Articles Economic Activity and Congenital Anomalies: An Ecologic Study in Argentina Eduardo E. Castilla,1'2 Hebe Campala,3 Jorge S. L6pez Camelo,3 and the ECLAMC ECOTERAT Group* 1ECLAMC (Latin-American Collaborative Study of Congenital Malformations, WHO Collaborating Centre for the Prevention of Birth Defects), Instituto Oswaldo Cruz, Rio de Janeiro, Brazil; 2ECLAMC, Centro de Educaci6n M6dica e Investigaciones Clinicas, Buenos Aires, Argentina; 3ECLAMC, Instituto Multidisciplinario de Biologia Celular, La Plata, Argentina In this study, we anlyze the association between industrial activity and the occurrence of 34 con- genital anomalies. We selected 21 counties in Argentina during 1982-1994 and examined a tota of 614,796 births in these counties in consecutive series. We used the International Standard Indunril Clwsficaion of All EconomicActivties (United Nations, 1968) as an indicator of expo- sure to 80 specific industrial actiities. Incidence rate ratios for each congenital anomaly were adjusted by the socioeconomic level of the county according to a census index of social deprivation. For a given exposurelanomaly association to be considered as significant and relevant, the exposure had to be a satisstic sgnificant risk for the occurrence of the anomaly and an increase in the birth prevaence. rate of the congeni tal anomaly type involved had to be observed in those counties where the putative caual activity was being performed. Significant associations (p < 0.01) were identified between textile industry and anencephaly, and between the manufucture of engines and turbines and microcephaly. These observations are consistent with previous reports on occupa- tional exposure, and their further int on by means of case-control studies is recommended. Key work anencephaly, antonotive industry, congenital anomaly, fur-dyeing industrial activity, pes equinovarus, ttile. Envron Perpe 108:193-197 (2000). [Onlie 19 January 2000] hap:llehpnatl.bnies.nib.goWdou/:0001108p13-l97catabstractbtml Chronic exposure to environmental pollu- tants, before or after conception, is suspected to affect reproduction through cellular dam- age or death, which may lead to infertility, fetal loss, intrauterine growth retardation, and the occurrence of birth defects, both functional and anatomical, in the progeny of the exposed population (1). Nevertheless, the number of proven teratogenic pollutants is still quite limited. The most outstanding examples are methylmercury, which causes central nervous system damage () and ioniz- ing radiation (3) and lead (4) contamination, which cause microcephaly and mental retar- dation. The scarcity of proven examples of environmental teratogens could be due to methodologic limitations imposed by a possi- ble exposure to a weak teratogen, which affects the entire population or a very large part of it. The exiguous information available on this subject, as well as the serious concern of the community about environmental repro- ductive risks, justifies an exploratory study such as this one, in which we compare birth prevalence rates for specific types of malfor- mation in populations who are either exposed or unexposed to a given industrial activity. To propose potentially teratogenic envi- ronmental pollutants, we base our study approach on two assumptions: * Because environmental protection is almost completely lacking in the develop- ing world, industrial activities can be taken as a proxy for specific types of pollutants. * Because most teratogens are effect specific (they produce a given type or pattern of congenital anomalies), a teratogenic pollu- tant is expected to be associated with a spe- cific type of congenital anomaly instead of with birth defects in general. We aimed to test the association between industrial activity and congenital anomalies in small areas (counties) of Argentina, as sampled out by the Latin American Collaborative Study of Congenital Malformations (ECLAMC) (5). Subjects and Methods The data presented here include 614,796 births of a consecutive birth series during 1982-1994 in 36 maternity hospitals partic- ipating in the ECLAMC (5). The ECLAMC is a hospital-based registry of birth defects. All consecutive live and stillborn infants weighing . 500 g were examined by a trained pediatrician according to definitions given in a ECLAMC procedures manual (6). The 36 hospitals were selected for this study because they are located in 21 counties of Argentina where the ECLAMC included at least 20% of all births that occurred during the study period. For each county, Table 1 specifies name, geographic location, mean socioeconomic level indicator, number of performed indus- trial activities, number of annual births, and ECLAMC sample characteristics (i.e., num- ber of maternity hospitals, number of births, and the period covered). The large metro- politan area of Buenos Aires, Argentina, was omitted because of residential mobility and highly heterogeneous economical activities. From the ECLAMC database of prospectively registered congenital anomalies, we included only 34 major isolated anomaly types, with a sample size of at least 20 observed cases (Table 2). We excluded multiple malformed infants and chromosome anomalies except Down syndrome. Each of 80 industrial activities was used as an exposure factor. The activities carried out in each county were obtained from the Argentine National Economic Census of 1985 (7) coded according to the International Standard Industrial Classification of All Economic Activities (8). For each activity in turn, the counties were grouped into those where the activity was carried out and those where it was not; the prevalence of each mal- formation at birth in the two groups was compared. Because in developing countries some industrial activities are closely related to the socioeconomic level of the community (5), we considered this variable to be a poten- tial confounding factor. The mean socioeco- nomic level in each county was established through the NBI (Necesidades Basicas Insatisfechas), a social deprivation index (1J) that defines poverty according to unsatisfacto- ry conditions for housing, health, and school attendance (11). According to their NBI Address correcpondence to E.E. Castilla, Genetical Fiocruz, ECLAMA, CP 926, Rio de Janeiro 20001- 970 Brazil. Telephone: 55 21 552 8952. Fax: 55 21 260 4282. E-mail: [email protected]*The ECLAMC ECOTERAT Group includes A. Echegaray, Maternidad Provincial, Cordoba; C. Alazard, Hospital del Centenario, Gualeguaychui; C. de Rosas, Hospital Italiano, Mendoza; C. Negri, Hospital Ferrupato, San Martin; C. Picon, Hospital Perrando, Resistencia; C. Saleme. Maternidad de Tucuman, Tucuman; C. Rivelis, Hospital San Roque, Parana; J.C. Mereb, Hospital de Area, El Bolson; L. Salgado, Hospital Melendez, Adrogue; M. Mussi, Maternidad Martin, Rosario; M. Lerner, Hospital del Centenario, Gualeguaychu; M. Rittler, Maternidad Sarda, Buenos Aires; M. Roubicek, Hospital de la Comunidad, Mar del Plata; R. Lombardelli, Hospital Zonal, Esquel; and S. Morales, Maternidad Martin, Rosario. This study was supported by the Consejo Nacional de Investigaciones Cientificas y Tecnicas and the Comision de Investigaciones Cientificas de la provincia de Buenos Aires of Argentina, the Conselho Nacional de Desenvolvimento Cientffico e Tecnologico of Brazil, and the Programa de Apoio a Pesquisa Estrat6gica em Saude da Fiocruz, of Brazil. Received 26 May 1999; accepted 14 September 1999. Environmental Health Perspectives * Volume 108, Number 3, March 2000 193 brought to you by CORE View metadata, citation and similar papers at core.ac.uk provided by PubMed Central
Transcript
Articles
Economic Activity and Congenital Anomalies: An Ecologic Study inArgentinaEduardo E. Castilla,1'2 Hebe Campala,3 Jorge S. L6pez Camelo,3 and the ECLAMC ECOTERAT Group*1ECLAMC (Latin-American Collaborative Study of Congenital Malformations, WHO Collaborating Centre for the Prevention of BirthDefects), Instituto Oswaldo Cruz, Rio de Janeiro, Brazil; 2ECLAMC, Centro de Educaci6n M6dica e Investigaciones Clinicas, Buenos Aires,Argentina; 3ECLAMC, Instituto Multidisciplinario de Biologia Celular, La Plata, Argentina
In this study, we anlyze the association between industrial activity and the occurrence of 34 con-genital anomalies. We selected 21 counties in Argentina during 1982-1994 and examined a totaof 614,796 births in these counties in consecutive series. We used the International StandardIndunril Clwsficaion ofAll EconomicActivties (United Nations, 1968) as an indicator of expo-sure to 80 specific industrial actiities. Incidence rate ratios for each congenital anomaly wereadjusted by the socioeconomic level of the county according to a census index of social deprivation.For a given exposurelanomaly association to be considered as significant and relevant, the exposurehad to be a satisstic sgnificant risk for the occurrence of the anomaly and an increase in thebirth prevaence. rate of the congenital anomaly type involved had to be observed in those countieswhere the putative caual activity was being performed. Significant associations (p < 0.01) wereidentified between textile industry and anencephaly, and between the manufucture of engines andturbines and microcephaly. These observations are consistent with previous reports on occupa-tional exposure, and their further int on by means of case-control studies is recommended.Key work anencephaly, antonotive industry, congenital anomaly, fur-dyeing industrial activity,pes equinovarus, ttile.Envron Perpe 108:193-197 (2000). [Onlie 19 January 2000]hap:llehpnatl.bnies.nib.goWdou/:0001108p13-l97catabstractbtml
Chronic exposure to environmental pollu-tants, before or after conception, is suspectedto affect reproduction through cellular dam-age or death, which may lead to infertility,fetal loss, intrauterine growth retardation,and the occurrence of birth defects, bothfunctional and anatomical, in the progeny ofthe exposed population (1). Nevertheless, thenumber of proven teratogenic pollutants isstill quite limited. The most outstandingexamples are methylmercury, which causescentral nervous system damage () and ioniz-ing radiation (3) and lead (4) contamination,which cause microcephaly and mental retar-dation. The scarcity of proven examples ofenvironmental teratogens could be due tomethodologic limitations imposed by a possi-ble exposure to a weak teratogen, whichaffects the entire population or a very largepart of it.
The exiguous information available onthis subject, as well as the serious concern ofthe community about environmental repro-ductive risks, justifies an exploratory studysuch as this one, in which we compare birthprevalence rates for specific types of malfor-mation in populations who are either exposedor unexposed to a given industrial activity.
To propose potentially teratogenic envi-ronmental pollutants, we base our studyapproach on two assumptions:* Because environmental protection isalmost completely lacking in the develop-ing world, industrial activities can be takenas a proxy for specific types of pollutants.
* Because most teratogens are effect specific
(they produce a given type or pattern ofcongenital anomalies), a teratogenic pollu-tant is expected to be associated with a spe-cific type of congenital anomaly instead ofwith birth defects in general.We aimed to test the association between
industrial activity and congenital anomaliesin small areas (counties) of Argentina, assampled out by the Latin AmericanCollaborative Study of CongenitalMalformations (ECLAMC) (5).
Subjects and MethodsThe data presented here include 614,796births of a consecutive birth series during1982-1994 in 36 maternity hospitals partic-ipating in the ECLAMC (5). The ECLAMCis a hospital-based registry of birth defects.All consecutive live and stillborn infantsweighing . 500 g were examined by atrained pediatrician according to definitionsgiven in a ECLAMC procedures manual (6).The 36 hospitals were selected for this studybecause they are located in 21 counties ofArgentina where the ECLAMC included atleast 20% of all births that occurred duringthe study period.
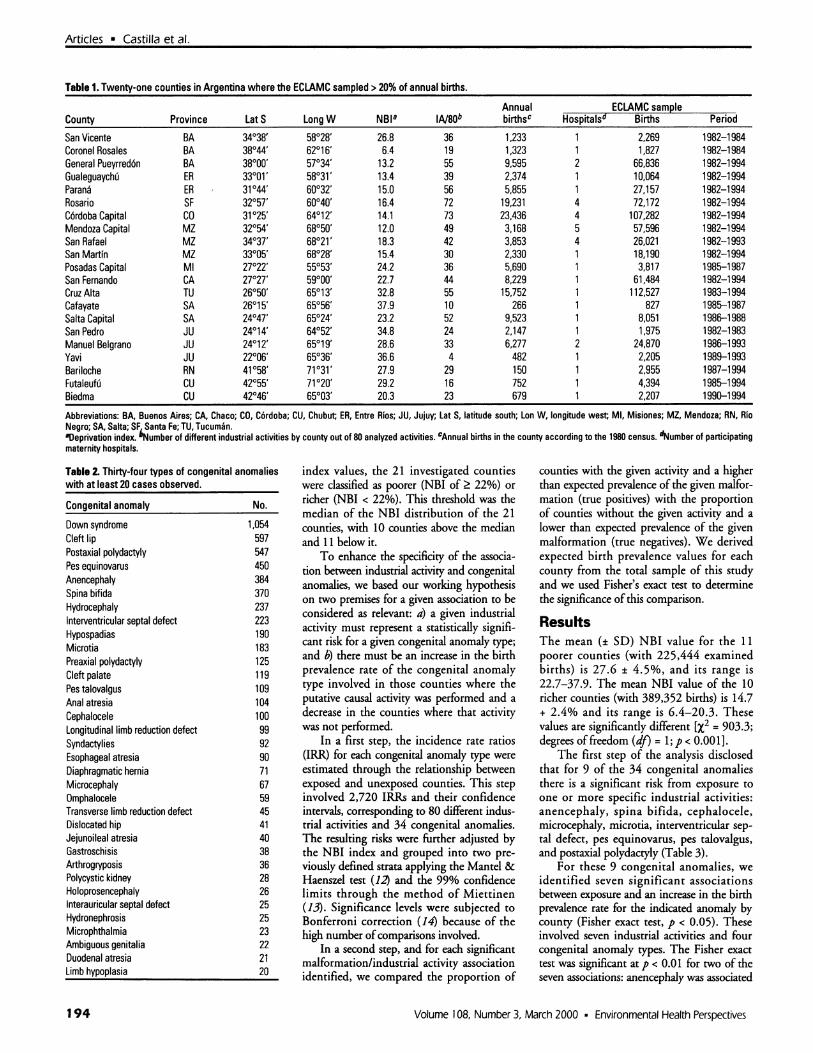
For each county, Table 1 specifies name,geographic location, mean socioeconomiclevel indicator, number of performed indus-trial activities, number of annual births, andECLAMC sample characteristics (i.e., num-ber of maternity hospitals, number of births,and the period covered). The large metro-politan area of Buenos Aires, Argentina, wasomitted because of residential mobility and
highly heterogeneous economical activities.From the ECLAMC database of prospectivelyregistered congenital anomalies, we includedonly 34 major isolated anomaly types, with asample size of at least 20 observed cases(Table 2). We excluded multiple malformedinfants and chromosome anomalies exceptDown syndrome.
Each of 80 industrial activities was used asan exposure factor. The activities carried outin each county were obtained from theArgentine National Economic Census of1985 (7) coded according to the InternationalStandard Industrial Classification ofAllEconomic Activities (8). For each activity inturn, the counties were grouped into thosewhere the activity was carried out and thosewhere it was not; the prevalence of each mal-formation at birth in the two groups wascompared. Because in developing countriessome industrial activities are closely related tothe socioeconomic level of the community(5), we considered this variable to be a poten-tial confounding factor. The mean socioeco-nomic level in each county was establishedthrough the NBI (Necesidades BasicasInsatisfechas), a social deprivation index (1J)that defines poverty according to unsatisfacto-ry conditions for housing, health, and schoolattendance (11). According to their NBI
Address correcpondence to E.E. Castilla, GeneticalFiocruz, ECLAMA, CP 926, Rio de Janeiro 20001-970 Brazil. Telephone: 55 21 552 8952. Fax: 55 21260 4282. E-mail: [email protected]*The ECLAMC ECOTERAT Group includes A.
Echegaray, Maternidad Provincial, Cordoba; C.Alazard, Hospital del Centenario, Gualeguaychui; C.de Rosas, Hospital Italiano, Mendoza; C. Negri,Hospital Ferrupato, San Martin; C. Picon, HospitalPerrando, Resistencia; C. Saleme. Maternidad deTucuman, Tucuman; C. Rivelis, Hospital SanRoque, Parana; J.C. Mereb, Hospital de Area, ElBolson; L. Salgado, Hospital Melendez, Adrogue;M. Mussi, Maternidad Martin, Rosario; M. Lerner,Hospital del Centenario, Gualeguaychu; M. Rittler,Maternidad Sarda, Buenos Aires; M. Roubicek,Hospital de la Comunidad, Mar del Plata; R.Lombardelli, Hospital Zonal, Esquel; and S.Morales, Maternidad Martin, Rosario.This study was supported by the Consejo Nacional
de Investigaciones Cientificas y Tecnicas and theComision de Investigaciones Cientificas de laprovincia de Buenos Aires of Argentina, theConselho Nacional de Desenvolvimento Cientffico eTecnologico of Brazil, and the Programa de Apoio aPesquisa Estrat6gica em Saude da Fiocruz, of Brazil.Received 26 May 1999; accepted 14 September
1999.
Environmental Health Perspectives * Volume 108, Number 3, March 2000 193
brought to you by COREView metadata, citation and similar papers at core.ac.uk
Table 1. Twenty-one counties in Argentina where the ECLAMC sampled > 20% of annual births.
Annual ECLAMC sampleCounty Province Lat S LongW NBIa 1A/80b birthsc Hospitalsd Births Period
San Vicente BA 34`38' 58028' 26.8 36 1,233 1 2,269 1982-1984Coronel Rosales BA 38044' 62016' 6.4 19 1,323 1 1,827 1982-1984General Pueyrred6n BA 38000' 57034' 13.2 55 9,595 2 66,836 1982-1994Gualeguaychu ER 33001' 58031' 13.4 39 2,374 1 10,064 1982-1994Parana ER 31044' 60032' 15.0 56 5,855 1 27,157 1982-1994Rosario SF 32057' 60040' 16.4 72 19,231 4 72,172 1982-1994C6rdoba Capital CO 31°25' 64012' 14.1 73 23,436 4 107,282 1982-1994Mendoza Capital MZ 32054' 68`50' 12.0 49 3,168 5 57,596 1982-1994San Rafael MZ 34037' 68021' 18.3 42 3,853 4 26,021 1982-1993San Martin MZ 33005' 68028' 15.4 30 2,330 1 18,190 1982-1994Posadas Capital Ml 27022' 55053' 24.2 36 5,690 1 3,817 1985-1987San Fernando CA 27027' 59°00' 22.7 44 8,229 1 61,484 1982-1994Cruz Alta TU 26050' 65013' 32.8 55 15,752 1 112,527 1983-1994Cafayate SA 26015' 65056' 37.9 10 266 1 827 1985-1987Salta Capital SA 24047' 65024' 23.2 52 9,523 1 8,051 1986-1988San Pedro JU 24014' 64052' 34.8 24 2,147 1 1,975 1982-1983Manuel Beigrano JU 24012' 65019' 28.6 33 6,277 2 24,870 1986-1993Yavi JU 22006' 65036' 36.6 4 482 1 2,205 1989-1993Bariloche RN 41058' 71031' 27.9 29 150 1 2,955 1987-1994Futaleufu CU 42055' 71020' 29.2 16 752 1 4,394 1985-1994Biedma CU 42046' 65003' 20.3 23 679 1 2,207 1990-1994
Abbreviations: BA, Buenos Aires; CA, Chaco; CO, C6rdoba; CU, Chubut; ER, Entre Rios; JU, Jujuy; Lat S, latitude south; Lon W, longitude west; MI, Misiones; MZ, Mendoza; RN, RioNegro; SA, Salta; SF Santa Fe; TU, Tucuman.'Deprivation index. 6Number of different industrial activities by county out of 80 analyzed activities. 'Annual births in the county according to the 1980 census. dNumber of participatingmaternity hospitals.
Table 2. Thirty-four types of congenital anomalieswith at least 20 cases observed.
index values, the 21 investigated countieswere classified as poorer (NBI of 2 22%) orricher (NBI < 22%). This threshold was themedian of the NBI distribution of the 21counties, with 10 counties above the medianand 11 below it.
To enhance the specificity of the associa-tion between industrial activity and congenitalanomalies, we based our working hypothesison two premises for a given association to beconsidered as relevant: a) a given industrialactivity must represent a statistically signifi-cant risk for a given congenital anomaly type;and b) there must be an increase in the birthprevalence rate of the congenital anomalytype involved in those counties where theputative causal activity was performed and adecrease in the counties where that activitywas not performed.
In a first step, the incidence rate ratios(IRR) for each congenital anomaly type wereestimated through the relationship betweenexposed and unexposed counties. This stepinvolved 2,720 IRRs and their confidenceintervals, corresponding to 80 different indus-trial activities and 34 congenital anomalies.The resulting risks were further adjusted bythe NBI index and grouped into two pre-viously defined strata applying the Mantel &Haenszel test (12) and the 99% confidencelimits through the method of Miettinen(13). Significance levels were subjected toBonferroni correction (14) because of thehigh number ofcomparisons involved.
In a second step, and for each significantmalformation/lindustrial activity associationidentified, we compared the proportion of
counties with the given activity and a higherthan expected prevalence of the given malfor-mation (true positives) with the proportionof counties without the given activity and alower than expected prevalence of the givenmalformation (true negatives). We derivedexpected birth prevalence values for eachcounty from the total sample of this studyand we used Fisher's exact test to determinethe significance ofthis comparison.
ResultsThe mean (± SD) NBI value for the 11poorer counties (with 225,444 examinedbirths) is 27.6 ± 4.5%, and its range is22.7-37.9. The mean NBI value of the 10richer counties (with 389,352 births) is 14.7+ 2.4% and its range is 6.4-20.3. Thesevalues are significantly different [X2 = 903.3;degrees of freedom (df) = 1; p < 0.00 1].
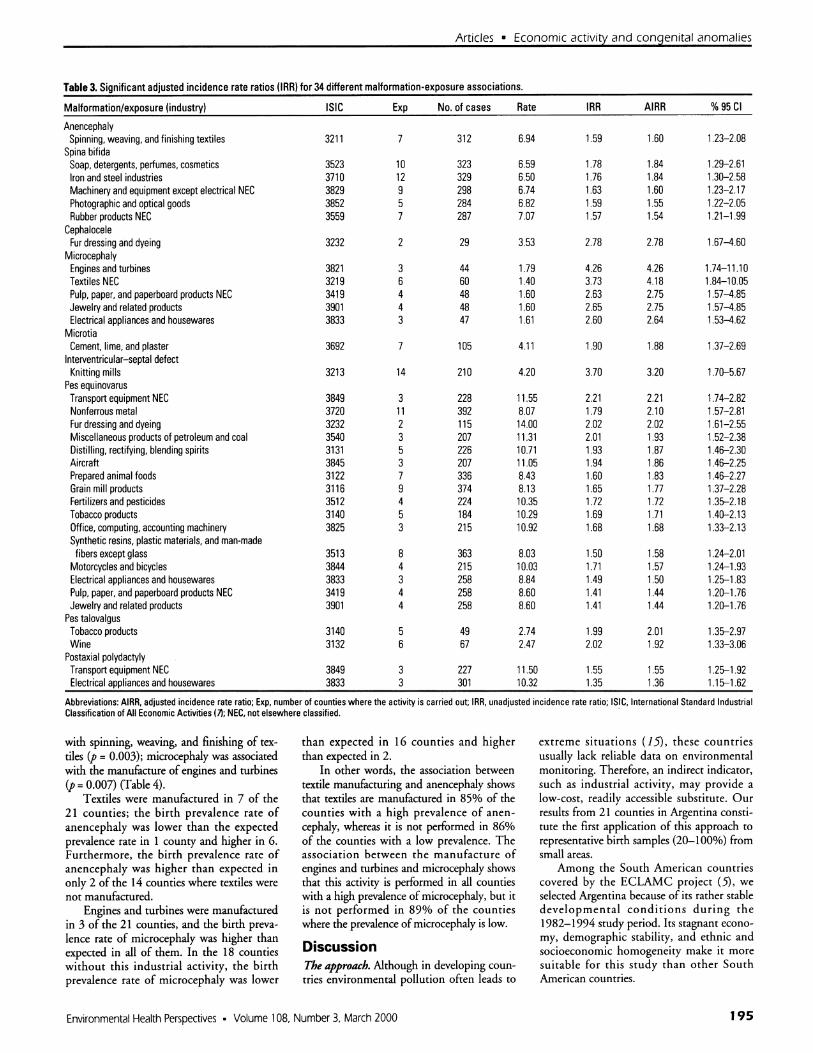
The first step of the analysis disclosedthat for 9 of the 34 congenital anomaliesthere is a significant risk from exposure toone or more specific industrial activities:anencephaly, spina bifida, cephalocele,microcephaly, microtia, interventricular sep-tal defect, pes equinovarus, pes talovalgus,and postaxial polydactyly (Table 3).
For these 9 congenital anomalies, weidentified seven significant associationsbetween exposure and an increase in the birthprevalence rate for the indicated anomaly bycounty (Fisher exact test, p < 0.05). Theseinvolved seven industrial activities and fourcongenital anomaly types. The Fisher exacttest was significant at p < 0.01 for two of theseven associations: anencephaly was associated
Volume 108, Number 3, March 2000 * Environmental Health Perspectives
11.~~~~~~~~~~2
194
Articles * Economic activity and congenital anomalies
Table 3. Significant adjusted incidence rate ratios (IRR) for 34 different malformation-exposure associations.
AnencephalySpinning, weaving, and finishing textiles
Spina bifidaSoap, detergents, perfumes, cosmeticsIron and steel industriesMachinery and equipment except electrical NECPhotographic and optical goodsRubber products NEC
CephaloceleFur dressing and dyeing
MicrocephalyEngines and turbinesTextiles NECPulp, paper, and paperboard products NECJewelry and related productsElectrical appliances and housewares
MicrotiaCement, lime, and plaster
Interventricular-septal defectKnitting mills
Pes equinovarusTransport equipment NECNonferrous metalFur dressing and dyeingMiscellaneous products of petroleum and coalDistilling, rectifying, blending spiritsAircraftPrepared animal foodsGrain mill productsFertilizers and pesticidesTobacco productsOffice, computing, accounting machinerySynthetic resins, plastic materials, and man-madefibers except glass
Motorcycles and bicyclesElectrical appliances and housewaresPulp, paper, and paperboard products NECJewelry and related products
Pes talovalgusTobacco productsWine
Postaxial polydactylyTransport equipment NECElectrical appliances and housewares
Abbreviations: AIRR, adjusted incidence rate ratio; Exp, number of counties where the activity is carried out; IRR,Classification of All Economic Activities 17); NEC, not elsewhere classified.
unadjusted incidence rate ratio; SIC, International Standard Industrial
with spinning, weaving, and finishing of tex-tiles (p = 0.003); microcephaly was associatedwith the manufacture of engines and turbines(p = 0.007) (Table 4).
Textiles were manufactured in 7 of the21 counties; the birth prevalence rate ofanencephaly was lower than the expectedprevalence rate in 1 county and higher in 6.Furthermore, the birth prevalence rate ofanencephaly was higher than expected inonly 2 of the 14 counties where textiles werenot manufactured.
Engines and turbines were manufacturedin 3 of the 21 counties, and the birth preva-lence rate of microcephaly was higher thanexpected in all of them. In the 18 countieswithout this industrial activity, the birthprevalence rate of microcephaly was lower
than expected in 16 counties and higherthan expected in 2.
In other words, the association betweentextile manufacturing and anencephaly showsthat textiles are manufactured in 85% of thecounties with a high prevalence of anen-cephaly, whereas it is not performed in 86%of the counties with a low prevalence. Theassociation between the manufacture ofengines and turbines and microcephaly showsthat this activity is performed in all countieswith a high prevalence of microcephaly, but itis not performed in 89% of the countieswhere the prevalence of microcephaly is low.
DiscussionThe approach. Although in developing coun-tries environmental pollution often leads to
extreme situations (15), these countriesusually lack reliable data on environmentalmonitoring. Therefore, an indirect indicator,such as industrial activity, may provide alow-cost, readily accessible substitute. Ourresults from 21 counties in Argentina consti-tute the first application of this approach torepresentative birth samples (20-100%) fromsmall areas.
Among the South American countriescovered by the ECLAMC project (5), weselected Argentina because of its rather stabledevelopmental conditions during the1982-1994 study period. Its stagnant econo-my, demographic stability, and ethnic andsocioeconomic homogeneity make it moresuitable for this study than other SouthAmerican countries.
Environmental Health Perspectives * Volume 108, Number 3, March 2000 195
Articles * Castilla et al.
Table 4. Industrial activities significantly associated with the birth prevalence rate of a given congenitalanomaly shown as the number of counties where a given industrial activity is or is not carried out.
Industrial activityFrequency of malformation/ Yes No Fisher exactexposure association ISIC Low High Low High testAnencephalySpinning,weaving, and finishing textiles 3211 1 6 12 2 0.003
MicrocephalyTextiles NEC 3219 2 4 14 1 0.011Pulp, paper, and paperboard products NEC 3419 1 3 15 2 0.027Engines and turbines 3821 0 3 16 2 0.007Jewelry and related products 3901 1 3 15 2 0.027
Pes equinovarusTransport equipment NEC 3849 0 3 14 4 0.026
Abbreviations: ISIC, International Standard Industrial Classification of all Economic Activities (18; NEC, not elsewhereclassified. High frequency indicates that the observed birth prevalence rate is higher than expected; low frequency indi-cates that the observed birth prevalence rate is lower than expected.
Because we assumed that the county of achild's birth is the same county where themother resided during pregnancy, a highresidential mobility could weaken the associ-ations between exposures and congenitalanomalies (16). For this reason, we did notinclude the large area of metropolitanBuenos Aires, with high residential mobility,in the present study.
Unlike acute or limited exposures, such asthose caused by accidents or certain types ofoccupations, respectively, chronic and wide-spread environmental exposures constituterisks for diseases, which may be of littleimportance at the individual level but areimportant for the population as a whole(17,18). Therefore, the cohort or case-controlapproaches, usually applied to the study ofoccupational exposures, are not readily appro-priate for environmental pollutants. An avail-able alternative is the cohort or case-controlstudy in small exposed and unexposed geo-graphic areas for which exposure rates areobtained from census data. Unfortunately,statutory statistics are highly unreliable for sci-entific purposes in the developing world.
The associations. Although the aim ofthis study was to suggest rather than to proveexposure-effect associations, the large num-ber of comparisons recommends that onlythe highly significant and relevant associa-tions should be considered. We found twospecific associations between industrial activ-ity and congenital anomalies that had statis-tically significant IRRs and an increasedbirth prevalence rate of the congenital anom-aly in the counties where the given industrialactivity was performed.
The textile industry was involved in oneof these highly significant associations-theassociation between textile manufacturingand anencephaly. Furthermore, we identifiedseven associations involving seven differentindustrial activities and four congenitalanomaly types. Two of the four anomalies
are related to the central nervous system(anencephaly and microcephaly), and both ofthem were associated with activities of the"textile, wearing apparel, and leather indus-tries," corresponding to code 32 at the two-digit level (8). The textile industry includesthree consecutive steps (preparing, dyeing, andfinishing) and uses diverse chemicals, includ-ing pesticides carried in the sheep's wool,formic and sulfuric acids, and organic solvents(19). In occupational exposure studies, organicsolvents have been reported to have adversereproductive effects in humans (20-24).
In a study on paternal occupation (vehiclemanufacturers) and birth defects, Schnitzer etal. (21) reported higher risks for central ner-vous system defects and deft lip; in the pre-sent study, the same type of industrial activitywas associated with microcephaly.
Profits and pitfalls. In spite of severalstrengths shown by the present approach,our results should be interpreted cautiously.Positive conditions include the following:* The study group is large enough (600,000births) to estimate valid expected andobserved birth prevalence rates for mostcongenital anomalies, and the sample isrepresentative (> 20%) of the total popula-tion of the small areas (counties) analyzed.
* The exposure indicator is objective, basedon an international coding system, makingthis approach suitable for other countries,and our observations are comparable withthose of other studies.
* Data were collected without knowledge ofthe working hypothesis, which was appliedto material stored in the ECLAMC projectdata bank.
* Diagnosis and description of specific mal-formations are ofgood quality, inasmuch asECLAMC is an ongoing clinical and epi-demiologic research project of birth defects.Nevertheless, the following limitations
should be considered when evaluating theproposed method and the present results:
* The employed approach suffers from theso-called "ecological fallacy" (25), whichresults by inferring individual risks frompopulational studies.
* Exposure data are of poor quality in thesense that the exposure indicator is unspe-cific as to the involved teratogen (one singleindustrial activity can release many differ-ent chemicals).
* The exposure indicator denotes the pres-ence of a given industry, which probablypollutes the environment of a small area,but at the same time increases the proba-bility of specific maternal occupationalexposures. Therefore, environmental andoccupational exposures cannot be disen-tangled by this approach.
* When analyzing the exposure risk for agiven activity, the remaining 79 activitiesthat make up the nonexposed groupdecrease the sensitivity of the test to detectteratogenic activities. However, this is acommon drawback for most studies onenvironmental exposures.
* Most congenital anomalies are of a complexnature as to their multifactorial causation;the effect of a given teratogen depends onthe embryologic stage of exposure, thethreshold dose to produce the defect, andmany other concurring variables.
* Our study adjusted the estimated risks bymeans of a socioeconomic index based onthe census. This, however, does not controlfor all lifestyle-related confounders, such asthe use of alcohol and smoking of cigarettes.
ConclusionsThe aim of this study was to determineassociations between potentially teratogenicindustrial pollutants and congenital anom-alies. In spite of the technical limitations ofour approach, we identified significant asso-ciations between the textile industry andanencephaly, and between the manufactureof engines and turbines and microcephaly.
Although the two observations are con-sistent with previous reports on occupationalexposure, further investigations, such ascase-control studies in small areas, would beworthwhile. There is no clear pattern of riskfor environmental teratogens in general, noteven through studying hazardous-wastelandfill sites (9,26).
REFERENCES AND NOTES1. Hemminki K, Saloniemi I, Luoma K, Salonen T, Partunen
T, Vainio K. Transplacental carcinogens and mutagens:childhood cancer, malformations and abortions as riskindicators. J Toxicol Environ Health 6:1115-1125 (1980).
4. Beatie AD, Moore MR, Goldberg A. Role of chronic lowlevel lead exposure in the aetiology of mental retarda-tion. Lancet 1:589-592 (1975).
196 Volume 108, Number 3, March 2000 * Environmental Health Perspectives
Articles * Economic activity and congenital anomalies
5. Castilla EE, Lopez-Camelo JS. The surveillance of birthdefects in South-America: I. The search for time clus-ters: epidemics. Adv Mutagen Res 2:191-210 (1990).
6. ECLAMC. ECLAMC Manual Operacional. Rio deJaneiro:ECLAMC (Latin-American Collaborative Study ofCongenital Malformations), 1982
7. INDEC. Censo Nacional Econ6mico 1985. IndustriaManufacturera. Resultados definitivos. Total del pais yjurisdicciones. Buenos Aires:Republica ArgentinaPresidencia de la Naci6n. Instituto Nacional deEstadistica y Censos, 1989.
8. ISIC. International Standard Industrial Classification ofAll Economic Activities. Statistical Papers, Series M No.4, Revision 2. New York:United Nations, 1968.
9. Dolk H, Vrijheid M, Armstrong B, Abramsky L, Bianchi F,Garne E, Nelen V, Robert E, Scott JE, Stone D, Tenconi R.Risk of congenital anomalies near hazardous-wastelandfill sites in Europe: the EUROHAZCON study. Lancet352:423-427 (1998).
10. Carstairs V. Deprivation indices: their interpretation anduse in relation to health. J Epidemiol Community Health49(suppl 2):S3-S8 (1995).
11. CEPA. Comite Ejecutivo para el estudio de la Pobreza enla Argentina. Doc # 4, INDEC. Buenos Aires:Ministerio deEconomia de la Naci6n Argentina, 1994.
12. Mantel N, Haenszel W. Statistical aspects of the analysisof data from retrospective studies of disease. J NatICancer Inst 32:719-748 (1959).
14. Armitage P, Berry 6, eds. Multiple Measurements. In:Statistical Methods in Medical Research, 3rd ed.London:Blackwell Scientific Publications, 1994;312-385.
15. Monteleone-Neto R, Castilla EE. Apparently normal fre-quency of congenital anomalies in the highly pollutedtown of Cubatao, Brazil. Am J Med Genet 52:319-323(1994).
16. Khoury MJ, Stewart W, Weinstein A, Panny S, Lindsay P,Eisenberg M. Residential mobility during pregnancy:implications for environmental teratogenesis. J ClinEpidemiol 41:15-20 (1988).
17. Ericson A, Eriksson M, Kaiien B, Zetterstrom R. Maternaloccupation and delivery outcome: a study using centralregistry data. Acta Pediatr Scand 76:512-518 (1987).
18. Kallen B, Landgren MS. Delivery outcome in pregnancieswhen either parent worked in the chemical industry. Astudy with central registries. J Occup Med 36:563-568(1994).
19. International Agency for Research on Cancer. SomeFlame Retardants and Textile Chemicals, and Exposures
in the Textile Manufacturing Industry. IARC Monogr EvalCarcinog Risk Chem Hum 48: (1990).
20. Brender JD, Suarez L. Paternal occupation and anen-cephaly. Am J Epidemiol 131:517-521 (1990).
21. Schnitzer PG, Olshan AF, Erickson JD. Paternal occupa-tion and risk of birth defects in offspring. Epidemiology6:577-583 (1995).
22. Marshall EG, Gensburg W, Deres DA, Geary NS, CayoMR. Maternal residential exposure to hazardous wastesand risk of central nervous system and musculoskeletalbirth defects. Arch Environ Health 52:416-425 (1997).
23. Correa A, Gray RH, Cohen R, Rothman N, Shah F, SeacatH, Corn M. Ethylene glycol ethers and risks of sponta-neous abortion and subfertility. Am J Epidemiol143:707-717 (1996).
24. Lindbohm ML, Hemminki K, Bonhomme MG, Antilla A,Rantala K, Heikkila P, Rosenberg MJ. Effects of paternaloccupational exposure on spontaneous abortions. Am JPublic Health 81:1029-1033 (1991).
25. Morgenstern H. Uses of ecological analysis in epidemio-logic research. Am J Public Health 72:1336-1344 (1982).
26. Croen LA, Shaw GM, Sanbonmatsu L, Selvin S, BufflerPA. Maternal residential proximity to hazardous wastesites and risk for selected congenital malformations.Epidemiology 8:347-354 (19971.
-~~~~~~A
Not if you subscribe toEnvironmental HealthPerspectives. With eachmonthly issue, Environmental HealthPerspectives gives you comprehensive,cutting-edge environmental health andmedicine research and news.
When it comes to outfitting your labwith the best research tools,Environmental Health Perspectives isthe state of the art.
Call 1-800-315-3010 today tosubscribe and visit us online.
What you know is more
important than what you have.
http:Ilehis.niehs.nih.gov/
Environmental Health Perspectives * Volume 108, Number 3, March 2000 197