Effect of mood states and infertilitystress on patients' attitudes towardembryo transfer andmultiple pregnancy
Christopher Newton, Ph.D.,a,b Valter Feyles, M.D.,a,b and Veronica Asgary-Eden, Ph.D.a
a Fertility Clinic, London Health Sciences Centre; and b Department of Obstetrics and Gynaecology, University of WesternOntario, London, Ontario, Canada
Objective: To examine whether mood state or infertility stress influences perceptions of risk, preferences for embryo transfer, or viewson multiple pregnancy.Design: Observational cohort study.Setting: Hospital-based fertility clinic.Patient(s): One hundred seventy-six women participating in IVF treatment.Intervention(s): None.Main Outcome Measure(s): Mood scores, ratings of risk, preference for multiple embryo transfer, and attitudes toward multiplepregnancy.Result(s): Growing feelings of tension across the cycle corresponded with increases in the perceived riskiness of double-embryotransfer, but there was no change in strength of transfer preferences. Women experiencing negative moods, such as depression,viewed twin and triplet pregnancy as less likely, whereas increasing positive feelings across the cycle were associated withincreasing desire for twin pregnancy. Overall, women perceived double- and triple-embryo transfer as less risky by cycle end thanat cycle beginning and felt more certain about multiple-embryo transfer.Conclusion(s): The dyssynchrony observed among changes in mood, perceptions of risk, and transfer preferences challengesassumptions about the way medical risk information influences transfer preferences, and the findings suggest that mood states
Use your smartphone
experienced during an IVF cycle might affect transfer preferences by influencing attitudestoward multiple pregnancy. Additional considerations beyond providing risk information areneeded to facilitate effective patient decision making. (Fertil Steril� 2013;100:530–7. �2013by American Society for Reproductive Medicine.)Key Words: Embryo transfer, mood, stress, decision making
Discuss: You can discuss this article with its authors and with other ASRM members at http://fertstertforum.com/newtonc-mood-infertility-stress-embryo-transfer/
to scan this QR codeand connect to thediscussion forum forthis article now.*
* Download a free QR code scanner by searching for “QRscanner” in your smartphone’s app store or app marketplace.
oncern about the rate of multi- and efficacy of eSET (1), the practice <35 years old in the United States (3)
C ple births associated with theuse of assisted reproductive
technologies has resulted in growinginterest in elective single-embryotransfer (eSET). Despite the benefits
Received January 15, 2013; revised April 16, 2013; ac2013.
C.N. has nothing to disclose. V.F. has nothing to discSupported by a grant (R1630A03) from the Canadian
Canada).Preliminary results presented at the 23rd Annual Me
duction and Embryology, Lyon, France, July 200Reprint requests: Christopher Newton, Ph.D., Fertilit
remains less common in NorthAmerica than in certain Europeancountries. Reports from 2010 suggestthat 6% of all IVF cycles in Canada(2) and �19% of cycles among women
cepted April 18, 2013; published online May 15,
lose. V.A.-E. has nothing to disclose.Institutes of Health Research (Ottawa, Ontario,
eting of the European Society of Human Repro-7.y Clinic, London Health Sciences Centre, London,[email protected]).
015-0282/$36.00behalf of the American Society for Reproductive
involved eSET.Many infertility patients see twin
pregnancy as a desirable outcome (4,5), and few view a twin pregnancy ashaving significant risks (6). Theprovision of relevant risk informationhas been reported to decrease thedesirability of twin pregnancy amongwomen experiencing fertility problems(7) and to decrease the theoreticalpreference for multiple-embryo trans-fer among IVF patients (8, 9).However, in a contrasting finding, theprovision of risk information by itselfdid not increase theoretical acceptance
of eSET (10). Transfer decisions seem to be influenced notonly by an understanding of medical risks associated withmultiple pregnancy, but also estimates of the likelihood ofsingleton and multiple pregnancy, demographic factors, andpast treatment experience (8, 11).
There is also growing evidence that transient emotionalstates can influence decision making. Decisions made in anemotionally aroused state can differ substantially fromdecisions made in a nonaroused state and may lead to choicesinconsistent with long-term preferences (12). In addition,anticipated feelings (e.g., joy or sadness) can make a choiceappear to be more or less attractive (12). For example, patientdecisions to have a flu vaccination seem to be influenced by adesire to avoid anticipated future worry and regret rather thanby factual risk information provided (13).
Emotional states can also influence the process of riskassessment. In conditions of heightened arousal anduncertainty, memory and processing capacity can be impaired(14). For example, in a situation of nonmedical decision mak-ing, anxious individuals tended to select an option withoutconsidering every alternative (15). Decision making can alsobe emotion focused, and choices can reflect an effort to reducecurrent negative emotions (or to sustain positive feelings)rather than the result of a reasoned analysis of risks (16).For example, independently from objective risk, womenexperiencing elevated levels of anxiety were more likely toundergo genetic screening for breast cancer (17, 18), andhigher levels of anxiety have been linked to more frequentthan expected choice of bilateral mastectomy (18) and thechoice of alternativemedicine over conventional therapy (19).
The empirical evidence on the relation between mood andrisk taking is mixed, but a recent meta analysis concludedthat anger tends to evoke more risk-seeking choices andfear/anxiety sensitizes individuals to the likelihood of riskyevents and leads to ‘‘safer’’ (low-risk/low-reward) choices(20), whereas sadness can lead to a preference for high-risk/reward options (21). In contrast, in situations perceived tobe low risk, positive moods can lead people to underestimatethe likelihood of negative events and result in greater risk tak-ing (22). In situations viewed as high risk, positive moods maysensitize people to potential losses, resulting in risk-aversivebehavior, at least in economic decision-making/gamblingtasks (23).
Infertility has been conceptualized as a source of chronicstress with a variety of emotional consequences (24, 25), andIVF treatment has been characterized as additionally stressfulfor women who report decreased positive mood and increasednegative mood during an IVF cycle (26) and heightenedanxiety immediately before oocyte retrieval (26–28).However, it remains unclear whether pretreatment moodstates, preexisting levels of infertility stress, or changingmood states during a treatment cycle influence women'sdecision making. If mood states or infertility stress play arole, then transfer choices might be considered as ‘‘copingbehaviors’’ and IVF physicians would need to consider abroader approach, involving more than information giving,to facilitate effective decision making.
The purpose of the present study was to determinewhether mood states experienced by women during IVF
VOL. 100 NO. 2 / AUGUST 2013
treatment might influence decision making regarding embryotransfer. It was hypothesized that negative mood states wouldincrease over the course of a treatment cycle and that womenwould experience more acute negative mood states immedi-ately before egg retrieval compared with after embryo trans-fer. It was further hypothesized that women experiencingmore negative mood states or greater infertility stress wouldprefer multiple-embryo transfer, perceive the personal likeli-hood of experiencing multiple pregnancy as lower, and reporta greater desire for a multiple pregnancy. Conversely, thedevelopment of a positive mood state and its impact ontransfer decisions was uncertain and might be associatedwith either greater risk taking or greater risk aversion.
MATERIALS AND METHODSThis study was reviewed and approved by the Research EthicsBoard for Health Sciences Research Involving HumanSubjects (University of Western Ontario), and informedconsent was obtained from each of the participants.
Participants
Women participating in either a first or a second IVFtreatment cycle at a university-affiliated Canadian hospitalwere recruited from all patients consecutively referred forIVF treatment over a 2-year period. Women were requiredto be legally married or in a cohabiting relationship. Becausesingle women or women in same-sex relationships mighthave different attitudes toward multiple pregnancy andembryo transfer, and because it was not possible to examinethis question separately owing to limited sample sizes, thesegroups, together with women lacking fluency in English,were excluded from the study.
Measures
Mood. The Profile of Mood States (POMS) is a 30-itemstandardized self-report questionnaire which provides ameasure of five negative and one positive mood states(Depression, Tension, Anger, Fatigue, Confusion, and Vigor)and a Total Mood Disturbance score. For example, Tensionreflects subjective and physical anxiety with complaintssuch as feeling ‘‘nervous,’’ ‘‘anxious,’’ ‘‘uneasy,’’ and ‘‘tense’’and Vigor reflects a state of physical well-being such asfeeling ‘‘energetic,’’ ‘‘lively,’’ ‘‘active,’’ or ‘‘vigorous.’’ Respon-dents rate the extents to which different mood adjectives areapplicable on a 5-point Likert scale from 0 (‘‘not at all’’) to4 (‘‘extremely’’) for the past week. The questionnaire hasdemonstrated reliability and validity (29).
Attitudes toward embryo transfer. To assess attitudes towardembryo transfer and multiple pregnancy, women werepresented with two hypothetical scenarios and asked toindicate, through a forced choice format, their preferredchoice for embryo transfer (Fig. 1). In the first scenario, twogood-quality embryos were assumed to be available andwomen were asked to indicate a preference for eSET or thetransfer of two embryos (2ET). Women then rated the strengthof this preference on a 10-point Likert scale where a low scoreindicated a stronger preference for eSET and a high score a
531
FIGURE 1
Schematic presentation of the study design: two scenarios for embryo transfer, assessment of transfer preferences and attitude toward multiplepregnancy. 2ET ¼ two-embryo transfer; 3ET ¼ three-embryo transfer; eSET ¼ elective single-embryo transfer.Newton. Mood, stress, and preferences for embryo transfer. Fertil Steril 2013.
ORIGINAL ARTICLE: MENTAL HEALTH, SEXUALITY, AND ETHICS
stronger preference for 2ET. Women then rated the perceivedriskiness of this choice, the desirability of a twin versussingleton pregnancy, and the estimated personal likelihoodof experiencing a twin pregnancy with 2ET. Reflecting knownoutcome data, women were informed of a 43% chance of apregnancy with 2ET and a 33% chance a birth would involvetwins versus a 39% chance of pregnancy with eSET and a 1%chance of twins (30). In the second scenario, assuming thatthree embryos were available for transfer (3ET); womenwere asked to indicate a preference for 2ET or 3ET, strengthof preference, perceived risk, desire for triplet pregnancy,and estimated chance of triplet pregnancy with 3ET. Womenwere informed of a 48% chance of pregnancy, a 36% chanceof twins, and a 9% chance of triplets with 3ET (31).
Fertility Problem Inventory. The Fertility Problem Inventory(FPI) is a 46-item standardized self-report questionnaire withdemonstrated reliability and validity (32). The questionnaireprovides a measure of five different dimensions ofinfertility-specific stress including social stress, relationshipstress, sexual stress, need for parenthood, attitude towardchild-free living, and a global stress score. Participantsindicated their degree of agreement with each item(e.g., ‘‘When I see families with children I feel left out’’) on a6-point scale ranging from 1 (‘‘Strongly disagree’’) to 6(strongly agree’’).
Procedure
Baseline assessment. Women in their first IVF cyclewere enrolled during a regularly scheduled orientationappointment 1 month before starting treatment medications.Women returning for a second cycle were enrolled at their
532
first appointment, �14 days before oocyte retrieval. Allparticipants were interviewed separately without the presenceof a partner to assess attitudes toward embryo transfer andmultiple pregnancy. Women completed the POMS to assesscurrent mood states and the FPI to measure perceivedinfertility-specific stress.
Cycle end reassessment. At enrollment, women wererandomly assigned for reassessment either at late cycle stage(1 day before oocyte retrieval) or 30 minutes after embryotransfer. The same interviewer-administered questionnairewas used to reassess attitudes toward embryo transfer andmultiple pregnancy. Again the women were interviewedalone and then completed the POMS to assess current moodstates.
Information and decisions about transfer. Before a first IVFcycle, patients were verbally informed by their physician ofclinic policy to transfer 1–3 embryos in women <40 yearsold, depending on the number and quality of embryosavailable, and provided with a brief verbal description ofthe risks of multiple pregnancy. A final decision on thenumber of embryos to transfer wasmade through a discussionbetween the couple and a physician immediately before thetransfer procedure.
Statistical Analyses
Statistical analyses were performed with the StatisticalPackage for Social Sciences (version 19.0 for Windows;SPSS). Pearson correlation coefficients were calculated toassess the association between individual variables and thepredictive value of infertility stress. Repeated-measuresanalyses of variance (ANOVAs) were conducted to assess
VOL. 100 NO. 2 / AUGUST 2013
Fertility and Sterility®
changes in strength of transfer preferences, perceptions ofrisk, mood states as measured by the POMS, and attitudestowardmultiple pregnancy across time (from baseline to cycleend) and between groups (e.g., women reassessed before eggretrieval or after embryo transfer, women with or withoutbiologic children).
Hierarchic multiple regression was used to test if changesin mood states from baseline to cycle end were associatedwith corresponding changes in strength of transferpreferences and perceptions of risk, desire for, and perceivedlikelihood of experiencing a twin or triplet pregnancy.
RESULTSDemographic Characteristics
A total of 320 women were invited to participate and176 women (55%) completed the baseline assessment. Ofthose women, 61% (107/176) completed the reassessment atcycle end (48 women before egg retrieval and 59 women onthe day of embryo transfer). Women who completed bothphases of the study did not differ from women completingonly baseline measures regarding strength of transferpreferences, desire for, or expectations of experiencing atwin or triplet pregnancy, POMS mood scores, or FPI globalinfertility stress. The majority of women (85%) had noprevious experience with embryo transfer. Patient character-istics are presented in Table 1. The treatment cycle was fullypaid by government health insurance for almost one-half ofthe women.
Mood States and Risk Taking
Transient mood states were not associated with strength ofpreference for 2ET (vs. eSET) or 3ET (vs. 2ET) at either baselineor the end of the cycle. However, mood states were associatedwith perceptions of risk.At baseline, amongwomenwho chose2ET (vs. eSET), those experiencing higher Total NegativeMoodscores (r ¼ 0.20; P< .05), including higher Tension scores(r ¼ 0.28; P< .001) and higher levels of Confusion (r ¼ 0.23;
TABLE 1
Patient characteristics.
Characteristic Data
Participants enrolled 176Participants completing both baseline and
reassessment107
Age (y), mean (SD) 33.1 (4.0)Duration of infertility (mo), mean (SD) 35.2 (31.2)Primary infertility, % 89.2First IVF treatment cycle, % 84.7IVF treatment government funded, % 42.6Cause of infertility, %
Newton. Mood, stress, and preferences for embryo transfer. Fertil Steril 2013.
VOL. 100 NO. 2 / AUGUST 2013
P< .05), rated 2ET as more risky. Among women who chose3ET (vs. 2ET), those reporting higher Tension scores rated theirchoice as more risky (r ¼ 0.20; P< .05). At cycle end, Tensionscores were the onlymood state associated with perceptions ofrisk. Among womenwho chose 2ET (vs. eSET), those reportinghigher Tension scores rated this preference as more risky(r ¼ 0.23; P< .05).
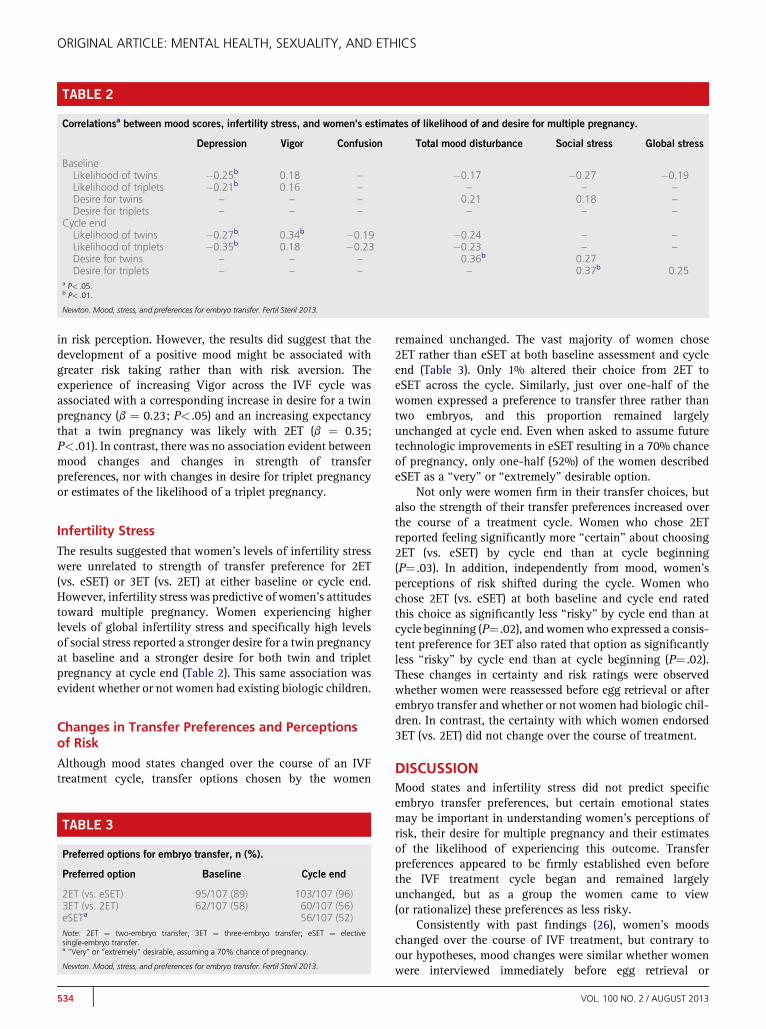
No specific mood states were associated with desire for atwin or triplet pregnancy, but women reporting a greatermood disturbance overall reported a stronger desire for twinpregnancy (Table 2) both at baseline and again at cycle end.Associations were observed between particular mood statesand perceptions of risk regarding estimates of the personallikelihood of experiencing twin pregnancy with 2ET or atriplet pregnancy with the 3ET. At baseline, women reportinghigher Depression scores and lower Vigor scores estimated thechance of experiencing both twin and triplet pregnancy aslower than did women reporting normal moods. Similarly atcycle end, women reporting lower Vigor scores and higherDepression, Confusion, and Total Mood Disturbance scoresestimated the personal chance of both twin and tripletpregnancy as lower than did women reporting normal moods(Table 2).
Changes in Mood States
Women's mood states changed significantly during thecourse of the treatment cycle. Women reported a significantincrease in Total Mood Disturbance between baseline andthe end of the treatment cycle (P< .001). Separate ANOVAsfor individual mood states indicated that increased Tension(P< .01), Anger (P< .001), and Fatigue (P< .001) anddecreased Vigor (P< .01) across the cycle each contributedto the overall mood change. Contrary to our hypothesis,similar mood changes were evident whether women werereassessed before egg retrieval or immediately after embryotransfer, whether or not women had existing children, andwhether this was a first or subsequent IVF cycle.
Changes in Mood States and Changes in RiskTaking
Hierarchic multiple regression was used to test whetherobserved changes in mood from baseline to cycle end wereassociated with corresponding changes in strength ofpreference for 2ET (vs. eSET) and 3ET (vs. 2ET), perceptionsof the riskiness in choosing 2ET (vs. eSET) and 3ET(vs. 2ET), desire for twin and triplet pregnancy, and perceivedlikelihood of experiencing a twin or triplet pregnancy. Inparticular, we tested the hypothesis that increases in Tension,Anger, and Fatigue and decreases in Vigor would give rise tochoices indicative of greater risk taking.
Among women who chose 2ET (vs. eSET) at both baselineand cycle end, an increase in Tension scores across the IVFcycle was associated with an increase in the perceivedriskiness of 2ET (b¼ 0.25; P< .05). In contrast, among womenwith a continued preference for 3ET, increasing Tension wasnot associated with any increase in the perceived risk of thisoption. No other mood changes were associated with changes
533
TABLE 2
Correlationsa between mood scores, infertility stress, and women's estimates of likelihood of and desire for multiple pregnancy.
Depression Vigor Confusion Total mood disturbance Social stress Global stress
BaselineLikelihood of twins �0.25b 0.18 – �0.17 �0.27 �0.19Likelihood of triplets �0.21b 0.16 – – – –
Desire for twins – – – 0.21 0.18 –
Desire for triplets – – – – – –
Cycle endLikelihood of twins �0.27b 0.34b �0.19 �0.24 – –
Likelihood of triplets �0.35b 0.18 �0.23 �0.23 – –
Desire for twins – – – 0.36b 0.27Desire for triplets – – – – 0.37b 0.25
a P< .05.b P< .01.
Newton. Mood, stress, and preferences for embryo transfer. Fertil Steril 2013.
ORIGINAL ARTICLE: MENTAL HEALTH, SEXUALITY, AND ETHICS
in risk perception. However, the results did suggest that thedevelopment of a positive mood might be associated withgreater risk taking rather than with risk aversion. Theexperience of increasing Vigor across the IVF cycle wasassociated with a corresponding increase in desire for a twinpregnancy (b ¼ 0.23; P< .05) and an increasing expectancythat a twin pregnancy was likely with 2ET (b ¼ 0.35;P< .01). In contrast, there was no association evident betweenmood changes and changes in strength of transferpreferences, nor with changes in desire for triplet pregnancyor estimates of the likelihood of a triplet pregnancy.
Infertility Stress
The results suggested that women's levels of infertility stresswere unrelated to strength of transfer preference for 2ET(vs. eSET) or 3ET (vs. 2ET) at either baseline or cycle end.However, infertility stress was predictive of women's attitudestoward multiple pregnancy. Women experiencing higherlevels of global infertility stress and specifically high levelsof social stress reported a stronger desire for a twin pregnancyat baseline and a stronger desire for both twin and tripletpregnancy at cycle end (Table 2). This same association wasevident whether or not women had existing biologic children.
Changes in Transfer Preferences and Perceptionsof Risk
Although mood states changed over the course of an IVFtreatment cycle, transfer options chosen by the women
TABLE 3
Preferred options for embryo transfer, n (%).
Preferred option Baseline Cycle end
2ET (vs. eSET) 95/107 (89) 103/107 (96)3ET (vs. 2ET) 62/107 (58) 60/107 (56)eSETa 56/107 (52)Note: 2ET ¼ two-embryo transfer; 3ET ¼ three-embryo transfer; eSET ¼ electivesingle-embryo transfer.a‘‘Very’’ or ‘‘extremely’’ desirable, assuming a 70% chance of pregnancy.
Newton. Mood, stress, and preferences for embryo transfer. Fertil Steril 2013.
534
remained unchanged. The vast majority of women chose2ET rather than eSET at both baseline assessment and cycleend (Table 3). Only 1% altered their choice from 2ET toeSET across the cycle. Similarly, just over one-half of thewomen expressed a preference to transfer three rather thantwo embryos, and this proportion remained largelyunchanged at cycle end. Even when asked to assume futuretechnologic improvements in eSET resulting in a 70% chanceof pregnancy, only one-half (52%) of the women describedeSET as a ‘‘very’’ or ‘‘extremely’’ desirable option.
Not only were women firm in their transfer choices, butalso the strength of their transfer preferences increased overthe course of a treatment cycle. Women who chose 2ETreported feeling significantly more ‘‘certain’’ about choosing2ET (vs. eSET) by cycle end than at cycle beginning(P¼ .03). In addition, independently from mood, women'sperceptions of risk shifted during the cycle. Women whochose 2ET (vs. eSET) at both baseline and cycle end ratedthis choice as significantly less ‘‘risky’’ by cycle end than atcycle beginning (P¼ .02), and womenwho expressed a consis-tent preference for 3ET also rated that option as significantlyless ‘‘risky’’ by cycle end than at cycle beginning (P¼ .02).These changes in certainty and risk ratings were observedwhether women were reassessed before egg retrieval or afterembryo transfer and whether or not women had biologic chil-dren. In contrast, the certainty with which women endorsed3ET (vs. 2ET) did not change over the course of treatment.
DISCUSSIONMood states and infertility stress did not predict specificembryo transfer preferences, but certain emotional statesmay be important in understanding women's perceptions ofrisk, their desire for multiple pregnancy and their estimatesof the likelihood of experiencing this outcome. Transferpreferences appeared to be firmly established even beforethe IVF treatment cycle began and remained largelyunchanged, but as a group the women came to view(or rationalize) these preferences as less risky.
Consistently with past findings (26), women's moodschanged over the course of IVF treatment, but contrary toour hypotheses, mood changes were similar whether womenwere interviewed immediately before egg retrieval or
VOL. 100 NO. 2 / AUGUST 2013
Fertility and Sterility®
immediately after embryo transfer, and no particular moodstates were associated with the strength of any specifictransfer preferences (e.g., eSET vs. 2ET). However, changesin one particular mood state, Tension (subjective and physicalfeelings of anxiety) did appear to be quite relevant in under-standing women's perceptions of risk. Higher tension/anxietylevels appear to be associated with perceptions of higher riskboth before treatment and at the end of the cycle, andincreases in a woman's anxiety level across the cycle leadto corresponding increases in her perceptions of risk.
Traditionally, it has been understood that relevant medicalrisk information heightens concern (tension/anxiety) and asso-ciated perceptions of increased risk,which then lead to different(safer) transfer choices. As a result, both feelings of anxiety andobjective risk are reduced. The present findings offer addedevidence that negative states, such as anxiety, can activatehigher estimates of the likelihood of risky events occurring(20). However, anxious feelings were not associated with‘‘safer’’ choices. In fact, anxious patients viewed both 2ET (vs.eSET) and 3ET (vs. 2ET) asmoremedically risky, and as anxietylevels rose during the IVF cycle women paradoxically grewmore certain in their preference to transfer more rather thanfewer embryos. Therefore, the present findings suggest thatthe linkage among mood states, perceived risk, and behavioris more complex than traditionally assumed and might explainwhy, even when relevant risk information is provided, transferchoices seem to be largely unaffected (10, 33, 34).
There may be two underlying mechanisms. First, in somesituations induced negative states have been known toincrease the preference for risky options, and it has beenargued that people who feel bad may be more willing totake chances to cope with (reduce) an unpleasant emotionalstate (16). Second, the perceived risk of not achieving a preg-nancy might override medical concerns. Viewed this way, theanxious patient, rather than gambling on eSET, makes a‘‘safer’’ decision to transfer more embryos. There is someevidence for the latter, because expectations about thelikelihood of pregnancy can be more influential than riskinformation in determining transfer preferences (8). Thequestion of which risks are most salient needs further study.
The present findings also suggest that the experience ofmarked negative or positive mood states during the IVF cyclemight indirectly influence the choice of more risky transferoptions. Both before treatment and at the end of the cycle,women experiencing more general distress, feelings ofdepression, and reduced vigor viewed the likelihood ofexperiencing either a twin or triplet pregnancy as lowerthan did women reporting normal mood states. Depression,commonly reported before or during an IVF cycle (25), hasbeen associated with negative expectations about futureevents (35). Therefore, a preference for multiple-embryotransfer might be related to deteriorating mood with atendency to underestimate the likelihood of any pregnancy.Unfortunately, the depressed patient who experiences amultiple pregnancy might also be most vulnerable to thestresses of a multiple birth and more likely to experiencepostpartum depression (36).
Although the development of positive feelings during anIVF cycle might be seen as a favorable development, it should
VOL. 100 NO. 2 / AUGUST 2013
be noted that positive moods can lead people to underestimatelikelihood of negative events and result in greater risk taking(22). In the present study, women who experienced increasingfeelings of energy and optimism also reported a correspond-ing increase in desire for a twin pregnancy and a growingexpectancy that twin pregnancy was likely. Therefore,markedly positive emotions could lead women to experiencefalse confidence, underestimate or ignore potential risks, andthereby welcome the transfer of multiple embryos.
As with mood states, women's level of infertility specificstress was not predictive of actual embryo transferpreferences, at either the beginning or the end of the IVFcycle. However, women experiencing greater global infertilitystress and particularly greater social stress related toinfertility had a stronger desire for both twin pregnancyand triplet pregnancy at the end of the cycle. One advantageof multiple birth identified by women with fertility problemsis the opportunity to have an instant family (37), and forwomen finding social situations difficult due to theirinfertility this might well seem to be an attractive option.
As the time approached for final decision making, thewomen as a group seemed to grow more confident in theirchoice to transfer more rather than fewer embryos, in termsof feeling both more certain about this option and lessconcerned about possible risks. The basis for this change isunclear. Women may have received new and relevantinformation over the course of the cycle that reduced theperceived risks inherent in multiple-embryo transfer.However, the women's views were similar whether askedbefore egg retrieval or after embryo transfer, suggestingthat these judgments were not much influenced by embryonumber or quality. Women's characterization of 2ET(vs. eSET) as less risky by cycle end might reflect a greaterconcern about the risk of not becoming pregnant, as discussedpreviously. Alternatively, it might reflect an effort to elimi-nate ‘‘cognitive dissonance’’ (38), i.e., an uncomfortablefeeling caused by holding conflicting ideas simultaneously(i.e., having a preference for a riskier choice). In situationsviewed as less risky, individuals have been found to bemore likely to engage in greater risk taking (39). In the presentstudy, where most women already had a strong preexistingpreference for 2ET, a growing perception that 2ET was lessrisky understandably did not translate into a shift in transferpreferences, but it might in another context among womenwho had an initial preference for eSET. This shift in riskperception needs further study, because it suggests anotherfactor that might militate against eSET.
For patients, the time of embryo transfer is a crucial stagein IVF treatment and likely to be fraught with emotion,particularly anxiety, and the possibility that transientemotional states might affect decision making has a numberof implications. First, physicians need to be sensitive tounexpected changes in transfer preferences, because anxiousor depressed mood might lead to a decision inconsistent withlong-term goals. Second, physicians need to be aware that thecontent and manner in which risk information is providedmight provoke an expected emotional reaction (heightenedanxiety) but lead to an unexpected transfer decision. Wherea marked mood states are evident and choices may reflect
535
ORIGINAL ARTICLE: MENTAL HEALTH, SEXUALITY, AND ETHICS
‘‘coping behaviors,’’ adjunct counseling for some patientsmight address certain known thought patterns associatedwith strong mood states (e.g., ‘‘jumping to conclusions’’ or‘‘all-or-nothing thinking’’) and how such thinking might beinfluencing decision making (40). Therefore, facilitatingeffective decision making may require more than providingfactual information and at times could benefit from a moremultidisciplinary approach using the skills of a healthpsychologist. Finally, the day of embryo transfer, when thenumber and quality of embryos is known, is often highlightedas the day for serious and final discussion of transfer options(41). However, the present results suggest that transferpreferences can solidify at an early stage and could berelatively impervious to events and feedback during theongoing cycle. This would suggest the merit of providinginformation and an opportunity for discussion at severalpoints during the treatment cycle.
This study represents the only known research examiningthe role of mood in decision making about IVF embryo trans-fer. However, positivemoodwas assessed bymeans of a singlebrief scale which assessed feelings of energy and enthusiasm,and there may be other positive states (e.g., happiness,contentment) that are equally or more relevant. Futureresearch might use a broader measure of positive emotions.In addition, the way in which men's emotions and opinionsmight affect women's attitudes to transfer were not examinedand remains unclear. Past research has suggested that womenviewed their partners as having amajor influence on the trans-fer decision (42), but other findings indicated that men viewedthemselves as less influential and that women's satisfactionwith the transfer decision was unrelated to partner participa-tion (8). Finally, the present study assessed the strength of hy-pothetic transfer preferences, but not the actual number ofembryos transferred. The latter measure is highly relevant totreatment outcome and is often seen as the criterion standard,although final transfer decisions might be heavily influencedby external factors such as the physician's recommendationand clinic policies. However, the influence of mood on actualtransfer decisions needs investigation, particularly amongpatients who receive standardized information about the risksand benefits of different transfer options.
Acknowledgments: The authors thank Joanna McBride forcollection of the data, London Health Sciences Centre andparticularly the nursing staff for their assistance in recruitingparticipants for the study, and Francis Tekpetey for hissupport of the project.
REFERENCES1. Pandian A, Templeton A, Serour G, Bhattacharya S. Number of embryos
for transfer after IVF and ICSI: a Cochrane review. Hum Reprod 2005;20:2681–7.
2. Gunby J. Assisted reproductive technologies (ART) in Canada: 2009 resultsfrom the Canadian ART Register. Available at: http://www.cfas.ca/index.php?option¼com_content&view¼article&id¼1169%3Acartr-annual-report-2009&catid¼1012%3Acartr&Itemid¼668. Accessed January31, 2012.
3. Centers for Disease Control and Prevention, U.S. Department of Health andHuman Services. Assisted reproductive technology success rates: national
536
summary and clinic reports. 2010. Available at: http://www.cdc.gov/art/ARTReports.htm. Accessed January 31, 2012.
4. Ryan GL, Zhang SH, Dokras A, Syrop CH, van Voorhis BJ. The desire ofinfertile patients for multiple births. Fertil Steril 2004;81:500–4.
5. Hojgaard A, Ottosen LDM, Kesmodel U, Ingerslev HJ. Patient attitudestoward twin pregnancies and single embyro transfer a questionnaire study.Hum Reprod 2007;22:2673–8.
6. Gleicher N, Campbell DP, Chan CL, Karande V, Rao R, Balin M, et al. Thedesire for multiple births in couples with infertility problems contradictspresent practice patterns. Hum Reprod 1995;10:1079–84.
7. Grobman WA, Milad M, Stout J, Klock SC. Patient perceptions of multiplegestations: an assessment of knowledge and risk aversion. Am J ObstetGynecol 2001;185:920–4.
8. Newton CR, McBride J, Feyles V, Tekpetey F, Power S. Factors affectingpatients' attitudes toward single- and multiple-embryo transfer. Fertil Steril2007;87:269–78.
9. Hope N, Rombauts L. Can an educational DVD improve the acceptability ofelective single embryo transfer? A randomized controlled study. Fertil Steril2010;94:489–95.
10. Murray S, Shetty A, Rattray A, Taylor V, Bhattacharya S. A randomizedcomparison of alternative methods of information provision on the accept-ability of elective single embryo transfer. Hum Reprod 2004;19:911–6.
11. van Peperstraten AM, Kreuwel IAM, Hermens RPMG, Nelen WLDM, vanDop PA, Grol RPTM, et al. Determinants of the choice for single or doubleembryo transfer in twin prone couples. Acta Obstet Gyn Scan 2008;87:226–31.
12. Loewenstein G. Hot-cold empathy gaps and medical decision making.Health Psychol 2005;24:S49–56.
13. Chapman GB, Coups EJ. Emotions and preventive health behavior: worry,regret and influenza vaccination. Health Psychol 2006;25:82–90.
14. Pham MT. Emotion and rationality: a critical review and interpretation ofempirical evidence. Rev Gen Psychol 2007;11:155–78.
15. Keinan G. Decision-making under stress—scanning of alternatives undercontrollable and uncontrollable threats. J Pers Soc Psychol 1987;52:639–44.
16. Power TE, Swartzman LC, Robinson JW. Cognitive-emotional decisionmaking (CEDM): a framework of patient medical decision making. PatientEduc Couns 2011;83:163–9.
17. France L, Gray J, Elwyn G, Tischkowitz M, Brain K, Sampson J, et al.Genetic testing considerations in breast cancer patients. J Genet Couns1999;8:289–99.
18. Schwartz MD, Peshkin BN, Valdimarsdottir H, Tereyak KP, Taylor KL.Decision making and decision support for hereditary breast-ovarian cancersusceptibility. Health Psychol 2005;24:S78–84.
19. Astin JA. Why patients use alternative medicine: results of a national study.JAMA 1998;279:1548–53.
20. Angie AD, Connelly S, Waples EP, Kligyte V. The influence of discreteemotions on judgement and decision-making: a meta-analytic review.Cogn Emot 2011;25:1393–422.
21. Raghunathan R, Pham MT. All negative moods are not equal: motivationalinfluences of anxiety and sadness on decision making. Organ Behav HumDecis Process 1999;79:56–77.
22. Johnson EJ, Tversky A. Affect, generalization and the perception of risk.J Pers Soc Psychol 1983;45:20–31.
23. Nygren TE, Isen AM, Taylor PJ, Dulin J. The influence of positive affect onthe decision rule in risk situations: focus on outcome (and especiallyavoidance of loss) rather than probability. Organ Behav Hum Decis Proc1996;66:59–72.
24. Greil AL. Infertility and psychological distress: a critical review of theliterature. Soc Sci Med 1997;45:1679–704.
25. Newton CR, Hearn MT, Yuzpe AA. Psychological assessment and follow-upafter in vitro fertilization: assessing the impact of failure. Fertil Steril 1990;54:879–86.
26. Klonoff-Cohen H, Chu E, Natarajan L, SieberW. A prospective study of stressamong women undergoing in vitro fertilization or gamete intrafallopiantransfer. Fertil Steril 2001;76:675–87.
27. Harlow CR. Stress and stress-related hormones during in-vitro fertilizationtreatment. Hum Reprod 1996;11:274–9.
28. Merari D. Psychological and hormonal changes in the course of in vitrofertilization. J Assist Reprod Genet 1992;9:161–9.
29. McNair DM, Lorr M, Droppleman LF. Manual: Profile of MoodStates, Revised. San Diego, CA: Educational and Industrial Testing Service;1992.
30. Thurin A, Hausken J, Hillensjo T, Jablonowska B, Pinborg A, Strandell A, et al.Elective single-embryo transfer versus double-embryo transfer in in vitrofertilization. N Engl J Med 2004;351:2392–402.
32. Newton CR, SherrardW, Glavac I. The fertility problem inventory: measuringperceived infertility-related stress. Fertil Steril 1999;72:54–62.
33. Hartshorne GM, Lilford RJ. Different perspectives of patients and health careprofessionals on the potential benefits and risks of blastocyst culture andmultiple embryo transfer. Hum Reprod 2002;17:1023–30.
34. Porter M, Bhattacharya S. Investigation of staff and patients' opinions of aproposed trial of elective single embryo transfer. Hum Reprod 2005;20:2523–30.
36. O'Hara MW, Swain AM. Rates and risk of postpartum depression—a meta-analysis. Int Rev Psychiatry 1996;8:37–54.
37. Pinborg A, Loft A, Schmidt L. Nyboe Andersen A. Attitudes of IVF/ICSI-twinmothers toward twins and single embryo transfer. Hum Reprod 2003;18:621–7.
38. Festinger L. A theory of cognitive dissonance. Stanford, CA: StanfordUniversity Press; 1957.
39. Nygren TE. Reacting to perceived high- and low-risk win-lose opportunitiesin a risky decision-making task: is it framing or affect or both?Motiv Emotion1998;22:73–98.
40. Clark DA, Beck A. Cognitive therapy of anxiety disorders: science andpractice. New York: Guilford; 2010.
41. Min J, Hughes E, Young D. Elective single embryo transfer following in vitrofertilization. J Obstet Gynaecol Can 2010;32:363–77.
42. BlennbornM, Nilson S, Hillervik C, Hellberg D. The couple's decision-makingin IVF: one or two embryos at transfer? Hum Reprod 2005;20:1292–7.