68
Basic Dysrhythmias Adam Glaser, BS, EMT-P -Electrical Conduction of the Heart -A System of Defining 3-Lead EKG’s

Basic Dysrhythmias
Adam Glaser, BS, EMT-P-Electrical Conduction of the Heart-A System of Defining 3-Lead EKG’s

Pieces Parts
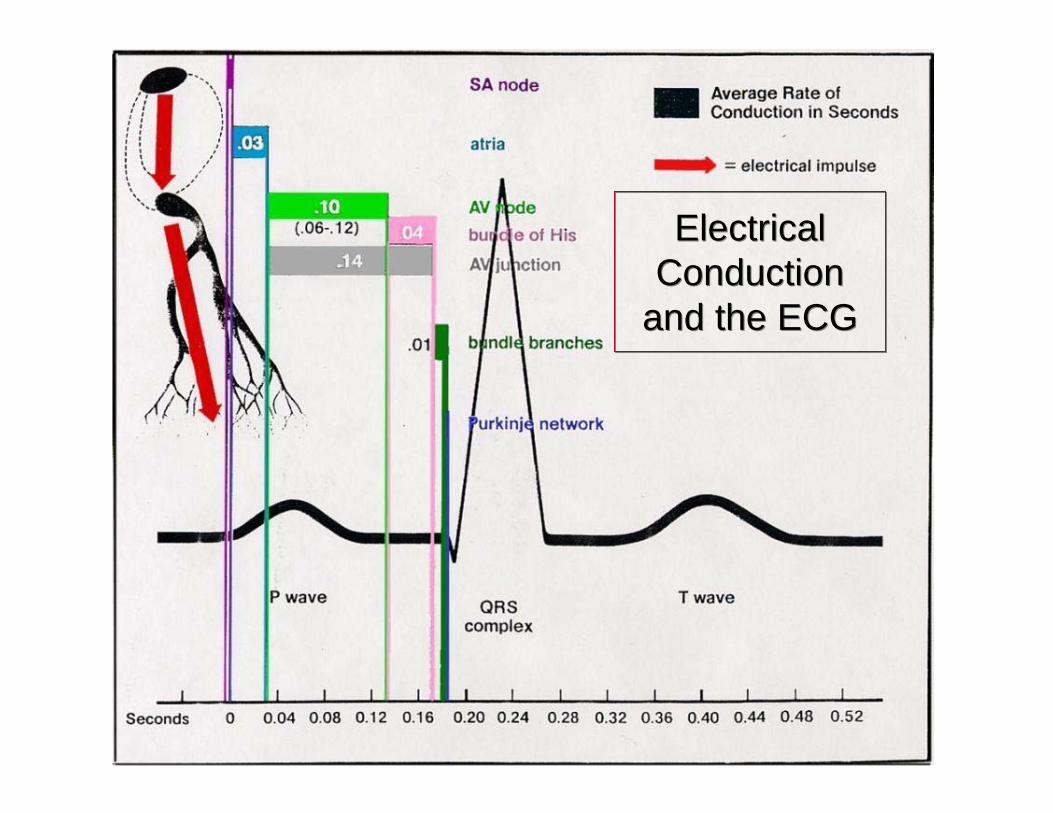
Electrical Conduction
and the ECG
Electrical Conduction
and the ECG

The Isoelectric Line
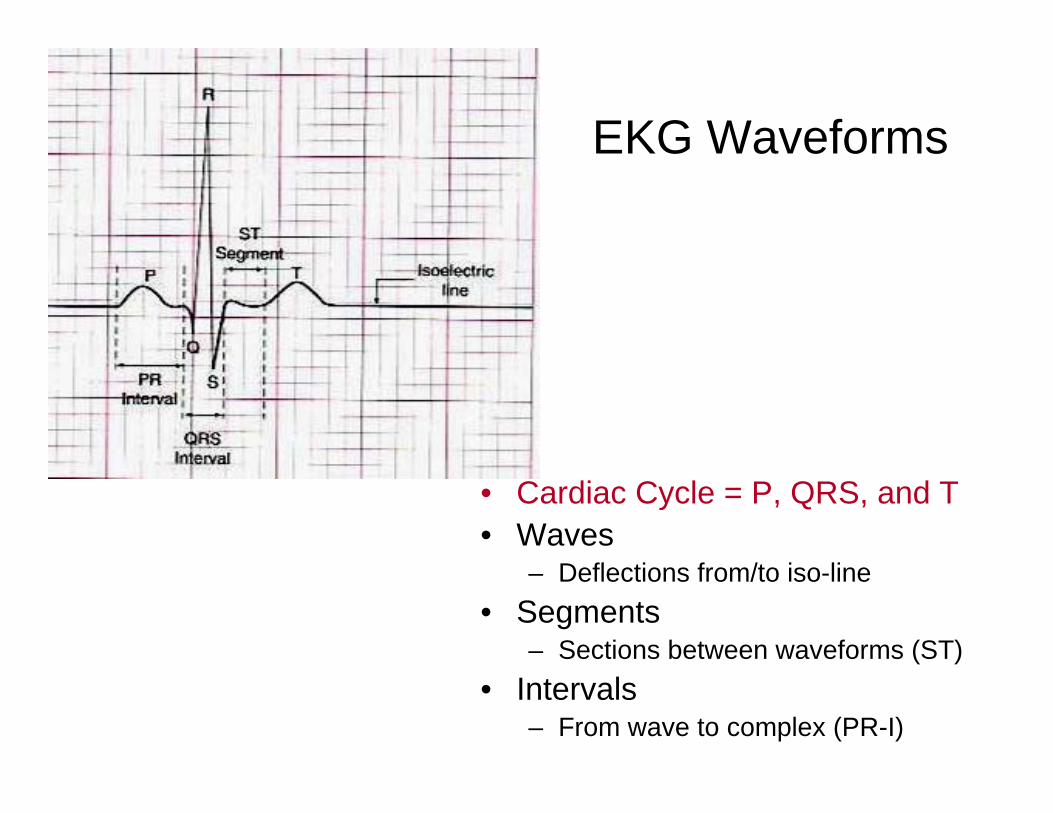
EKG Waveforms
• Cardiac Cycle = P, QRS, and T• Waves
– Deflections from/to iso-line• Segments
– Sections between waveforms (ST)• Intervals
– From wave to complex (PR-I)

The Electrocardiograph
• Electrical Activity– Not Muscle
• Records +/– impulses• Paper 25mm/s• Counting Rates
– 300-150-100-75-70-60-50
– 6 s x 10– 10 s x 6– The little number on
the monitor ☺
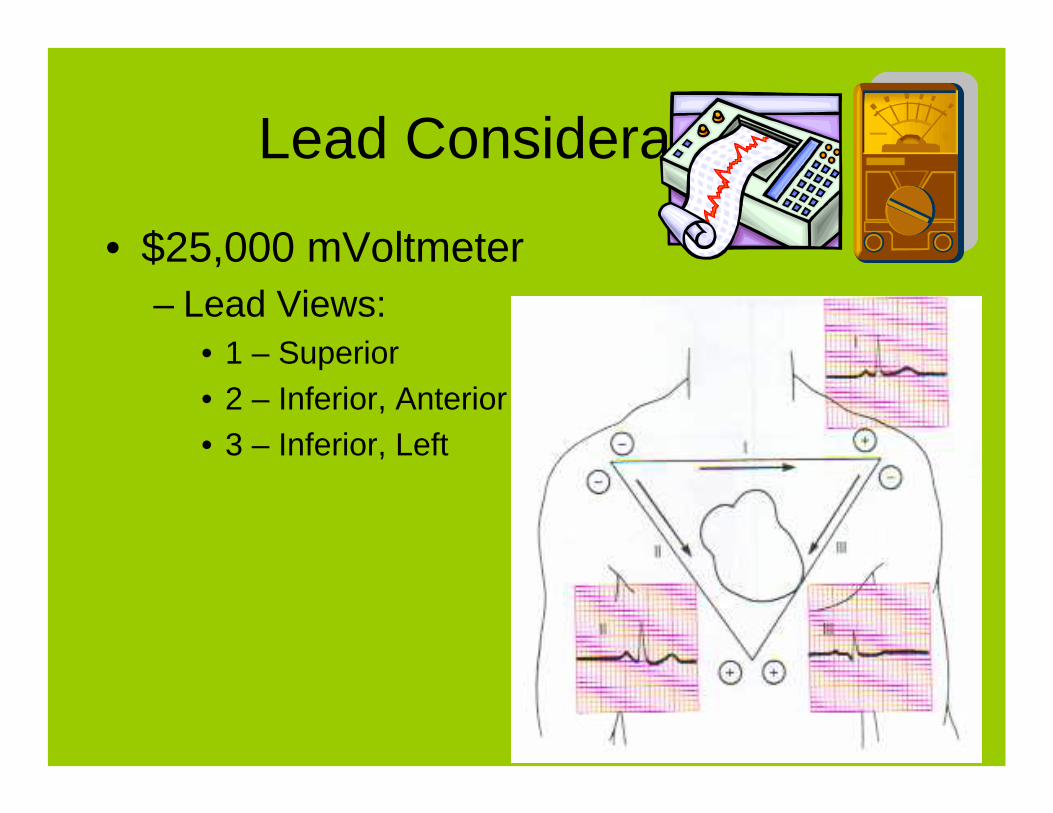
Lead Considerations
• $25,000 mVoltmeter– Lead Views:
• 1 – Superior• 2 – Inferior, Anterior• 3 – Inferior, Left

The Components
• SA Node• Internodal Pathways• AV Junction• AV Node• Bundle of His• L & R Bundle Branch• Purkinje Network• Purkinje Fibers

Ode to a Node• Have a heart, and have no fear,
The SA node is over here.Beating at a constant rate,
60 – 100 is really great.The AV node can make a show,If SA node has gone too slow.
40 – 60 is not too badIf it’s all you’ve got, you will be glad.
Should the whole thing drop it’s speed,His and bundle branches will take the lead.And that, my friend is the whole and part,Of the conduction system of your heart.
– Flip and See ECG, Cohn/Gilroy-Doohan
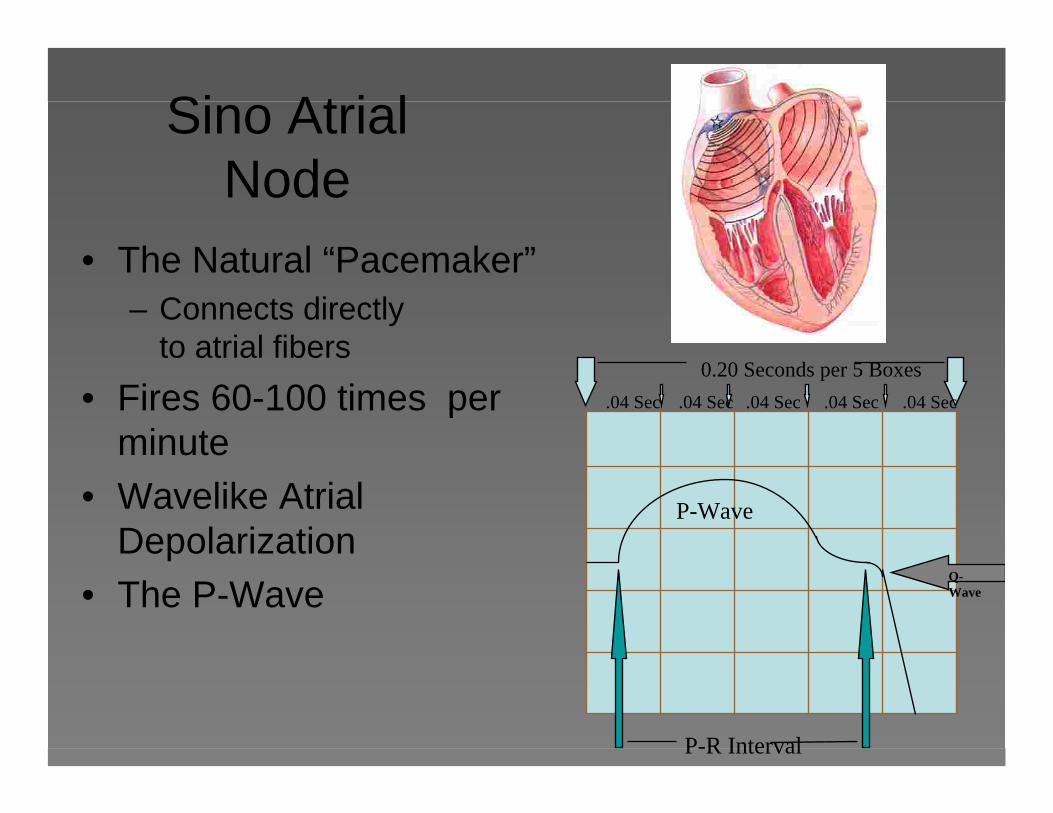
Sino Atrial Node
• The Natural “Pacemaker”– Connects directly
to atrial fibers• Fires 60-100 times per
minute• Wavelike Atrial
Depolarization• The P-Wave
P-Wave
P-R Interval
Q-Wave
.04 Sec .04 Sec .04 Sec .04 Sec .04 Sec
0.20 Seconds per 5 Boxes
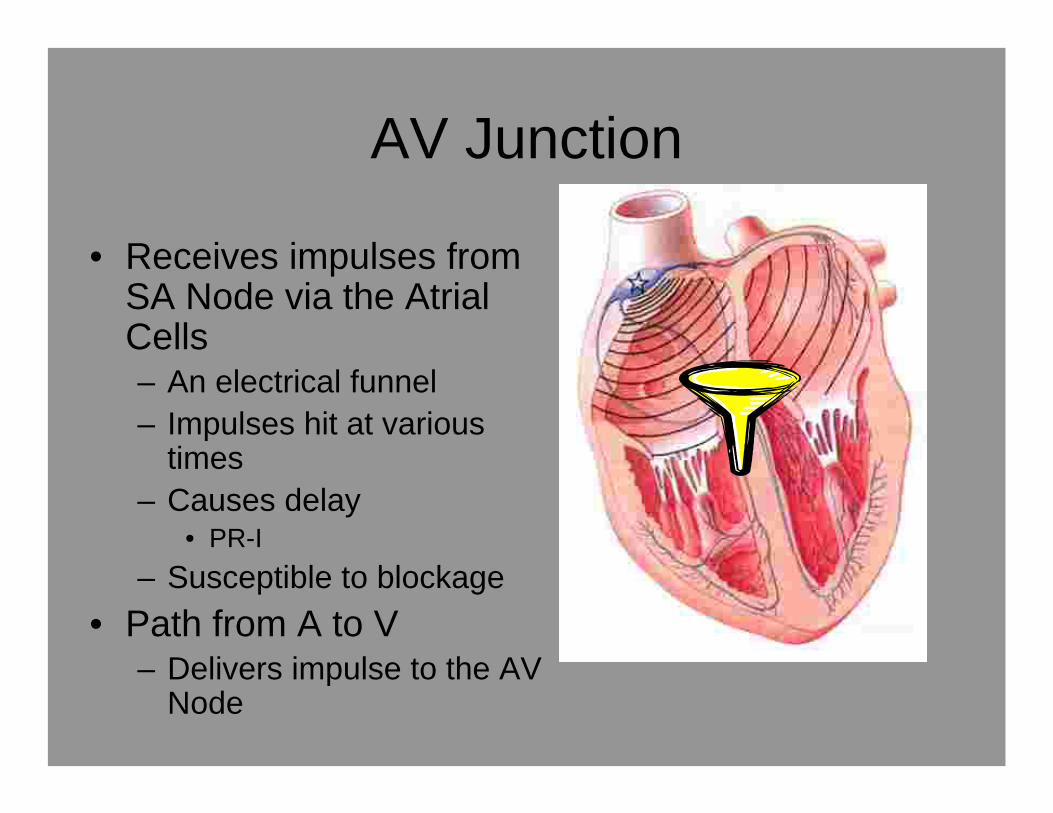
AV Junction
• Receives impulses from SA Node via the AtrialCells– An electrical funnel– Impulses hit at various
times– Causes delay
• PR-I– Susceptible to blockage
• Path from A to V– Delivers impulse to the AV
Node

Atrio-Ventricular Node• Lies between the Atria
and Ventricles• Collects impulses from
above• Stimulates Ventricles• If unstimulated
– Intrinsic rate 40-60
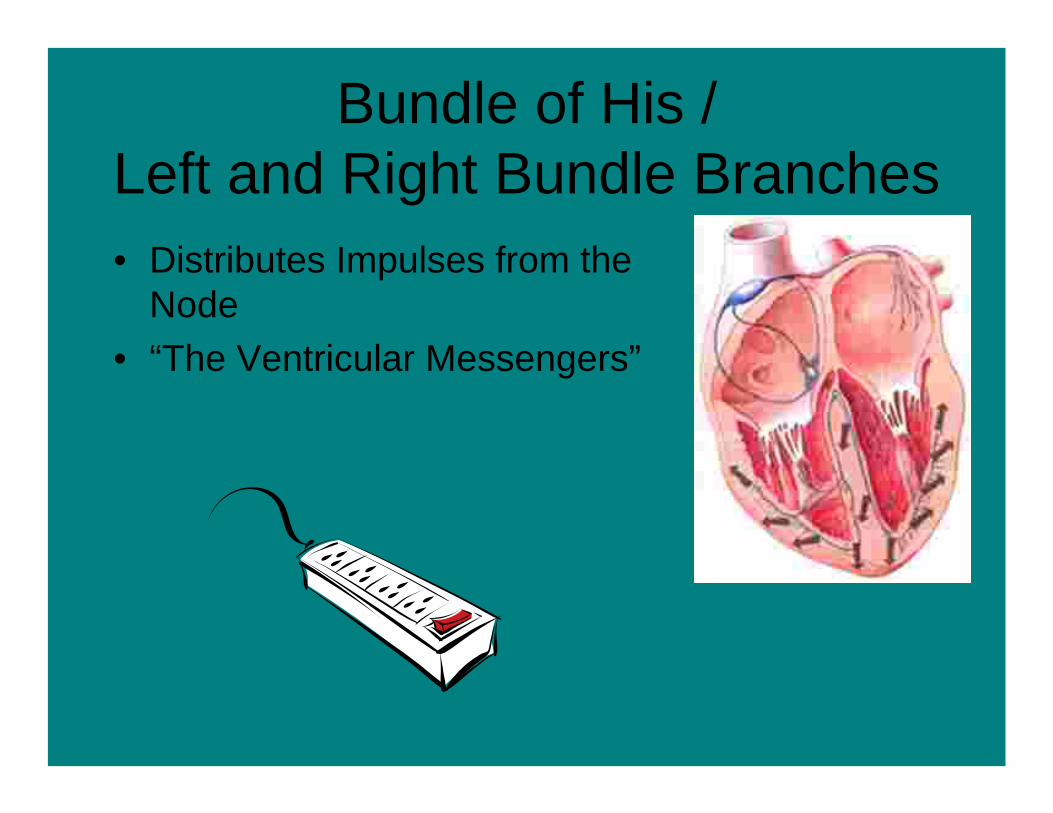
Bundle of His / Left and Right Bundle Branches• Distributes Impulses from the
Node• “The Ventricular Messengers”
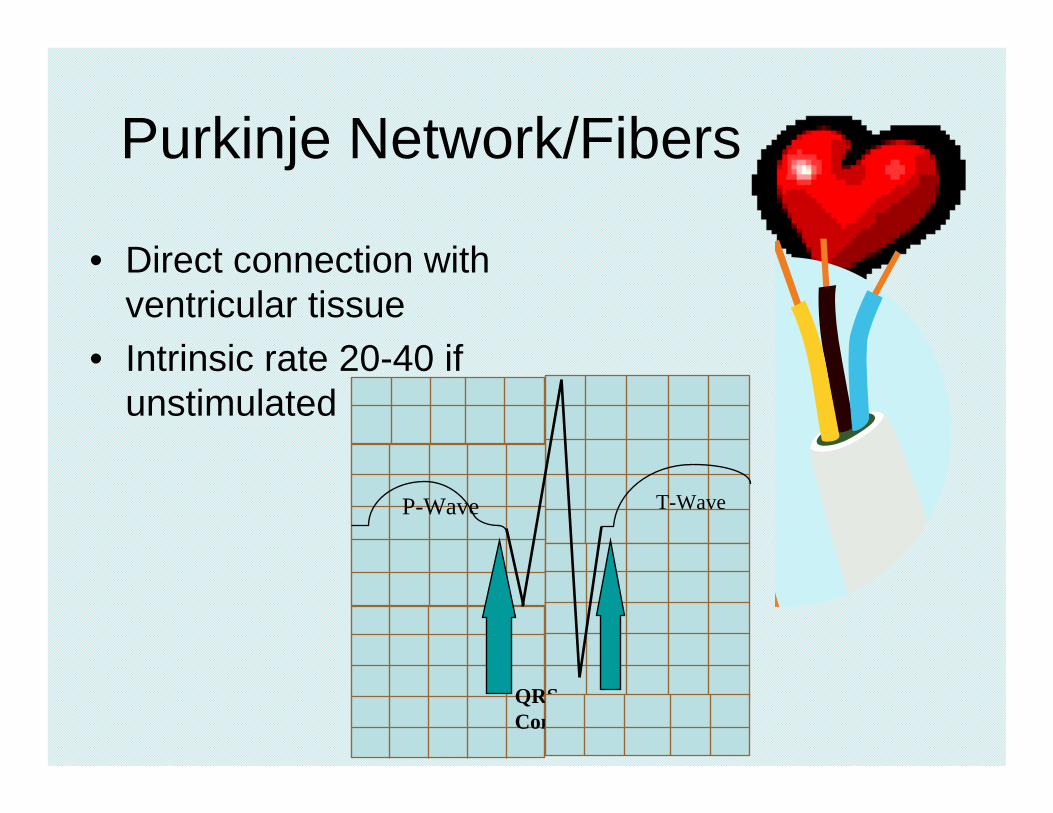
Purkinje Network/Fibers
• Direct connection with ventricular tissue
• Intrinsic rate 20-40 if unstimulated
P-Wave
P-R Interval
QRS Complex
T-Wave

The Six Step Approach
• What is the Rate?• Is the Rhythm Regular?• Are there P-Waves?• Is the P-R Interval Normal?• Is the QRS Complex Normal?• Is There a P-Wave for Every QRS?
Step 1 = Rate
• Is the rate between 60-100 (Sinus)• Between 40-60 (Junctional/Bradycardic)• Above 100 (Tachycardic)• Between 20-40 (Ventricular)

Step 2 = Regularity
• At-a-glance: Does it look regular?• Are the P-Waves evenly spaced?• Are the QRS Complexes evenly spaced?

Step 3 = P-Waves
• Are P-Waves present?• Are they upright and rounded?• Are they irregular in any way: Notched /
Peaked / Depressed…?• Are they all the same?

Step 4 = P-R Interval
• Is the P-R Interval between 0.12-0.20?• Is it too long / too short? (Block)• Is it the same on every conduction?• Is it absent?
Step 5 = QRS Complex
• Is it there?• Is it between 0.04 - 0.12?• Does it have any abnormalities? (Notched
/ Rabbit Eared / Wide / Bizarre)

Step 6 = P-QRS Married?
• Is there a P-wave for every QRS?• Are there more P-Waves than QRS?• Are the P-Waves after or within the QRS?

Describe What You’ve Found!!!
• IN GENERAL (underlying rhythms)!!!• What are the abnormalities?• Does it originate in the Sinus Node?• Does it follow through from the Atria to the
ventricles? Are there abnormal delays?• What are the exceptions to the underlying
rhythm? (Describe those also)
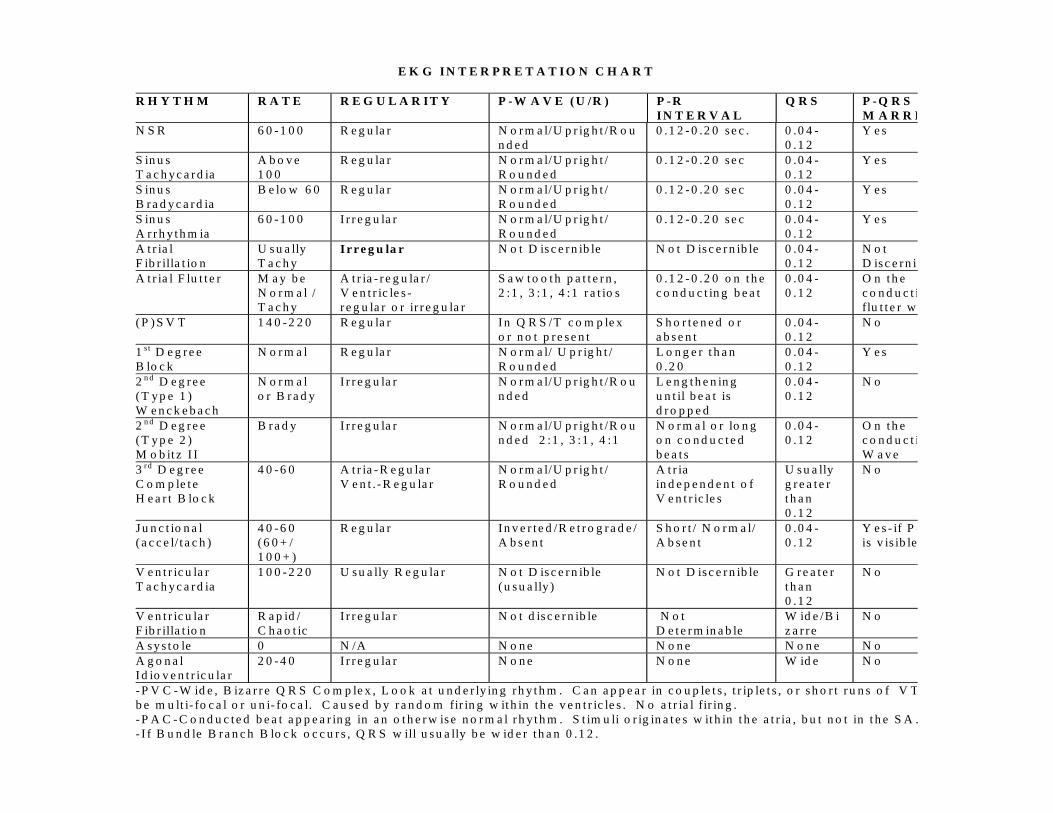
E K G I N T E R P R E T A T I O N C H A R T
R H Y T H M R A T E R E G U L A R I T Y P - W A V E ( U /R ) P - RI N T E R V A L
Q R S P - Q R SM A R R I
N S R 6 0 - 1 0 0 R e g u la r N o r m a l/U p r ig h t /R o un d e d
0 .1 2 - 0 .2 0 s e c . 0 .0 4 -0 .1 2
Y e s
S in u sT a c h y c a r d ia
A b o v e1 0 0
R e g u la r N o r m a l/U p r ig h t /R o u n d e d
0 .1 2 - 0 .2 0 s e c 0 .0 4 -0 .1 2
Y e s
S in u sB r a d y c a r d ia
B e lo w 6 0 R e g u la r N o r m a l/U p r ig h t /R o u n d e d
0 .1 2 - 0 .2 0 s e c 0 .0 4 -0 .1 2
Y e s
S in u sA r r h y t h m ia
6 0 - 1 0 0 I r r e g u la r N o r m a l/U p r ig h t /R o u n d e d
0 .1 2 - 0 .2 0 s e c 0 .0 4 -0 .1 2
Y e s
A t r ia lF ib r illa t io n
U s u a llyT a c h y
I r r e g u la r N o t D is c e r n ib le N o t D is c e r n ib le 0 .0 4 -0 .1 2
N o tD is c e r n ib
A t r ia l F lu t t e r M a y b eN o r m a l /T a c h y
A t r ia - r e g u la r /V e n t r ic le s -r e g u la r o r ir r e g u la r
S a w t o o t h p a t t e r n ,2 :1 , 3 :1 , 4 :1 r a t io s
0 .1 2 - 0 .2 0 o n t h ec o n d u c t in g b e a t
0 .0 4 -0 .1 2
O n t h ec o n d u c t iflu t t e r w
( P ) S V T 1 4 0 - 2 2 0 R e g u la r I n Q R S /T c o m p le xo r n o t p r e s e n t
S h o r t e n e d o ra b s e n t
0 .0 4 -0 .1 2
N o
1 st D e g r e eB lo c k
N o r m a l R e g u la r N o r m a l/ U p r ig h t /R o u n d e d
L o n g e r t h a n0 .2 0
0 .0 4 -0 .1 2
Y e s
2 n d D e g r e e( T y p e 1 )W e n c k e b a c h
N o r m a lo r B r a d y
I r r e g u la r N o r m a l/U p r ig h t /R o un d e d
L e n g t h e n in gu n t il b e a t isd r o p p e d
0 .0 4 -0 .1 2
N o
2 n d D e g r e e( T y p e 2 )M o b it z I I
B r a d y I r r e g u la r N o r m a l/U p r ig h t /R o un d e d 2 :1 , 3 :1 , 4 :1
N o r m a l o r lo n go n c o n d u c t e db e a t s
0 .0 4 -0 .1 2
O n t h ec o n d u c t iW a v e
3 rd D e g r e eC o m p le t eH e a r t B lo c k
4 0 - 6 0 A t r ia - R e g u la rV e n t . - R e g u la r
N o r m a l/U p r ig h t /R o u n d e d
A t r iain d e p e n d e n t o fV e n t r ic le s
U s u a llyg r e a t e rt h a n0 .1 2
N o
J u n c t io n a l( a c c e l/ t a c h )
4 0 - 6 0( 6 0 + /1 0 0 + )
R e g u la r I n v e r t e d /R e t r o g r a d e /A b s e n t
S h o r t / N o r m a l/A b s e n t
0 .0 4 -0 .1 2
Y e s - if P -is v is ib le
V e n t r ic u la rT a c h y c a r d ia
1 0 0 - 2 2 0 U s u a lly R e g u la r N o t D is c e r n ib le( u s u a lly )
N o t D is c e r n ib le G r e a t e rt h a n0 .1 2
N o
V e n t r ic u la rF ib r illa t io n
R a p id /C h a o t ic
I r r e g u la r N o t d is c e r n ib le N o tD e t e r m in a b le
W id e /B iz a r r e
N o
A s y s t o le 0 N /A N o n e N o n e N o n e N oA g o n a lI d io v e n t r ic u la r
2 0 - 4 0 I r r e g u la r N o n e N o n e W id e N o
- P V C - W id e , B iz a r r e Q R S C o m p le x , L o o k a t u n d e r ly in g r h y t h m . C a n a p p e a r in c o u p le t s , t r ip le t s , o r s h o r t r u n s o f V Tb e m u lt i- fo c a l o r u n i- fo c a l. C a u s e d b y r a n d o m fir in g w it h in t h e v e n t r ic le s . N o a t r ia l fir in g .- P A C - C o n d u c t e d b e a t a p p e a r in g in a n o t h e r w is e n o r m a l r h y t h m . S t im u li o r ig in a t e s w it h in t h e a t r ia , b u t n o t in t h e S A .- I f B u n d le B r a n c h B lo c k o c c u r s , Q R S w ill u s u a lly b e w id e r t h a n 0 .1 2 .
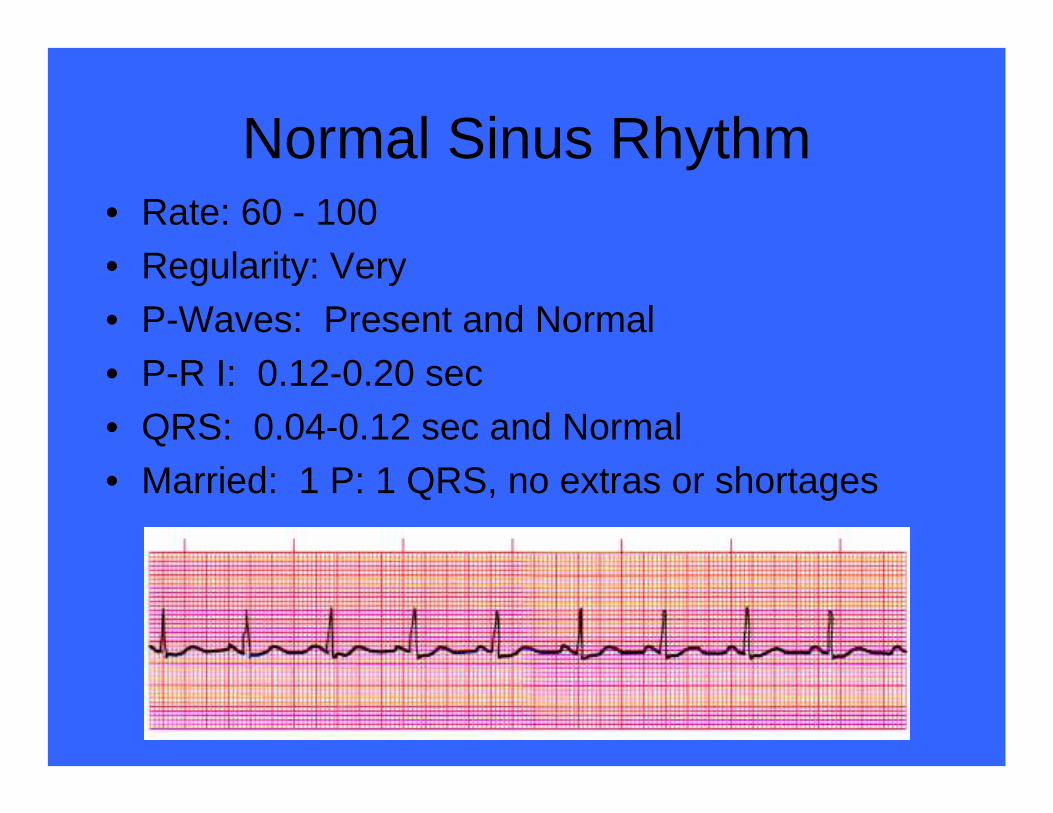
Normal Sinus Rhythm• Rate: 60 - 100• Regularity: Very• P-Waves: Present and Normal• P-R I: 0.12-0.20 sec• QRS: 0.04-0.12 sec and Normal• Married: 1 P: 1 QRS, no extras or shortages

Sinus ArrhythmiaRate: 60 - 100Regularity: IrregularP-Waves: Present and NormalP-R I: 0.12-0.20 secQRS: 0.04-0.12 sec and NormalMarried: 1 P: 1 QRS, no extras or shortages
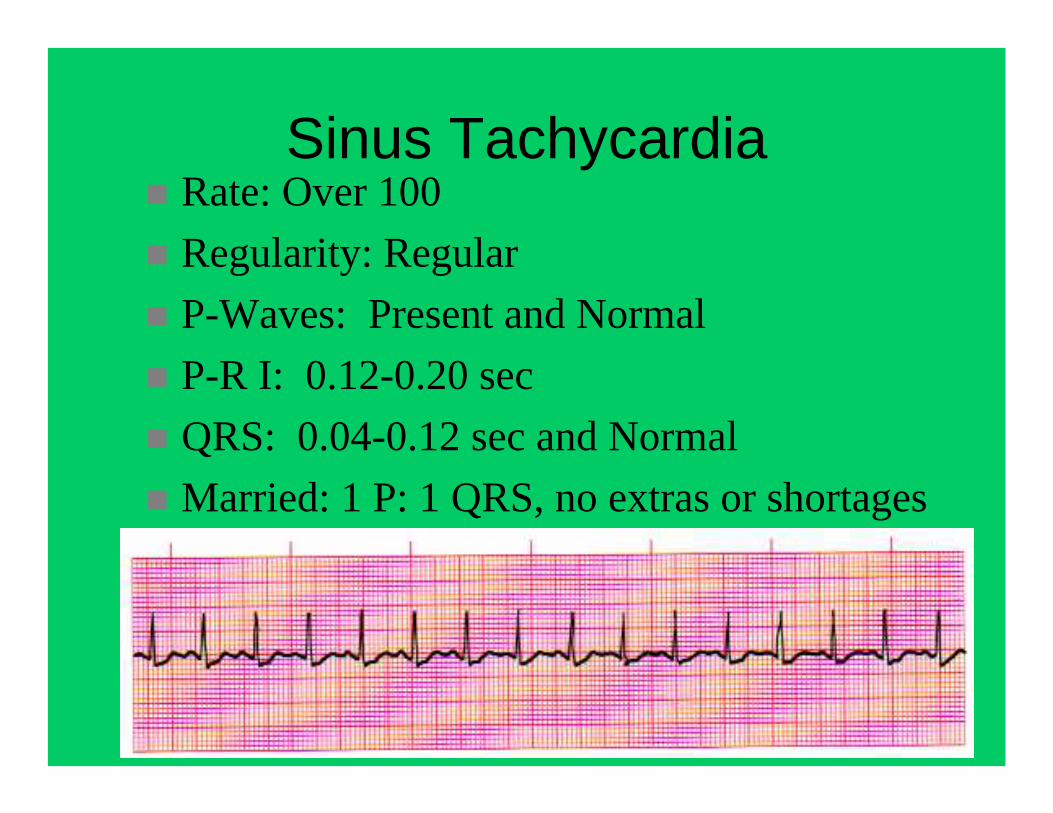
Sinus TachycardiaRate: Over 100Regularity: RegularP-Waves: Present and NormalP-R I: 0.12-0.20 secQRS: 0.04-0.12 sec and NormalMarried: 1 P: 1 QRS, no extras or shortages

Sinus BradycardiaRate: Less than 60Regularity: RegularP-Waves: Present and NormalP-R I: 0.12-0.20 secQRS: 0.04-0.12 sec and NormalMarried: 1 P: 1 QRS, no extras or shortages

Atrial FibrillationRate: Usually tachyRegularity: Irregular (Irregularly irregular)P-Waves: Not DiscernibleP-R I: UndeterminableQRS: 0.04-0.12 secMarried: Undeterminable

Atrial FlutterRate: Usually tachyRegularity: Atria Regular
• Ventricles May be Irregular
P-Waves: Sawtooth Pattern 2:1, 3:1, 4:1...P-R I: 0.12-0.20 sec on conducting beatQRS: 0.04-0.12 secMarried: P-waves outnumber QRS
(Picket fence)

(Paroxysmal) Supra Ventricular TachRate: 140-220
Regularity: RegularP-Waves: Usually falls within the QRS-T complex (not visible)P-R I: Shorter than 0.12, or absentQRS: 0.04-0.12 sec and NormalMarried: Undeterminable

SVT• WPW
– Usually based on Hx.– Delta wave on Q– Shortened PR-I– No Verapamil – Accessory Path use
increase

1st Degree Heart BlockRate: 60 - 100Regularity: VeryP-Waves: Present and NormalP-R I: Longer than 0.20 secQRS: 0.04-0.12 sec and NormalMarried: 1 P: 1 QRS, no extras or shortages
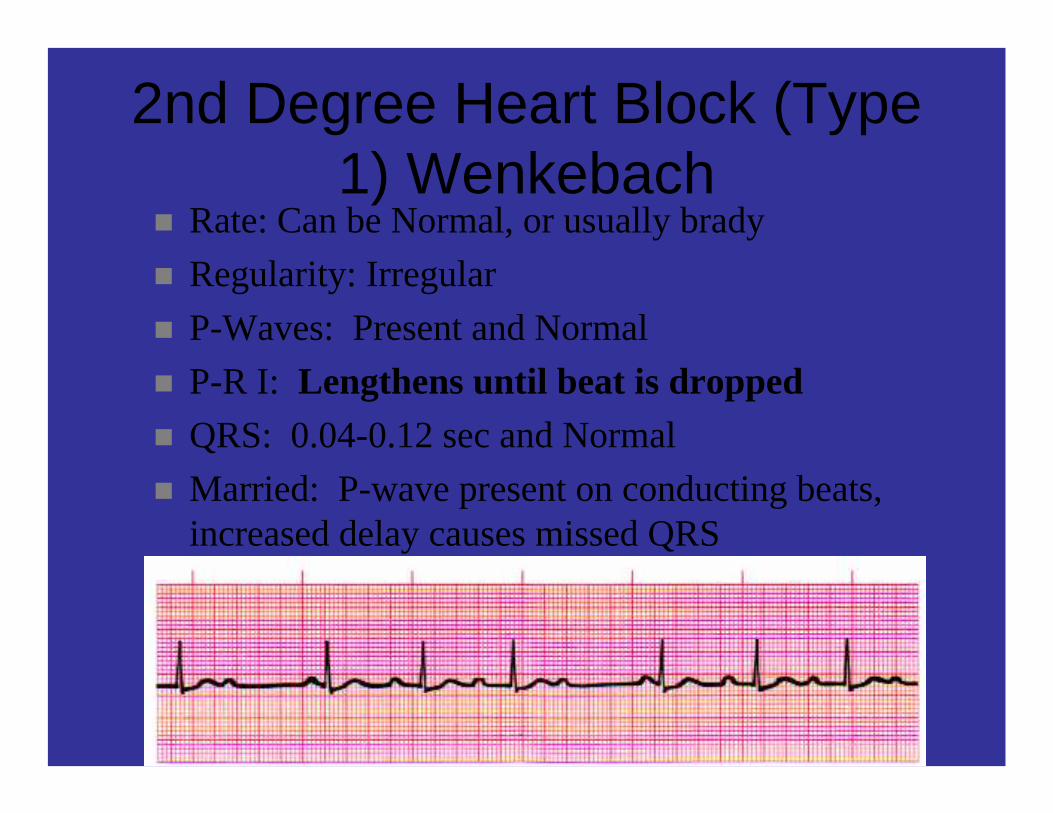
2nd Degree Heart Block (Type 1) Wenkebach
Rate: Can be Normal, or usually bradyRegularity: IrregularP-Waves: Present and NormalP-R I: Lengthens until beat is droppedQRS: 0.04-0.12 sec and NormalMarried: P-wave present on conducting beats, increased delay causes missed QRS

2nd Degree Heart Block (Type 2)
Mobitz IIRate: Less than 60Regularity: IrregularP-Waves: Present, 2:1, 3:1, 4:1P-R I: 0.12-0.20 sec on conducting beatQRS: 0.04-0.12 sec, may begin to widenMarried: P-wave for every QRS and extras depending on conduction ratio
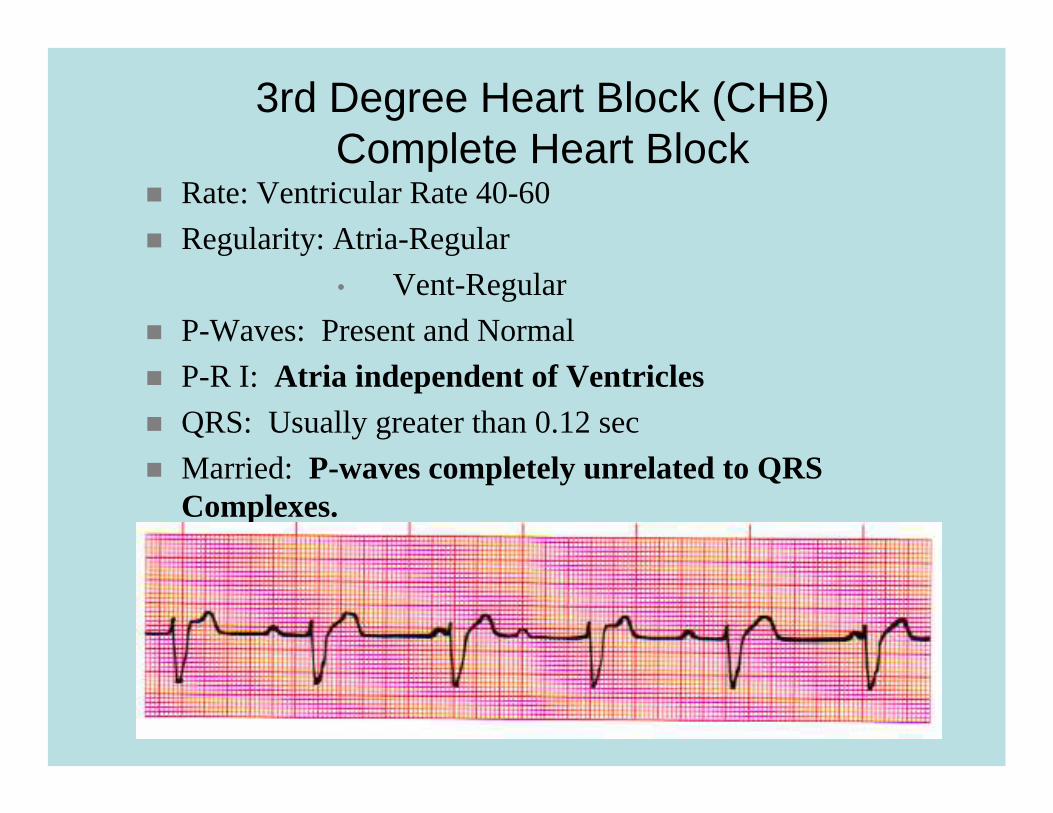
3rd Degree Heart Block (CHB)Complete Heart Block
Rate: Ventricular Rate 40-60Regularity: Atria-Regular
• Vent-RegularP-Waves: Present and NormalP-R I: Atria independent of VentriclesQRS: Usually greater than 0.12 secMarried: P-waves completely unrelated to QRS Complexes.

Complete Heart Block

Junctional RhythmRate: 40-60Regularity: RegularP-Waves: Inverted, Retrograde or AbsentP-R I: Shortened or absentQRS: 0.04-0.12 secMarried: P-wave for every QRS, sometimes not visible

Junctional
Junctional Accelerated Rhythm
Rate: 60-100Regularity: RegularP-Waves: Inverted, Retrograde or AbsentP-R I: Shortened or absentQRS: 0.04-0.12 secMarried: P-wave for every QRS, sometimes not visible

Junctional Tachycardia
Rate: 100-140Regularity: RegularP-Waves: Inverted, Retrograde or AbsentP-R I: Shortened or absentQRS: 0.04-0.12 secMarried: P-wave for every QRS, sometimes not visible

Ventricular TachycardiaRate: 100-220Regularity: RegularP-Waves: NoneP-R I: NoneQRS: Greater than 0.12 secMarried: NO
We’ll look at Torsades de Pointes in Lab
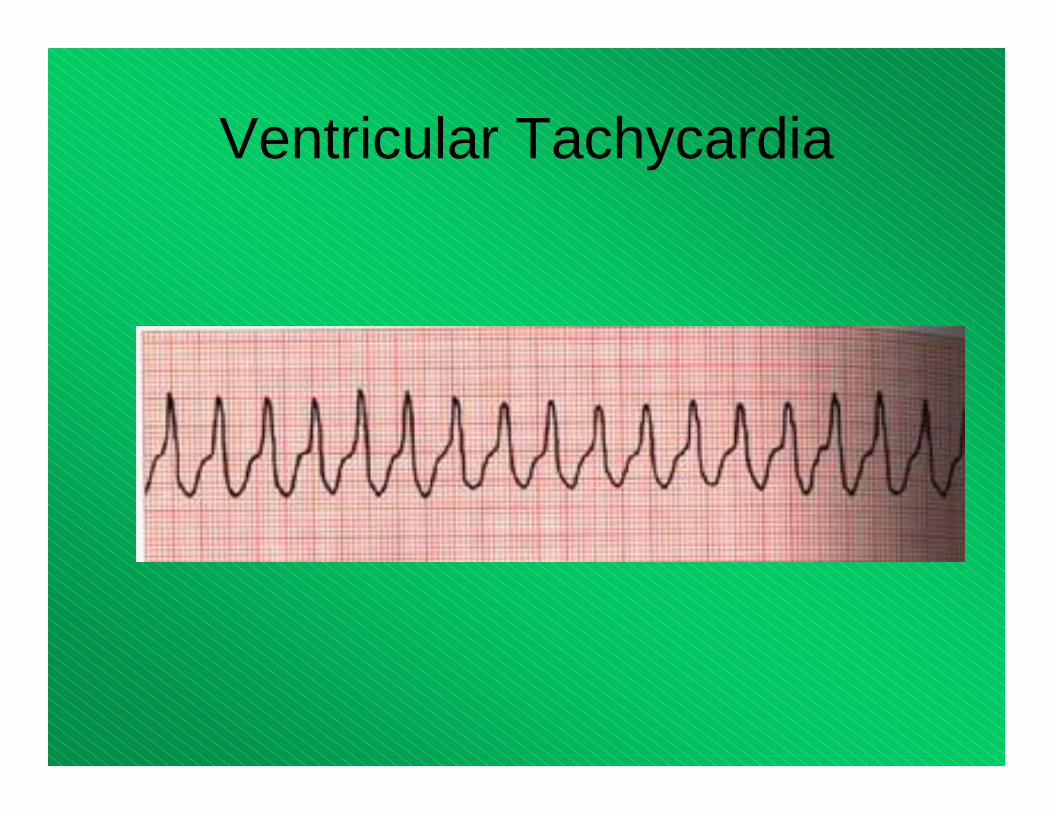
Ventricular Tachycardia
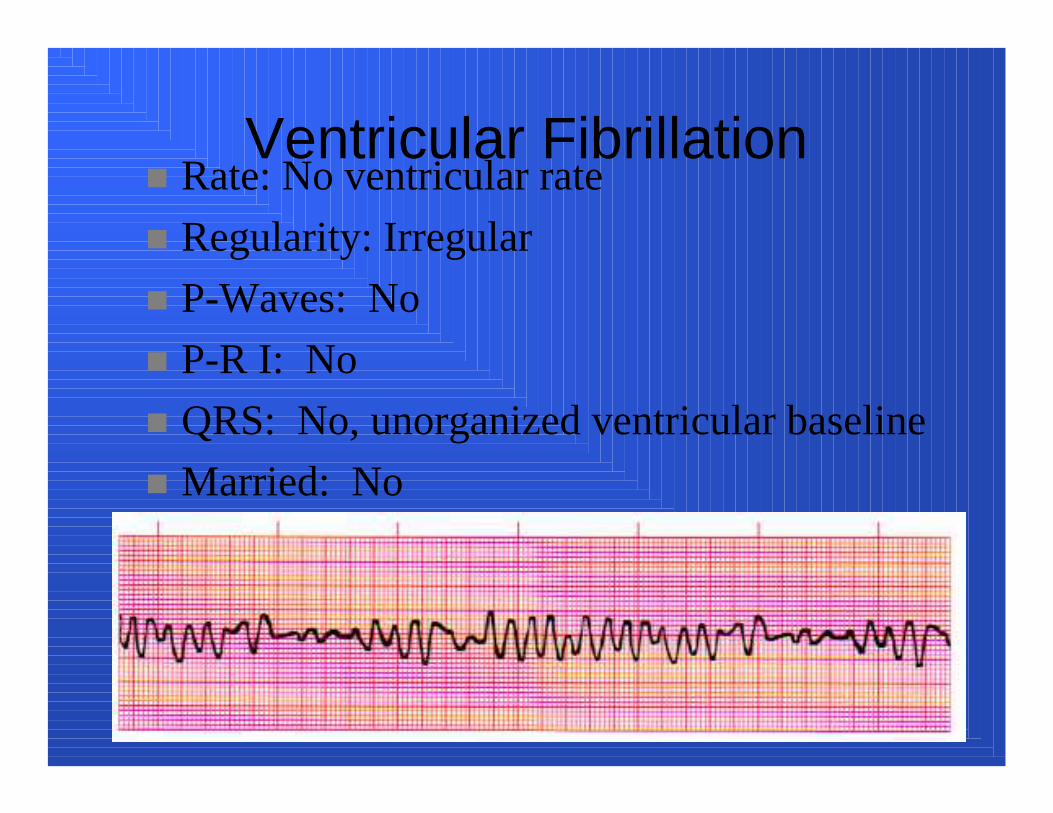
Ventricular FibrillationRate: No ventricular rateRegularity: IrregularP-Waves: NoP-R I: NoQRS: No, unorganized ventricular baselineMarried: No

Ventricular Fibrillation

Asystole
Rate: 0Regularity: N/AP-Waves: NoneP-R I: N/AQRS: NoneMarried: No (verify a second lead)

Asystole
Agonal / Idioventricular
Rate: 20-40Regularity: IrregularP-Waves: NoneP-R I: N/AQRS: Wider than 0.12 secMarried: NO (a dying heart)

Idioventricular
• Less regular than this!

Exceptions / Disruptions
• Premature Ventricular Contractions• Premature Atrial Contractions• Bundle Branch Blocks• Pacer Considerations (Atrial, Ventricular or
Both)

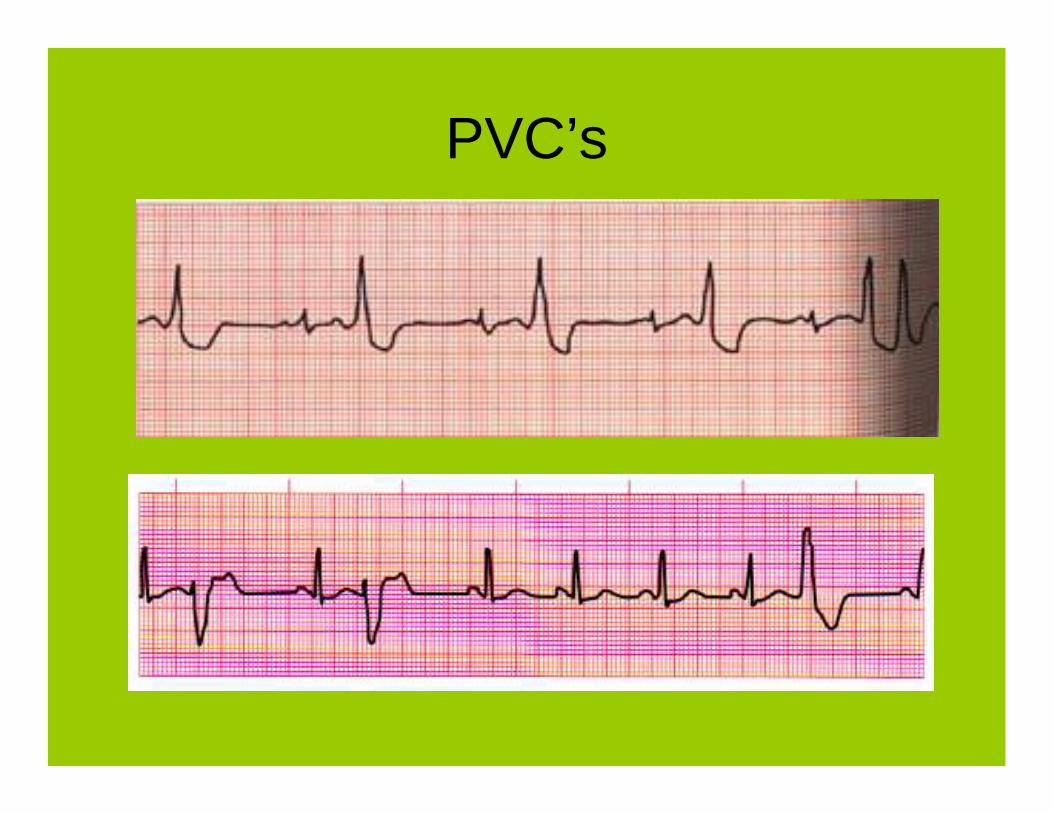
Premature Ventricular Contractions
• Wide, Bizarre QRS Complex• Always identify the underlying rhythm first• Can appear in couplets, triplets, short runs
of V-Tach, bigeminy and trigeminy• Can be uni-focal or multi-focal• Caused by random firing within the
ventricles• Not accompanied by a P-wave
PVC’s
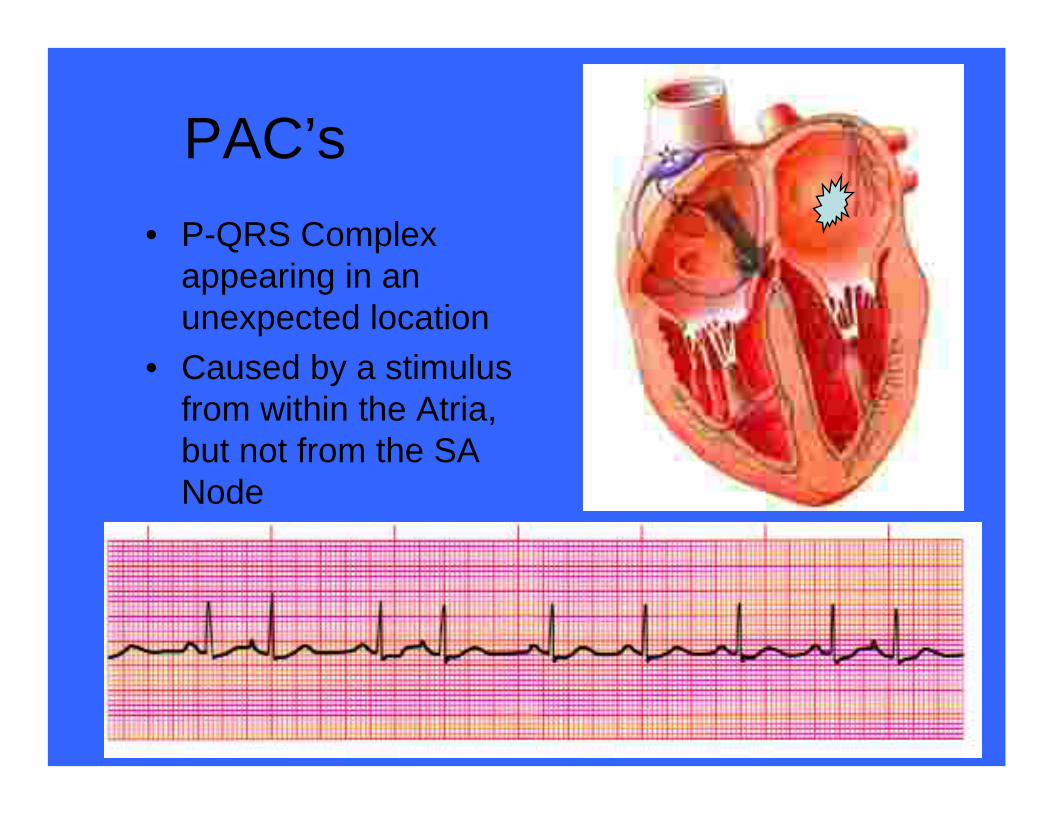
PAC’s• P-QRS Complex
appearing in an unexpected location
• Caused by a stimulus from within the Atria, but not from the SA Node

PJC
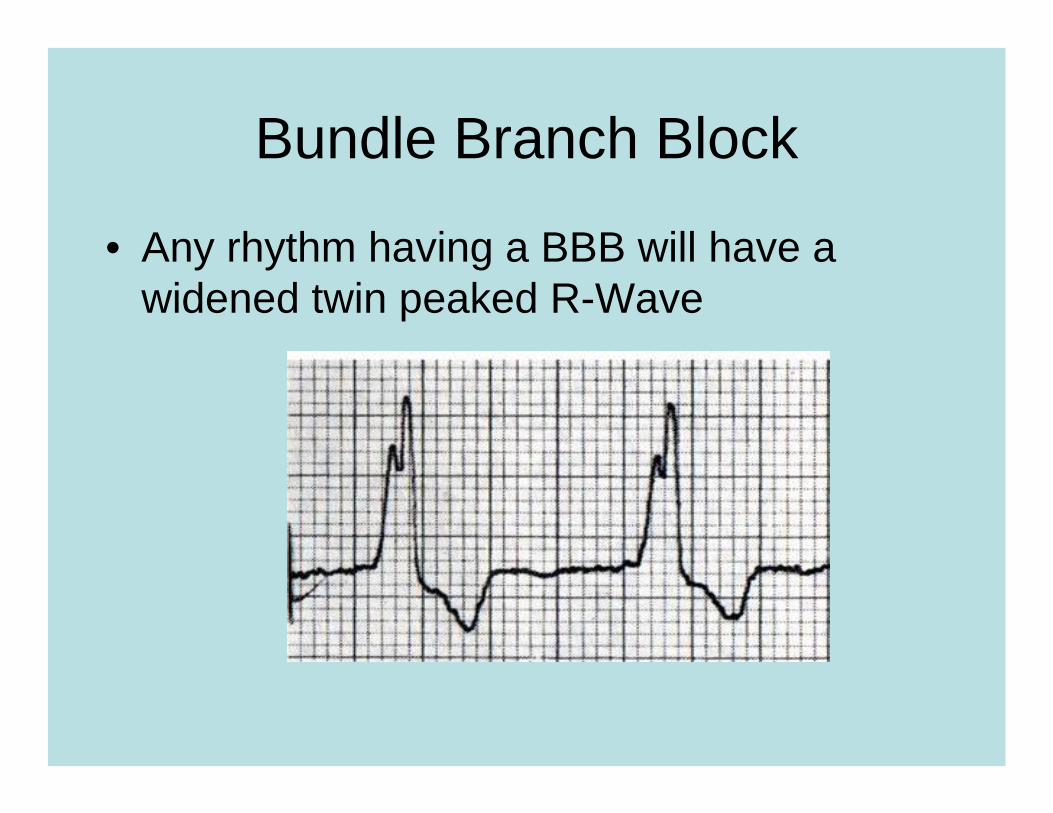
Bundle Branch Block
• Any rhythm having a BBB will have a widened twin peaked R-Wave

Paced Rhythms
• Patients may have various types of pacemakers
• Atrial • Ventricular• Both• Vertical spike on monitor is an indicator

Paced Rhythms Various

Artifact
• 60 Cycle Interference
• Loose Leads/Moving Ambulance

Rhythm Interpretation and Patient Assessment

A 68 year-old female complains of shortness of breath for the last day. She is feverish and has a
productive cough. Her BP is 164/78, HR matches with the ECG below, and RR of 20. She speaks in 6 word-sentences. She has rhonchi in her right lung. Her past medical history includes an MI 4 years ago and mild
hypertension.
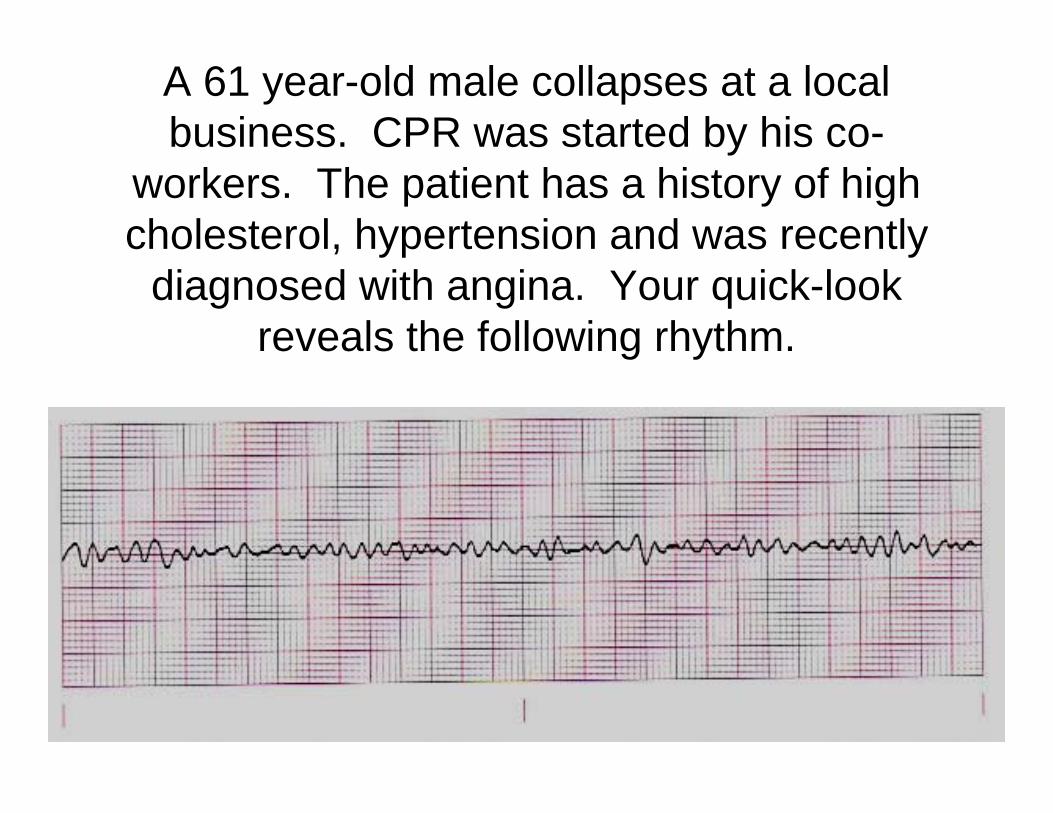
A 61 year-old male collapses at a local business. CPR was started by his co-
workers. The patient has a history of high cholesterol, hypertension and was recently
diagnosed with angina. Your quick-look reveals the following rhythm.

A 65 year-old male calls for weakness. The patient states that he has been feeling this way over the
last 2 days and becomes more short of breath with activity. He also becomes dizzy when he stands up. The patient has a history of COPD and is on
home oxygen at 2 liters/minute. His BP is 128/84, RR 22 with some pursed-lip breathing. He states
that he has a history of “skipped heart beats.” Lung sounds reveal wheezes in the mid-lobes and bases. He takes Alupent, prednisone, Altace and Cozaar.

A 78 year-old male is found unconscious in his bed. He was last seen the night before by his family. As you move him to the floor, you see that a bottle of nitroglycerin falls out of the bed and onto the floor. The patient is warm but his
back reveals mottling. He is pulseless and apneic.

You respond to a 58 year-old male in cardiac arrest. The patient’s daughter tells you that he
didn’t feel well for the last few days. She also states that he is a chronic alcoholic.
The patient is lying in his bed, pale-gray in color and apneic. He is also pulselessness. His
abdomen is distended and he has large blood stains on his pillow.
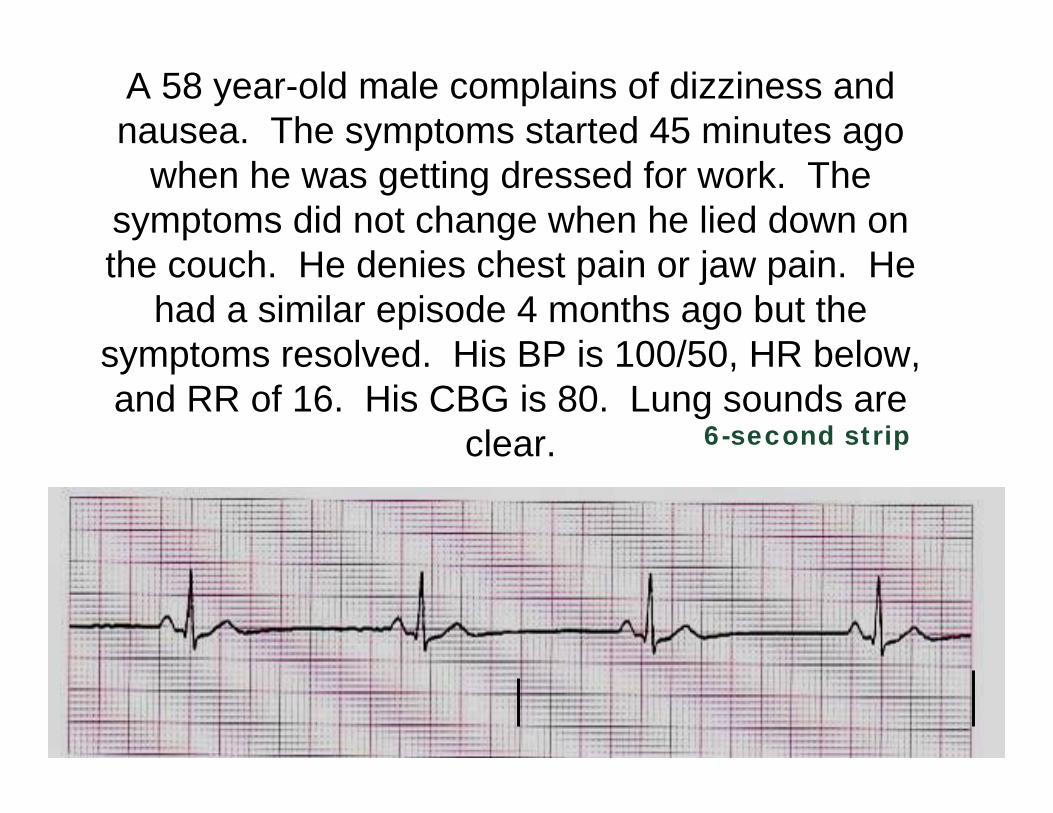
A 58 year-old male complains of dizziness and nausea. The symptoms started 45 minutes ago
when he was getting dressed for work. The symptoms did not change when he lied down on the couch. He denies chest pain or jaw pain. He
had a similar episode 4 months ago but the symptoms resolved. His BP is 100/50, HR below, and RR of 16. His CBG is 80. Lung sounds are
clear. 6-second strip
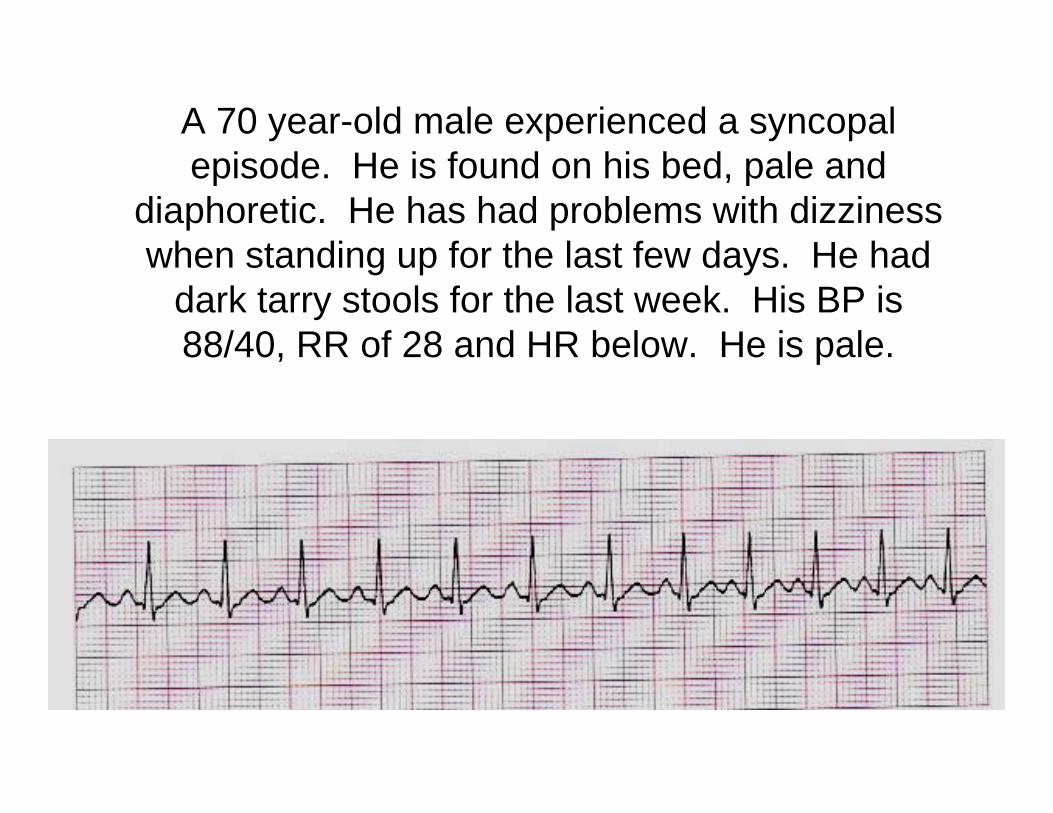
A 70 year-old male experienced a syncopalepisode. He is found on his bed, pale and
diaphoretic. He has had problems with dizziness when standing up for the last few days. He had
dark tarry stools for the last week. His BP is 88/40, RR of 28 and HR below. He is pale.
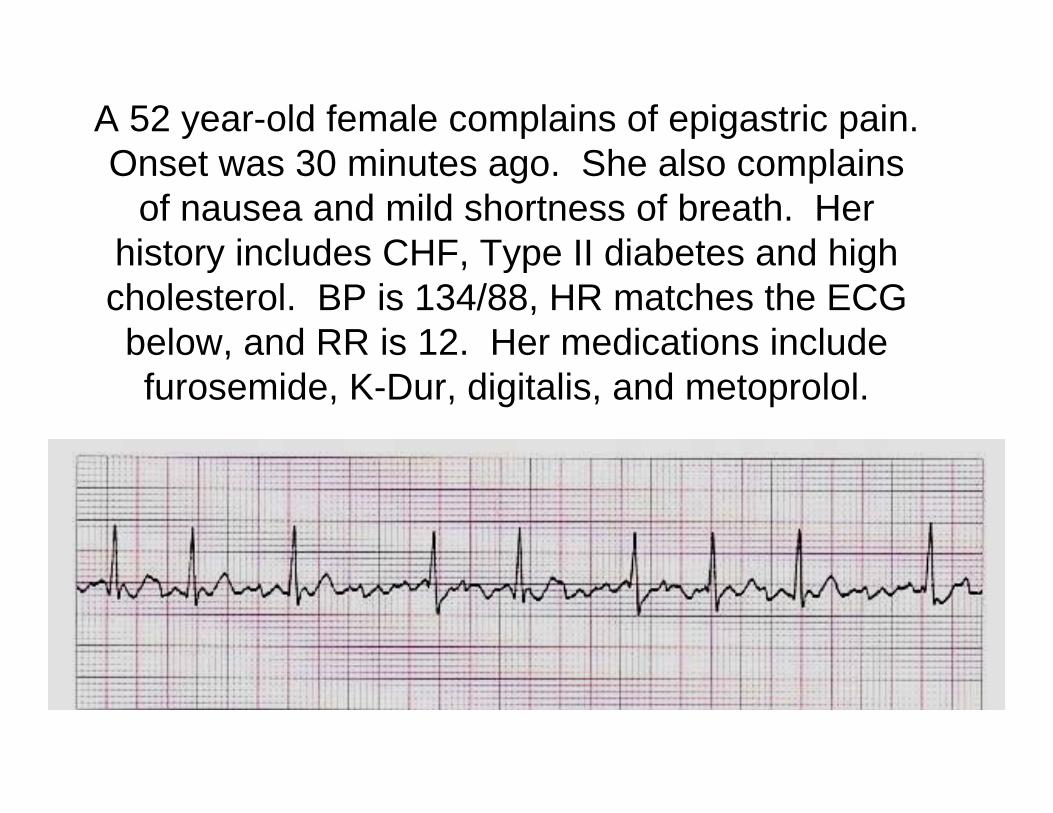
A 52 year-old female complains of epigastric pain. Onset was 30 minutes ago. She also complains
of nausea and mild shortness of breath. Her history includes CHF, Type II diabetes and high cholesterol. BP is 134/88, HR matches the ECG below, and RR is 12. Her medications include furosemide, K-Dur, digitalis, and metoprolol.
And Now For the Summary
• The ECG should confirm what you know about the patient– V-fib for dead folks– Tachycardia for dehydration– PVCs for chronic heart conditions– AV blocks – chronic or acute conditions
• Treat the rhythm in perspective– Underlying cause – drug overdose, hypovolemia

Sources – In order of preference
• Many of the pictures and info from:– Flip and See ECG, 2nd Edition
• Cohn/Gilroy-Doohan– A great resource
– Paramedic Paramedic Textbook, Revised 2nd Edition• Mick J. Sanders, Mosby
– ECG’s Made Easy, 2nd Edition• Barbara Aehlert, RN, Mosby
– Basic Dysrhythmias, Interpretation and Management, 3rd Edition
• Robert J. Huszar, Mosby

















