28
EFFECT OF ANESTHETIC AGENTS ON UTERINE ACTIVITY DR AFTAB HUSSAIN
| Date post: | 18-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | aftab-hussain |
| View: | 33 times |
| Download: | 7 times |

EFFECT OF ANESTHETIC AGENTS ON UTERINE ACTIVITY
DR AFTAB HUSSAIN
ANATOMY
Uterus is part of female reproductive organ which also includes ovary and fallopian tubes.
Uterus is fibro-muscular organ which varies in size, shape and weight depending on age, parturition and estrogenic stimulation.
Upper part is muscular and lower part is fibrous in nature.
Musculature of uterus is in 3 layer
Outer - longitudinal muscle layer
Middle – vascular layer
Inner – muscle layer in both longitudinal and oblique fashion
PHYSIOLOGY
Uterus receives fertilized egg and protects and provide nutrition to fetus during development.
At end of pregnancy uterus contract facilitating child birth.
Endometrium of uterus sheds periodically as menses.
UTERINE PHYSIOLOGY
Uterus is a smooth muscle organ that carry out their physiological role through tonic or phasic contraction.
Duration and frequency of action potential determines pattern of contraction.
Contractility of muscle group is influenced by changes in electrical activity. This is in turn influenced by hormonal changes and stimulants (oxytocin, prostaglandins, catchecholamines).
ELECTRICAL ACTIVITY AND CONTRACTION
Uterine contractility is direct consequence of the underlying electrical activity in the myometrial cells.
Spontaneous electrical activities are composed of intermittent burst of spike action potentials.
Uterine volume (chronic stretch) and ovarian hormones (estrogen) contribute to change in action potential spikes.
ELECTRICAL ACTIVITY AND CONTRACTION (cont.)
The action potential in uterine smooth muscle result from voltage and time dependent changes in membrane ionic permeability.
In both longitudinal and circular muscle of uterus the depolarizing phase of spike is due to inward current carried by Ca2+ ion and Na+ ions.
Each burst of activity stops before uterus completely relax.
Agents that stimulate or inhibit electrical activity do so by altering electrical property and excitability of myometrial cells.

UTERINE ACTIVITY (definitions)
Frequency: beginning of one contraction to beginning of next (minutes)
Duration: beginning to end of one contraction (seconds) Must be at least 40 seconds to quantify as a contraction.
Intensity: strength (mild, moderate, strong) with external monitor, determined by palpation
Resting Tone: relaxed or not relaxed (determined by palpation with external monitor)

UTERINE ACTIVITY
Normal uterine activity: < 5 contractions in 10 minutes averaged over 30 minutes
Tachysystole: > 5 contractions in 10 minutes averaged over 30 minutes.
Tachysystole with uterine hypertonia: incomplete relaxation between frequently occurring contractions
Tetanic contraction: Sustained uterine activity with incomplete relaxation. Absent O2 exchange at intervillous space.

Cause of Uterine irritability
Uterine irritability may be caused from
Dehydration
Infection
Abruption
Precursor to labor contractions.
Effect of drugs uterotonics, anesthetics (regional or systemic).
CARDIOTOCOGRAPHY
Method to assess uterine activity and fetal well being.
Cardio- FHR, Toco- Uterine, Graphy- recording
Methods:
FHR- External by Auscultation of FHR
Internal by fetal scalp electrodes
Uterine contraction monitoring
External by pressure sens. Tocodynamometer.
Internal by Intra uterine pressure catheter.

CTG of uterine activity
CALCULATING NORMAL UTERINE ACTIVITY WITH IUPC
Internal uterine pressure catheter (IUPC)
Montevideo Units: Calculated by subtracting resting tone from peak uterine activity for each contraction in 10 minutes. (Caldeyro-Barcia)
Labor found to begin clinically when MVU’s rose to 80-120 with contraction strength of > 40 mm Hg. This equates to 2-3 contractions every 10 min.
1. First stage: MVU’s- 100-250, frequency of 3-5 every 10 min
2. Second stage: MVU’s 300-400; ctx frequency of 5-6 every 10 min.
Effect of anesthetics on uterine activity

INHALATIONAL AGENTS
Sevoflurane, desflurane, isoflurane and halothane depress uterine activity
Dose dependent uterine relaxation.
They act on GABA1 receptors, and voltage sensitive Ca2+ and Na+ channels
Dose more than 0.75 MAC result in uterine atony and increase in blood loss.
N2O has minimal effect.
PARENTERAL AGENTS
Opioids ---- cause minimal decrease in progression of labor.
However,--- significant decrease in uterine contractility has been seen--- with increased conc. of opioids.1
Propofol---- has shown to decrease myometrial contractility in vitro studies.2
1 In vitro effect of opioids on uterine muscle. Nurten Kayakan et al. Adv. In Therapy 2007
2Effects of propofol on gravid human uterine muscle Tat-Leang Lee, P. Ganesan Adaikan, Lang Chu Lau, Ashok Kumar, Shan S. Ratnam. Journal of anesthesia 1997

REGIONAL ANESTHESIA
Epidural analgesia:
Dilute concentration (bupivacaine- 0.125% or less) do not prolong labor.
However, when conc. greater than 0.25% of bupivacaine--- may prolong labor by 15-30 min.
By -decreasing the urge to bear down (Ferguson reflex).
Therefore, use of dilute local anesthetic and opioid preserve motor function-- thus allowing bear down.
Normal saline IV fluids
In a study conducted by Cheek et al. using normal saline infusion during normal labor in women receiving extradural block, decreased uterine activity in groups receiving 1000ml of NS. (P<0.01).3
It returned to baseline over next 20 minutes.
3Normal saline iv fluid load decreases uterine activity in active labour. TG Cheek, P Samuels, F Miller… - BJA, 1996

Explanation for decreased uterine activity observed
after a fluid load
Oxytocin and vasopressin secretion are inhibited directly at the neurohypophysis.
Transient dilution of plasma oxytocin concentration by a fluid load.
However, both these suggestion are in dispute.
Role of ANP is also being suggested.

VASOPRESSORS
Uterine muscles have both alpha and beta receptors.
Alpha1 receptors--- cause uterine contraction.
Beta2 receptors--- cause uterine relaxation.
Large dose of phenylephrine-- can cause tetanic uterine contraction. It also cause uterine arterial constriction.
Ephedrine-- has little effect on uterine contraction.
NITROGLYCRINE
NO is a powerful vasodilator synthesized by amino acid oxidation catalysed by NO synthase.
It is present in myometrial cells and increases cGMP.
NO production leads to uterine relaxation.
Thereby-- administration of Nitroglycrine is associated with uterine relaxation.4
4 H.N. simhans, S.N. Caritis:Prevention of preterm delivery. The new england journal of medicine 2010
OXYTOCIN
It is used to induce labor or augment uterine contraction or to maintain uterine tone postpartum.
Activates G protein coupled receptors that trigger increase in intracellular calcium level in uterine myofibrils, which results in uterine contraction.
Also increases local PG production which further stimulate uterine contraction.
Used in IV dosage of 0.5 – 8mUI/min to induce labor.
OXYTOCIN ( contd.)
Hyperstimulation may cause fetal distress by increasing tone of uterus leading to uterine tetany.
Volatile anesthetic dose should be reduced in obstetric patients undergoing C/S to avoid its relaxation properties.
Other side effects– Rapid infusion can cause hypotension and reflex tachycardia.
ERGOT ALKALOIDS
Methergine
It cause intense and prolonged uterine contraction.
Used postpartum to treat uterine atony.
Administered-- IM dose of 0.2 mg.
Uterine contractions are usually initiated within 2-5 minute following IM and --1 min. following IV administration.
Cause intense vasoconstriction , thus may lead to severe hypertension.

PROSTAGLANDINS
Carboprost
It is a synthetic analogue of prostaglandin F2 .
Stimulate uterine contraction.
Acts by stimulating Prostaglandin F2a receptor, a G protein coupled receptor.
Oxytocin potentiates its action.
Used to treat postpartum uterine hemorrhage.
Dose – 0.25mg IM may be repeated to max 2mg.
Misoprost
Prostaglandin E1 analogue, it also stimulates uterine contraction minus side effect of bronchoconstriction.
MAGNESIUM
Inhibit premature uterine contraction. (Tocolytic action)
Act as Ca2+ antagonist, it decreases calcium intracellularly and inhibits contraction process.
Dose – Loading 4 gm IV over 20 min followed by 2gm/hr infusion.
Other side effects- Hypotension, heart block, muscle weakness, sedation.
Mg intensifies NM-blockade by Non dep. muscle relaxants.
Beta2 agonists
Ritodrine and Terbutaline
Inhibit uterine contraction by stimulating beta2 receptors.
Selective beta2 agonist.
Impair intracellular cyclic AMP conc. --- facilitate myometrial relaxation.
They are used to treat premature labor.
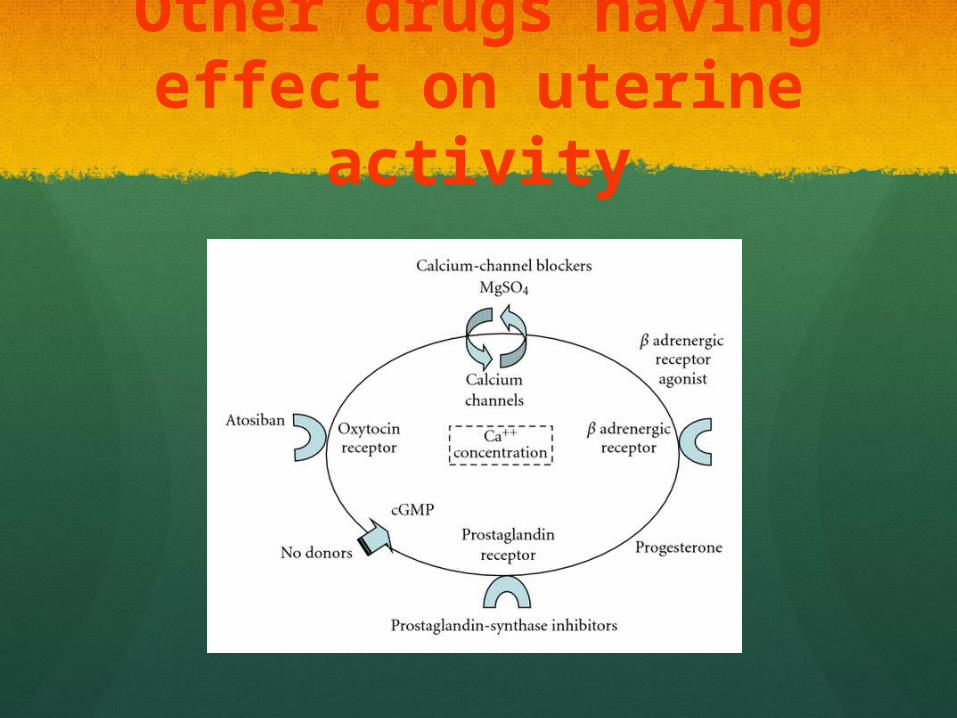
Other drugs having effect on uterine activity
Thank You

















