Effectiveness of diabetes and hypertension management by rural primary health-care workers (Behvarz workers) in Iran: a nationally representative observational study Farshad Farzadfar, MD, MPH, D.Sc Non Communicable Diseases Research Center Endocrinology and Metabolism Research Institute Tehran University of Medical Sciences July 13, 2012 1 SAPHIR Monthly Webinar
Transcript
Effectiveness of diabetes and hypertension management by rural primary health-care workers (Behvarz workers) in Iran: a nationally representative observational study
Farshad Farzadfar, MD, MPH, D.Sc
Non Communicable Diseases Research CenterEndocrinology and Metabolism Research Institute Tehran University of Medical Sciences
July 13, 2012
1
SAPHIR Monthly Webinar
2
Outline of the presentation
• Epidemiology of metabolic risk factors at global, regional, and country levels
• Objectives of the study
• Methodology and results of phase one of the study
• Methodology and results of phase two of the study
• Conclusion and take home messages
3
Global epidemiologic transition
4
Lopez et al. Lancet 2006
Age-standardized cardiovascular mortality trends in selected high-income countries
Vital registration data from WHO
0
4
8
12
16
20
1950 1960 1970 1980 1990 2000 2010
Year
Dea
th R
ate
(per
1,0
00)
USA
Denmark
Finland
Sweden
UK
Australia
Female - CVD
0
4
8
12
16
20
1950 1960 1970 1980 1990 2000 2010
Year
Dea
th R
ate
(per
1,0
00)
Male - CVD
Male Female
Regional FPG trends
6
North America
North America
Mal
eF
emal
e
North Africa and Middle East
Danaei et al. Lancet 2011
North Africa and Middle East
Ma
le F
em
ale
FPG, BMI and SBP trends in Iran between 1980 and 2008
FPG BMI SBP
7
Farzadfar et al. Lancet 2011, Finucane et al. Lancet 2011, Danaei et al. Lancet 2011
4.0
4.4
4.8
5.2
5.6
6.0
1980 1990 2000 2010
mm
ol/L
20
22
24
26
28
30
1980 1990 2000 2010
kg/m
^2
20
22
24
26
28
30
1980 1990 2000 2010kg
/m^2
115
120
125
130
135
140
1980 1990 2000 2010
mm
Hg
4.0
4.4
4.8
5.2
5.6
6.0
1980 1990 2000 2010
mm
ol/L
115
120
125
130
135
140
1980 1990 2000 2010
mm
Hg
The effects of risk factors on life expectancy in 2005, by region
Fe
ma
leL
ife
ex
pe
cta
nc
y
Southeast North-Northeast West Central National
Ma
leL
ife
ex
pe
cta
nc
y
Southeast North-Northeast West Central National
8Farzadfar, et al, population Health metrics, 2011
Iran’s health system
Inputs Rural areas Urban areas
Population 32% 68%
Primary healthcare system Well-established
High coverage rates
Inefficient
Low coverage rates
Insurance coverage 63% before 2005 and 94% in 2008
77%
General practitioners 6,250 52,700
Specialists 135 14,300
Nurses/midwives 4,470 62,600
Behvarz 32,000 0
9
Annual report of MoH . 2005 , Utilization study. 2005
The objectives of the study
• Phase one: Estimating prevalence, diagnosis and coverage of treatment for diabetes and hypertension by
residency area
Estimating the treatment effects of diabetes and hypertension by residency area
• Phase two:
Estimating the association of Behvarz density with levels of FPG (which has an integrated and well defined program in PHC) and SBP
10
11
Data source and definitions
• Data source: Non-Communicable diseases surveillance survey (2005)
• Diabetic definition: Fasting plasma glucose (FPG) ≥ 126 mg/dl or on medication to control blood sugar (either oral anti-hyperglycemic agents or insulin)
• Hypertensive definition: Blood pressure (SBP/DBP) ≥ 140/90 mmHg or on medication to control blood pressure
11
Estimation of treatment effects
• Matching:
– All treated individuals were matched to controls based on propensity score of their age, sex, BMI, education and wealth index
• Random intercept regression analysis with an instrumental variable:
– A proxy for potentially unobserved confounders that could affect the use of treatment but not the distribution of risk factors
12
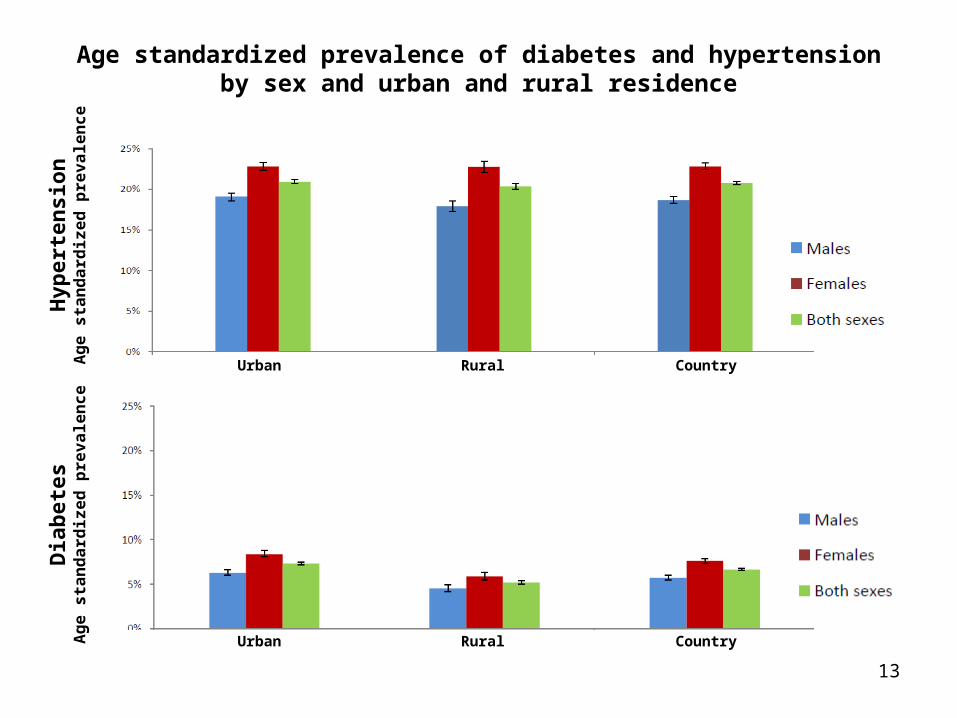
Age standardized prevalence of diabetes and hypertension by sex and urban and rural residence
13
Hyp
erte
nsi
on
Ag
e s
tan
da
rdiz
ed
pre
va
len
ce
RuralUrban Country
Dia
bet
esA
ge
sta
nd
ard
ize
d p
rev
ale
nc
e
RuralUrban Country
Diabetes and hypertension diagnosis in Iran
14
Coverage of treatments for diabetes and hypertension in Iran by sex and urban and rural residence
15
Dia
bet
esC
rud
e c
ov
era
ge
of
tre
atm
en
t (
pe
rce
nt)
RuralUrban Country
Hyp
erte
nsi
on
Cru
de
co
ve
rag
e o
f tr
ea
tme
nt
(p
erc
en
t)
RuralUrban Country
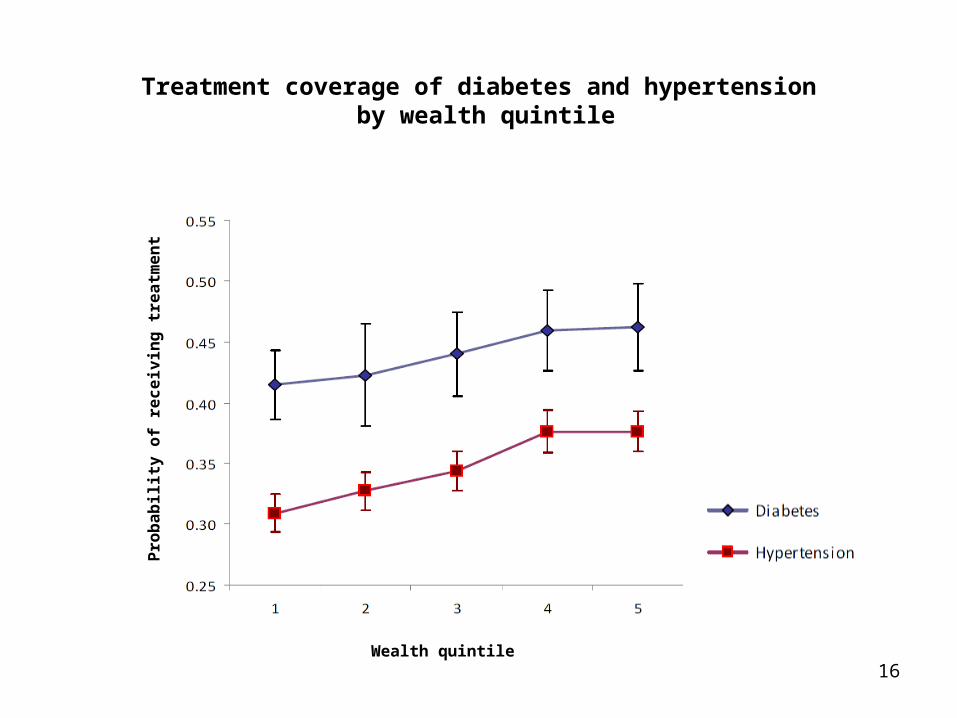
Treatment coverage of diabetes and hypertension by wealth quintile
Pro
ba
bil
ity
of
rec
eiv
ing
tre
atm
en
t
16Wealth quintile
Coefficients of regression to estimate the effect of diabetes and hypertension treatment on fasting plasma glucose and systolic blood pressure of treated
individuals
17
The average effect of treatment by area of residency
18
Tre
atm
en
t e
ffe
cts
fo
r h
yp
ert
en
siv
ein
div
idu
als
(m
mH
g)
RuralUrban
Tre
atm
en
t e
ffe
cts
fo
r d
iab
eti
cs
(m
mo
l/L
)
RuralUrban
What could be the reason for the diabetes treatment effect differences between rural and urban areas?
• Physician: Outpatient care center mapping (2005)
• ICU bed Ministry of health database (2005)
• Other socioeconomic indicators Census data (2006)
21
22
Methods
• Propensity score matching:
– Individuals living in districts falling in different Behvarz density quintiles were matched based on age, sex, body mass index (BMI), education, marital status, wealth index, physician density, ICU bed density and employment rate
• District level random intercept regression:
– Adjust for age, sex, BMI, education, marital status, wealth index, physician density, ICU bed density and employment rate
22
The association between Behvarz and physician densities and district average wealth index
23
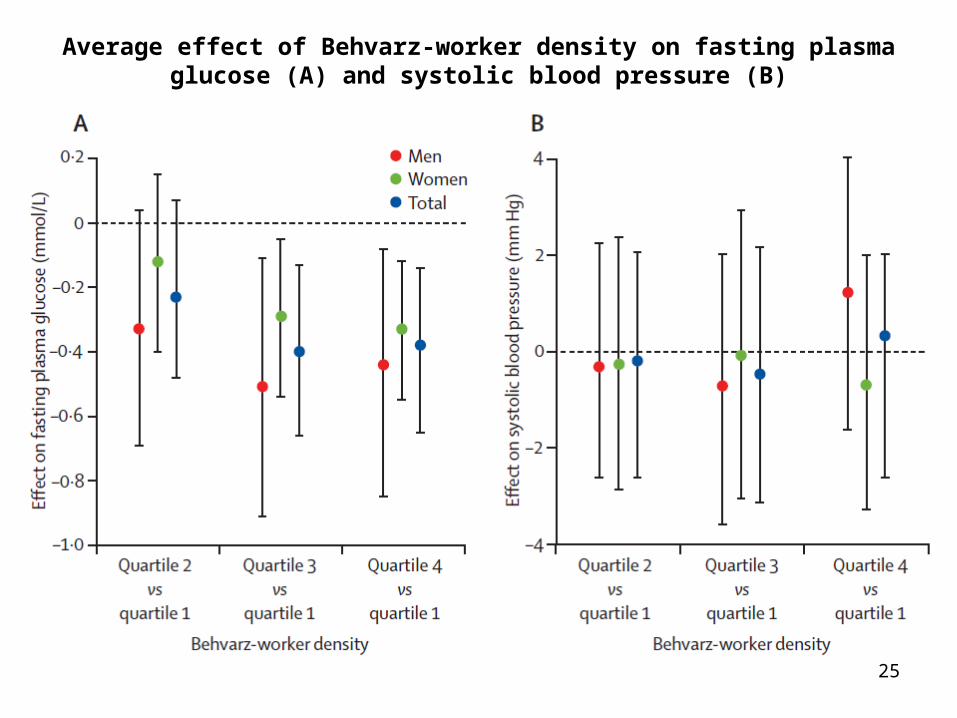
Coefficients of regression to estimate the effect of Behvarz-worker density on fasting plasma glucose and systolic blood pressure in Iran
24
Average effect of Behvarz-worker density on fasting plasma glucose (A) and systolic blood pressure (B)
25
Take home messages
• Risk factors with large burden but no current program to control
• Sub-national level policy making
• Primary healthcare as an effective management of chronic conditions such as diabetes


































![Developing an Observational Technique of Assessing and ...ijshr.com/IJSHR_Vol.2_Issue.2_April2017/IJSHR001.pdf · ergonomic related syndromes and complaints among the workers. [12-14]](https://static.documents.pub/doc/80x56/5ed4d98b8811581aea4da0ce/developing-an-observational-technique-of-assessing-and-ijshrcomijshrvol2issue2april2017.jpg)







