Efficacy and predictors of long-term treatment success for Cognitive-Behavioral Treatment and Behavioral Weight-Loss-Treatment in overweight individuals with binge eating disorder Simone Munsch a, * , Andrea H. Meyer b,1 , Esther Biedert a, 2 a University of Fribourg, Department of Psychology, 2 Rue de Faucigny, CH-1700 Fribourg, Switzerland b University of Basel, Faculty of Psychology, Department of Clinical Psychology and Epidemiology, Division of Applied Statistics in Life Sciences, Missionsstrasse 62a, CH-4055 Basel, Switzerland article info Article history: Received 14 February 2012 Received in revised form 28 August 2012 Accepted 29 August 2012 Keywords: BED Cognitive-Behavioral Therapy Behavioral Weight-Loss-Treatment Long-term follow-up Predictors abstract Objective: The aim of the study was to assess the long-term efficacy of Cognitive-Behavioral Treatment (CBT) and Behavioral Weight-Loss-Treatment (BWLT) in patients with binge eating disorder (BED) and to identify potential predictors of long-term treatment success. Method: In a sample of overweight to obese BED patients from a randomized comparative trial we evaluated the efficacy of four months of CBT or BWLT, followed by 12 months extended care, and a final follow-up assessment 6 years after the end of active treatment. Outcomes included binge eating, eating disorder pathology, depressive feelings, and body mass index. Results: After a strong improvement during active treatment, outcomes worsened during follow-up, yet remained improved at 6-year follow-up relative to pretreatment values. Long-term effects between CBT and BWLT were comparable. Rapid response during the early treatment phase was the only characteristic that was predictive of favorable treatment outcome in the long term. Conclusions: Both CBT and BWLT can be considered to be comparably efficacious in the long-term. Patients not responding strongly enough during the first four therapy sessions might be in need of tailored interventions early during the treatment phase. Ó 2012 Published by Elsevier Ltd. Introduction Binge eating disorder (BED) is likely to achieve canonical status as fully recognized subcategory of eating disorders in DSM-V. Binge eating is associated with significant distress as feelings of disgust, shame and guilt regularly occur. BED represents the most common eating disorder and its prevalence rates amount up to 3% (Striegel- Moore & Franko, 2008). On average 3.5% of women and 2% of men will develop BED during lifetime (Yager, 2008). More than 60% of all patients suffering from BED additionally suffer from obesity with ongoing weight gain (Striegel-Moore et al., 2001). Additional impairment stems from higher rates of comorbid mental disorders in BED patients such as affective, anxiety and substance use disorder (Hudson, Hiripi, Pope, & Kessler, 2007). Psychological treatments such as cognitive-behavioral therapy (CBT) and interpersonal therapy (IPT) are most extensively studied and strong evidence supports their efficacy regarding binge eating and to different degrees regarding accompanying eating disorder and general psychopathology (Wilson, Wilfley, Agras, & Bryson, 2010). Despite the identification of efficacious short- and longer term treatment options for BED, findings regarding treatment outcome reveal a broad range of variation with remission rates between 41 and 87% for CBT, IPT and behavioral weight loss (BWLT) approaches at the end of treatment (Agras et al., 1995; Agras, Telch, Arnow, Eldredge, & Marnell, 1997; Eldredge et al., 1997; Hilbert et al., 2012; Munsch et al., 2007; Telch, Agras, Rossiter, Wilfley, & Kenardy, 1990; Wilfley et al., 2002; Wilson et al., 2010). Alto- gether recent findings indicate a slightly weaker effect for BWLT programs in eliminating binge eating during the first two years after treatment than specialized psychological treatments (Munsch et al., 2007; Vocks et al., 2010; Wilson et al., 2010). But with respect * Corresponding author. Tel.: þ41 26 300 76 57/55; fax: þ41 26 300 97 12. E-mail addresses: [email protected](S. Munsch), andrea.meyer@ unibas.ch (A.H. Meyer), [email protected](E. Biedert). 1 Tel.: þ41 61 267 06 55; fax: þ41 61 267 06 59. 2 Tel.: þ41 41 726 57 57; fax: þ41 41 726 57 90. Contents lists available at SciVerse ScienceDirect Behaviour Research and Therapy journal homepage: www.elsevier.com/locate/brat 0005-7967/$ e see front matter Ó 2012 Published by Elsevier Ltd. http://dx.doi.org/10.1016/j.brat.2012.08.009 Behaviour Research and Therapy 50 (2012) 775e785
Transcript
at SciVerse ScienceDirect
Behaviour Research and Therapy 50 (2012) 775e785
Contents lists available
Behaviour Research and Therapy
journal homepage: www.elsevier .com/locate/brat
Efficacy and predictors of long-term treatment success for Cognitive-BehavioralTreatment and Behavioral Weight-Loss-Treatment in overweight individuals withbinge eating disorder
Simone Munsch a,*, Andrea H. Meyer b,1, Esther Biedert a,2
aUniversity of Fribourg, Department of Psychology, 2 Rue de Faucigny, CH-1700 Fribourg, SwitzerlandbUniversity of Basel, Faculty of Psychology, Department of Clinical Psychology and Epidemiology, Division of Applied Statistics in Life Sciences, Missionsstrasse 62a,CH-4055 Basel, Switzerland
a r t i c l e i n f o
Article history:Received 14 February 2012Received in revised form28 August 2012Accepted 29 August 2012
0005-7967/$ e see front matter � 2012 Published byhttp://dx.doi.org/10.1016/j.brat.2012.08.009
a b s t r a c t
Objective: The aim of the study was to assess the long-term efficacy of Cognitive-Behavioral Treatment(CBT) and Behavioral Weight-Loss-Treatment (BWLT) in patients with binge eating disorder (BED) and toidentify potential predictors of long-term treatment success.Method: In a sample of overweight to obese BED patients from a randomized comparative trial weevaluated the efficacy of four months of CBT or BWLT, followed by 12 months extended care, and a finalfollow-up assessment 6 years after the end of active treatment. Outcomes included binge eating, eatingdisorder pathology, depressive feelings, and body mass index.Results: After a strong improvement during active treatment, outcomes worsened during follow-up, yetremained improved at 6-year follow-up relative to pretreatment values. Long-term effects between CBTand BWLT were comparable. Rapid response during the early treatment phase was the only characteristicthat was predictive of favorable treatment outcome in the long term.Conclusions: Both CBT and BWLT can be considered to be comparably efficacious in the long-term.Patients not responding strongly enough during the first four therapy sessions might be in need oftailored interventions early during the treatment phase.
� 2012 Published by Elsevier Ltd.
Introduction
Binge eating disorder (BED) is likely to achieve canonical statusas fully recognized subcategory of eating disorders in DSM-V. Bingeeating is associated with significant distress as feelings of disgust,shame and guilt regularly occur. BED represents the most commoneating disorder and its prevalence rates amount up to 3% (Striegel-Moore & Franko, 2008). On average 3.5% of women and 2% of menwill develop BED during lifetime (Yager, 2008). More than 60% of allpatients suffering from BED additionally suffer from obesity withongoing weight gain (Striegel-Moore et al., 2001). Additionalimpairment stems from higher rates of comorbid mental disorders
in BED patients such as affective, anxiety and substance usedisorder (Hudson, Hiripi, Pope, & Kessler, 2007).
Psychological treatments such as cognitive-behavioral therapy(CBT) and interpersonal therapy (IPT) are most extensively studiedand strong evidence supports their efficacy regarding binge eatingand to different degrees regarding accompanying eating disorderand general psychopathology (Wilson, Wilfley, Agras, & Bryson,2010). Despite the identification of efficacious short- and longerterm treatment options for BED, findings regarding treatmentoutcome reveal a broad range of variation with remission ratesbetween 41 and 87% for CBT, IPT and behavioral weight loss (BWLT)approaches at the end of treatment (Agras et al., 1995; Agras, Telch,Arnow, Eldredge, & Marnell, 1997; Eldredge et al., 1997; Hilbertet al., 2012; Munsch et al., 2007; Telch, Agras, Rossiter, Wilfley, &Kenardy, 1990; Wilfley et al., 2002; Wilson et al., 2010). Alto-gether recent findings indicate a slightly weaker effect for BWLTprograms in eliminating binge eating during the first two yearsafter treatment than specialized psychological treatments (Munschet al., 2007; Vocks et al., 2010; Wilson et al., 2010). But with respect
S. Munsch et al. / Behaviour Research and Therapy 50 (2012) 775e785776
to weight loss, BWLT seems to be the only psychological treatmentachieving at least moderate results (Devlin et al., 2005; Grilo,Masheb, Brownell, Wilson, & White, 2007; Munsch et al., 2007;Vocks et al., 2010; Wilson et al., 2010).
Even though for binge eating there are valuable treatmentoptions, a considerable percentage of patients in most studies stilldo not achieve remission from binge eating. Hence an importantresearch priority concerns the identification of predictors ofsuccessful treatment outcome (Kraemer, Wilson, Fairburn, & Agras,2002; Wilson, Grilo, & Vitousek, 2007). Recent studies haveinvestigated several pretreatment factors potentially predictingtreatment outcomes in BED. But these findings remain isolated, asthey do not reveal a stable predictive association of these factorswith binge eating and mostly fail to be corroborated in differentpopulations and study settings (Grilo, White, Wilson, Gueorguieva,&Masheb, 2012;Masheb &Grilo, 2008b;Wilson et al., 2010). One ofthe predictive factors that have been investigated intensivelyrelates to initial treatment response. Rapid response defined asa reduction of binge eating of at least 65% within the first fourweeks of treatment was repeatedly and reliably observed indifferent treatment studies for BED by Grilo et al. (2012) (see therefor an overview). It was found that rapid response led to increasedrates of remission from binge eating episodes but that this effectvaried between different treatment options for BED. As an example,in CBT whether applied through face-to-face treatment or by self-help, individuals without rapid response caught up and improveduntil the end of the treatment, whereas in pharmacological andBWLT self-help offers, lack of rapid response was associated withless favorable treatment effects. Another important issue in BEDtreatment research is the lack of data regarding the comparativelong-term efficacy between BWLT, CBT, and IPT. This is an impor-tant problem, as BWLT is frequently applied as treatment option forBED because of its short-term efficacy in weight loss and its cost-effectiveness compared to other treatment options. In addition,other professionals than psychotherapists can implement BWLT aswell. Because the availability of other specialized psychologicaltreatments such as IPT is limited at least in Europe, there isa specific interest in studying long-term efficacy of CBT and BWLTtreatments (Yager, 2008).
The present study therefore examines the efficacy of CBT andBWLT in a randomized comparative treatment trial (Munsch et al.,2007) up to 6-year follow-up. Based on the literature and on theresults that we obtained when analyzing data up to 12 monthfollow-up, our main hypothesis is that CBT will lead to sustainedbeneficial effects regarding binge eating relative to BWLT. Furtherwe suppose that the CBT approach will lead to a stronger long-termreduction of negative affect compared to BWLT. With respect tobody weight change we expect both treatments to reveal compa-rable and minimal effects in the long term.
In order to shed light on factors allowing to predict the long-term course in BED, we concentrate on robust constructs such asrapid response, but also include a broader range of characteristicssuch as intensity of eating disorder symptoms, BMI, negative affect,and existence of comorbidity (Hilbert, Saelens, et al., 2007; Masheb& Grilo, 2008a;Wilson et al., 2010) at both pre- and post-treatment.Additionally we investigate the predictive effect of therapeuticprocess variables (Flückiger, Regli, Zwahlen, Hostettler, & Caspar,2010; Hilbert, Saelens, et al., 2007; Masheb & Grilo, 2008a).
Method
Participants
Participants met DSM-IV TR (American Psychiatric Association,APA, 2000) research criteria for BED, were between 18 and 70
years, had a BMI between 27 and 39 kg/m2 and participated ina randomized comparative trial to evaluate the efficacy of CBT andBWLT. Methods, design and treatment efficacy up to the 12-monthfollow-up assessment are fully reported in the main outcomereport (Munsch et al., 2007). Threehundred and seventy-five peoplewere recruited through newspaper advertisements and partici-pated in an initial telephone screening. Altogether 80 patients wereeligible for randomization andwere allocated to either CBTor BWLT(Fig.1). For a detailed description of the study sample refer toTable 1.Randomization was accomplished according to a permuted blockdesign (Kracht, 1992). Drop out rates during active treatment were27.5% (n ¼ 13) in CBT and 25.0% (n ¼ 9) in BWLT and did notsignificantly differ between treatment options. After treatment,another two (CBT) and four (BWLT) patients did no longer partici-pate in the follow-up booster sessions until 12-month follow-up.A final follow-up measurement took place on average 307.5 weeks(median ¼ 314.5, SD ¼ 46.9, MIN ¼ 217, MAX ¼ 373), i.e. c. 6 years,after the active treatment had ended. To this end, all patientsattending at least one session of active treatment were again con-tacted. Of the initial 44 patients allocated to the CBT condition andthe 36 patients allocated to the BWLTcondition, 26 (59%) in the CBT,and 26 (72%) in the BWLT took part in the 6-year follow-upassessments. Assessment of treatment efficacy at the end of activetreatment and at 6-year follow-up was based on reports of partici-pants who attended on average 13.3 (SD¼ 2.1), and 12.0 (SD ¼ 3.7),respectively, of the 16 treatment sessions.
Diagnostic assessment
At pretreatment, at the end of treatment, and at 12-monthfollow-up, BED diagnosis and its core symptomatology wereassessed according to the German version of the Eating DisorderExamination (Fairburn & Cooper, 1993a, 1993b; Hilbert, Tuschen-Caffier, & Ohms, 2004). At 6-year follow-up, due to the urge toreduce subject burden, we had to rely on the assessment of BEDsymptomatology using the questionnaire form of the EDE, theEating Disorder Examination, EDE-Q (Hilbert, Tuschen-Caffier,Karwautz, Niederhofer, & Munsch, 2007). The BED diagnosis wasconfirmed by telephone-based assessment of the BED researchcriteria of DSM-IV according to diagnostic interview (Diag-nostisches Interview zur Erfassung psychischer Störungen, DIPS)and interrater reliabilities were computed.
At pretreatment, mental disorders on axis I were assessed usingface-to-face diagnostic interviews for axes I (DIPS) and II (Struk-turiertes Klinisches Interview für DSM-IV, Achse-II, Persön-lichkeitsstörungen, SKID-II). At 6-year follow-up, mental disorderson axis I were re-evaluated according to the DIPS during telephoneinterviews. Telephone calls were tape-recorded and rated by twoindependent raters who were regularly supervised by the authors(SM and EB). For BED diagnosis (three categories: clinical,subclinical, none) percent agreement was 97.9% and interraterreliability (Cohen’s kappa) was 0.96 (n ¼ 48). For other mentaldisorders according to DIPS (coded y/n) percent agreement was100% and interrater reliability was 1.0 (n ¼ 49). Standardizedadministration of the interviews by master’s students of thedepartment at pretreatment and at 6-year follow-up was trainedand qualified during a two-days workshop and further ensured byweekly supervision by two of the authors (S.M. and E.B.).
German version by Hilbert & Tuschen-Caffier, 2006), which is theself-report version of the EDE, was administered repeatedly
Fig. 1. Participant-flow between pretreatment and 6-year follow-up for Cognitive-Behavioral Treatment and Behavioral Weight-Loss-Treatment.
S. Munsch et al. / Behaviour Research and Therapy 50 (2012) 775e785 777
S. Munsch et al. / Behaviour Research and Therapy 50 (2012) 775e785778
between pretreatment and 6-year follow-up to assess the numberof objective binge episodes (OBEs; i.e., binge eating defined as theconsumption of unusually large amounts of food with a subjectivesense of loss of control during the last 28 days), remission(proportion of patients not experiencing any OBEs), and the foursubscales restraint eating, eating concern, weight concern, andshape concern. A number of studies have demonstrated similarfindings for the EDE-Q and the EDE in describing eating disordersymptoms and changes in these symptoms over time (Mond, Hay,Rodgers, Owen, & Beumont, 2004; Sysko, Walsh, & Fairburn,2005). The EDE-Q has received empirical support for its use withpatients with BED (Grilo, Masheb, & Wilson, 2001a, 2001b). Goodtest-retest reliability has been reported (Hilbert, Tuschen-Caffier,et al., 2007; Reas, Grilo, & Masheb, 2006). In the current studyremission from binge eating was defined as having no objectivebinge episode during the last 28 days according to EDE-Q.
Patients also recorded their number of weekly binge eatingepisodes (self-reported weekly binge eating episodes; number of“episodes of overeating during which you felt out of control” duringthe past week) according to DSM-IV-TR criteria (Munsch et al.,2009) during the active treatment phase and at 6-year follow-up.
Body weightBody mass index, BMI, was measured by trained therapists or
co-therapists between pretreatment and 12-month follow-up. At 6-year follow-up BMI was self-reported by telephone and by mailing,with comparable BMI values between the two assessment methods(telephone: M ¼ 32.35, mailing: M ¼ 32.40, p ¼ 0.66; r ¼ 0.988,p < 0.001; n¼ 44). We therefore used the BMI as orally reported bytelephone for which the sample size was higher (n ¼ 52) than forthe mailed BMI (n ¼ 44). BMI change was documented using threecategories: more than 10% weight loss, between 5 and 10% weightloss, and less than 5% weight loss or weight gain betweenpretreatment and 6-year follow-up.
Negative affectParticipants completed the German version of the Beck
Depression Inventory (BDI, Hautzinger, Bailer, Worall, & Keller,1995). Following the suggestions of Wilson et al. (2010), we usedthe cut-off of 18 points and divided participants into a low anda high negative affect group.
Therapeutic process variables and contentment with therapyPatients completed the Bern post-session reports for patients,
short form 2000 (BPSR-P; Flückiger, Regli, et al., 2010), after eachtherapy session. The seven scales are based on general curativefactors proposed by Grawe (1997) and include global alliance,clarification and contentment with the bond. The scales have beenshown to have a satisfactory factor structure (Flückiger et al., 2011;Flückiger, Wüsten, Zinbarg, & Wampold, 2010).
At 6-year follow-up, contentment with therapy was measuredusing a self-developed questionnaire. Values were assessedaccording to a 7-point Likert scale ranging from�3 (not at all) toþ3(very much). The following seven questions were included in thequestionnaire: “I think, another therapeutic procedure would havebeen more appropriate for me”, “Are you satisfied with the treat-ment you received?”, “Would you again follow the treatment?”,“Would you recommend the treatment to another person?”, “Doyou think the treatment is credible?”, “Do you believe that treat-ment interventions are efficacious?”.
Treatments
The CBTmanual (Munsch, Biedert, & Schlup, 2011)was developedaccording to the treatment approach of Fairburn,Marcus, andWilson
(1993). The BWLT was based on a manualized treatment instructingpatients to achieve a regular, flexibly controlled and balancednutrition. Further, patients were encouraged to increase physicalactivity and to reduce eating without hunger (Margraf, 2000). Alto-gether seven CBT and six BWLT groups were carried through. Theactive treatment phase consisted of 16weekly 90-min group sessionsin each CBT and BWLT. During follow-up treatment six monthly 90-min group sessions were conducted. The last session took placetwelve months after the end of active treatment (see Munsch et al.,2007 for details about specific treatment contents).
At 12-month follow-up treatment suitability was high andpatients in CBT gave higher ratings than patients in BWLT. Assess-ment of treatment integrity revealed that raters identified 100% ofCBT and BWLT sessions correctly. Video tapes were classified intotreatment phases with a high accuracy. Interrater reliability wassatisfactory and overall ratings of therapeutic skills did not differbetween the two treatment conditions. For a detailed overview,refer to the outcome report of the 12-month follow-up (Munschet al., 2007).
Subcategorized predictors of treatment outcomeOvervaluation of shape and weight was defined according to
Masheb and Grilo (2008a) using the specific items from EDE(importance of shape: i.e. “Over the past 4 weeks has your shapeinfluenced how you feel about (judge, think, evaluate) yourself asa person?”; importance of weight: i.e. “Over the past 4 weeks hasyour weight influenced how you feel about (judge, think, evaluate)yourself as a person?”). Composite scores were built on the basis ofthe mean score at pretreatment and categorized as being above(clinical overvaluation) or below (subclinical) the clinical cut-off of4 (Fairburn & Cooper, 1993a, 1993b). Further individuals werecategorized into the rapid response to treatment subgroup accord-ing to Masheb and Grilo (2007) if they revealed a 65% or moredecrease in binge eating within the first four weeks. We used linearmixed models to estimate the decrease in binge eating (self-re-ported weekly binge eating episodes) within the first 4 weeks asthis allowed us to obtain reliable estimates also for patients withpartly missing values within that period. A further sub-categorization was made with respect to negative affect subtype,where individuals revealing a BDI above the 18 cut-off point wereconsidered to belong to the high negative affect subtype (Masheb &Grilo, 2008b; Wilson et al., 2010).
Statistical analysis
Primary outcomes included remission from binge eating, BED-diagnose, the number of self-reported weekly binge eatingepisodes, all EDE-subscales, and BMI. The only secondary outcomewas negative affect. There were four times points included in theanalysis: pretreatment, end of active treatment, 12-month follow-up, and 6-year follow-up. For specific characters like the numberof weekly binges thereweremore time points available which wereused to assess rapid responders. To analyze continuously distrib-uted outcomes we used linear mixed models (Fitzmaurice, Laird, &Ware, 2004; see also Schlup, Meyer, & Munsch, 2010). To analyzedichotomous outcomes we used generalized linear mixed modelsor, if fitting problems occurred because estimates were near 0 or 1,generalized linear models (Agresti, 2002).
Treatment efficacy was assessed either for both treatmentscombined or comparatively between treatments. For the combinedmodel explanatory variables were time (ln [weeks]) between end oftreatment and 6-year follow-up including a linear and a quadraticcomponent, the latter to account for nonlinear trajectories, and thepretreatment value of the outcome as covariate. For the compara-tive model we additionally included the factor treatment plus its
S. Munsch et al. / Behaviour Research and Therapy 50 (2012) 775e785 779
interaction with time components. Response variables weredifference scores between the outcome and its pretreatment value.
Predictors of treatment outcome included the followingpretreatment characteristics: (a) the temporal onset of binge eatingor dieting, (b) and (c) comorbidity with other mental disorders onaxis I and II, respectively (d) negative affect in terms of BDI � 18 ornot, (e) overvaluation of shape and weight, and (f) BMI. Predictorsassessed during active treatment included: (g) rapid response, and(h)e(j) the three therapeutic process variables global alliance,clarification, and contentment with the bond. Finally, we used (k)remission status at the end of treatment as sole post-treatmentpredictor. All predictors were tested for all nine primaryoutcomes. This resulted in a total of 86 analyses (11 predictors � 8outcomes minus 2 models not performed minus the 11 models forthe outcome BED diagnose, which were also not performed; seenotes in Table 5). The statistical model to analyze predictor effectsincluded the predictor, time (ln [weeks]) between end of treatmentand 6-year follow-up (linear and quadratic polynomial), and theinteraction between the two. We additionally included thepretreatment value of the outcome as covariate in the model as inrandomized controlled studies pretreatment outcomes are ex-pected to be equal on average among treatment groups andcontrolling for this covariate renders the analysis more efficient(Fitzmaurice et al., 2004). Further, adjusting for pretreatmentvalues of the outcome will also control for spurious correlationsbetween predictor and outcome (Cohen, 2003). We were particu-larly interested in the effect of the predictor on the outcome valuesat 6-year follow-up and hence point estimates for this specific timepoint are reported. Treatments were pooled for predictor analyses.
Effect sizes are based on descriptive statistics. Analyses wereperformed using PASW Statistics 18 (PASW Statistics, 2010) and R2.11 (R Development Core Team, 2010), including the R packagelme4 (Bates, Maechler, & Bolker, 2011) to analyze generalized linearmixed models.
Results
Information regarding the study sample and clinical character-istics at 6-year follow-up is shown in Tables 1 and 2, respectively. Atthe end of active treatment 2.1% (N¼ 48) of all participants revealeda BED diagnosis. The corresponding proportion at 6-year follow-upwas 7.7%. At 6-year-follow-up more than two thirds of participantsreported a regular intake of medicine, of which 39% were psycho-tropics. More than 30% indicated that they were seeking for
Table 1Sample description at pretreatment and 6-year follow-up for CBT and BWL treatments.
Patient characteristics Pretreatment
CBT B
Mean (SD) N M
Age, years 44.4 (11.5) 44 4BMI 33.1 (4.1) 43 3Self-reported onset of obesity, years 19.9 (12.7) 42 2Self-reported onset of BED, years 24.0 (13.2) 42 2ISEI 48.4 (9.6) 44 5Occurrence of self-reported binge first, % 28.6 42 2Occurrence of self-reported diet first, % 69.0 42 5Female sex, % 90.9 44 8Mental disorders, DSM-IV-TR: Comorbidity, % 40.9 44 4Anxiety disorders 29.5 3Affective disorders 9.1 1Somatoform disorders 2.3
Mental disorders on axis-II, % 11.4 44 1
Note. BMI values at 6-year follow-up are based on self-reported data. BDI, Beck Depressionin kilograms divided by height in meters squared); BWL, Behavioral Weight-Loss-TreatmOccupational Status (Ganzeboom, de Graaf, & Treiman, 1992).
additional psychological treatment after the end of treatment and23% reported to have undergone a diet to lose weight after treat-ment. Altogether 38% of all participants reported the experience ofa critical life event between end of treatment and 6-year follow-up.Contentment with therapy at the end of follow-up was 0.85 (�0.21,range: �3 to þ3) for both treatments combined and was signifi-cantly higher than the value 0 denoting neither contentment nordiscontentment (t(45) ¼ 4.00, p < 0.001). Values for CBT and BWLTwere 1.11 (�0.27) and 0.52 (�0.33), respectively, and were notsignificantly different from each other (t(44) ¼ 1.39, p ¼ 0.17).
The proportion of patients who were in the high negative affectcategory (BDI� 18) was 24% (N¼ 70) at pretreatment and 20% at 6-year follow-up. Finally, the proportion of patients who were in theclinical group with respect to overvaluation (values �4) was 38%(N ¼ 80) at pretreatment and 33% at 6-year follow-up.
Primary outcomes: treatment efficacy in terms of remission of bingeeating, eating disorder pathology and weight change
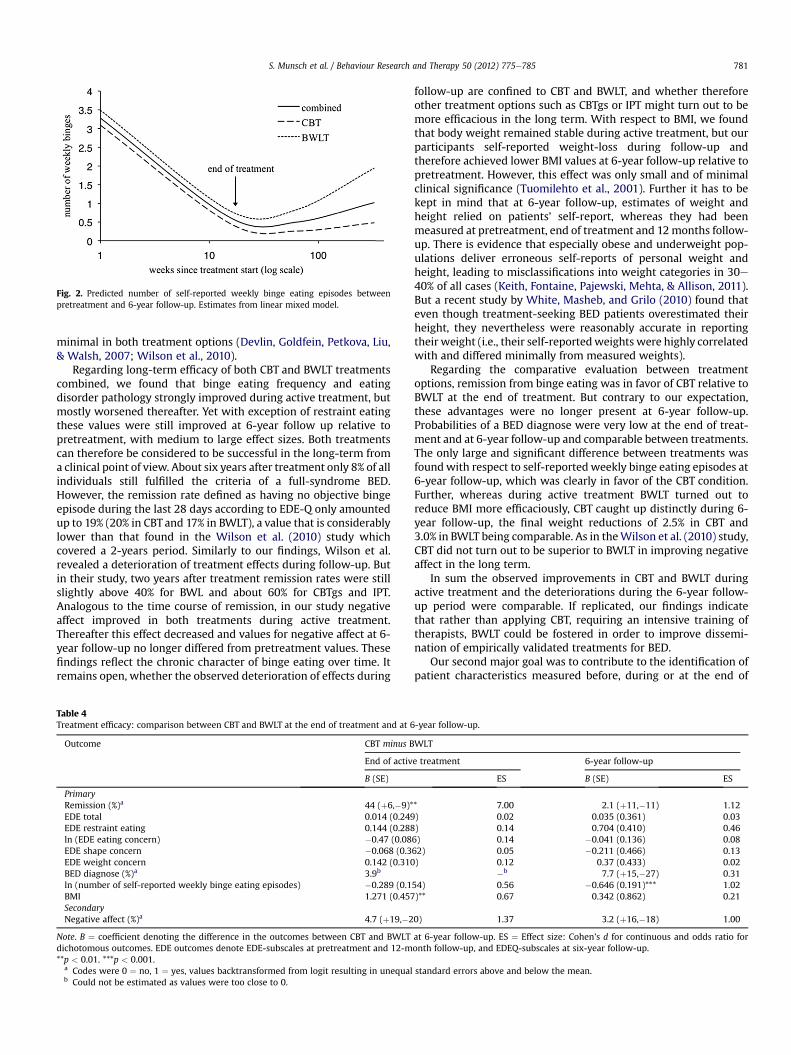
Results regarding treatment efficacy are summarized in Table 3.For treatment efficacy between end of active treatment and 6-yearfollow-up for both conditions combined, we obtained one majorpattern that was observed in most of the eating disorder pathologyoutcomes: remission of binge eating, BED diagnose, the number ofself-reported weekly binge eating episodes (see Fig. 2), and all EDE-subscales except restraint eating all significantly improved at theend of treatment relative to pretreatment but significantly wors-ened during follow-up. The values at 6-year follow-up werethereby still significantly improved relative to pretreatment andeffect sizes (Cohen, 1988) were medium to large (Table 3). The EDE-scale restraint eating showed a similar pattern, except that values at6-year follow-up did not differ from pretreatment values and theeffect size was very small. BMI was the only primary outcome forwhich estimates at the end of treatment did not significantly differfrom those at pretreatment but significantly improved duringfollow-up relative to end of treatment. BMI values at 6-year follow-up were improved relative to pretreatment though the effect sizewas small.
Looking at treatment comparisons, the probability of remissionwas significantly improved in CBT relative to BWLT at the end oftreatment but worsened more in CBT than BWLT during follow-upsuch that values at 6-year follow-up were comparable betweentreatments (Table 4). Estimates for BED diagnose and for all EDE-subscales were comparable between treatments at the end of
Inventory; BED, binge eating disorders; BMI, body mass index (calculated as weightent; CBT, Cognitive Behavior Therapy; ISEI: International Socio-Economic Index of
Table 2Clinical characteristics at 6-year follow-up for CBT and BWL treatments.
Patient characteristics CBT BWLT Total
% N % N % N
BED diagnosis, % 3.8 26 11.5 22 7.7 48Regular intake of medicine, % 74 19 67 15 71 34. of which psychotropics 43 14 33 9 39 23
Seeking additional psychological treatmentafter end of active therapy
31 26 31 26 31 52
Undergoing a diet to lose weight afteractive treatment
35 26 12 26 23 52
Reporting intake of weight-loss medications 0 19 0 15 0 34Critical life event between end of active
treatment and 6-year follow-up interms of .
44 16 31 13 38 29
physical problem/death 13 15 14loss of friend/living alone/marriage/lackof social support
S. Munsch et al. / Behaviour Research and Therapy 50 (2012) 775e785780
treatment and at 6-year follow-up. For self-reported weekly bingeeating episodes, estimates did not differ between treatments at theend of treatment but those in BWLT increased more than those inCBT during follow-up thereby reaching values at 6-year follow-upthat were significantly higher compared to CBT. Finally, BMI wassignificantly lower in BWLT relative to CBT at the end of treatment,but decreased more in CBT than BWLT during follow-up such thatthe values at 6-year follow-up were comparable between treat-ment options. Note that effect sizes regarding differences betweentreatments options at the end of treatment and at 6-year follow-upwere mostly small to very small (Table 4). Exceptions concernedremission, BMI, and the number of self-reported weekly bingeeating episodes at the end of treatment, where medium to higheffect sizes were observed, and the number of self-reported weeklybinge eating episodes at 6-year follow-up where the effect size waslarge.
Based on the mixed model for the outcome BMI and for bothtreatments combined, 17.9% (n ¼ 12) of all patients lost more than10% weight, 22.4% (n ¼ 15) lost between 5 and 10% weight, and59.7% (n ¼ 40) lost less than 5% or gained weight between
Table 3Treatment efficacy of both CBT and BWLT combined until 6-year follow-up.
Note. B ¼ coefficient denotes the difference in the outcomes between two time points ascolumn). ES ¼ Effect size: Cohen’s d based on descriptive values between pretreatment amonth follow-up, and EDEQ-subscales at six-year follow-up.*p < 0.05. **p < 0.01. ***p < 0.001.
a Codes were 0 ¼ no, 1 ¼ yes, values back-transformed from logit resulting in unequab must be significantly different from both 0 or 1 by definition.c For dichotomous outcomes no effect size could be computed as the reference was a
pretreatment and 6-year follow-up. Corresponding values for eachtreatment condition were 17.1% (n ¼ 6), 20.0% (n ¼ 7), and 62.9%(n¼ 22) for CBT, and 18.8% (n¼ 6), 25.0% (n¼ 8), and 56.3% (n¼ 18)for BWLT, and did not significantly vary between conditions(c2 ¼ 0.33, p ¼ 0.85).
Secondary outcome: treatment efficacy in terms of negative affect
Negative affect significantly improved during active treatment,nonsignificantly worsened during follow-up and finally reachedvalues at 6-year follow-up that no longer differed from pretreat-ment values (Table 3). The temporal course of negative affect wascomparable between the two treatment conditions and there wereno differences between CBT and BWLT at the end of treatment andat 6-year follow-up, the effect sizes being very small (Table 4).
Predictors of treatment outcome during follow-up
Results of predictor effects on outcomes at 6-year follow-up aresummarized in Table 5. Rapid response during the first four weeksof active treatment was predictive of five out of eight outcomes.Thus rapid responders had fewer self-reported weekly binge eatingepisodes, lower values for all EDE-subscales except for restrainteating, and lower BMI at 6-year follow-up. The effect sizes for theserelationships were mostly large (Table 5). All other predictors didnot affect outcomes at 6-year follow-up if adjusting error proba-bilities for multiple testing.
Discussion
The present study examines for the first time the efficacy ofa BWLT compared to a CBT program for BED patients in a controlledtreatment trial during a period of six years between end of activetreatment and end of follow-up. Based on previous findings(Munsch et al., 2007) and data from a large treatment trial onCBTgsh, BWL and IPT (Wilson et al., 2010) we expected CBT to bemore efficacious in terms of remission from binge eating and eatingdisorder pathology in the long term. We further hypothesized CBTto reveal a more favorable long-term effect on negative affect thanBWLT. Taking into account recent data about weight loss in BEDtreatment programs we expected change of body weight to be
p minust
6-year-follow-up minus pretreatment 6-year follow-up
indicated in the corresponding column head, or the 6-year follow-up value (far rightnd end-of follow-up. EDE outcomes denote EDE-subscales for pretreatment and 12-
l standard errors above and below the mean.
lways a constant (0 or 1).
Fig. 2. Predicted number of self-reported weekly binge eating episodes betweenpretreatment and 6-year follow-up. Estimates from linear mixed model.
S. Munsch et al. / Behaviour Research and Therapy 50 (2012) 775e785 781
minimal in both treatment options (Devlin, Goldfein, Petkova, Liu,& Walsh, 2007; Wilson et al., 2010).
Regarding long-term efficacy of both CBT and BWLT treatmentscombined, we found that binge eating frequency and eatingdisorder pathology strongly improved during active treatment, butmostly worsened thereafter. Yet with exception of restraint eatingthese values were still improved at 6-year follow up relative topretreatment, with medium to large effect sizes. Both treatmentscan therefore be considered to be successful in the long-term froma clinical point of view. About six years after treatment only 8% of allindividuals still fulfilled the criteria of a full-syndrome BED.However, the remission rate defined as having no objective bingeepisode during the last 28 days according to EDE-Q only amountedup to 19% (20% in CBT and 17% in BWLT), a value that is considerablylower than that found in the Wilson et al. (2010) study whichcovered a 2-years period. Similarly to our findings, Wilson et al.revealed a deterioration of treatment effects during follow-up. Butin their study, two years after treatment remission rates were stillslightly above 40% for BWL and about 60% for CBTgs and IPT.Analogous to the time course of remission, in our study negativeaffect improved in both treatments during active treatment.Thereafter this effect decreased and values for negative affect at 6-year follow-up no longer differed from pretreatment values. Thesefindings reflect the chronic character of binge eating over time. Itremains open, whether the observed deterioration of effects during
Table 4Treatment efficacy: comparison between CBT and BWLT at the end of treatment and at 6
Note. B ¼ coefficient denoting the difference in the outcomes between CBT and BWLTdichotomous outcomes. EDE outcomes denote EDE-subscales at pretreatment and 12-m**p < 0.01. ***p < 0.001.
a Codes were 0 ¼ no, 1 ¼ yes, values backtransformed from logit resulting in unequalb Could not be estimated as values were too close to 0.
follow-up are confined to CBT and BWLT, and whether thereforeother treatment options such as CBTgs or IPT might turn out to bemore efficacious in the long term. With respect to BMI, we foundthat body weight remained stable during active treatment, but ourparticipants self-reported weight-loss during follow-up andtherefore achieved lower BMI values at 6-year follow-up relative topretreatment. However, this effect was only small and of minimalclinical significance (Tuomilehto et al., 2001). Further it has to bekept in mind that at 6-year follow-up, estimates of weight andheight relied on patients’ self-report, whereas they had beenmeasured at pretreatment, end of treatment and 12months follow-up. There is evidence that especially obese and underweight pop-ulations deliver erroneous self-reports of personal weight andheight, leading to misclassifications into weight categories in 30e40% of all cases (Keith, Fontaine, Pajewski, Mehta, & Allison, 2011).But a recent study by White, Masheb, and Grilo (2010) found thateven though treatment-seeking BED patients overestimated theirheight, they nevertheless were reasonably accurate in reportingtheir weight (i.e., their self-reportedweights were highly correlatedwith and differed minimally from measured weights).
Regarding the comparative evaluation between treatmentoptions, remission from binge eating was in favor of CBT relative toBWLT at the end of treatment. But contrary to our expectation,these advantages were no longer present at 6-year follow-up.Probabilities of a BED diagnose were very low at the end of treat-ment and at 6-year follow-up and comparable between treatments.The only large and significant difference between treatments wasfoundwith respect to self-reportedweekly binge eating episodes at6-year follow-up, which was clearly in favor of the CBT condition.Further, whereas during active treatment BWLT turned out toreduce BMI more efficaciously, CBT caught up distinctly during 6-year follow-up, the final weight reductions of 2.5% in CBT and3.0% in BWLT being comparable. As in theWilson et al. (2010) study,CBT did not turn out to be superior to BWLT in improving negativeaffect in the long term.
In sum the observed improvements in CBT and BWLT duringactive treatment and the deteriorations during the 6-year follow-up period were comparable. If replicated, our findings indicatethat rather than applying CBT, requiring an intensive training oftherapists, BWLT could be fostered in order to improve dissemi-nation of empirically validated treatments for BED.
Our second major goal was to contribute to the identification ofpatient characteristics measured before, during or at the end of
Note. b¼ regression coefficient denoting the change in the outcome value at six-year follow-up for a one unit change in the predictor value. ES¼ Cohen’s d for continuous and odds ratio for dichotomous outcomes. EDE outcomesdenote EDE scales at pretreatment and one-year follow-up, and EDEQ scales at six-year follow-up. Significances are not adjusted/adjusted for multiple testing within each outcome across predictors using the Hochbergcorrection method (Hochberg, 1988). If not indicated, effects were neither significant for the unadjusted nor adjusted model at alpha ¼ 0.05.*p < 0.05. **p < 0.01. ***p < 0.001.
a The predictor BED diagnose could not be analyzed due to fitting problems. As these values were mostly very small during follow-up for both treatments, they are likely not to differ between treatments.b Not performed.c 1 ¼ yes, 2 ¼ no.d 0 ¼ yes, 1 ¼ no.
S.Munsch
etal./
BehaviourResearch
andTherapy
50(2012)
775e785
782
S. Munsch et al. / Behaviour Research and Therapy 50 (2012) 775e785 783
treatment allowing to predict the long term treatment success forspecific individuals. As in previous studies, rapid response, i.e.a strong decrease of symptomatology during the first four therapysessions, was the most important predictor of post-treatment(Grilo, Masheb, & Wilson, 2006; Masheb & Grilo, 2007; Safer &Joyce, 2011; Zunker et al., 2010) and 12-month follow-up (Griloet al., 2012) outcomes, with our study providing new findingsregarding the predictive significance of rapid response through 6-year follow-up.
This finding could be attributed to the application of treatmentstrategies such as homework assignment and self-monitoringusually introduced during early treatment phase in both treat-ments. These strategies are known to have alleviating effects onself-efficacy and depression. The importance of early self-efficacyexperiences was also shown in a previous study of our group,where process variables during early treatment phase turned out tobe predictive of dropouts later in therapy (Flückiger et al., 2011).From a clinical perspective this result implies the need of a repeatedassessment of patients during early CBT or BWLT treatment. Anearly detection of non-response in terms of the lack of a rapidimprovement from binge eating episodes allows the therapist toreact and administer additional interventions. Such strategiesmight include interventions focusing on the regulation of emotionsor impulses and on the training in interpersonal skills, tailored topatients’ individual needs. For further studies, it might be of interestto reevaluate the Masheb and Grilo (2008a) definition of rapidresponsewith respect to the time-span and the amount of symptomreduction in order to assess the generalizability of this conceptacross a broad range of study populations suffering from BED.
In our study predictor effects were controlled for pretreatmentvalues of the outcome, assuming that the predictor variable ofinterest is causally linked to the pretreatment value of the outcome.It nevertheless needs to be mentioned that if the predictor actuallyaffected the outcome from the beginning, i.e. patients withincreased values for a specific predictor had already higheroutcome values at pretreatment then adjusting for pretreatmentvalues of the outcome would be problematic as it would removepart of the predictor effect, thereby leading to biased predictoreffects (Miller & Chapman, 2001). In the present study, however,the predictive effect of rapid response remained more or less thesame when not adjusting for baseline outcomes.
Apart from rapid response, none of the other predictors, i.e.overvaluation of shape and weight, pretreatment BMI, comorbidityon axis I and II, and psychological process variables such as alliance,clarification and contentment with the bond affected treatmentoutcome at 6-year follow-up. These results are corroborating otherstudies who did not find a predictive effect of the before mentionedpatient characteristics (Wilfley et al., 2000). They are but partiallyin contrast to the study of Hilbert, Saelens, et al. (2007) andDingemans, Spinhoven, and van Furth (2007) who underlined therole of group cohesion and baseline palliative reacting as anunspecific factor for treatment efficacy after two years. Wheninterpreting these partially contradictory findings it must beconsidered that predictors may vary regarding the duration of theirinfluence: factors identified in studies covering a shorter time-spanmay not be predictive in the longer term, i.e. at 6 years follow-up asin the present study.
Our results are subject to several limitations. Most importantly,our study sample of 80 participants was relatively small and wasfurther reduced by 27% during treatment. At 6-year follow-up 65%of all initially participating patients again replied to our follow upinquiry. Participants and nonparticipants in the 6-year follow-upassessment did not differ significantly from each other in anyprimary outcome assessed at the end of active treatment and atone-year follow-up. Thus these 52 patients were likely to be
representative for our original sample of 80. A further limitationdeals with the assessment of objective bingeing according to EDEduring active treatment and 12 month follow-up and by ques-tionnaire (EDE-Q) at 6 year follow-up. The psychometric charac-teristics of the EDE-Q are critically discussed when it comes toassessing objective binge eating episodes (Striegel-Moore et al.,2010) even though Reas et al. (2006) found substantial reliabilityfor the EDE-Q in BED patients regarding the number of OBEs.
To summarize, in our study sample of BED patients the efficacyof CBT and BWLT at the end of active treatment underwenta considerable worsening during the 6-year follow-up course. Ifthese results are replicated, BED has to be considered an ongoingand severe mental condition, even if BED symptoms initiallyrespond well to interventions. Our findings regarding the comor-bidity rates at 6-year follow-up are more encouraging. Even thougha considerable proportion of patients continued to experiencebinge eating, only less than half of all patients still revealedcomorbid mental disorders.
Rapid response turned out to be the only stable predictor oflong-term outcome in our sample. In order to enhance earlytreatment response in a majority of BED patients, an importantfocus could lie on the evaluation of the individual’s self-regulatorycompetences as these might influence early treatment response(Aldao, Nolen-Hoeksema, & Schweizer, 2010; Heatherton &Wagner, 2011). Future studies should further not only investigatepredictors (as we did) but also moderators andmediators of changeof treatment in order to answer questions about efficacy mecha-nisms during BED treatment (Murphy, Cooper, Hollon, & Fairburn,2009). Another important issue for future research is the inclu-sion of subjective and objective binge episodes (SBE, OBE). Moredata about the transition of OBE into SBE after treatment trials isneeded, as a current study investigating the natural course of OBEand SBE in eating disorders could not corroborate the suggestedbinge drift from OBE toward SBE during treatment (Hildebrandt &Latner, 2006; Peterson et al., 2012).
In order to allow more fine grained but feasible research onpredictors of treatment effects future studies could fostera comprehensive assessment of treatment efficacy in the naturalenvironment, using electronic agendas including the role of familyatmosphere or dyadic emotion regulation as well as psychophysi-ological parameters such as stress reactivity.
References
Agras, W. S., Telch, C. F., Arnow, B., Eldredge, K., Detzer, M. J., Henderson, J., et al.(1995). Does interpersonal therapy help patients with binge eating disorderwho fail to respond to cognitive-behavioral therapy. Journal of Consulting andClinical Psychology, 63, 356e360. http://dx.doi.org/10.1037/0022-006X.63.3.356.
Agras, W. S., Telch, C. F., Arnow, B., Eldredge, K., & Marnell, M. (1997). One-yearfollow-up of cognitive-behavioral therapy for obese individuals with bingeeating disorder. Journal of Consulting and Clinical Psychology, 65, 343e347.http://dx.doi.org/10.1037/0022-006X.65.2.343.
Agresti, A. (2002). Categorical data analysis (2nd ed.). John Wiley & Sons.Aldao, A., Nolen-Hoeksema, S., & Schweizer, S. (2010). Emotion-regulation strate-
gies across psychopathology: a meta-analytic review. Clinical Psychology Review,30(2), 217e237.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mentaldisorders. Text revision (4th ed.). Washington, DC: American PsychiatricAssociation.
Bates, D., Maechler, M., & Bolker, B. (2011). lme4: Linear mixed-effects models using S4classes (Version R package version 0.999375-41). Vienna, Austria. Retrievedfrom. http://cran.r-project.org/web/packages/lme4/index.html.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Hillsdale, NJ:Erlbaum.
Cohen, J. (2003). Applied multiple regression/correlation analysis for the behavioralsciences, Vol. 1. Mahwah (N.J.): Lawrence Erlbaum.
Devlin, M. J., Goldfein, J. A., Petkova, E., Jiang, H., Raizman, P. S., Wolk, S., et al.(2005). Cognitive behavioral therapy and fluoxetine as adjuncts to groupbehavioral therapy for binge eating disorder. Obesity, 13(6), 1077e1088. http://dx.doi.org/10.1038/oby.2005.126.
S. Munsch et al. / Behaviour Research and Therapy 50 (2012) 775e785784
Devlin, M. J., Goldfein, J. A., Petkova, E., Liu, L., & Walsh, B. T. (2007). Cognitivebehavioral therapy and fluoxetine for binge eating disorder: two-year follow-up. Obesity, 15(7), 1702e1709. http://dx.doi.org/10.1038/oby.2007.203.
Dingemans, A. E., Spinhoven, P., & van Furth, E. F. (2007). Predictors and mediatorsof treatment outcome in patients with binge eating disorder. Behaviour Researchand Therapy, 45(11), 2551e2562. http://dx.doi.org/10.1016/j.brat.2007.06.003.
Eldredge, K. L., Agras, W. S., Arnow, B., Telch, C. F., Bell, S., Castonguay, L., et al.(1997). The effects of extending cognitive-behavioral therapy for binge eatingdisorder among initial treatment nonresponders. International Journal of EatingDisorders, 21, 347e352, pii:10.1002/(SICI)1098-108X(1997)21:4<347::AID-EAT7>3.0.CO;2-O.
Fairburn, C. G., & Cooper, Z. (1993a). The eating disorder examination [question-naire]. In C. G. Fairburn, & G. T. Wilson (Eds.), Binge eating: Nature, assessment,and treatment (pp. 317e360). New York, NY: Guilford, Retrieved from. http://webtools.klapp.no/data/kropp/vedlegg/387_EDE-Qvalidertversjonfebr2009(2).dat.pdf.
Fairburn, C. G., & Cooper, Z. (1993b). The eating disorder examination. In (12th ed.).In G. Wilson, & C. Fairburn (Eds.)., Binge eating: Nature, assessment, and treat-ment, Vol. xii (pp. 419) New York, NY, US: Guilford Press.
Fairburn, C. G., Marcus, M. D., & Wilson, G. T. (1993). Cognitive-behavioraltherapy for binge eating and bulimia nervosa: A comprehensive treatmentmanual. In C. G. Fairburn, & G. T. Wilson (Eds.), Binge Eating: Nature, Assessment,and Treatment (pp. 361e404). New York, NY: Guilford.
Fitzmaurice, G. M., Laird, N. M., & Ware, J. H. (2004). Applied longitudinal analysis.Hoboken NJ: Wiley.
Flückiger, C., Meyer, A. H., Wampold, B. E., Gassmann, D., Messerli-Bürgi, N., &Munsch, S. (2011). Predicting premature termination in a randomizedcontrolled trial for binge-eating patients. Behavior Therapy, . http://dx.doi.org/10.1016/j.beth.2011.03.008.
Flückiger, C., Regli, D., Zwahlen, D., Hostettler, S., & Caspar, F. (2010). Der BernerPatienten- und Therapeutenstundenbogen 2000 [Presentation report at the TheBern post-session reports for patients and therapists 2000]. Zeitschrift für Kli-nische Psychologie und Psychotherapie, 39(2), 71e79. http://dx.doi.org/10.1026/1616-3443/a000015.
Flückiger, C., Wüsten, G., Zinbarg, R. E., & Wampold, B. E. (2010). Resource activation:Using clients’ own strengths in psychotherapyand counseling. Hogrefe&Huber Pub.
Ganzeboom, H. B. G., de Graaf, P. M., & Treiman, D. J. (1992). A standard interna-tional socio-economic index of occupational status. Social Science Research, 21,1e56. http://dx.doi.org/10.1016/0049-089X(92)90017-B.
Grilo, C. M., Masheb, R. M., Brownell, K. D., Wilson, G. T., White, M. A. (2007).Randomized comparison of cognitive behavioral weight loss treatments for obesepatients with binge eating disorder: 12-month outcomes. Paper presented atWorldCongress of Behavioral and Cognitive Therapy; July 11, 2007; Barcelona, Spain.
Grilo, C. M., Masheb, R. M., & Wilson, G. T. (2001a). A comparison of differentmethods for assessing the features of eating disorders in patients with bingeeating disorder. Journal of Consulting and Clinical Psychology, 69(2), 317e322.http://dx.doi.org/10.1037//0022-006x.69.2.317.
Grilo, C. M., Masheb, R. M., & Wilson, G. T. (2001b). Different methods for assessingthe features of eating disorders in patients with binge eating disorder: a repli-cation. Obesity Research, 9(7), 418e422. http://dx.doi.org/10.1038/oby.2001.55.
Grilo, C. M., Masheb, R. M., & Wilson, G. T. (2006). Rapid response to treatment forbinge eating disorder. Journal of Consulting and Clinical Psychology, 74(3), 602e613. http://dx.doi.org/10.1037/0022-006X.74.3.602, pii:2006-08433-019.
Grilo, C. M., White, M. A., Wilson, G. T., Gueorguieva, R., & Masheb, R. M. (2012).Rapid response predicts 12-month post-treatment outcomes in binge-eatingdisorder: theoretical and clinical implications. Psychological Medicine, 42,807e817.
Hautzinger, M., Bailer, M., Worall, H., & Keller, F. (1995). Beck-Depressions-Inventar(BDI). Bern: Hans Huber.
Heatherton, T. F., & Wagner, D. D. (2011). Cognitive neuroscience of self-regulationfailure. Trends in Cognitive Sciences, 15(3), 132e139.
Hilbert, A., Bishop, M. E., Stein, R. I., Tanofsky-Kraff, M., Swenson, A. K., Welch, R. R.,et al. (2012). Long-term efficacy of psychological treatments for binge eatingdisorder. British Journal of Psychiatry, 200, 232e237.
Hilbert, A., Saelens, B. E., Stein, R. I., Mockus, D. S., Welch, R. R., Matt, G. E., et al.(2007). Pretreatment and process predictors of outcome in interpersonal andcognitive behavioral psychotherapy for binge eating disorder. Journal ofConsulting and Clinical Psychology, 75(4), 645e651. http://dx.doi.org/10.1037/0022-006X.75.4.645, pii:2007-11558-013.
Hilbert, A., & Tuschen-Caffier, B. (2006). Eating disorder examination-questionnaire.Deutsche Übersetzung Münster: Verlag für Psychotherapie.
Hilbert, A., Tuschen-Caffier, B., Karwautz, A., Niederhofer, H., & Munsch, S. (2007).Eating disorder examination-questionnaire. Evaluation der deutschsprachigenÜbersetzung. Diagnostica, 53(3), 144e154. http://dx.doi.org/10.1026/0012-1924.53.3.144.
Hilbert, A., Tuschen-Caffier, B., & Ohms, M. (2004). Eating disorder examination:Deutschsprachige Version des strukturierten Essstörungsinterviews. Diag-nostica, 50(2), 98e106. http://dx.doi.org/10.1026/0012-1924.50.2.98.
Hildebrandt, T., & Latner, J. D. (2006). Effect of self-monitoring on binge eating:treatment response or “binge drift”? European Eating Disorders Review, 14, 16e22.
Hochberg, Y. (1988). A sharper Bonferroni procedure for multiple tests of signifi-cance. Biometrika, 75, 800e803.
Hudson, J. I.,Hiripi, E., Pope,H.G., Jr.,&Kessler, R. C. (2007). Theprevalenceandcorrelatesof eating disorders in the national comorbidity survey replication. BiologicalPsychiatry, 61(3), 348e358. http://dx.doi.org/10.1016/j.biopsych.2006.03.040.
Keith, S. W., Fontaine, K. R., Pajewski, N. M., Mehta, T., & Allison, D. B. (2011). Use ofself-reported height and weight biases the body mass index-mortality associ-ation. International Journal of Obesity (London), 35(3), 401e408. http://dx.doi.org/10.1038/ijo.2010.148.
Kracht, M. (1992). Randomisierung. In J. Adam (Ed.), Statistisches know how in dermedizinischen Forschung (pp. 172e210). Berlin: Ullstein Mosby GmbH.
Kraemer, H. C., Wilson, G. T., Fairburn, C. G., & Agras, W. S. (2002). Mediators andmoderators of treatment effects in randomized clinical trials. Archives of GeneralPsychiatry, 59(10), 877e883, pii:ynv10179.
Margraf, J. (2000). Aus dick wird nicht dünn. Falsche Erwartungshaltungen. InE. Roche (Ed.), In Hülle und Fülle. Dem Fett auf den Leib gerückt (pp. 43e54).Basel: Hoffmann-La Roche.
Masheb, R. M., & Grilo, C. M. (2007). Rapid response predicts treatment outcomes inbinge eating disorder: implications for stepped care. Journal of Consulting andClinical Psychology, 75(4), 639e644. http://dx.doi.org/10.1037/0022-006X.75.4.639, pii:2007-11558-012.
Masheb, R. M., & Grilo, C. M. (2008a). Prognostic significance of two sub-categorization methods for the treatment of binge eating disorder: negativeaffect and overvaluation predict, but do not moderate, specific outcomes.Behaviour Research and Therapy, 46(4), 428e437. http://dx.doi.org/10.1016/j.brat.2008.01.004, pii:S0005-7967(08)00007-7.
Masheb, R.M., & Grilo, C.M. (2008b). Examination of predictors andmoderators for self-help treatmentsofbinge-eatingdisorder. Journal of ConsultingandClinical Psychology,76(5), 900e904. http://dx.doi.org/10.1037/a0012917, pii:2008-13625-019.
Miller, G. A., & Chapman, J. P. (2001). Misunderstanding analysis of covariance.Journal of Abnormal Psychology, 110(1), 40e48. http://dx.doi.org/10.1037/0021-843X.110.1.40.
Mond, J. M., Hay, P. J., Rodgers, B., Owen, C., & Beumont, P. J. (2004). Temporalstability of the eating disorder examination questionnaire. International Journalof Eating Disorders, 36(2), 195e203. http://dx.doi.org/10.1002/eat.20017.
Munsch, S., Biedert, E., Meyer, A., Michael, T., Schlup, B., Tuch, A., et al. (2007).A randomized comparison of cognitive behavioral therapy and behavioral weightloss treatment foroverweight individualswithbingeeatingdisorder. InternationalJournal of Eating Disorders, 40(2), 102e113. http://dx.doi.org/10.1002/eat.20350.
Munsch, S., Biedert, E., & Schlup, B. (2011). Kognitive Verhaltenstherapie bei bingeeating disorder (2nd rev. ed.). Weinheim: Beltz PVU.
Munsch, S., Meyer, A. H., Milenkovic, N., Schlup, B., Margraf, J., & Wilhelm, F. H.(2009). Ecological momentary assessment to evaluate cognitive-behavioraltreatment for binge eating disorder. International Journal of Eating Disorders,42(7), 648e657. http://dx.doi.org/10.1002/eat.20657.
Murphy, R., Cooper, Z., Hollon, S. D., & Fairburn, C. G. (2009). How do psychologicaltreatments work? Investigating mediators of change. Behaviour Research andTherapy, 47(1), 1e5. http://dx.doi.org/10.1016/j.brat.2008.10.001, pii:S0005-7967(08)00204-0.
PASW Statistics (Version 18). (2010). Chicago: SPSS Inc.Peterson, C. B., Swanson, S. A., Crow, S. J., Mitchell, J. E., Agras, S. W., Halmi, K. A.,
et al. (2012). Longitudinal stability of binge-eating type in eating disorders.International Journal of Eating Disorders, 45(5), 664e669. http://dx.doi.org/10.1002/eat.22008.
R Development Core Team, R. D. C. (2010). R: A language and environment forstatistical computing. Vienna, Austria: R Foundation for Statistical Computing.
Reas, D. L., Grilo, C. M., & Masheb, R. M. (2006). Reliability of the eating disorderexamination-questionnaire in patients with binge eating disorder. BehaviourResearch and Therapy, 44(1), 43e51. http://dx.doi.org/10.1016/j.brat.2005.01.004.
Safer, D. L., & Joyce, E. E. (2011). Does rapid response to two group psychotherapies forbinge eating disorder predict abstinence? Behaviour Research and Therapy, 49(5),339e345. http://dx.doi.org/10.1016/j.brat.2011.03.001, pii:S0005-7967(11)00060-X.
Schlup, B., Meyer, A. H., & Munsch, S. (2010). A non-randomized direct comparison ofcognitive-behavioral short- and long-term treatment for binge eating disorder.Obesity Facts, 3(4), 261e266. http://dx.doi.org/10.1159/000319538, pii:000319538.
Striegel-Moore, R. H., Cachelin, F. M., Dohm, F. A., Pike, K. M., Wilfley, D. E., &Fairburn, C. G. (2001). Comparison of binge eating disorder and bulimia nervosain a community sample. International Journal of Eating Disorders, 29(2), 157e165, pii:10.1002/1098-108X(200103)29:2<157::AID-EAT1005>3.0.CO;2-8.
Striegel-Moore, R., & Franko, D. (2008). Should binge eating disorder be included in theDSM-V? A critical review of the state of evidence. Annual Review of ClinicalPsychology, 4, 305e324. http://dx.doi.org/10.1146/annurev.clinpsy.4.022007.141149.
Striegel-Moore, R. H., Wilson, G. T., DeBar, L., Perrin, N., Lynch, F., Rosselli, F., et al.(2010). Cognitive behavioral guided self-help for the treatment of recurrentbinge eating. Journal of Consulting and Clinical Psychology, 78(3), 312. http://dx.doi.org/10.1037/a0018915.
Sysko, R., Walsh, B. T., & Fairburn, C. G. (2005). Eating disorder examination-questionnaire as a measure of change in patients with bulimia nervosa. Inter-national Journal of Eating Disorders, 37(2), 100e106. http://dx.doi.org/10.1002/eat.20078.
Telch, C. F., Agras, W. S., Rossiter, E. M., Wilfley, D., & Kenardy, J. (1990). Groupcognitive-behavioral treatment for the nonpurging bulimic: an initial evalua-tion. Journal of Consulting and Clinical Psychology, 58, 629e635. http://dx.doi.org/10.1037/0022-006X.58.5.629.
Tuomilehto, J., Lindström, J., Eriksson, J. G., Valle, T. T., Hämäläinen, H., Ilanne-Parikka, P., et al. (2001). Prevention of type 2 diabetes mellitus by changes inlifestyle among subjects with impaired glucose tolerance. New England Journal
S. Munsch et al. / Behaviour Research and Therapy 50 (2012) 775e785 785
of Medicine, 344(18), 1343e1350, Retrieved from. http://www.nejm.org/doi/pdf/10.1056/NEJM200105033441801.
Vocks, S., Tuschen-Caffier, B., Pietrowsky, R. K., Rustenbach, S. J., Kersting, A., &Herpertz, S. (2010). Meta-analysis of the effectiveness of psychological andpharmacological treatments for binge eating disorder. International Journal ofEating Disorders, 43(3), 205e217. http://dx.doi.org/10.1002/eat.20696.
White, M. A., Masheb, R. M., & Grilo, C. M. (2010). Accuracy of self-reported weightand height in binge eating disorder: misreport is not related to psychologicalfactors. Obesity, 18, 1266e1269.
Wilfley, D., Friedman, M., Dounchis, J., Stein, R., Welch, R., & Ball, S. (2000).Comorbid psychopathology in binge eating disorder: relation to eating disorderseverity at baseline and following treatment. Journal of Consulting and ClinicalPsychology, 68(4), 641e649. http://dx.doi.org/10.1037/0022-006X.68.4.641.
Wilfley, D. E., Welch, R. R., Stein, R. I., Spurrell, E. B., Cohen, L. R., Saelens, B. E., et al.(2002). A randomized comparison of group cognitive-behavioral therapy andgroup interpersonal psychotherapy for the treatment of overweight individuals
with binge-eating disorder. Archives of General Psychiatry, 59, 713e721,Retrieved from. http://archpsyc.ama-assn.org/cgi/reprint/59/8/713.pdf.
Wilson, G. T., Grilo, C. M., & Vitousek, K. M. (2007). Psychological treatment of eatingdisorders. The American Psychologist, 62(3), 199e216. http://dx.doi.org/10.1037/0003-066X.62.3.199, pii:2007-04834-006.
Wilson, G. T., Wilfley, D. E., Agras, W. S., & Bryson, S. W. (2010). Psychologicaltreatments of binge eating disorder. Archives of General Psychiatry, 67(1), 94e101. http://dx.doi.org/10.1001/archgenpsychiatry.2009.170, pii:67/1/94.
Yager, J. (2008). Binge eating disorder: the search for better treatments. AmericanJournal of Psychiatry,165(1), 4e6. http://dx.doi.org/10.1176/appi.ajp.2007.07101541,pii:165/1/4.
Zunker, C., Peterson, C. B., Cao, L., Mitchell, J. E., Wonderlich, S. A., Crow, S., et al.(2010). A receiver operator characteristics analysis of treatment outcome inbinge eating disorder to identify patterns of rapid response. Behaviour Researchand Therapy, 48(12), 1227e1231. http://dx.doi.org/10.1016/j.brat.2010.08.00, pii:S0005-7967(10)00181-6.