36
Efficacy of exogenous Growth hormon (GH) treatment in children with growth hormon deficiency (GHD) in Children Hospital 1 MD.Trần Thị Bích Huyền Children hospital 1 Endocrine department
| Date post: | 01-Jan-2016 |
| Category: |
Documents |
| Upload: | abraham-hall |
| View: | 228 times |
| Download: | 2 times |
Efficacy of exogenous Growth hormon (GH)
treatment in children with growth hormon
deficiency (GHD) in Children Hospital 1
MD.Trần Thị Bích Huyền
Children hospital 1
Endocrine department
Growth hormon (GH): secreted by anterior pituitary lobe,
stimulates cartilage growth.
GH deficiency (GHD) causes growth failure in children.
The etiology of GHD may be congenital or acquired.
Incidence of short stature associated GHD : 1/3500-4000
1. Introduction

In the world: GH has been available for management of short
stature associated GHD from 1985 ..
In1921: initial therapy with bovine GHnot efficiency.
1985: Recombinant DNA-derived human GH (hGH) has been
available.
1. Introduction
Vietnam: limitation in diagnosis and treatment GHD
(laboratory, drugs)
2010 : diagnostic approach to short stature and started to use
exogenous GH for GHD in Children hospital.
We report the efficacy of GH therapy in 7 patients with GHD in
my hospital.
1. Introduction

2. Background

Growth failure: defined as height velocity less than 2 SD
below the mean for age ( corresponds to approximately <
3rd percentile.
Definition

Aetiology of GHD
Congenital forms
Acquired forms
Tumours or defects of hypothalamus
Pituitary: tumours, trauma, central nervous system
disease, infections, late effects of cancer therapy ...

Diagnostic approach to Short stature
Clinical and auxological assessment Baseline Investigations:
Bone age
Karyotype
Systemic screen FBC, EUC, TSH, T4, Ca, Phos, urinalysis IGF-1, GH, LH, FSH, Testosterone/Estrogen
Subsequent Investigations:
GH stimulation tests
Imaging studies as indicated (MRI)

Stimulation testing
Clonidine, Arginine, Insulin, Glucagon, Levodopa, GHRH,
exercise test.
Diagnosis of GHD: 2 stimulation tests
Children hospital 1: Insulin and exercise test

Peak GH > 20mU/l (10ng/ml): normal
Peak GH: 10-20mU/l (5-10ng/ml): partial GH deficiency
Peak GH< 10mU/l (5ng/ml): GH deficiency
Stimulation testing

Definition of Biochemical GH deficiencyPeak GH cut off for diagnosis of GHD
mU/L No of provocative tests
Australia 10 2
UK (Kirk 2006) <20 1 or 2
USA <30
New Zealand <20
Germany <30 2 (1 with low IGF-1 or IGFBP-3)
France <30 2
Netherlands <30 2
Spain <30 2
Sweden <24
Canada <24 2
Israel <24 2
Japan(<2005) <30 2
Japan(>2005)* <18 2
Taiwan <30 2
Indications for GH treatment in CH 1:
GHD
Turner syndrome
Somatropin (Growth hormon: 0,2-0,3 mg/kg/ week)
Follow up
Management
Side effects Plotting on growth charts and monitoring growth rate over a 3 to
6 month period Reassessment : IGF-1, bone age every 6-12 month period
GH side effects
Uncommon overall
Benign intracranial hypertension (1 in 1000)
Slipped capital femoral epiphyses
Odema
Risk of diabetes
Progression of scoliosis
Cancer
3. Outcome

No Gender Age
1 M 10
2 M 9,5
3 F 4,5
4 M 5
5 M 11,5
6 M 12
7 F 12
Characteristics of the population
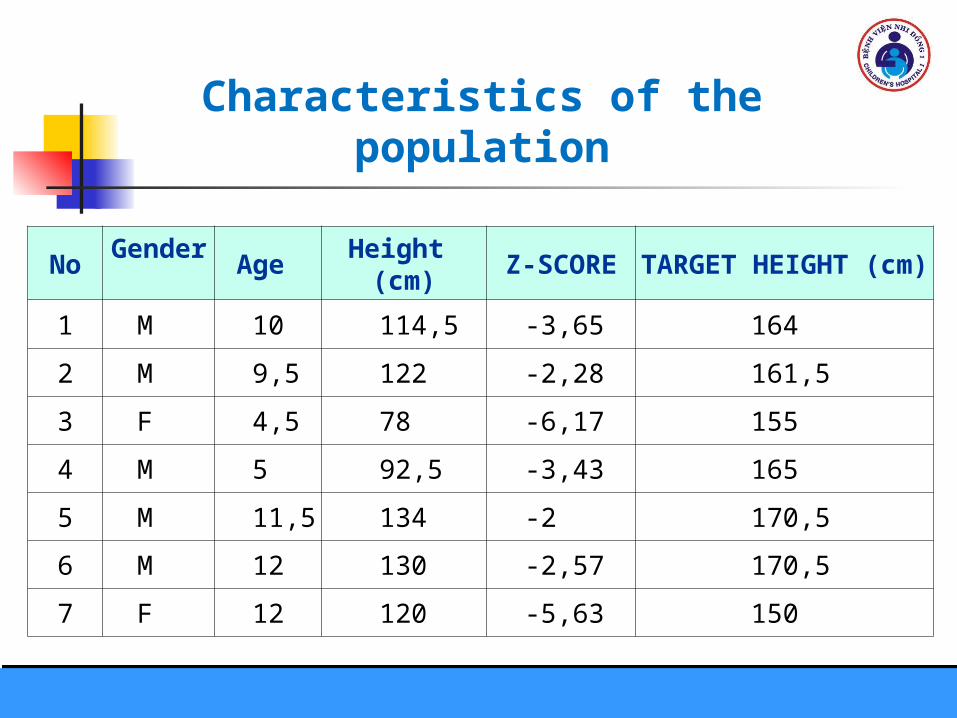
NoGender
Age Height (cm) Z-SCORE TARGET HEIGHT (cm)
1 M 10 114,5 -3,65 164
2 M 9,5 122 -2,28 161,5
3 F 4,5 78 -6,17 155
4 M 5 92,5 -3,43 165
5 M 11,5 134 -2 170,5
6 M 12 130 -2,57 170,5
7 F 12 120 -5,63 150
Characteristics of the population

Boys Height

Girls height

NoGender
Age Weight (Kg) BMI Z-SCORE
1 M 10 25 19,1 1,24
2 M 9,5 25,5 17,1 0,45
3 F 4,5 13 21,4 3,26
4 M 5 13 15,2 -0,02
5 M 11,5 30 16,7 -0,35
6 M 12 30 17,8 0,16
7 F 12 26 18,1 -0,55
Characteristics of the population

No Gender Age Bone age KARYOTYPE
1 M 10 7-8
2 M 9,5 8
3 F 4,5 1,5 46XX
4 M 5 2,5
5 M 11,5 6
6 M 12 9-10
7 F 12 7 46XX
Characteristics of the population

No Gender Age IGF1 (ng/ml) GH (ng/ml)
1 M 10 194 0,12
2 M 9,5 174 0,04
3 F 4,5 176 0,45
4 M 5 172 3,03
5 M 11,5 214 0,61
6 M 12 120 0,48
7 F 12 182 0,0
Characteristics of the population

NoTSH
(uIU/ml)FT4
(ng/dl)Cortisol(g/dl)
1 1,3 1,68 8,25
2 1,39 1,57 14,7
3 4,65 0,86 15,15
4 3,13 1,72 8,97
5 3,67 1,19 8,87
6 3,52 0,96 8,9
7 4,53 0,83 6,8
Screening tests: FBC, EUC, Ca, Phos, urinalysis: normal
Characteristics of the population
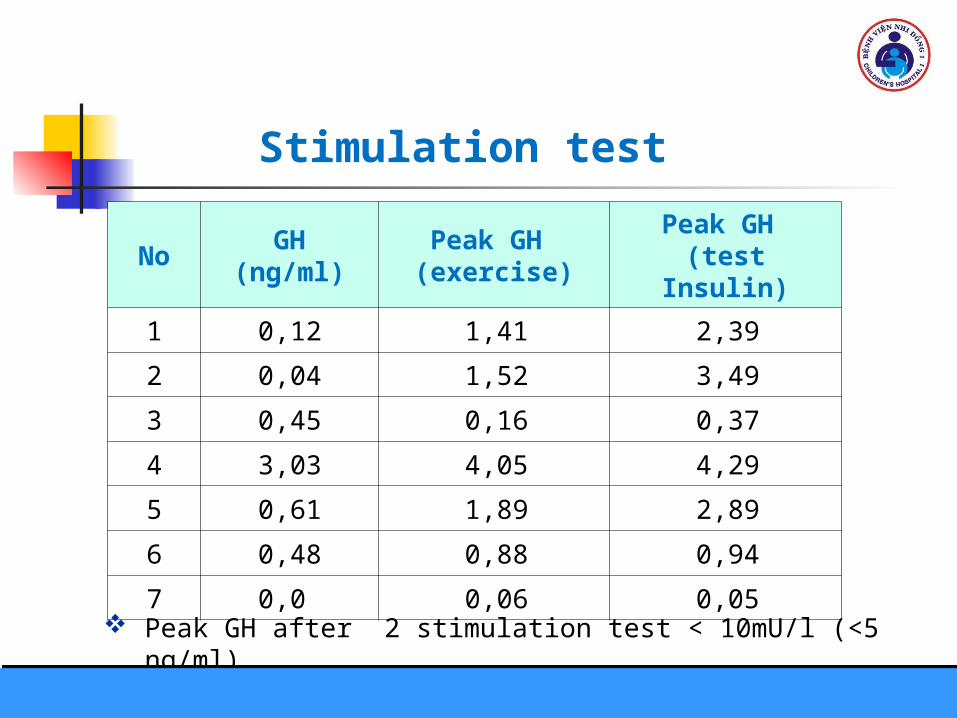
NoGH
(ng/ml)Peak GH (exercise)
Peak GH (test Insulin)
1 0,12 1,41 2,39
2 0,04 1,52 3,49
3 0,45 0,16 0,37
4 3,03 4,05 4,29
5 0,61 1,89 2,89
6 0,48 0,88 0,94
7 0,0 0,06 0,05
Stimulation test
Peak GH after 2 stimulation test < 10mU/l (<5 ng/ml)
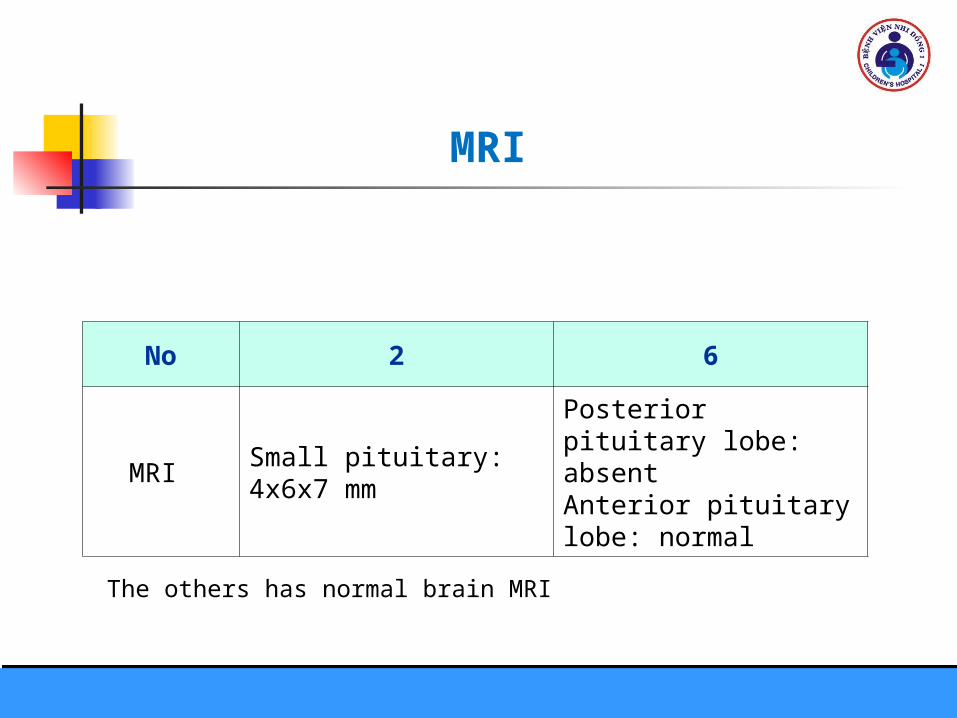
No 2 6
MRI Small pituitary: 4x6x7 mm
Posterior pituitary lobe: absentAnterior pituitary lobe: normal
MRI
The others has normal brain MRI

Outcome of therapy
STTDose of GH(mg/Kg/day)
Time (month)
Height (before) (cm)
Height (after) (cm)
∆H(cm)∆H
/month
1 0.04 13 114,5 126 11,5 0,88
2 0,03 4 122 125 3 0.75
3 0,04 14 78 101 23 1.64
4 0,04 3.5 92,5 96 3.5 1.00
5 0,035 9.5 134 144 10 1.05
6 0,035 24 130 146,5 16.5 0.69
7 0,04 5 120 125 5 1.00

Patient 1
TARGET HEIGHT (164cm)

Patient 2
TARGET HEIGHT (161,5cm)
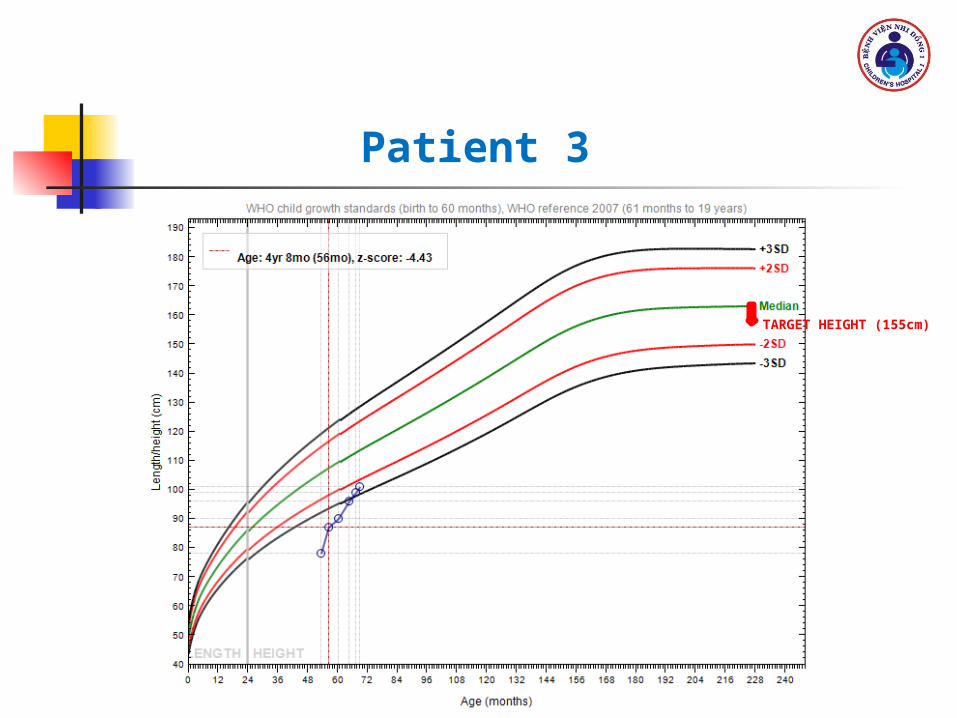
Patient 3
TARGET HEIGHT (155cm)
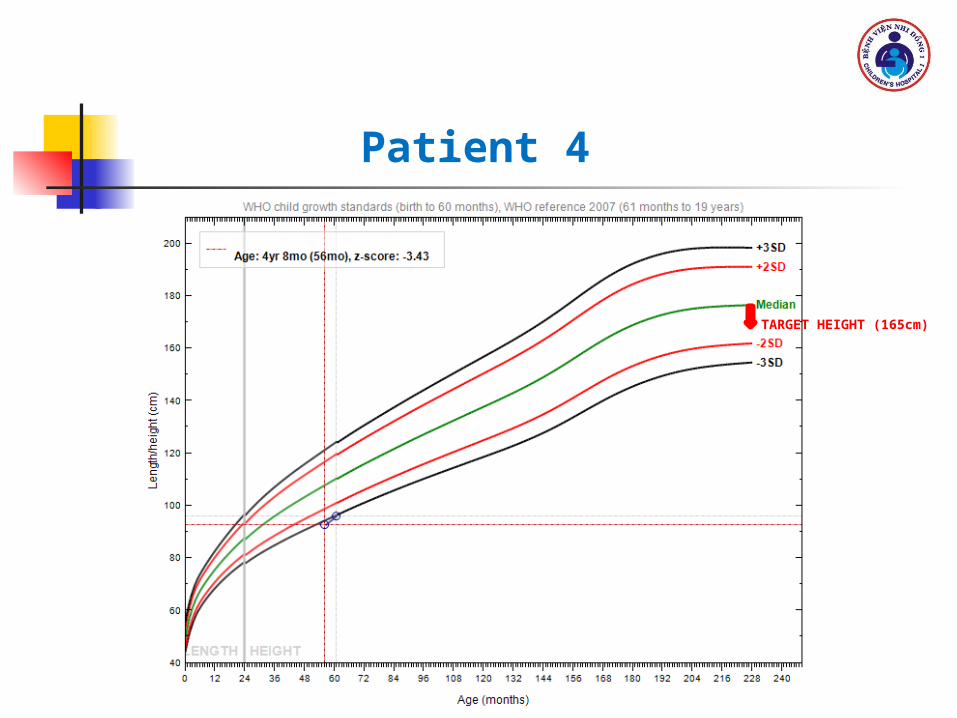
Patient 4
TARGET HEIGHT (165cm)

Patient 5
TARGET HEIGHT (170,5cm)
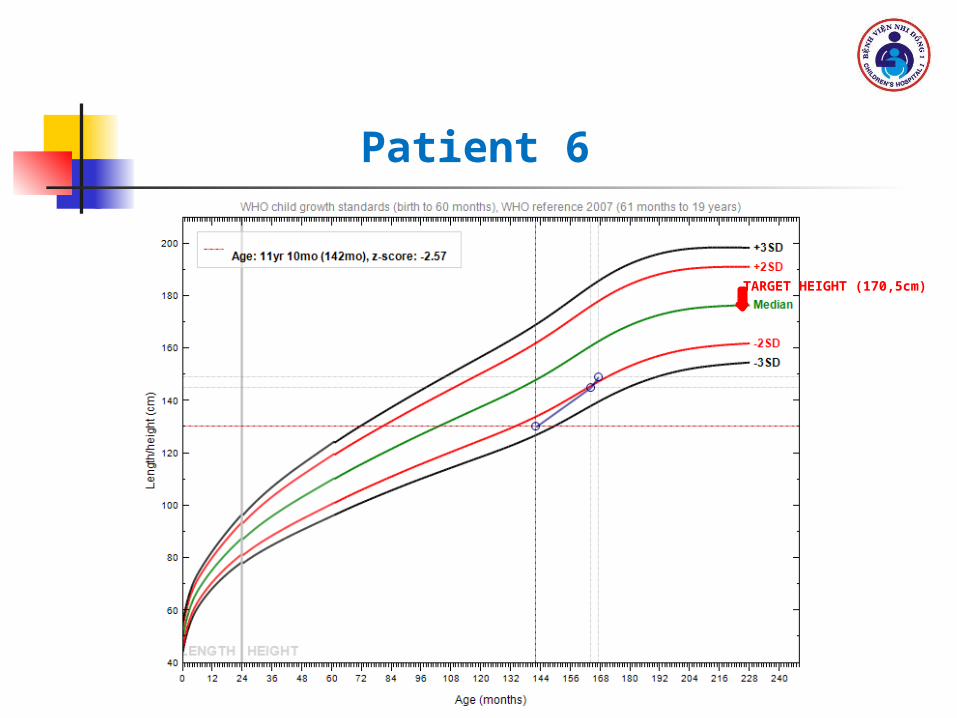
Patient 6
TARGET HEIGHT (170,5cm)

Patient 7
TARGET HEIGHT (150cm)
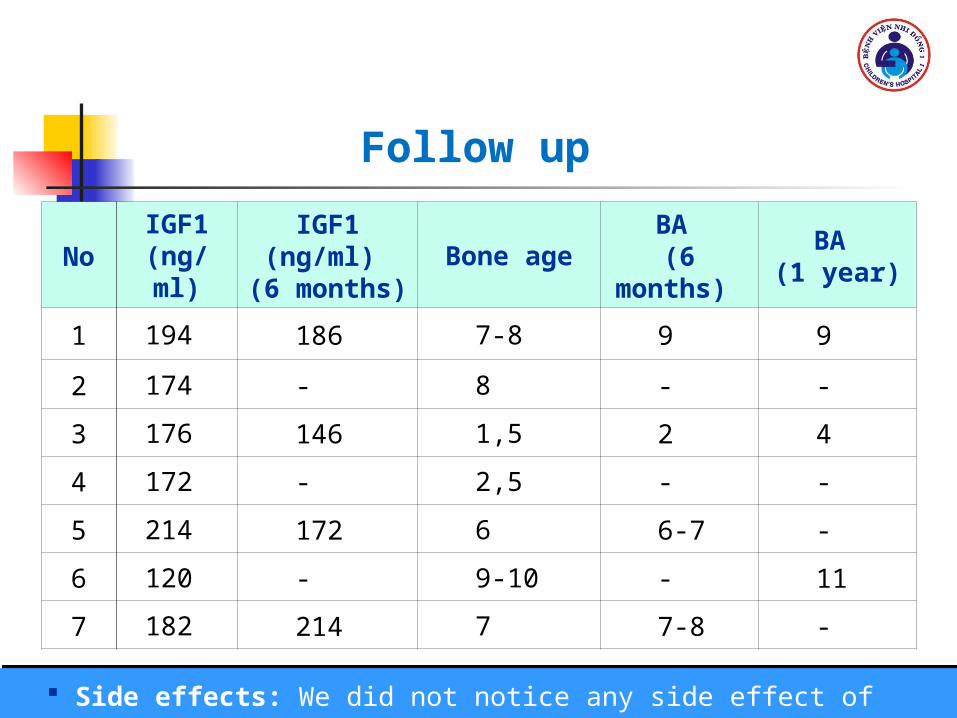
NoIGF1
(ng/ml)IGF1 (ng/ml) (6 months)
Bone ageBA
(6 months) BA
(1 year)
1 194 186 7-8 9 9
2 174 - 8 - -
3 176 146 1,5 2 4
4 172 - 2,5 - -
5 214 172 6 6-7 -
6 120 - 9-10 - 11
7 182 214 7 7-8 -
Follow up
Side effects: We did not notice any side effect of GH in all cases

All patients were diagnosed and started to treat with GH at
mean age 9,5 years.
Height of cases less than 3 SD below the mean for age before
treatment .
There was a clear improvement of height in all patients and
the mean of height velocity was 1cm/month in the first year .
We did not notice any side effect of GH in all cases.
Conclusion

Recommendations
Assessment of growth over time is an essential aspect of child health
care
More Scientific studies about GH treatment in Vietnam
Medical insurance

Thank you




![[Cv presentation][hồ thị bích huyền]](https://static.documents.pub/doc/80x56/55985b551a28ab65768b4693/cv-presentationho-thi-bich-huyen.jpg)












