88
Effective and Cost-Effective Treatment for Diabetes Edwin Gale Edwin Gale University of Bristol, UK
| Date post: | 11-Nov-2014 |
| Category: |
Health & Medicine |
| Upload: | emad-hamed |
| View: | 1,678 times |
| Download: | 6 times |

Effective and Cost-Effective Treatment for Diabetes
Edwin Gale
Edwin Gale
University of Bristol, UK

I have no financial conflicts of interest

The scope of the problem What are we trying to achieve? Choosing the right treatment
Effective and Cost-Effective Treatment

Most of the medical textbooks are based upon experience gained in Western populations. The culture, phenotype and genotype of diabetes differs between major population groups Egyptian people should rewrite the textbooks for use in Egypt!

High employment, increasing disposable income, cheap food and energy (and
everything that goes with these things) are changing the phenotype of the
human species
A Century of Economic Growth
The changing phenotype of the human species (affluent variety) Diabetologia 2004;47:1339-1342
Increasing height: 1 cm/decade Changing body proportions Increasing weight-to-height ratio Increasing longevity: 3-4 months for
every calendar year
Health Correlates of Economic Growth: A Changing Human Phenotype

Estimated Numbers with Diabetes (in millions) in 2000 and 2030
Western Countries Growing economies


Diabetes Prevalence as % Population in Denmark
Courtesy of Bendix Carstensen

Diabetes Prevalence as % Population in Denmark
Courtesy of Bendix Carstensen

Cancer
Lipids
Glucose Atheroma
BP
The Affluent Phenotype

Excess calorie intake is a major driver of the affluent phenotype …
Edwin Gale … and reduced calorie intake reverses
most of its features

Incidence of diabetes in Oslo, 1925-54
Westlund 1966

Diabetes Mortality in the UK, 1938-58
Deaths/
100k
Trowell, 1962
World War II

Edwin Gale
Calorie restriction is the only form of therapy that strikes at the root cause of diabetes
Pharmacotherapy largely represents the attempt to compensate for a failure of
calorie restriction

Affluent humans are developing a new and distinctive phenotype
Diseases of relative overnutrition have
emerged as the leading causes of death Increasing longevity is a major factor in
the diabetes epidemic
Summary: The Human Phenotype

The scope of the problem What are we trying to achieve? Choosing the right treatment
Effective and Cost-Effective Treatment
1. Near-normal glucose control? 2. Near-normal life expectancy? 3. Near-normal life quality?
What are we trying to achieve?

Offers strong protection against microvascular complications
- but the benefit diminishes with increasing age
But weak protection against cardiovascular outcomes
Has not been shown to improve life expectancy in type 2 diabetes
Intensified glucose control can reduce quality of life
Near-normal glucose control

Lifetime Risk of Blindness by Age at Diagnosis and HbA1c
Age at diagnosis
n/10
00
Ann Int Med 1997;127:788

Lifetime Risk of ESRF by Age at Diagnosis and HbA1c
Age at diagnosis
n/10
00
Ann Int Med 1997;127:788

Microvascular Disease
Risk diminishes with age and/or limited life expectancy.
The full benefits seen in young patients with type 1 diabetes are not achieved in older people with type 2 diabetes
Offers strong protection against microvascular complications
But weak protection against cardiovascular outcomes
Has not been shown to improve life expectancy in type 2 diabetes
Intensified glucose control can reduce quality of life
Near-normal glucose control

HRs for CV outcomes, DM vs non-diabetes
Emerging Risk Factors Collaboration (EFRC), Lancet 2010;375:2215-22

Emerging Risk Factors Collaboration (EFRC), NEJM 2011;364:829-41

Emerging Risk Factors Collaboration (EFRC), NEJM 2011;364:829-41
A 50-year-old man with diabetes loses 6 years of life expectancy
60% of the excess mortality is due to vascular deaths

Numbers Needed to Treat [To prevent 1 CVD event]
Glucose (HbA1c 0.9%) : 119
Cholesterol trials (1mM) 44
Blood Pressure trials (10/6mmHg) 34
Yudkin et al, Diabetologia 2010

Offers strong protection against microvascular complications
But weak protection against cardiovascular outcomes
Has not been shown to improve life expectancy in type 2 diabetes
Intensified glucose control can reduce quality of life
Near-normal glucose control

Boussageon R et al. BMJ 2011
All cause mortality
OR: 1.04 (0.91 – 1.19)
Cardiovascular death
OR: 1.11 (0.96 – 1.43)
Mortality – intensive versus standard Meta-Analysis: 13 studies, 34533 patients

Relationship Between Glycated Haemoglobin and Mortality in 47,970 Patients
UK General Practice Research Database, Currie et al, Lancet 2010
Oral therapy Insulin

Offers strong protection against microvascular complications
But weak protection against cardiovascular outcomes
Has not been shown to improve life expectancy in type 2 diabetes
Intensified glucose control can reduce quality of life
Near-normal glucose control

Patient perceptions of intensive glucose lowering
701 pts with T2DM asked re QOL utilities; a score of 1.0 = perfect health, 0 = death
Intensive glucose control scored 0.67, or 1/3 of a year‟s quality of life
Huang et al, Diabetes Care (2007) 30:2478

Intensified glucose lowering therapy ALONE offers limited benefits in type 2 diabetes
BUT Combined attention to all cardiovascular risk
factors can make a dramatic difference to outcomes
Check Point

160
80 80
67 63
55 38
Trial Ends
Study Ends
Mean 7.8 yr
Mean 5.5 yr
Died 24 (9 CVD) 40 (19 CVD)
Randomized
Conventional (2 dropped out)
Intensified (1 dropped out)
STENO-2 NEJM 2008;358:580

The scope of the problem What are we trying to achieve? Choosing the right treatment
Effective and Cost-Effective Treatment

When?
How? Who? Why?

When?
Why?
Life Quality
CV Risk
Other risks
Longevity

When?
Why?
Life Quality
CV Risk
Other risks
Longevity
Does intensified therapy benefit?
Hemmingsen B et al: Cochrane Database Syst Rev. 2011 Jun 15;6:CD008143 Yudkin et al, Diabetologia 2010;53:2079-85

When?
Why?
Life Quality
CV Risk
Other risks
Longevity
Does intensified therapy benefit?
No
Hemmingsen B et al: Cochrane Database Syst Rev. 2011 Jun 15;6:CD008143 Yudkin et al, Diabetologia 2010;53:2079-85

When?
Why?
Life Quality
CV Risk
Other risks
Longevity
Does intensified therapy benefit?
No
Marginal
Hemmingsen B et al: Cochrane Database Syst Rev. 2011 Jun 15;6:CD008143 Yudkin et al, Diabetologia 2010;53:2079-85

When?
Why?
Life Quality
CV Risk
Other risks
Longevity
Does intensified therapy benefit?
No
Marginal
Minor
Hemmingsen B et al: Cochrane Database Syst Rev. 2011 Jun 15;6:CD008143 Yudkin et al, Diabetologia 2010;53:2079-85

When?
Why?
Life Quality
CV Risk
Other risks
Longevity
Does intensified therapy benefit?
No
No
Marginal
Minor
Hemmingsen B et al: Cochrane Database Syst Rev. 2011 Jun 15;6:CD008143 Yudkin et al, Diabetologia 2010;53:2079-85

When?
Why?
Life Quality
CV Risk
Other risks
Longevity
Does intensified therapy benefit?
No
No
Marginal
Minor
Hemmingsen B et al: Cochrane Database Syst Rev. 2011 Jun 15;6:CD008143 Yudkin et al, Diabetologia 2010;53:2079-85
But early intervention is beneficial!

VADT - HR for Primary Outcome in Intensive Arm
0
0.2
0.4
0.6
0.8
1
1.2
1.4
0 3 6 9 12 15 18 21 24
Duration of Diabetes (yrs)
Ha
zard
Ra
tio

When?
Why? How?

Comorbidity and Glucose Control, New onset patients aged 60-64 yrs
Comorb. Life Exp Days added
Case 1 0 14.6 yrs +106
Case 2 3 9.7 yrs + 44
Case 3 7 4.8 yrs + 8
Huang et al, Ann Int Med (2008) 149:11-19

When?
Who? Why?
Life Quality
CV Risk
Other risks
Longevity
Life Quality
CV Risk
Other risks
Longevity

When?
Who? Why?
Life Quality
CV Risk
Other risks
Longevity
Life Quality
CV Risk
Other risks
Longevity
Prognosis, patient choice

When?
Who? Why?
Life Quality
CV Risk
Other risks
Longevity
Life Quality
CV Risk
Other risks
Longevity
Prognosis, patient choice
Established vascular disease?

When?
How? Who? Why?

When?
How? Who? Why?
Life Quality
CV Risk
Other risks
Longevity
Life Quality
CV Risk
Other risks
Longevity
Life Quality
CV Risk
Other risks
Longevity

When?
How? Who? Why?
Life Quality
CV Risk
Other risks
Longevity
Diabetes therapies previously considered solely in terms of HbA1c reduction ...

• Treatment A lowers HbA1c from 10.5% to 9% • Treatment B lowers HbA1c from 7.6% to 7% • Which treatment is more potent?
Spot Quiz

HbA1c: Baseline vs. change
Diabetes Care 2006;29:2137

When?
How? Who? Why?
Life Quality
CV Risk
Other risks
Longevity
Diabetes therapies previously considered solely in terms of HbA1c reduction ... But global profile now seen as more important

Most patients have been exposed to multiple
treatments RCT evidence does not (with some exceptions)
allow us to assess the global impact of specific therapies upon cardiovascular risk
Check Point

Glucose-lowering Agents
Core therapies: Biguanides Sulfonylureas Human Insulin Newer therapies: Thiazolidinediones DPP-4 inhibitors GLP-1 agonists Other: Acarbose Meglitinides SGLT-2 inhibitors

ADA / EASD Guidelines
Revised Treatment Algorithm
Intensive insulin
At diagnosis:
Lifestyle + metformin STEP 1
STEP 2
Tier 1* Tier 2†
STEP 3
Add basal insulin
Add sulfonylurea
Add GLP-1 agonist
Add pioglitazone ± SU
HbA1C >7.0%
Nathan et al. Diabetes Care 2008

Core Therapies
Lifestyle
Metformin
SUs
Human insulin

Lifestyle …
Is the starting point for any treatment No treatment for diabetes can work effectively without adjustment of lifestyle Diabetes conferences are 90% about pharmacology and 10% about human behaviour Real world therapy is the other way round

METFOR MIN
Reduces CV disease!
Fights cancer!
?

Myocardial Infarction Hazard Ratio (fatal or non-fatal myocardial infarction or sudden death)
Intensive (metformin) vs. Conventional glucose control
HR (95%CI)
UKPDS 80

Metformin in Patients with Established Atherosclerosis
Method:
Comparison of 2 year mortality in 19,691 patients with diabetes and known vascular disease, treated with or without metformin, in the REACH registry.
Roussel et al, Arch Int Med 2010;170:1892-99

Metformin in Patients with Established Atherosclerosis
+Metformin -Metformin
% Mortality 6.3 (5.2-7.4) 9.8 (8.4-11.2%)
Hazard Ratio 0.76 (0.65-0.89)
Roussel et al, Arch Int Med 2010;170:1892-99
(adjusted)

Benefits of Metformin (Hazard Ratios)
Age 65-80 0.77 (0.62-0.95)
Heart failure 0.69 (0.54-0.90)
GFR 30-60 0.64 (0.48-0.86)
MF + INS 0.64 (0.46-0.89)
Roussel et al, Arch Int Med 2010;170:1892-99

Metformin: Summary
Mechanism of cardiovascular protection unclear – related to mechanism of
cancer protection?
Observational studies to date show consistent reductions in overall and
cardiovascular mortality

Sulfonylureas
Gloyn et al, New Engl J Med 2004;350:1838-1849

Closure of the K+ channel leads to membrane depolarization

KATP channels
Transducers between intracellular energy metabolism and electrical excitability Found in many tissues including heart and brain Mostly closed in tissues outside the beta cell; open in response to ischaemia, hormones or neurotransmitters In cardiac muscle and neurones the reduction in electrical activity protects against damage
Frances Ashcroft, J Clin Invest 2005;115;2047-58

Variant forms of the channel
Kir 6.2 SUR1 beta cells Kir 6.2 SUR2A cardiomyocytes Kir 6.2 SUR2B arterial smooth muscle
All sulfonylureas show some cross-reactivity

Potential cardiovascular consequences of failure to open KATP channels
The default setting for cardiovascular KATP channels is closure. Opening results in -
• Limitation of myocardial damage during ischaemia
• Loss of preconditioning
• Masking of ST segment elevation
• Loss of smooth muscle relaxation in coronary arteries Bell, CMAJ 2006;174:185-6

Myocardial Infarction Hazard Ratio (fatal or non-fatal myocardial infarction or sudden death)
Intensive (SU/Ins) vs. Conventional glucose control
HR (95%CI)
UKPDS 80

Sulfonylureas: Summary
No clear evidence that theoretical risk translates into actual risk
No clear evidence that prognosis worse
after myocardial infarction
Best avoided in interventional cardiology
Gliclazide probably safer than glibenclamide

Benefits overstated
Unsupported claims
“Newer” may not mean „better”
Evidence base not yet established
Long term safety unknown
Much more expensive!
Disadvantages of Newer Therapies


A Situation of Diminishing Returns
1920 2010 1960
Insulin
SUs
Metformin TZDs
DPP4s Analogs

And Escalating Costs
Euros/yr
UK Formulary, 2006
1000
500
1500
Metformin Gliclazide
Rosiglitazone
Pork
Analog + Lantus
Pioglitazone
Human
Sitagliptin
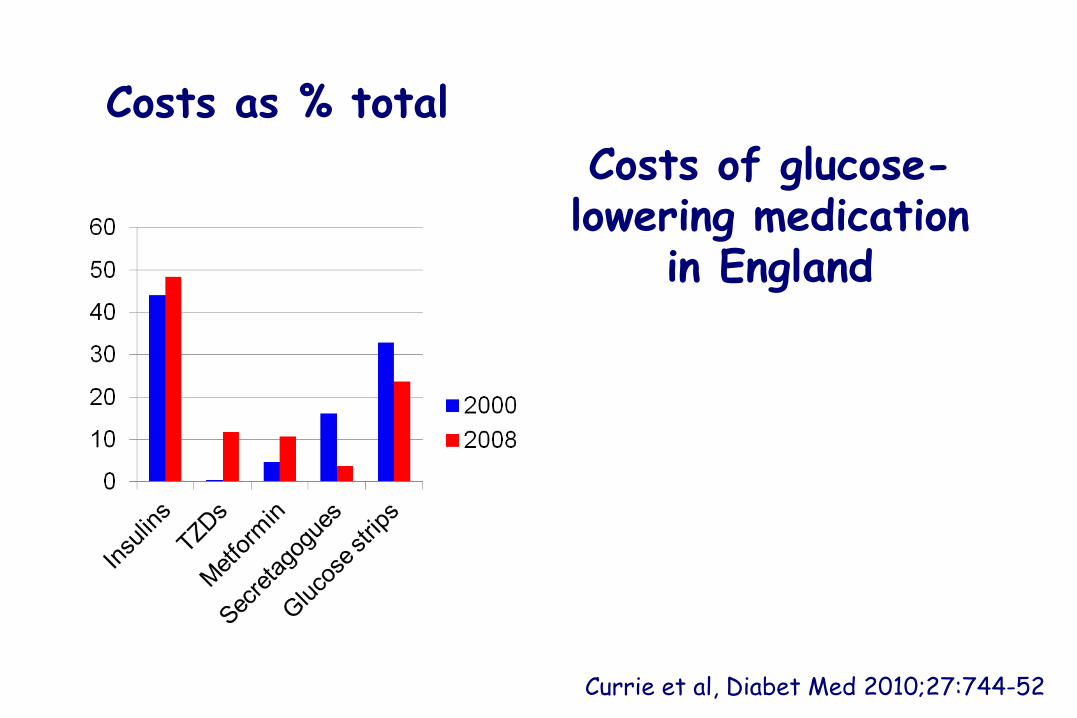
Costs as % total
Currie et al, Diabet Med 2010;27:744-52
Costs of glucose-lowering medication
in England

Costs as % total Total Costs (£m) Adjusted to 2008
Currie et al, Diabet Med 2010;27:744-52

Costs as % total Total Costs (£m) Adjusted to 2008
Currie et al, Diabet Med 2010;27:744-52
Costs (in England)
2000 = £289.9 million 2008 = £590.4 million

Prescriptions by Cost and Volume (2008)
Currie et al, Diabet Med 2010;27:744-52

Insulin costs (£) per 1000 units
BNF (accessed Oct 2011)

Insulin costs (£) per 1000 units
Currie et al, BMJ in press
Cumulative excess cost of analogues to
the NHS is ~£650 million


Overall Summary
Metformin emerges as “best buy”
The disadvantages of the sulfonylureas have been over-stated
Analogue insulins have marginal benefits only
in type 2 diabetes
Newer therapies should be reserved for second line use

Where Next?
Future clinical trials will need to evaluate global risks and benefits of individual
therapies (and combinations) rather than focusing on glucose-lowering efficacy

The Physician’s Prayer
From inability to let well alone, From too much zeal for the new and contempt for what is old, From putting knowledge before wisdom, Science before art and cleverness before common sense, From treating patients as cases And from making the cure of the disease more grievous than the endurance of the same, Good Lord deliver us.
Sir Robert Hutchison (1871-1960)

Thank you for listening

















