: |
Documents |
| Upload: | grace-patrick |
| View: | 217 times |
| Download: | 0 times |

ECMOECMO


Introduction
ECMO is frequently instituted using cervical cannulation, which can be performed under local anesthesia.
ECMO is used for longer-term support ranging from 3-10 days.
The purpose of ECMO is to allow time for intrinsic recovery of the lungs and heart

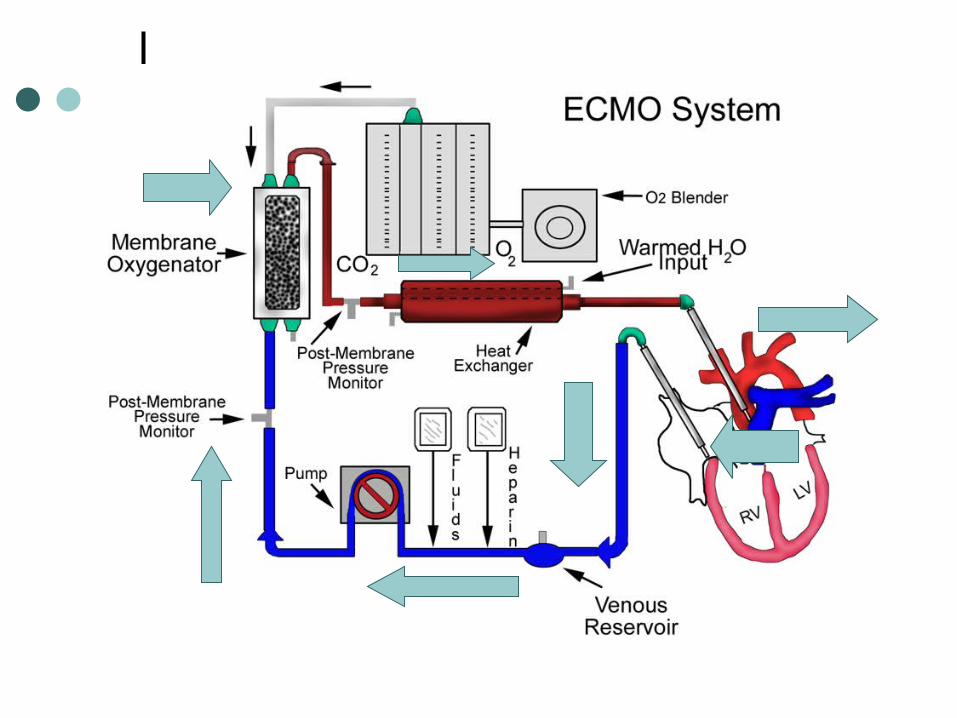
Equipment
Blood pump with raceway tubing, a venous reservoir, a membrane oxygenator, and a countercurrent heat exchanger
The blood pump is either a simple roller pump or a constrained vortex centrifugal pump. The roller pump causes less hemolysis and is used for neonatal ECMO. The oxygenator is responsible for exchanging both oxygen and carbon dioxide and is central to the successful performance of prolonged ECMO.

Neonatal extracorporeal membrane oxygenation Patients with the following 2 major neonatal
diagnoses require the use of extracorporeal membrane oxygenation (ECMO): Primary diagnoses associated with primary
pulmonary hypertension of the newborn (PPHN), including idiopathic PPHN, meconium aspiration syndrome, respiratory distress syndrome, group B streptococcal sepsis, and asphyxia
Congenital diaphragmatic hernia (CDH)

Selection criteria for neonates
Gestational age of 34 weeks or more Birth weight of 2000 g or higher No significant coagulopathy or uncontrolled bleeding No major intracranial hemorrhage (grade 1 intracranial
hemorrhage) Mechanical ventilation for 10-14 days or less Reversible lung injury No lethal malformations No major untreatable cardiac malformation Failure of maximal medical therapy Failure to meet these criteria is a relative
contraindication for ECMO

Qualifying patient criteria for ECMO Qualifying criteria are applied only when the infant
has reached maximal ventilatory support of 100% oxygen with peak inspiratory pressures (PIP) often as high as 35 cm H2 O.
Alveolar-arterial (A-a) gradient of 600-624 mm Hg for 4-12 hours at sea level, which may be computed as follows (where 47=partial pressure of water vapor): (A-a)(Diffusing capacity [D] of O2 equals atmospheric
pressure - 47 - (PaCO2 + PaO2])/FiO2

Qualifying patient criteria for ECMO
Oxygenation index (OI) greater than 40 in 3 of 5 postductal gas determinations obtained 30-60 minutes apart, which may be computed as follows (where MAP is mean airway pressure):
OI = (MAP x FiO2 x 100)/ PaO2 PaO2 = 35-50 mm Hg for 2-12 hours Acute deterioration PaO2 less than or equal to 30-40 mm Hg for 2
hours pH less than or equal to 7.25 for 2 hours Intractable hypotension
Pediatric ECMO
Low cardiac output resulting from right, left, and biventricular failure following repair of congenital heart defect
Pulmonary vasoreactive crisis following repair of congenital heart defect leading to severe hypoxemia, low cardiac output, or both
Rarely, as a bridge to cardiac surgery in patients with serious end-organ damage resulting from profound low cardiac output related to congenital heart disease

Types of ECMO
Venoarterial bypass. a cannula is placed through the right jugular vein into the right atrium. Blood is drained to a venous reservoir located 3-4 feet below heart level. The blood is actively pumped by a roller pump through the oxygenator, where gas exchange occurs via countercurrent flow of blood and gas. Next, the blood is warmed to body temperature by the heat exchanger before returning to the patient through a cannula placed through the right carotid artery into the aortic arch. Systemic anticoagulation therapy with heparin is administered throughout the bypass circuit, with frequent monitoring of activated clotting time (ACT), which should be maintained at 180-240 seconds.


Types of ECMO
venovenous bypass, a double-lumen cannula is placed through the right jugular vein into the right atrium. Desaturated blood is withdrawn from the right atrium through the outer fenestrated venous catheter wall, and oxygenated blood is returned through the inner lumen of the catheter and is angled to direct blood across the tricuspid valve.

Venoarterial ECMO Venovenous ECMO
Higher PaO2 is achieved. Lower PaO2 is achieved.
Lower perfusion rates are needed.
Higher perfusion rates are needed.
Bypasses pulmonary circulation Maintains pulmonary blood flow
Decreases pulmonary artery pressures
Elevates mixed venous PO2
Provides cardiac support to assist systemic circulation
Does not provide cardiac support to assist systemic circulation
Requires arterial cannulation Requires only venous cannulation

Clinical Management-Pulmonary ECMO is used temporarily while awaiting pulmonary
recovery. The typical ventilator settings are FiO2 of 21-30%, PIP
of 15-25 cm H2 O, a positive end-expiratory pressure (PEEP) of 3-5 cm H2 O, and intermittent mechanical ventilation (IMV) of 10-20 breaths per minute. In some centers, a high PEEP of 12-14 cm H2 0 has been used to avoid atelectasis; this has been found to shorten the bypass time in infants. Pulmonary hygiene is strict and requires frequent positional changes, endotracheal suctioning every 4 hours depending on secretions, and a daily chest radiograph.
Clinical Management-Cardiovascular
Systemic perfusion and intravascular volume should be maintained. Volume status can be assessed clinically by urine output and physical signs of perfusion and by measuring the central venous pressure and the mean arterial blood pressure. Native cardiac output can be enhanced with inotropic agents. Echocardiography should be performed to exclude any major congenital heart anomaly that may require immediate intervention other than ECMO

Clinical Management-CNS
CNS complications are the most serious and are primarily related to the degree of hypoxia and acidosis. Avoiding paralytic agents and performing regular neurologic examinations are recommended. If feasible, head ultrasonography should be performed before beginning ECMO in a neonate. Reevaluation with serial head ultrasonography may be needed on a daily basis, especially after any major event. In patients with seizures or suspected seizures, aggressive treatment is recommended (eg, phenobarbital)

Clinical Management-Renal
During the first 24-48 hours on ECMO, oliguria and acute tubular necrosis associated with capillary leak and intravascular volume depletion are common because ECMO triggers an acute inflammatory like reaction. The diuretic phase, which usually begins within 48 hours, is often one of the earliest signs of recovery. If oliguria persists for 48-72 hours, diuretics are often required to reduce edema. When renal failure does not improve, hemofiltration or hemodialysis filters may be added to the circuit.

Clinical Management-Hemalogic To optimize oxygen delivery, the patient's
hemoglobin should be maintained at 12-15 g/dL using packed RBCs (pRBCs). As a result of platelet consumption during ECMO, platelet transfusions are required to maintain platelet counts above 100,000/mcL. Activated clotting time (ACT) should be maintained at 180-240 seconds to avoid bleeding complications.

Clinical Management- Infection
Strict aseptic precautions are required. The presence of infection is monitored by obtaining cultures from the circuit at least once a week. Based on institutional experience, the protocol frequency may vary. Other appropriate cultures (eg, fungal and viral) should be obtained as needed.

Clinical Management-Fluids
Patients on ECMO require close monitoring of fluids and electrolytes. The high-energy requirements should be met using hyperalimentation techniques. The patient's weight increases in the first 1-3 days on ECMO because of fluid retention.
Hazards
As the blood travels around the circuit, there is a risk of clots forming as the blood is outside the body and in contact with the plastic of the circuit.
There is a risk of infection with any invasive procedure
When the blood in the body is thinned, bleeding into the head may occur.

ECMO Lecture
http://www.youtube.com/watch?v=rmGM984aVKU
http://www.youtube.com/watch?v=ISHOFf5QMyc

















