91
Ekarat Rattarittamrong, MD Division of Hematology Department of Internal Medicine Faculty of Medicine Chiang Mai University

Ekarat Rattarittamrong, MD Division of Hematology
Department of Internal Medicine Faculty of Medicine
Chiang Mai University

Multiple myeloma (MM) Systemic AL amyloidosis Monoclonal gammopathy of renal
significance (MGRS) POEMS syndrome

Multiple myeloma (MM) Systemic AL amyloidosis Monoclonal gammopathy of renal
significance (MGRS) POEMS syndrome

Clonal plasma cell disorder with evidence of specific end-organ damage
HyperCalcemia Renal failure Anemia Bone lesions
Rajkumar SV. Am J Hematol 2016;91:90–100.
CRAB features

Palumbo A. N Engl J Med 2011;364:1046-60.
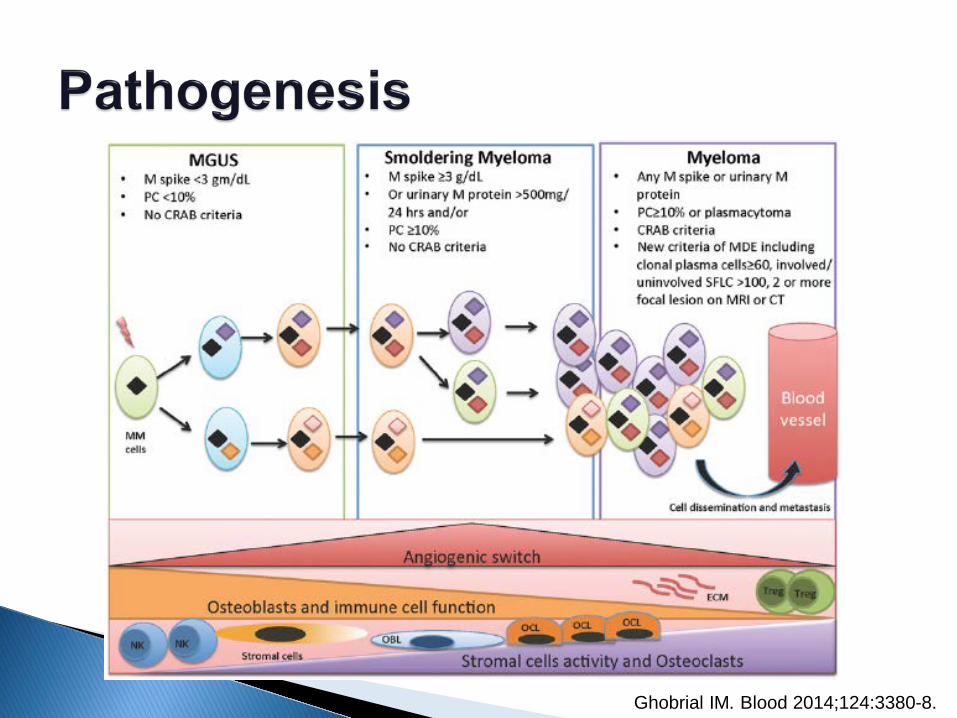
Ghobrial IM. Blood 2014;124:3380-8.

Palumbo A. N Engl J Med 2011;364:1046-60.

Clonal BM plasma cells ≥10% or plasmacytoma and any one or more of the following myeloma defining events (MDE):
Rajkumar SV. Lancet Oncol 2014;15:e538–48.
Evidence of end organ damage: Hypercalcemia: serum calcium > 1 mg/dL higher than UNL or > 11 mg/dL Renal insufficiency: CrCl < 40 mL/min or Cr > 2 mg/dL Anemia: Hb > 2 g/dL below LNL or < 10 g/dL Bone lesions: one or more osteolytic lesions on skeletal radiography, CT, or PET-CT
Biomarkers of malignancy: Clonal bone marrow plasma cell percentage ≥ 60% Involved : uninvolved serum free light chain ratio ≥ 100 > 1 focal lesions on MRI studies

BM plasma cells Abnormal FLC ratio
Kastritis E. Leukemia 2013;27:947–53.

Hillengass J. Leuk Lymphoma 2013;54:1355–63.

Not reached 13 months
Hillengass J. J Clin Oncol 2010;28:1606–10.

Monoclonal gammopathy of undetermined significance (MGUS) ◦ Serum monoclonal protein < 30 g/L or abnormal free light
chain ratio ◦ Clonal bone marrow plasma cells < 10% ◦ Absence of end-organ damage (CRAB) or amyloidosis
that can be attributed to the plasma cell proliferative disorder
Progression to MM, solitary plasmacytoma, or light chain amyloidosis 1% per year
Rajkumar SV. Lancet Oncol 2014;15:e538–48.

Go RS. Blood 2018;131:163-73.

Kyle RA. N Engl J Med 2018;378:241-9.

Go RS. Blood 2018;131:163-73.

Go RS. Blood 2018;131:163-73.

Go RS. Blood 2018;131:163-73.

Go RS. Blood 2018;131:163-73.

Go RS. Blood 2018;131:163-73.

Smoldering multiple myeloma Intermediate clinical stage between MGUS and MM ◦ Serum monoclonal protein > 30 g/L and/or clonal bone
marrow plasma cells 10-60% ◦ Absence of end organ damage ◦ No myeloma-defining biomarkers
Risk of progression to malignant disease 10% per year in the first 5 years
Rajkumar SV. Lancet Oncol 2014;15:e538–48.

Ghobrial IM. Blood 2014;124:3380-8.

Solitary plasmacytoma ◦ Biopsy-proven solitary lesion of bone or soft tissue
with evidence of clonal plasma cells ◦ Normal bone marrow with no evidence of clonal
plasma cells ◦ Normal skeletal survey and MRI (or CT) of spine and
pelvis (except for the primary solitary lesion) ◦ Absence of end-organ damage (CRAB) that can be
attributed to a lymphoplasma cell proliferative disorder Progression to MM 10% in 3 years
Rajkumar SV. Lancet Oncol 2014;15:e538–48.

CBC and blood smear ◦ Anemia 40-73% ◦ Rouleaux formation if hyperglobulinemia
Blood chemistry ◦ BUN, Cr ◦ Serum calcium ◦ LFT : hyperglobulinemia normal alkaline phosphatase

Detection of monoclonal protein ◦ Serum and urine protein electrophoresis
(SPEP, UPEP) ◦ Urine Bence Jones protein ◦ Serum immunofixation ◦ Serum free light chain
Bone marrow aspiration and biopsy ◦ Increase plasma cells (>10%)

Serum protein electrophoresis (SPEP)

Dispenzieri A. Leukemia 2009;23:215–24.
Normal kappa : lambda ratio 0.26-1.65

Kumar S. Lancet Oncol 2016; 17:e328–46.

Lahuerta JJ. J Clin Oncol 2017;35:2900-10.

Imaging study Conventional X-ray: IMWG guideline A complete conventional radiographic status is
recommended for each newly diagnosed patient ◦ Skull in 2 views ◦ Spine (cervical/thoracic/lumbar) in 2 views ◦ Chest AP ◦ Pelvis AP ◦ Long proximal bones AP
80% have radiological evidence of involvement
Dimopoulos M. Leukemia 2009;23:1545-56.


Hillengass J. Leuk Lymphoma 2013;54:1355–63.
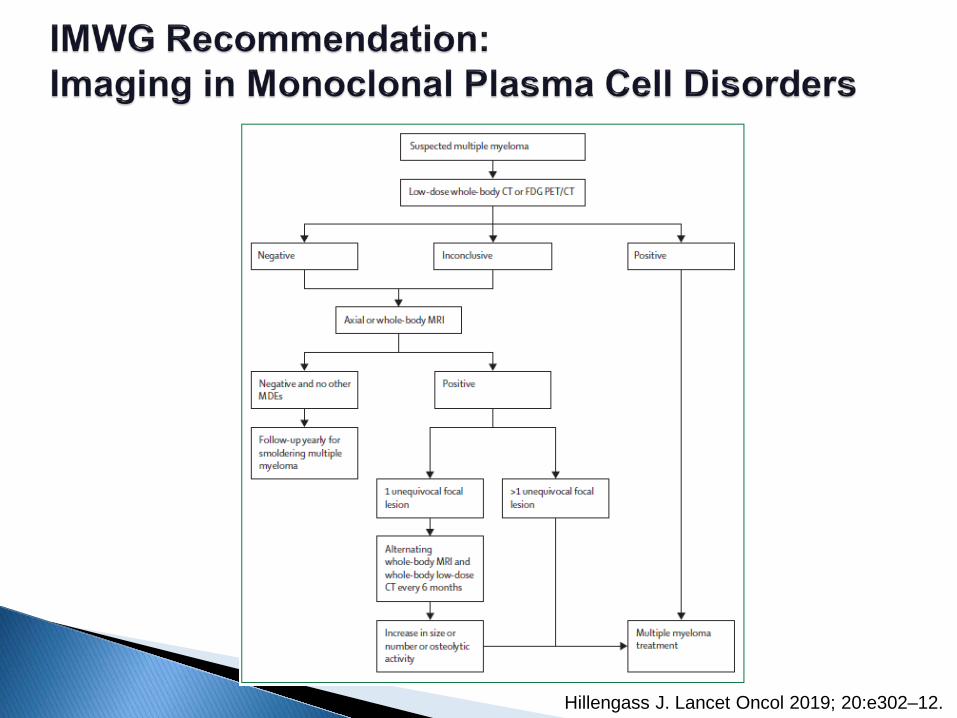
Hillengass J. Lancet Oncol 2019; 20:e302–12.

Hillengass J. Lancet Oncol 2019; 20:e302–12.

Revised ISS for MM Overall survival
Palumbo A. J Clin Oncol 2015;33:2863-9.

Kumar S. Lancet Oncol 2016;17:e328–46.

Kumar S. Lancet Oncol 2016;17:e328–46.
**Clinical relapse: for use in clinical practice

Dejoie T. Leukemia 2019;33:313–8.

Newly diagnosed patients with MM
Transplant-eligible patients Transplant-ineligible patients
Induction chemotherapy
Autologous stem cell transplantation (ASCT)
Induction chemotherapy
Adapted from Palumbo A. N Engl J Med 2011;364:1046-60.

Many choices of induction therapy Transplant-eligible patients Depth of response correlated with long-term outcome Combination with novel agents (usually with
corticosteriod) Proteasome inhibitors: bortezomib Immunomodulatory drugs: thalidomide, lenalidomide Non melphalan-based regimen
Transplant-ineligible patients ◦ Balance efficacy and toxicity
Palumbo A. N Engl J Med 2011;364:1046-60.

Long term follow up after high-dose therapy with autologous transplantation 10 year survival rate is 20% 10% of patients seem to remain in continuous CR
Martinez-Lopez J. Blood 2011;118:529-34.

Kyle RA. N Engl J Med 2004;351:1860-73.

Moreau P. Ann Oncol 2017;28 (Suppl 4):iv52–iv61.

Stewart AW. Blood 2009;114:5436-43.

1 Palumbo A. J Clin Oncol 2014;32:587-600. 2 Larocca A. Blood 2015;126:2179-85.
For frail patients: palliative care, reduced-dose corticosteroids, MP, Cy-dex2
Newly diagnosed elderly or younger patients with MM not eligible for high dose treatment (MEL 200)
Assessment of patient status Presence of comorbidities and/or limits in mental or mobility functions
Specific index and scores can be used
Very Fit Fit Unfit
Reduced-intensity ASCT (MEL 100)
MPT BMP/BMPT-BT
BCD/BRD MPR-R/Rd
Low-dose MPT/BMP
Bd/Rd

Progression/ Relapsed
Indication of treatment
Clinical relapsed √ √ Biochemical relapsed 25% increase
from baseline Doubling in 2-3 months
Serum M-protein AI > 0.5 g/dL AI ≥ 1 g/dL Urine M-protein AI > 200 mg/day AI ≥ 500 mg/day Percentage of BM plasma cells AI > 10% - Difference between involved FLC and uninvolved FLC
AI > 10 mg/dL AI ≥ 20 mg/dL + abnormal ratio or 25% increase
Sonneveld P. Haematologica 2016;101:396–406. Laubach J. Leukemia 2016;30:1005-17.
AI: absolute increase

Clinical relapse ◦ Development of new soft-tissue plasmacytomas or
bone lesions ◦ Definite increase (≥ 50%) in size of existing
plasmacytomas or bone lesions ◦ Hypercalcemia (≥ 11.5 mg/dL) ◦ Decrease in hemoglobin of ≥ 2 g/dL, or to < 10 g/dL ◦ Rise in serum creatinine by ≥ 2 mg/dL or more ◦ Hyperviscosity requiring therapeutic intervention
Sonneveld P. Haematologica 2016;101:396–406.

Patient factors Disease factors Previous treatment
Chim CS. Leukemia 2018;32:252–62. Moreau P. Ann Oncol 2017;28 (Suppl 4):iv52–iv61.
Laubach J. Leukemia 2016;30:1005-17.

Patient factors Disease factors Previous treatment
Chim CS. Leukemia 2018;32:252–62. Moreau P. Ann Oncol 2017;28 (Suppl 4):iv52–iv61.
Laubach J. Leukemia 2016;30:1005-17.
Age (still eligible for a second ASCT?)
Co-morbid illnesses Performance status Patient’s preference “Goal of therapy”

Patient factors Disease factors Previous treatment
Chim CS. Leukemia 2018;32:252–62. Moreau P. Ann Oncol 2017;28 (Suppl 4):iv52–iv61.
Laubach J. Leukemia 2016;30:1005-17.
High-risk karyotypic aberrations such as del(17p)
Aggressiveness Organ function Extramedullary
disease

Adverse cytogenetic abnormalities: hypodiploidy, t(4;14), del(17p), amp(1q21)
High B2M (> 5.5 mg/L) or low albumin (< 3.5 mg/dL) The presence of extramedullary disease Short duration of response to prior therapy or progression
while on current therapy Aggressive clinical features including ◦ Rapid onset of clinical symptoms ◦ Extensive disease at relapse based on laboratory, pathology, or
radiographic findings ◦ Disease-associated organ dysfunction at relapse including renal failure,
hypercalcemia, or bone event such as fracture High LDH Circulating plasma cells
Laubach J. Leukemia 2016;30:1005-17.

Patient factors Disease factors Previous treatment
Chim CS. Leukemia 2018;32:252–62. Moreau P. Ann Oncol 2017;28 (Suppl 4):iv52–iv61.
Laubach J. Leukemia 2016;30:1005-17.
Duration of response to prior induction or ASCT
Progression on therapy
Side-effects from prior treatments

Moreau P. Ann Oncol 2017;28 (Suppl 4):iv52–iv61.

New proteasome inhibitor ◦ Carfilzomib ◦ Ixazomib
New immunomodulatory agents ◦ Pomalidomide
Monoclonal antibodies ◦ Anti-CD38: daratumumab ◦ Anti-SLAMF7: elotuzumab
Histone deacetylase inhibitor ◦ Panobinostat
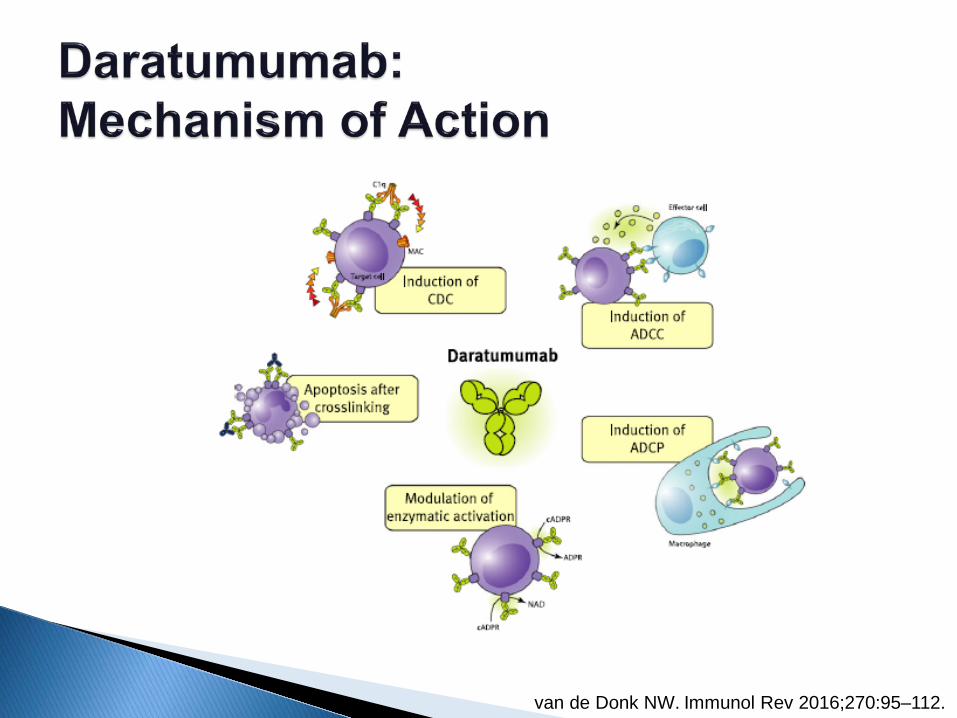
van de Donk NW. Immunol Rev 2016;270:95–112.

Lonial S. J Clin Oncol 2015;33 [abstract 8508].
SLAMF7: signaling lymphocytic activation molecule F7
Trial and Regimen CR (%)
Median PFS (mo)
HR for Disease Progression or Death (95% CI)
P Value
Lenalidomide-based regimen
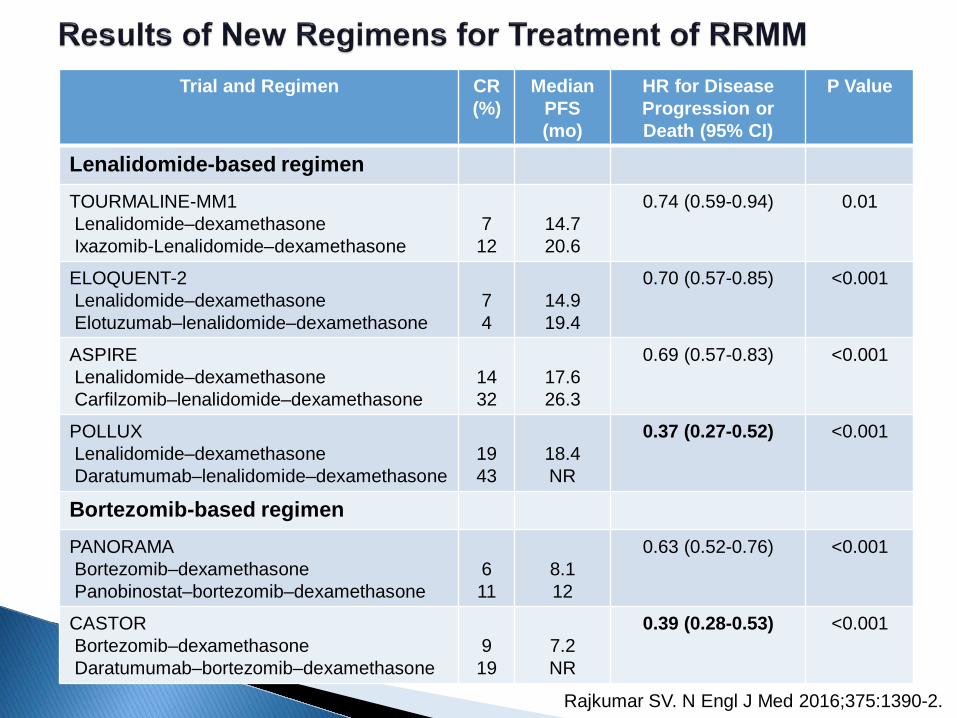
TOURMALINE-MM1 Lenalidomide–dexamethasone Ixazomib-Lenalidomide–dexamethasone
7 12
14.7 20.6
0.74 (0.59-0.94) 0.01
ELOQUENT-2 Lenalidomide–dexamethasone Elotuzumab–lenalidomide–dexamethasone
7 4
14.9 19.4
0.70 (0.57-0.85) <0.001
ASPIRE Lenalidomide–dexamethasone Carfilzomib–lenalidomide–dexamethasone
14 32
17.6 26.3
0.69 (0.57-0.83) <0.001
POLLUX Lenalidomide–dexamethasone Daratumumab–lenalidomide–dexamethasone
19 43
18.4 NR
0.37 (0.27-0.52) <0.001
Bortezomib-based regimen PANORAMA Bortezomib–dexamethasone Panobinostat–bortezomib–dexamethasone
6 11
8.1 12
0.63 (0.52-0.76) <0.001
CASTOR Bortezomib–dexamethasone Daratumumab–bortezomib–dexamethasone
9 19
7.2 NR
0.39 (0.28-0.53)
<0.001
Rajkumar SV. N Engl J Med 2016;375:1390-2.

Indications to initiate BMA Situation Management
MM patients with lytic disease or compression fracture
IV pamidronate 90 mg or zoledronic acid 4 mg q 3 to 4 wks Alternative treatment: denosumab
MM patients without lytic disease
The Expert Panel supports starting intravenous bisphosphonates
Solitary plasmacytoma or smoldering myeloma or MGUS with osteopenia
Bisphosphonates is not recommended
Anderson K. J Clin Oncol 2018;36:812-8.

All patients receiving MM therapy should be given ◦ Bisphosphonates (category 1) or ◦ Denosumab: preferred in patients with renal
insufficiency Baseline dental exam Monitor ◦ Renal dysfunction (bisphosphonate therapy) ◦ Osteonecrosis of the jaw
NCCN Guideline version 2.2019.

Multiple myeloma (MM) Systemic AL amyloidosis Monoclonal gammopathy of renal
significance (MGRS) POEMS syndrome

Merlini G. N Engl J Med 2003;349:583-96.

Merlini G. N Engl J Med 2003;349:583-96.

Merlini G. N Engl J Med 2003;349:583-96.

Nondiabetic nephrotic syndrome Nonischemic cardiomyopathy with “hypertrophy”
on echocardiography Hepatomegaly or increased alkaline phosphatase
value with no imaging abnormalities of the liver Chronic inflammatory demyelinating
polyneuropathy with a monoclonal protein
Gertz MA. Am J Hematol 2014;89:1133–40.

Presence of an amyloid-related systemic syndrome ◦ Renal, liver, heart, GI tract, or peripheral nerve
Positive amyloid staining by Congo red in tissue ◦ Fat aspirate, bone marrow, or organ biopsy
Evidence that amyloid is light-chain-related ◦ Direct examination of amyloid using mass spectrometry-
based proteomic analysis, or immunoelectronmicroscopy Evidence of a monoclonal plasma cell proliferative
disorder ◦ Serum or urine monoclonal protein, abnormal free light-chain
ratio, or clonal plasma cells in BM
Rajkumar SV. Lancet Oncol 2014;15:e538–48.

Clinical suspicion of amyloidosis
Tissue biopsy (Congo red staining of abdominal fat or other tissue*)
Immunohistochemical Staining of biopsy Identify Diagnosis
Kappa or lambda light chain
More invasive biopsy of other affected organ +
Monoclonal protein in serum or urine Plasma cell dyscrasia in BM
-
+
- No further work-up
AL amyloidosis (screening for cardiac, renal, hepatic, autonomic involvement, FX deficiency)
* Abdominal fat pad + BM biopsy identify 85% Harrison’s Principle of Internal Medicine, 18th edition.
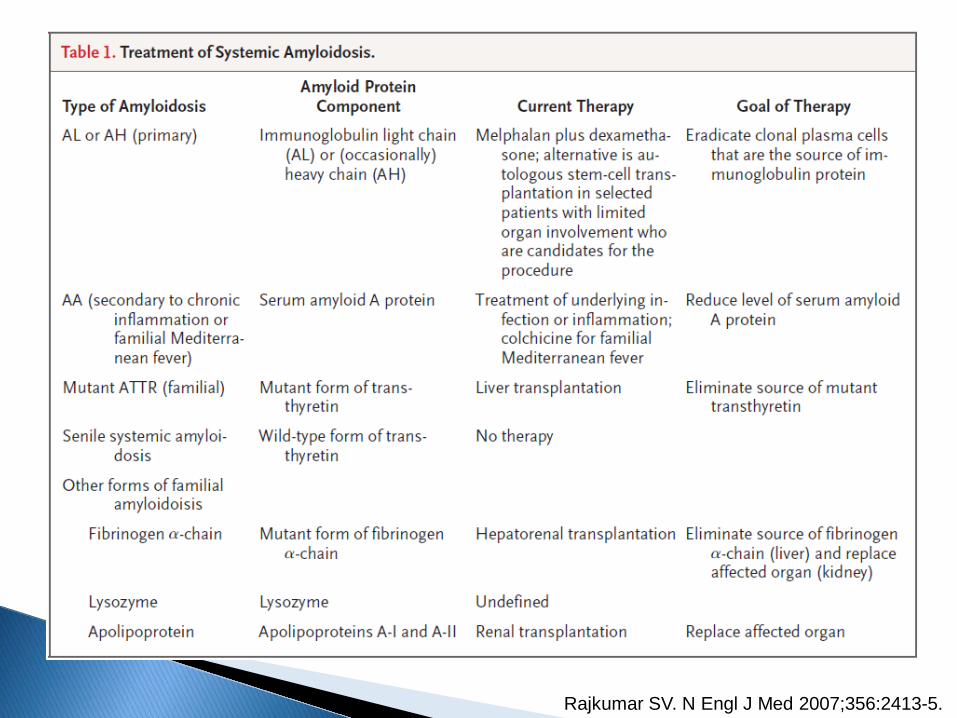
Rajkumar SV. N Engl J Med 2007;356:2413-5.

Chemotherapy ◦ Melphalan-dexamethasone (Mel-dex) ◦ Novel agent based therapy Bortezomib – dexamethasone +/- cyclophosphamide or
melphalan Thalidomide – dexamethasone +/- cyclophosphamide Lenalidomide – dexamethasone +/- cyclophosphamide
Autologous stem cell transplantation (ASCT)
Comenzo RL. Blood 2009;114:3147-57. Gertz MA. Am J Hematol 2014;89:1133–40.

Gertz MA. Amyloid 2010;17(s1):48.

Jaccard A. N Engl J Med 2007;357:1083-93.
56.9 months 22.2 months

Organ response Mel-Dex ASCT P value At least one organ response
39% (17/44) 45% (13/29) 0.60
Renal 11/44 8/29 Hepatic 3/44 5/29 Cardiac 3/44 4/29 Neurologic 2/44 1/29
Jaccard A. N Engl J Med 2007;357:1083-93.

Staging is defined by NT-proBNP and troponin T thresholds of 332 pg/mL and 0.035 ng/mL, respectively.
Dispenzieri A. Blood 2004;104:1881-7.

Jaccard A, et al. 2007 Cibeira MT, et al. 2011
Median OS 22.2 months Median OS 76 months
1 Jaccard A. N Engl J Med 2007;357:1083-93. 2 Cibeira MT. Blood 2011;118:4346-52.

Gertz MA. Am J Hematol 2014;89:1133–40.

Gertz MA. Am J Hematol 2014;89:1133–40.

Heart failure ◦ Salt restriction and weight monitoring ◦ Diuretics: do not reduce intravascular volume ◦ ACE inhibitors: should be used at the lowest dose with
caution due to hypotension ◦ Left ventricular assist devices: might be used as a
bridge for candidates for heart transplantation Hypotension ◦ Elastic leotards ◦ Midodrine
Gavriatopoulou M. Leukemia 2018;32:1883–98.

Arrhythmias ◦ Pacemaker for patients with recurrent syncope due to
arrhythmia/ICD use remains controversial ◦ Amiodarone: avoid digoxin
Nutritional support Diarrhea: octreotide Neuropathic pain: gabapentin or pregabalin Organ transplant for patients with end-organ
damage who achieve CR
Gavriatopoulou M. Leukemia 2018;32:1883–98.

Multiple myeloma (MM) Systemic AL amyloidosis Monoclonal gammopathy of renal
significance (MGRS) POEMS syndrome

Organized
Non-organized (granular)
Crystals Fibrillar Microtubular Myeloma cast nephropathy Light chain
amyloidosis Type I and type II cryoglobulinemic GN
Light chain proximal tubulopathy (with or without Fanconi syndrome)
Nonamyloid Immunotactoid GN
Crystal-storing histocytosis Fibrillary GN GOMMID
MIDD (Randall type) Other LCDD Proliferative GN with monoclonal Ig deposits
LHCDD Waldenström macroglobulinemia
HCDD
GOMMID, glomerulonephritis with organized microtubular monoclonal Ig deposits; MIDD, monoclonal immunoglobulin deposition disease; LCDD, light-chain deposition disease; LHCDD, light and heavy-chain deposition disease; HCDD, heavy-chain deposition disease
Leung N. Blood 2012;120:4292-5.

Dimopoulos MA. J Clin Oncol 2016;34:1544-57.

Fava A. Clin Kidney J 2018;11:777–85.

Dimopoulos MA. J Clin Oncol 2016;34:1544-57.

Dimopoulos MA. J Clin Oncol 2016;34:1544-57.

Multiple myeloma (MM) Systemic AL amyloidosis Monoclonal gammopathy of renal
significance (MGRS) POEMS syndrome

Paraneoplastic syndrome due to an underlying plasma cell neoplasm ◦ Polyneuropathy ◦ Organomegaly ◦ Endocrinopathy ◦ Monoclonal plasma cell disorder (M protein) ◦ Skin changes
Other important features: PEST ◦ Papilledema, Extravascular volume overload, Sclerotic
bone lesions, Thrombocytosis/erythrocytosis
Dispenzieri A. Am J Hematol 2017;92:814–29.
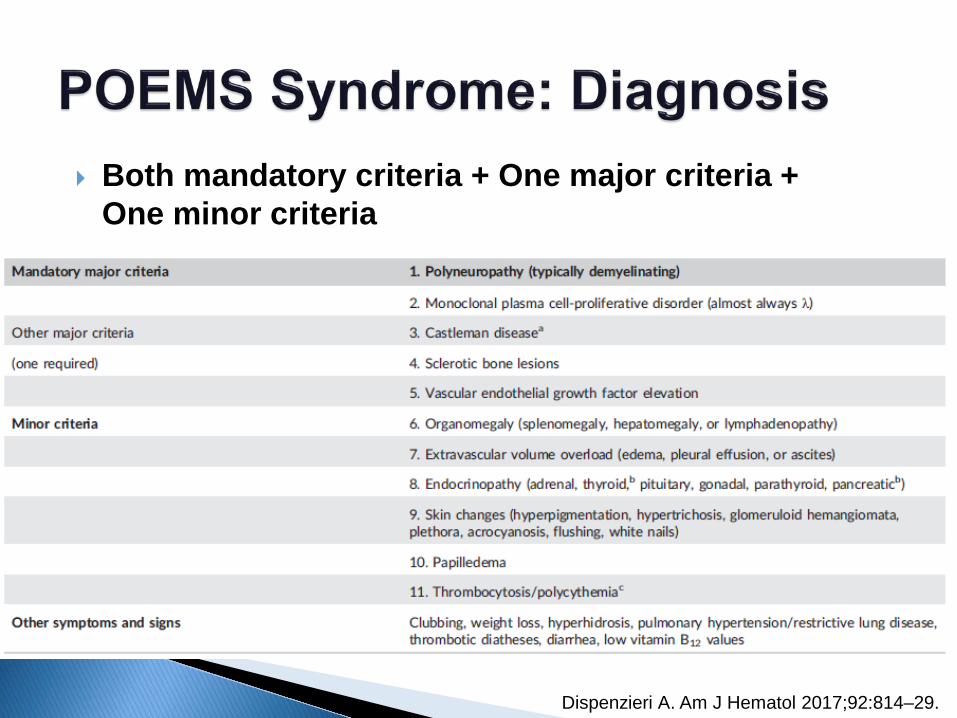
Both mandatory criteria + One major criteria + One minor criteria
Dispenzieri A. Am J Hematol 2017;92:814–29.

Dispenzieri A. Am J Hematol 2017;92:814–29.

Dispenzieri A. Am J Hematol 2017;92:814–29.

Slide from Lunn M. MRC Centre for neuromuscular disease.

Dispenzieri A. Am J Hematol 2017;92:814–29.
Systemic therapy e.g. melphalan-dexamethasone, corticosteriods, bortezomib, thalidomide, lenalidomide, ASCT

Spectrum of plasma cell disorders from MGUS, smoldering MM to MM ◦ MM: CRAB symptoms or biomarker of
malignancy Other organ involvement from monoclonal
immunoglobulin ◦ AL amyloidosis: nephrotic syndrome, cardiac
involvement, neuropathy, skin, GI ◦ MGRS: nephrotic-nephritis, renal failure ◦ POEMS: polyneuropathy (↑ VEGF)


















