EKG Recognition: When to Worry Roslinde M. Collins, MD, D,ABSM, FCCP, FAASM Medical Director, Center for Sleep Disorders at Rutland Regional Medical Center in Vermont [email protected]NEPS Conference September 14, 2012
Transcript
EKG Recognition: When to Worry
Roslinde M. Collins, MD, D,ABSM, FCCP, FAASM
Medical Director, Center for Sleep Disorders at Rutland Regional Medical Center in Vermont
• To gain basic understanding of the electricity of the heart
• To review patterns of arrhythmias
• To know when a rhythm is life threatening or potentially life threatening
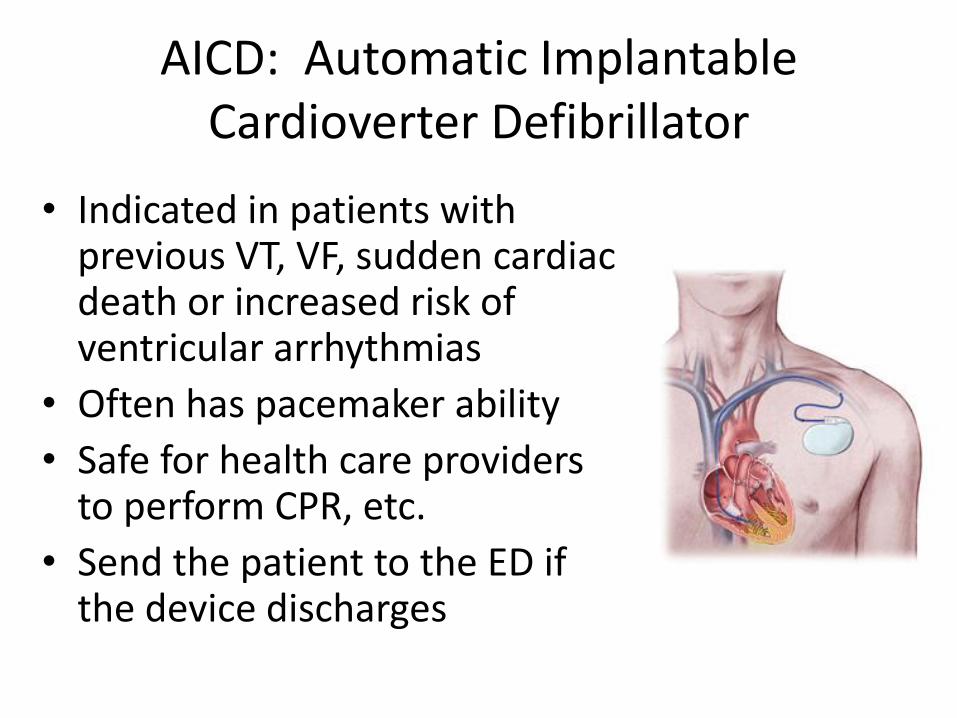
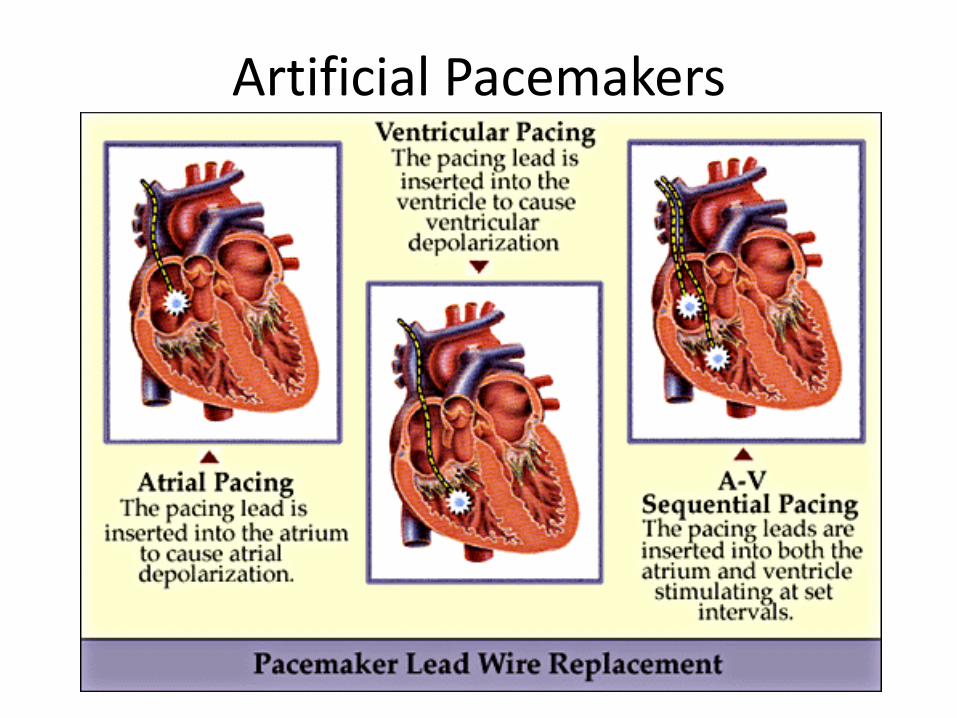
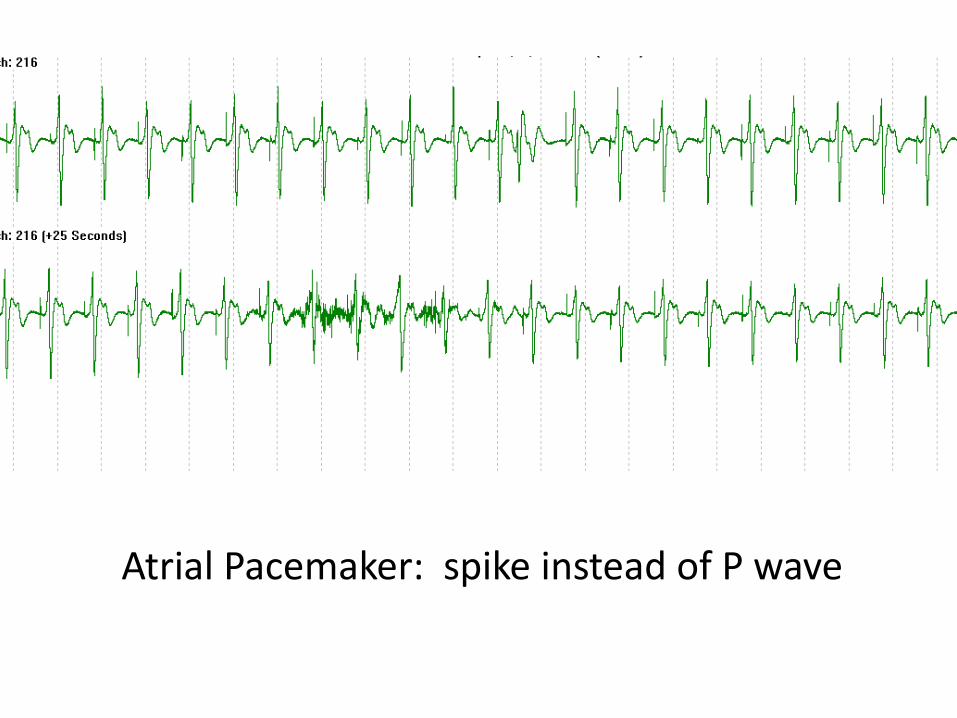
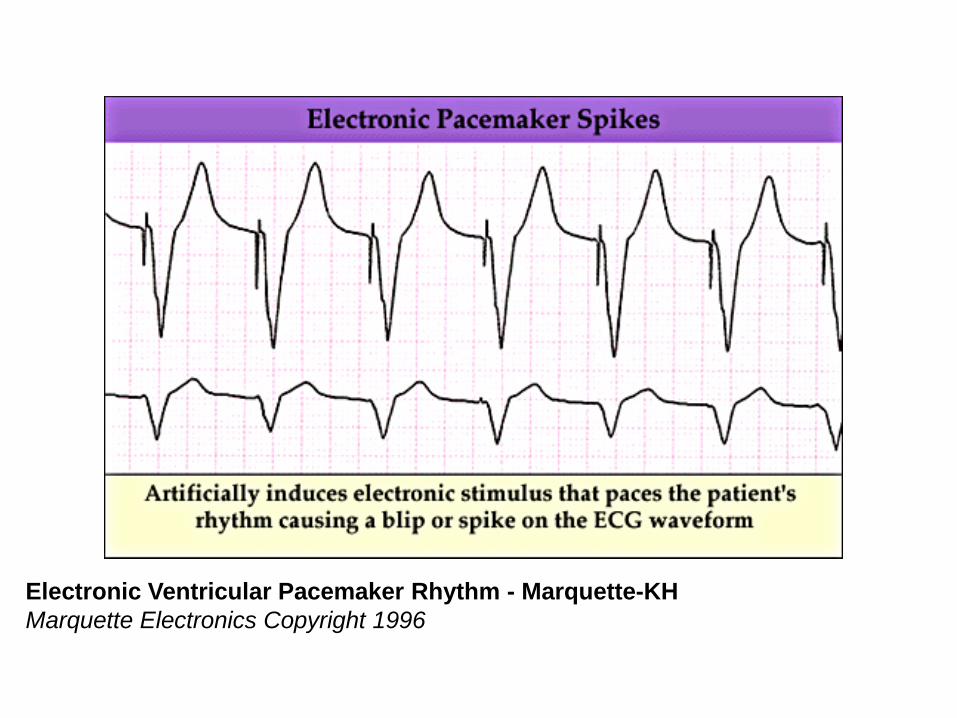
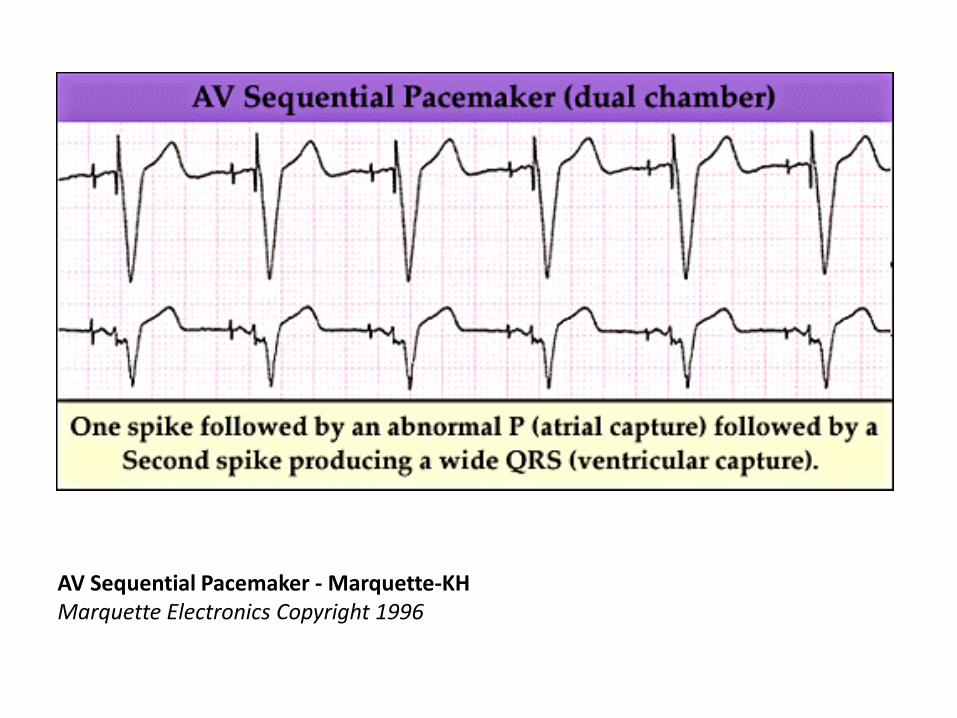
• Review special cases such as artificial pacemakers and AICDs
Case #1: Spike Jonze
Lessons Learned from Case #1:
• Keep an eye on your monitors
• It is helpful to hear your alarms
• No singing and dancing and fooling around in the trauma (control) room
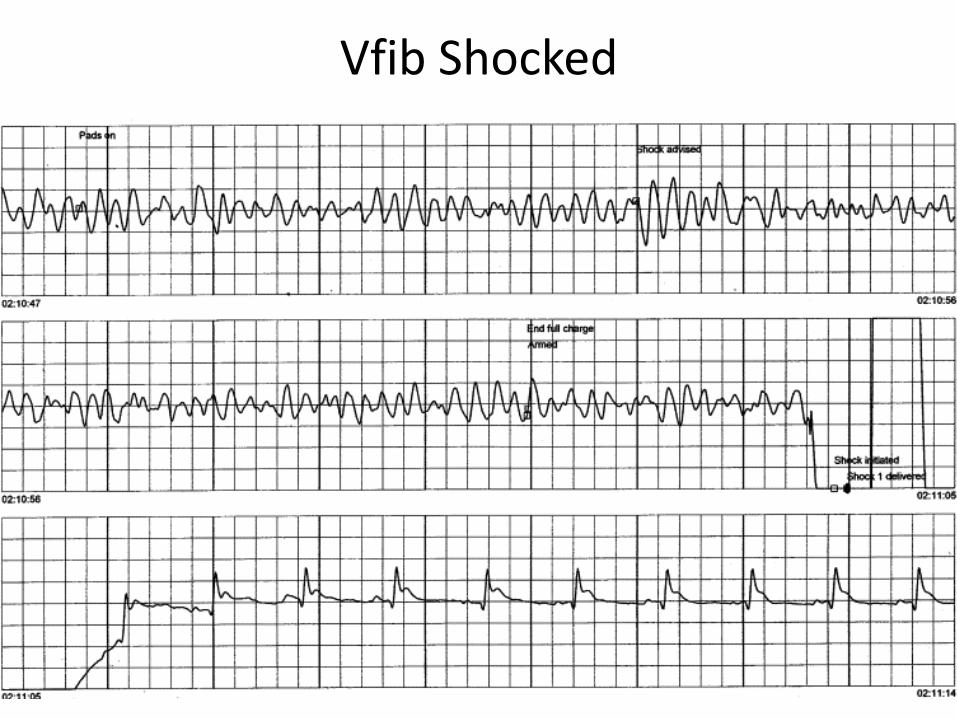
• Don’t shock asystole
AASM Cardiac Scoring Rules
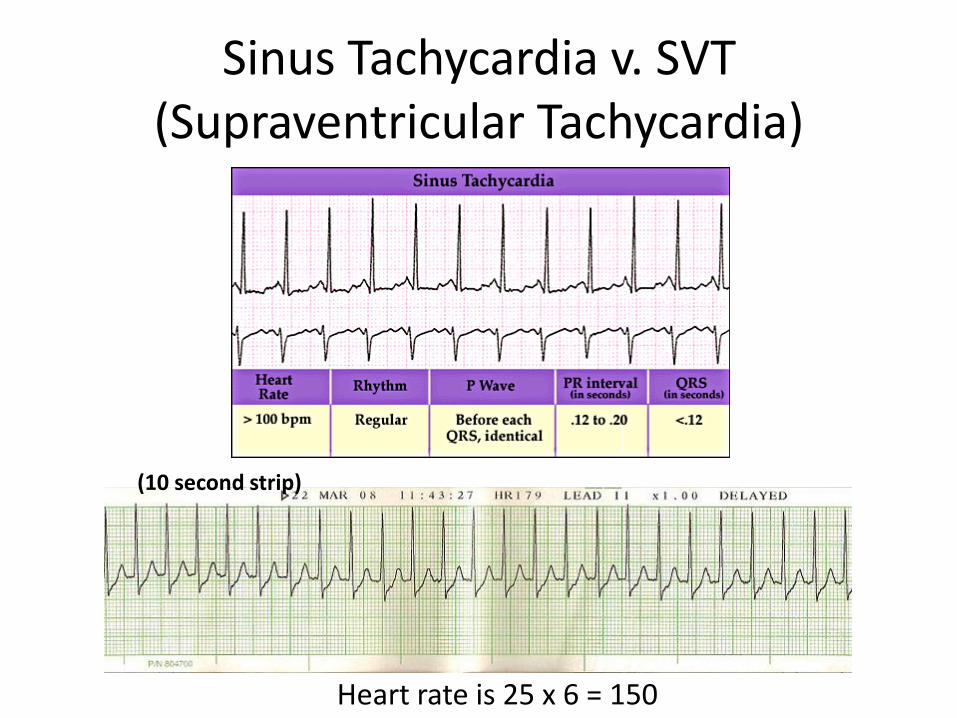
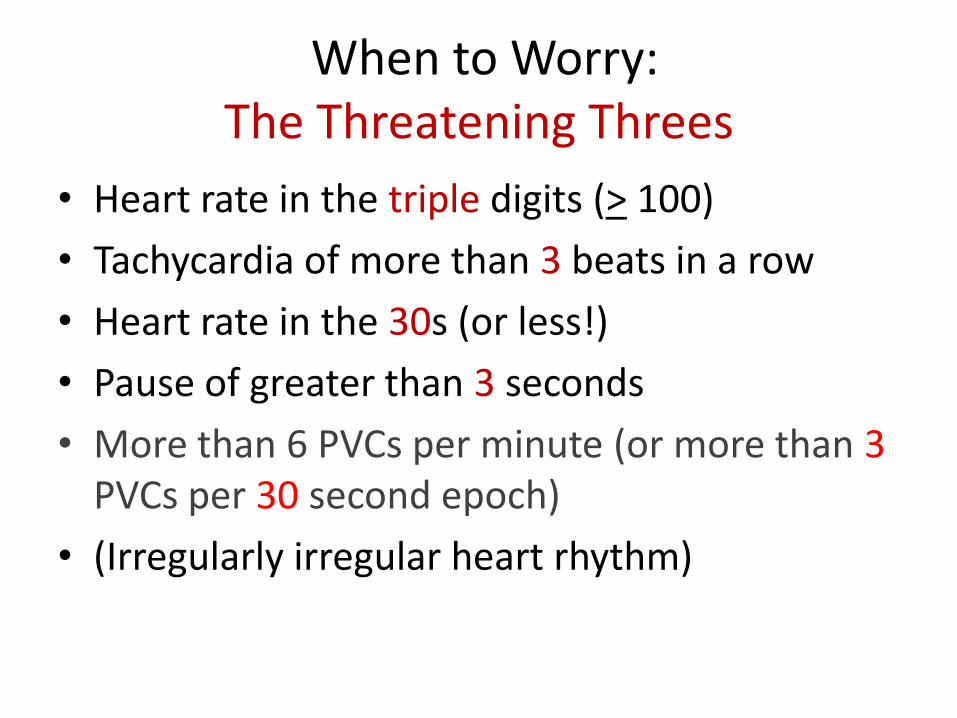
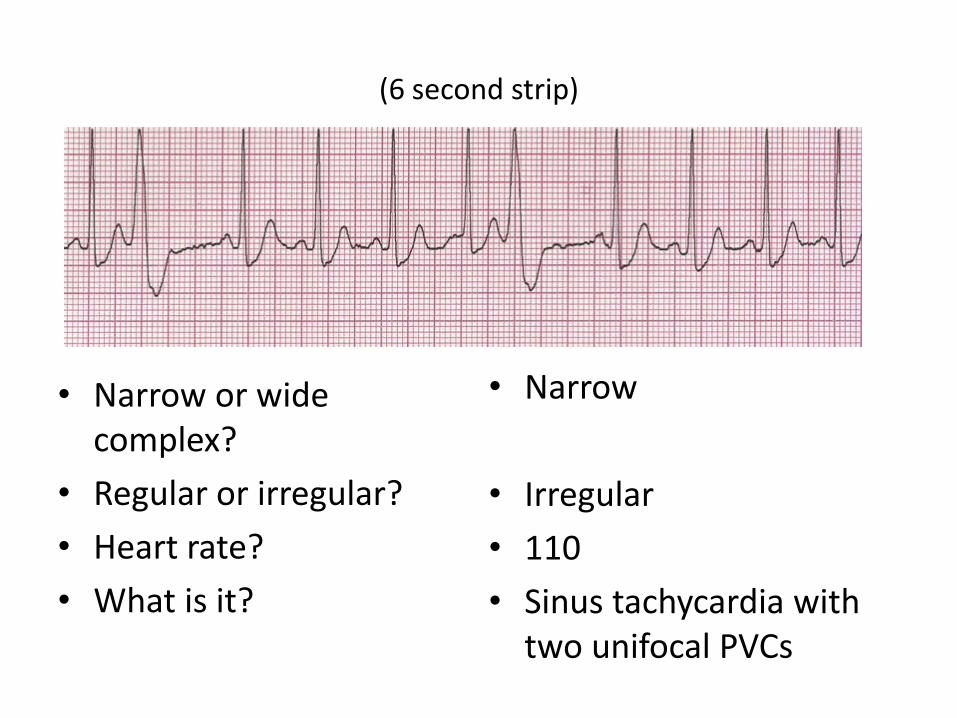
• Score sinus tachycardia during sleep for a sustained sinus heart rate of greater than 90 beats per minute (bpm) for adults
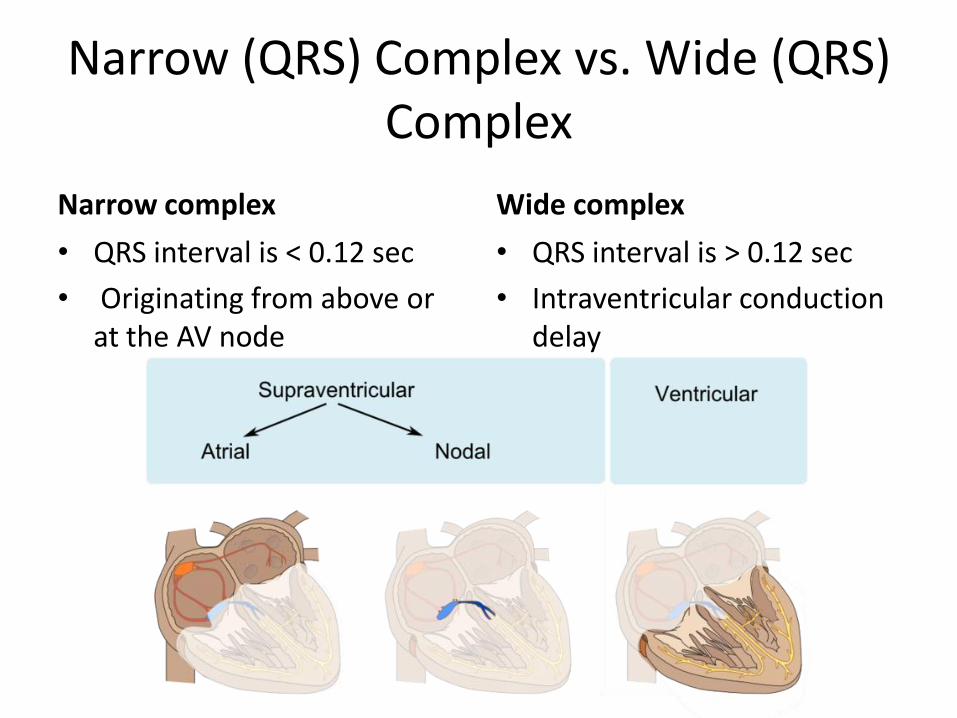
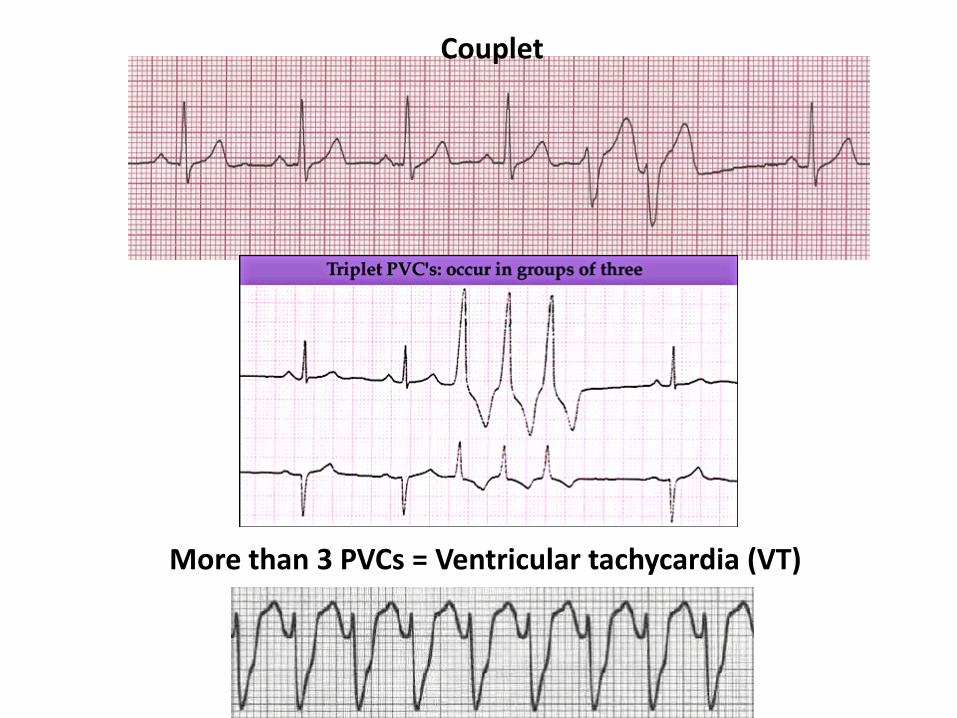
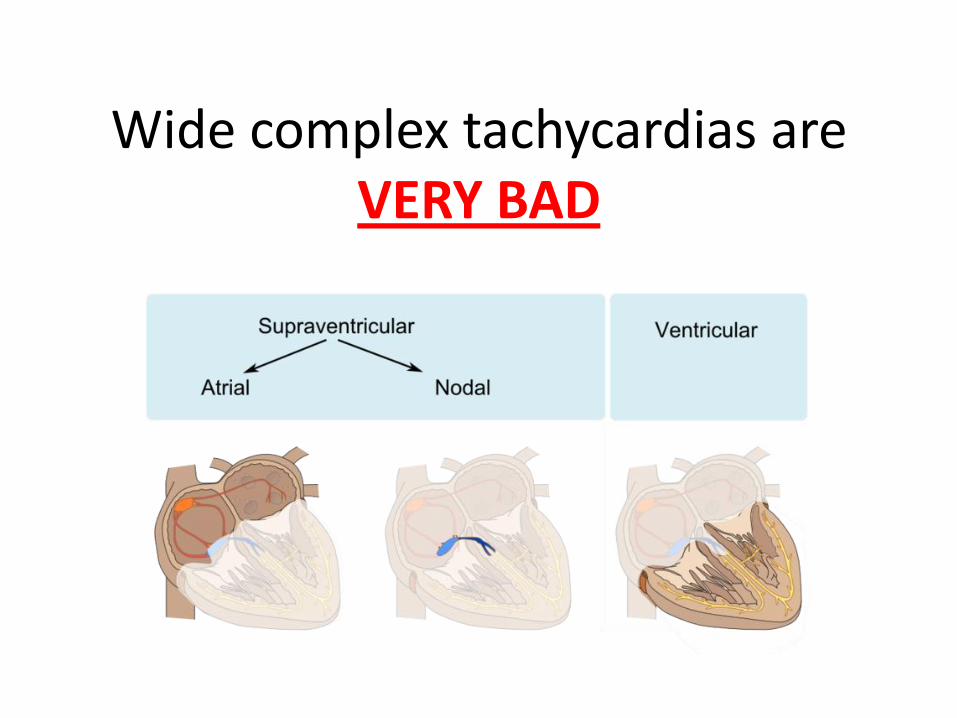
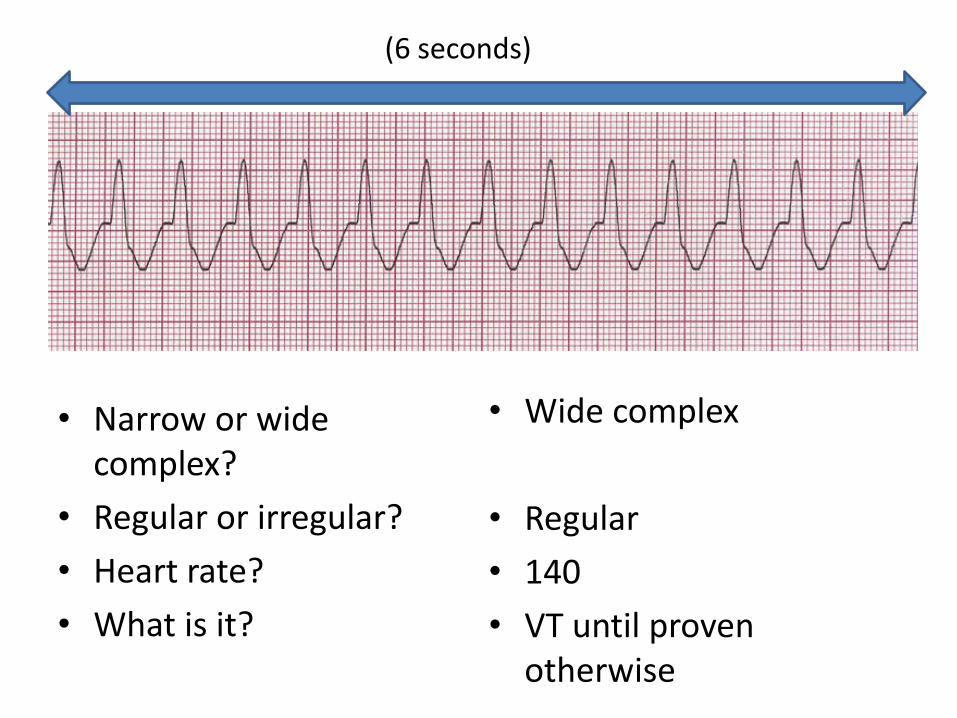
• Score wide complex tachycardia for a rhythm lasting a minimum of 3 consecutive beats at a rate of greater than 100 bpm with QRS duration of greater than or equal to 120 msec
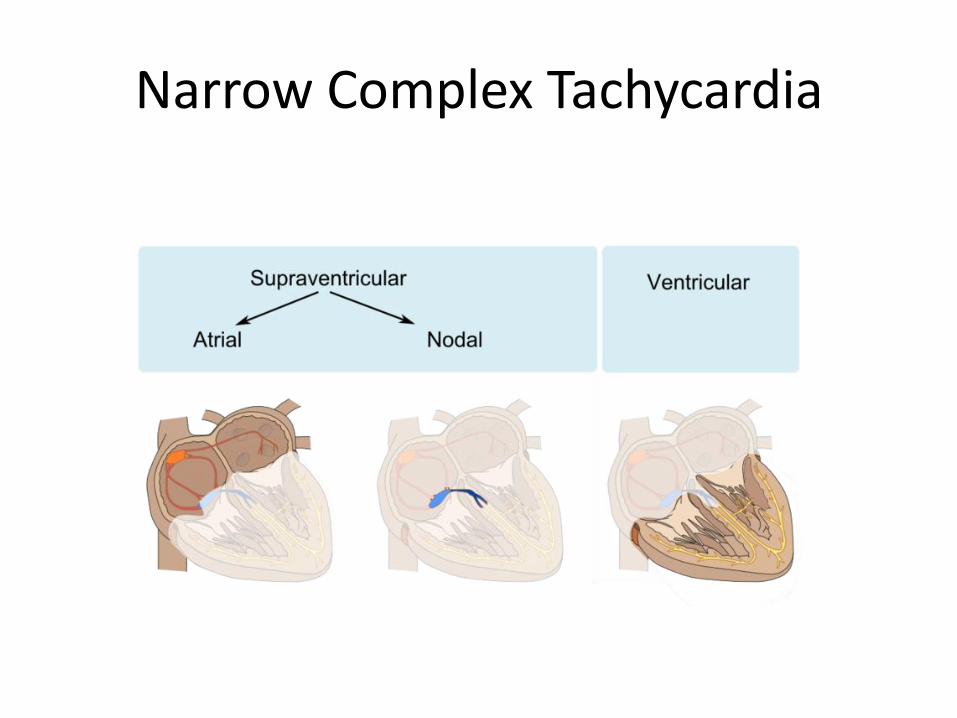
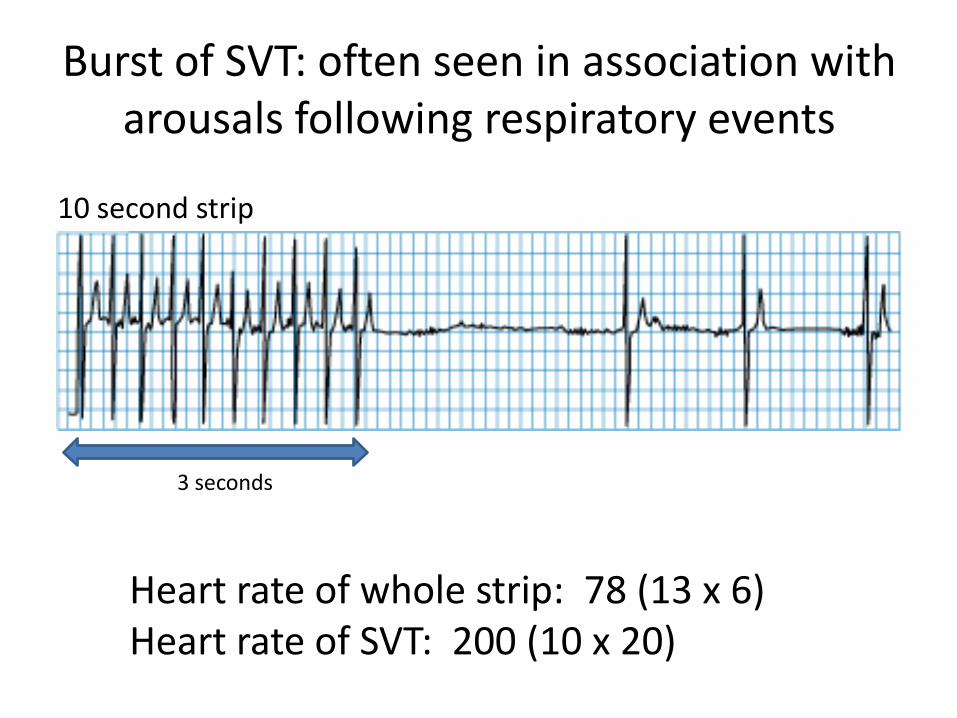
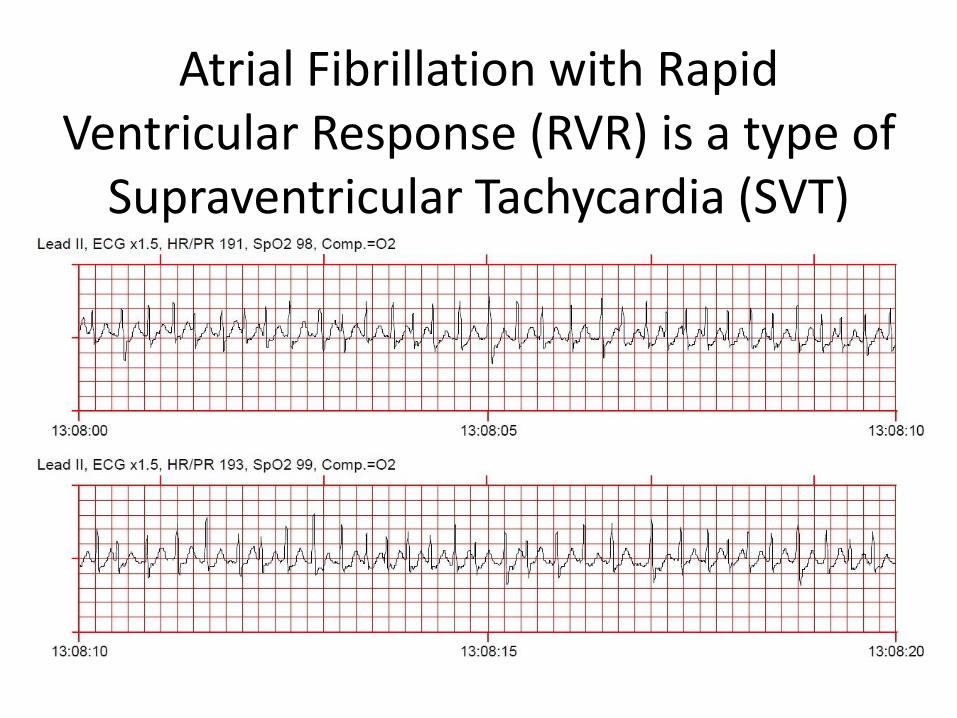
• Score narrow complex tachycardia for a rhythm lasting a minimum of 3 consecutive beats at a rate of greater than 100 bpm with QRS duration of less than 120 msec
AASM Cardiac Scoring Rules (cont.)
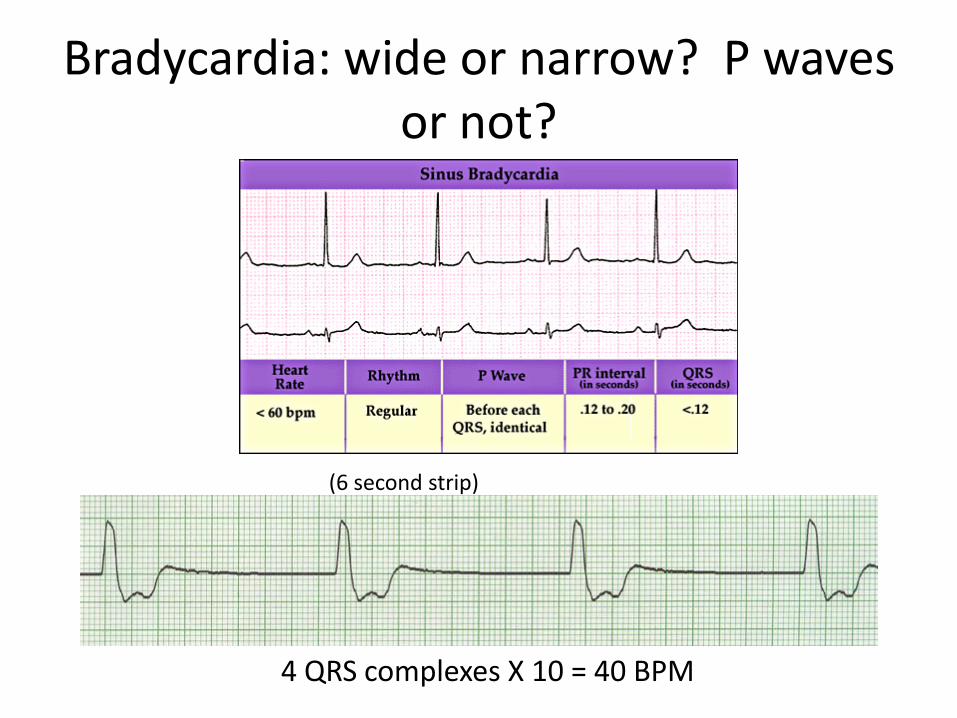
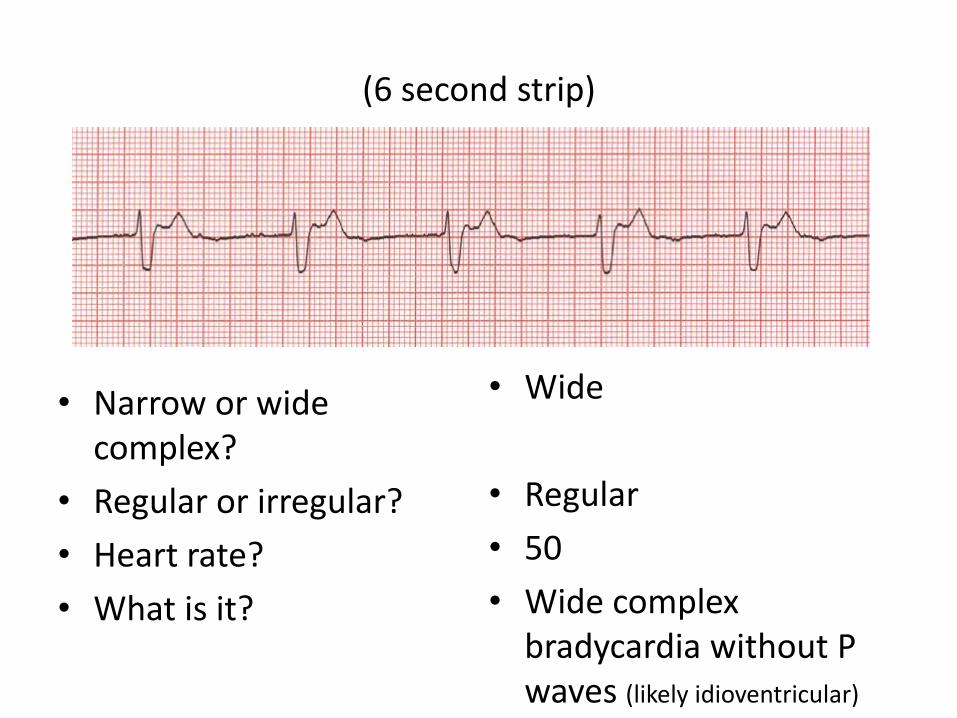
• Score bradycardia during sleep for a sustained heart rate of less than 40/minute for ages 6 years through adult
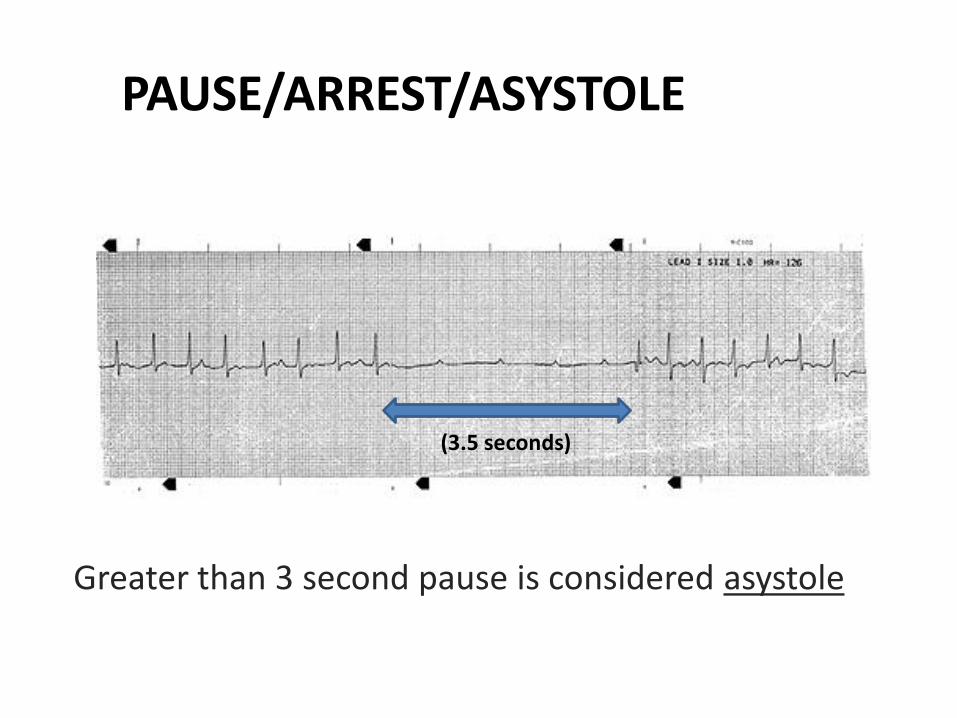
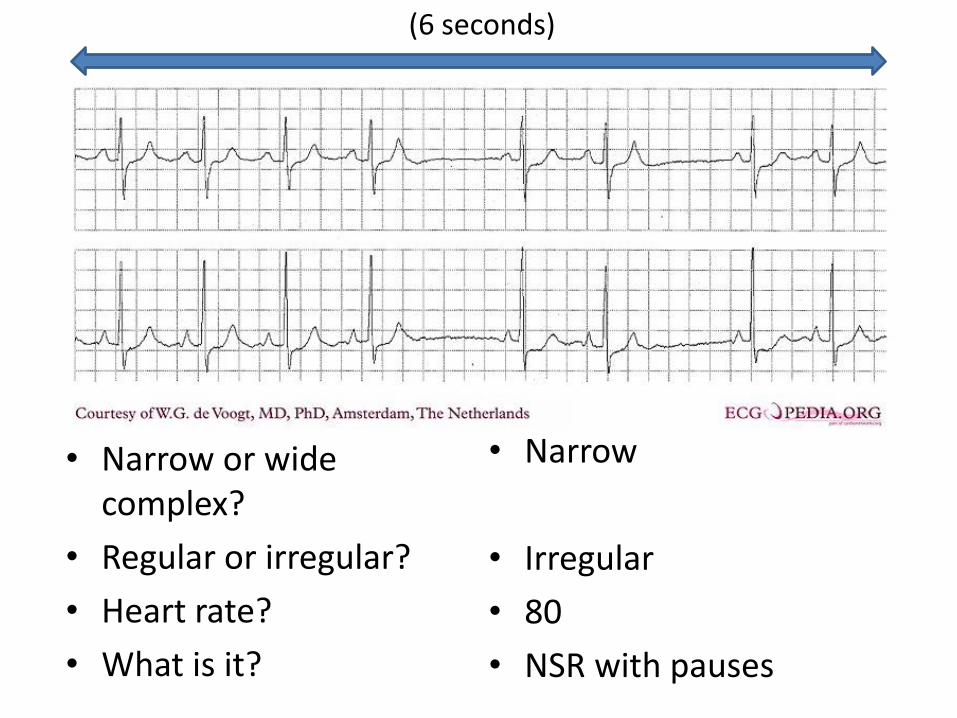
• Score asystole for cardiac pauses greater than 3 seconds for ages 6 years through adult
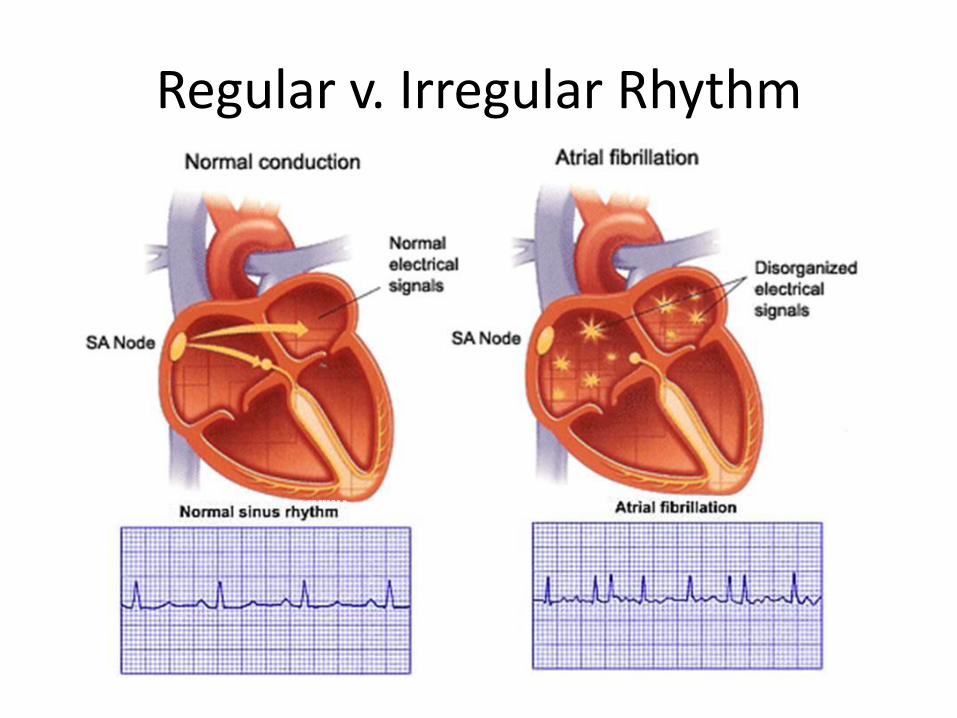
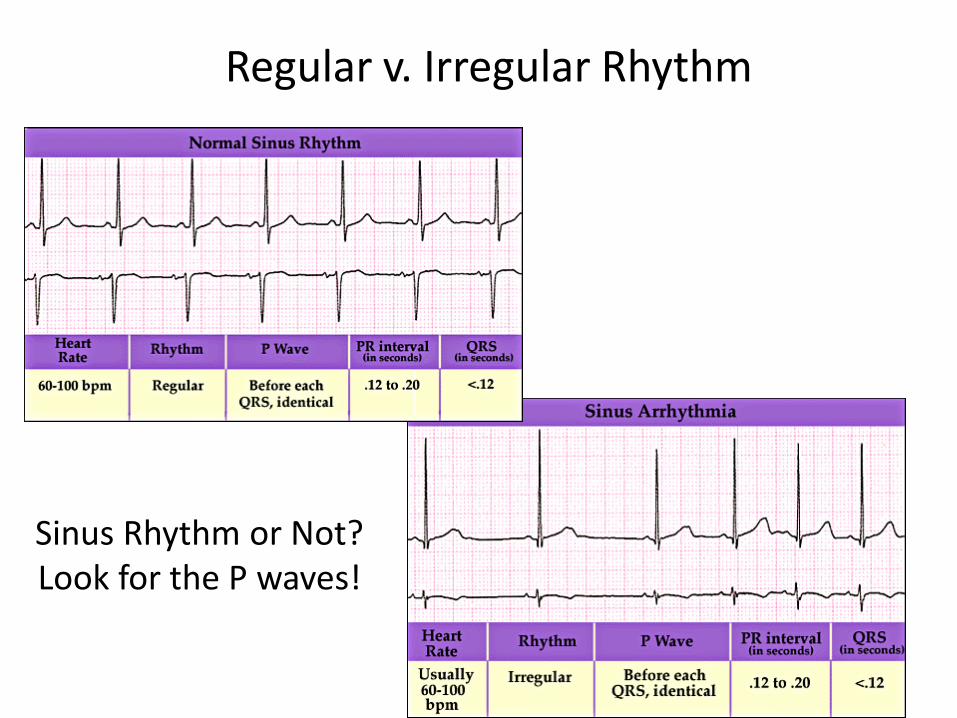
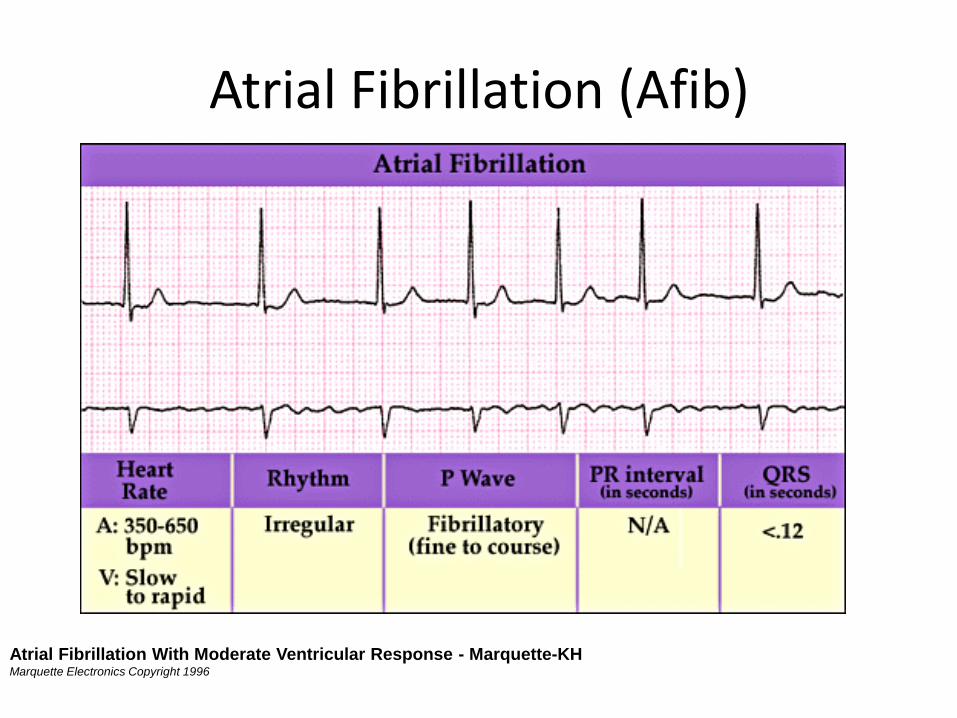
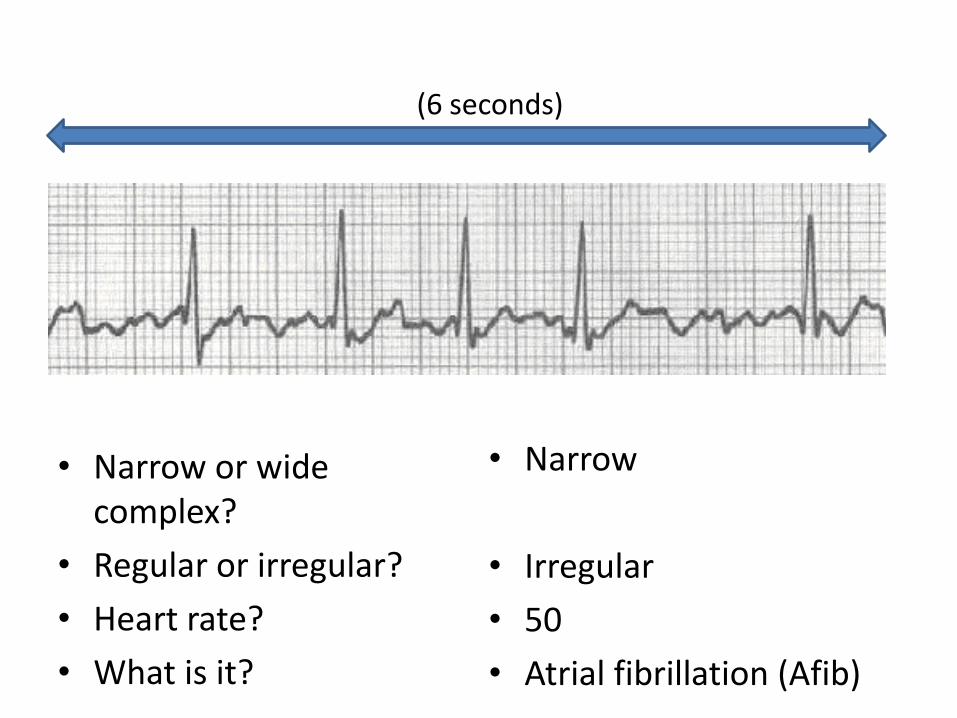
• Score atrial fibrillation if there is an irregularly irregular ventricular rhythm associated with replacement of consistent P waves by rapid oscillations that vary in size, shape , and timing
EKG Basics
EKG=
Electrocardiogram=
ECG
ECG Intervals and Waves-KH Frank G. Yanowitz, M.D., copyright 1997
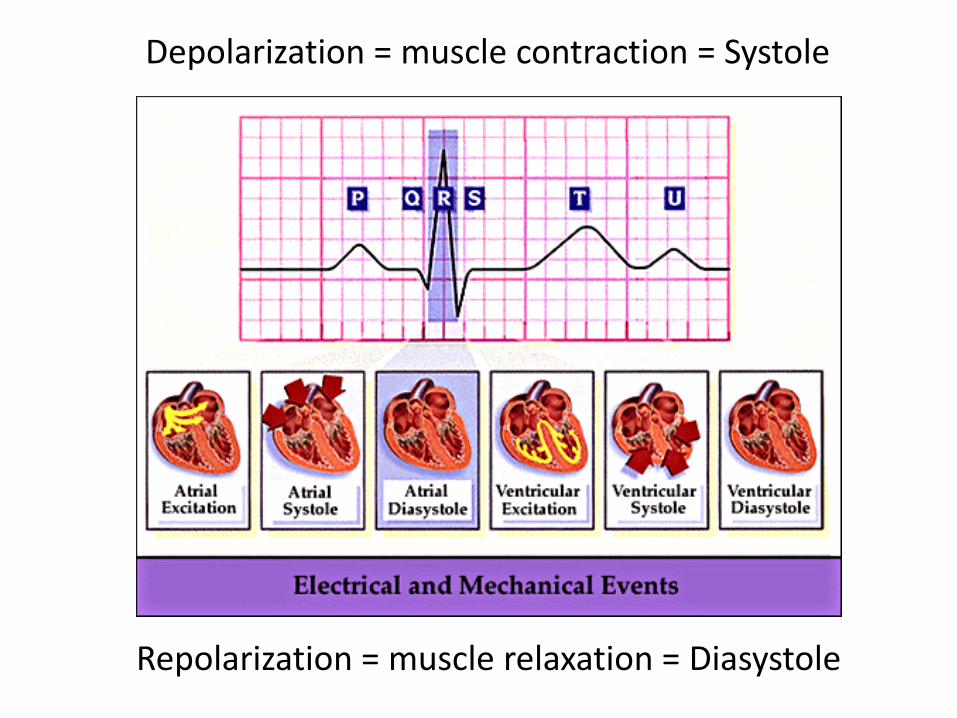
The EKG complex
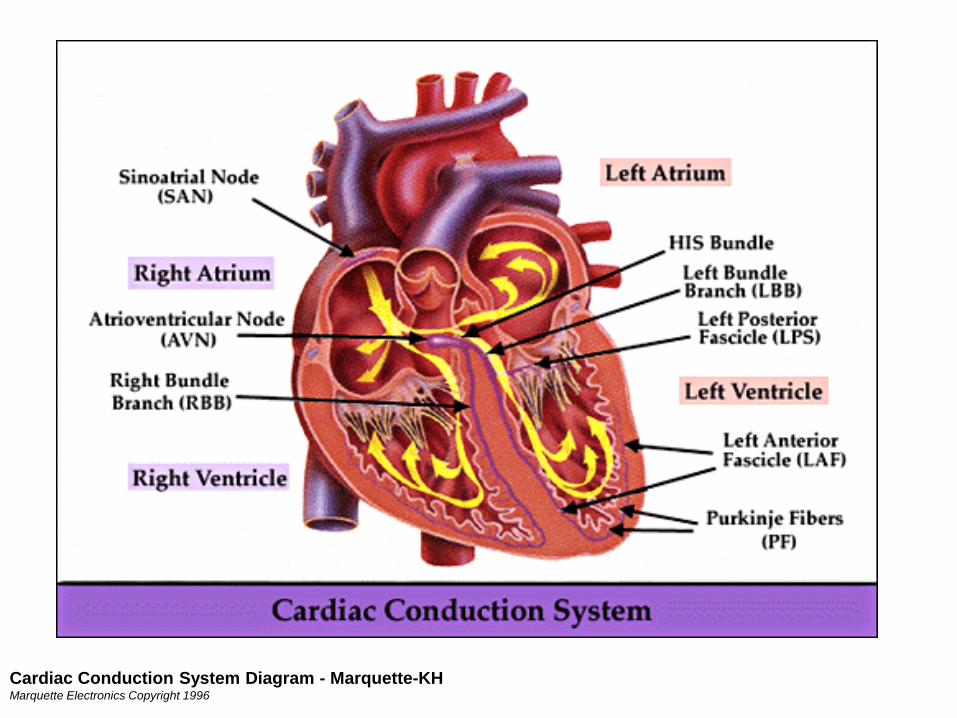
Cardiac Conduction System Diagram - Marquette-KH Marquette Electronics Copyright 1996
Depolarization = muscle contraction = Systole
Repolarization = muscle relaxation = Diasystole
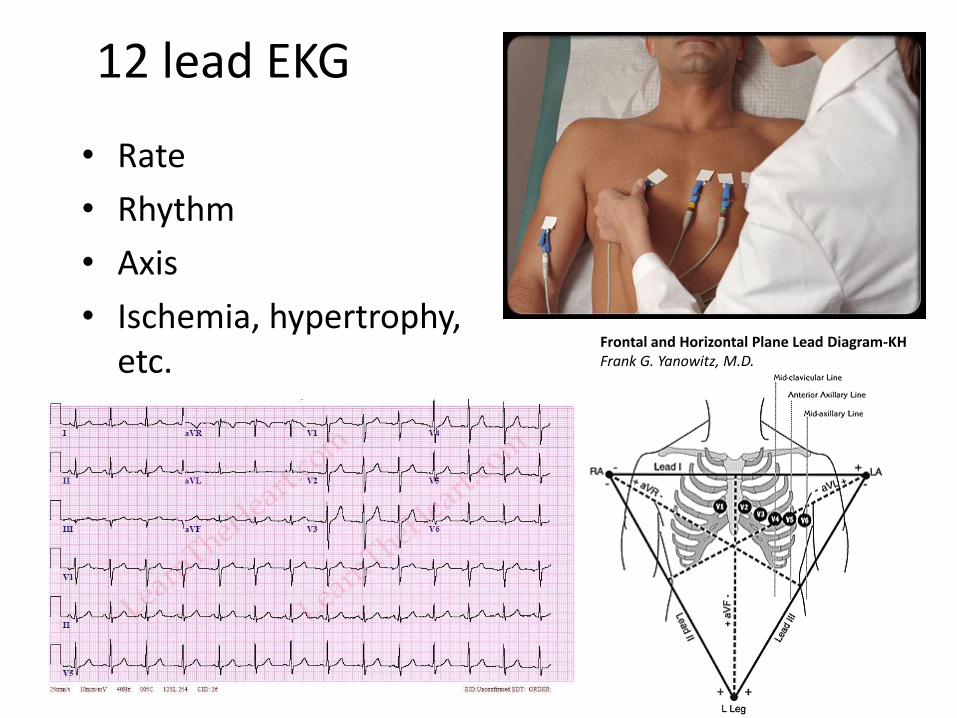
12 lead EKG
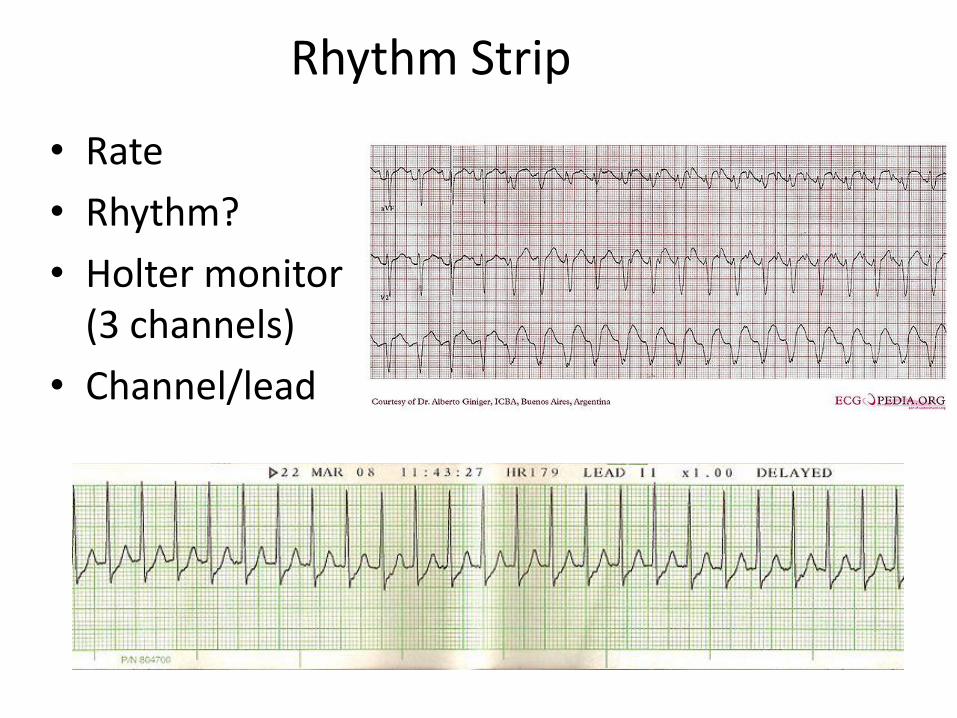
• Rate
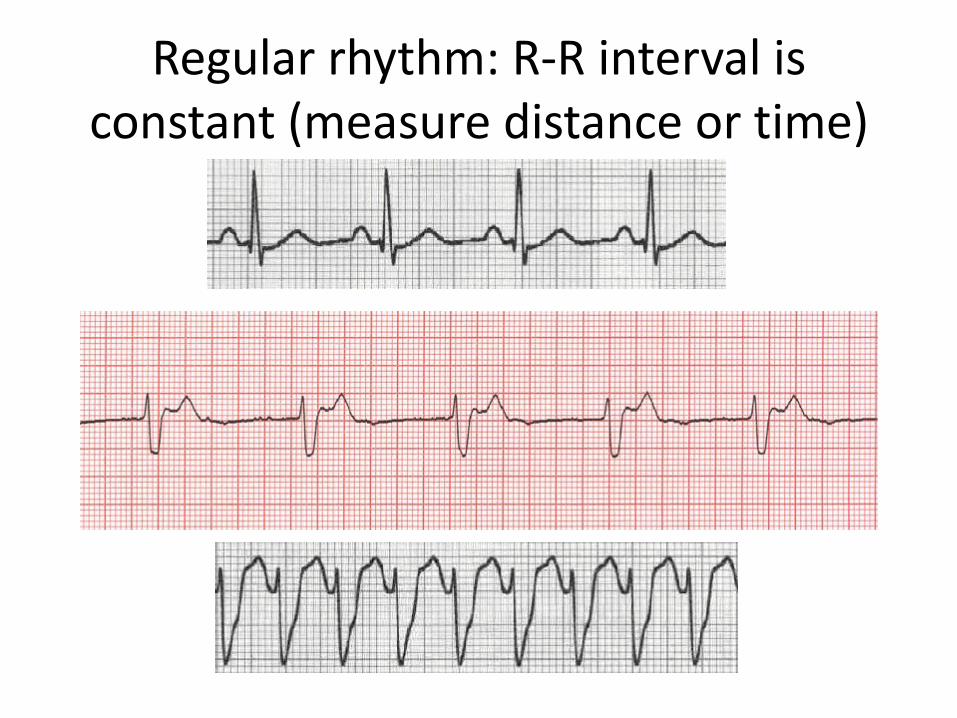
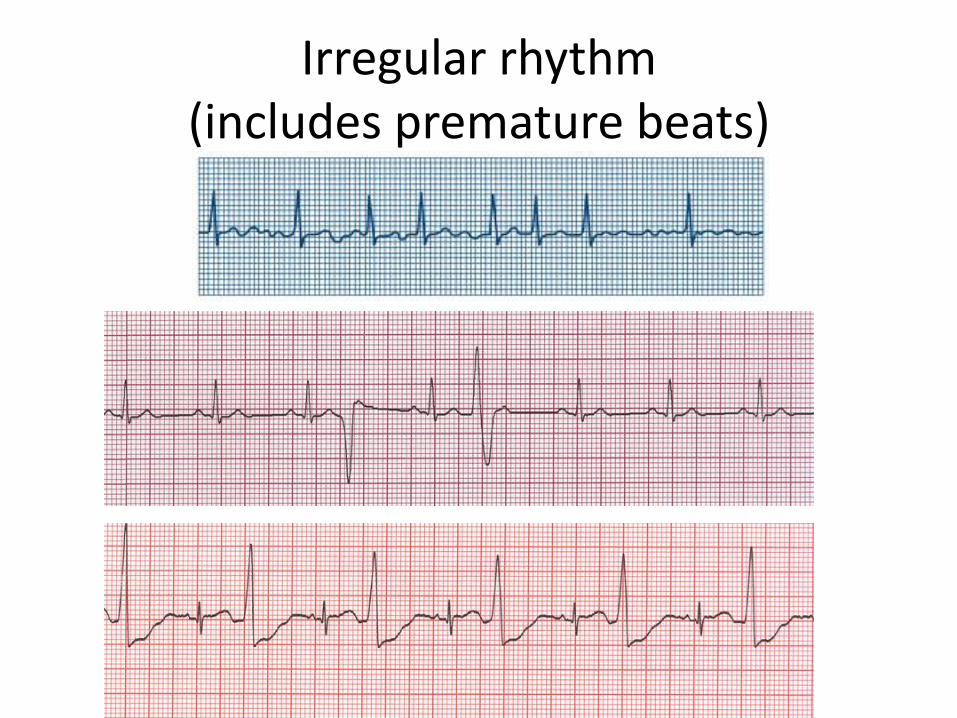
• Rhythm
• Axis
• Ischemia, hypertrophy, etc.
Frontal and Horizontal Plane Lead Diagram-KH Frank G. Yanowitz, M.D.
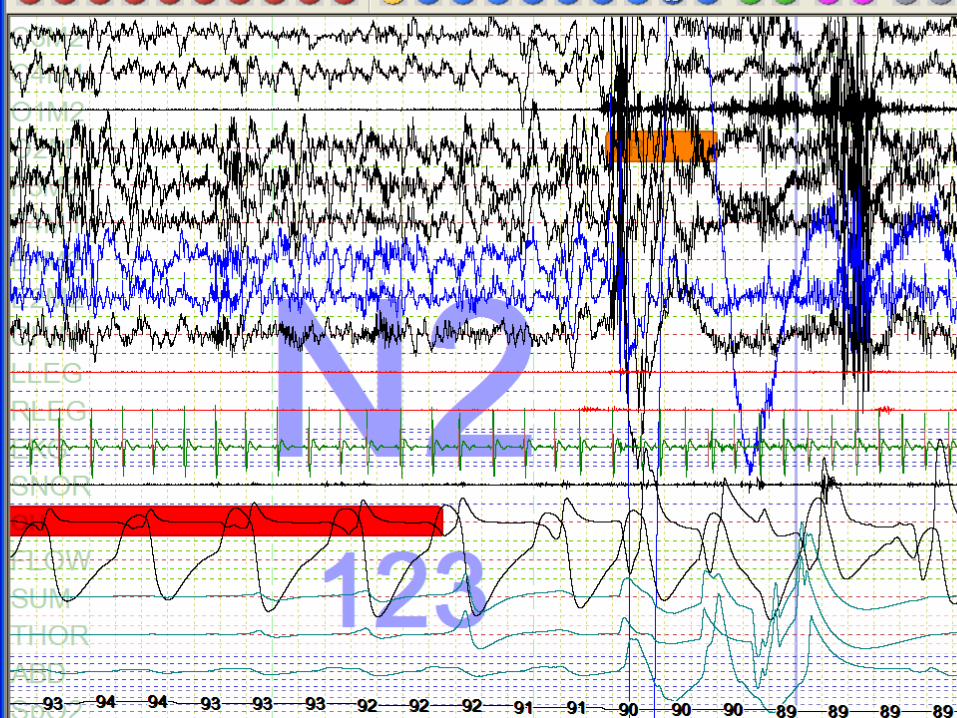
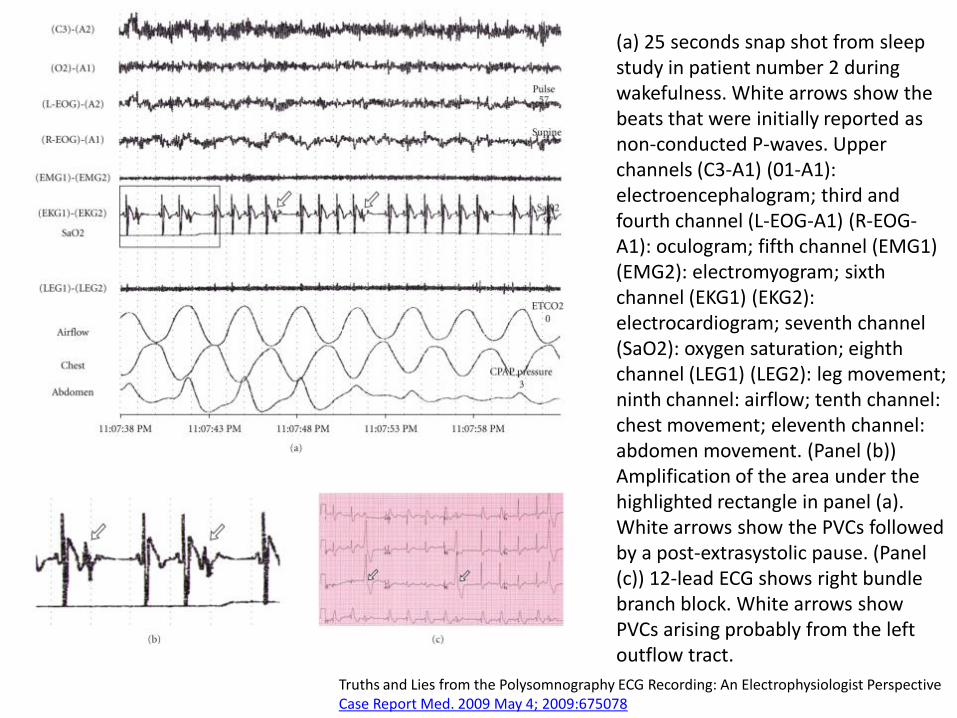
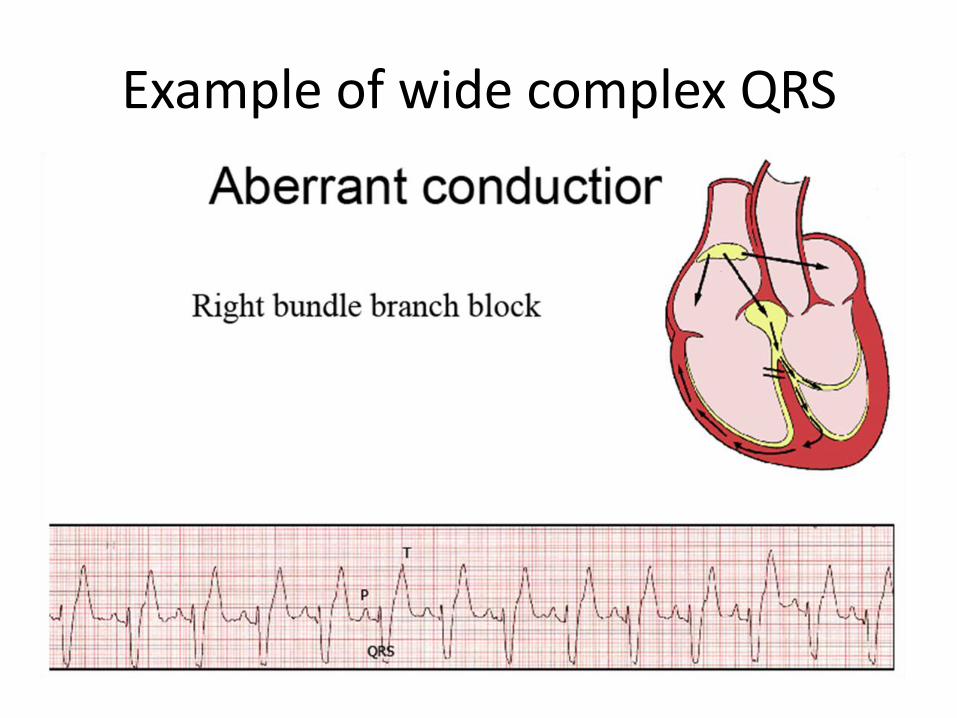
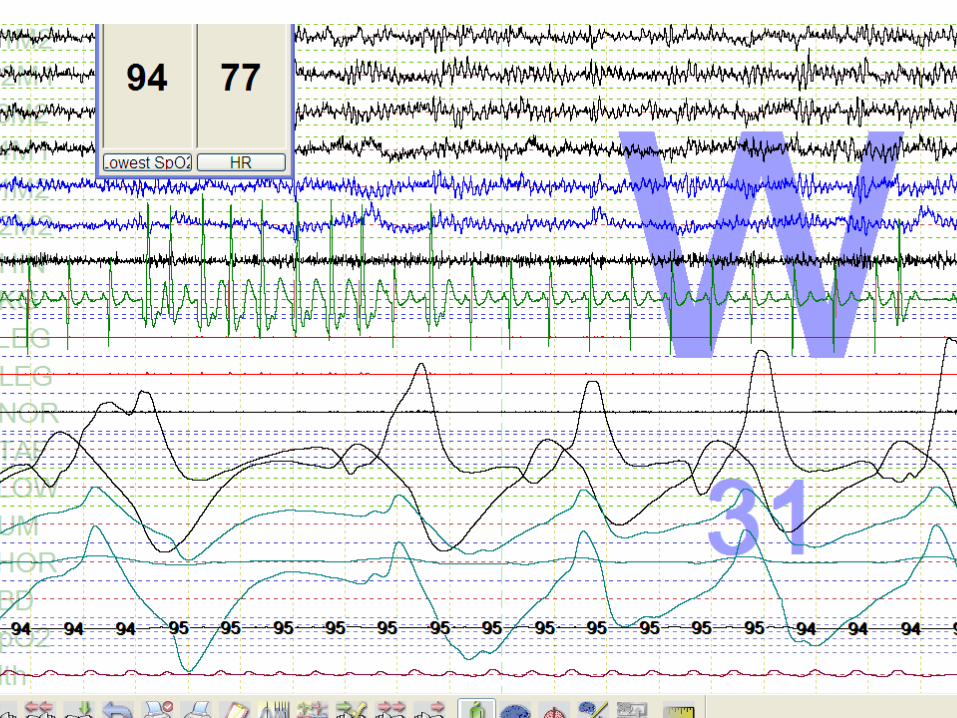
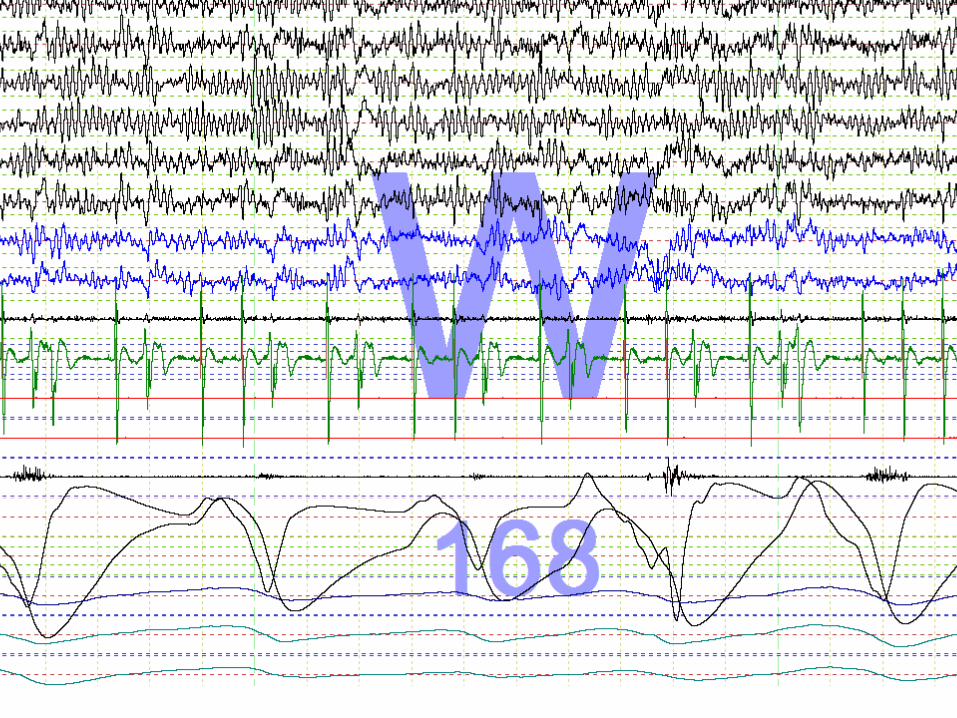
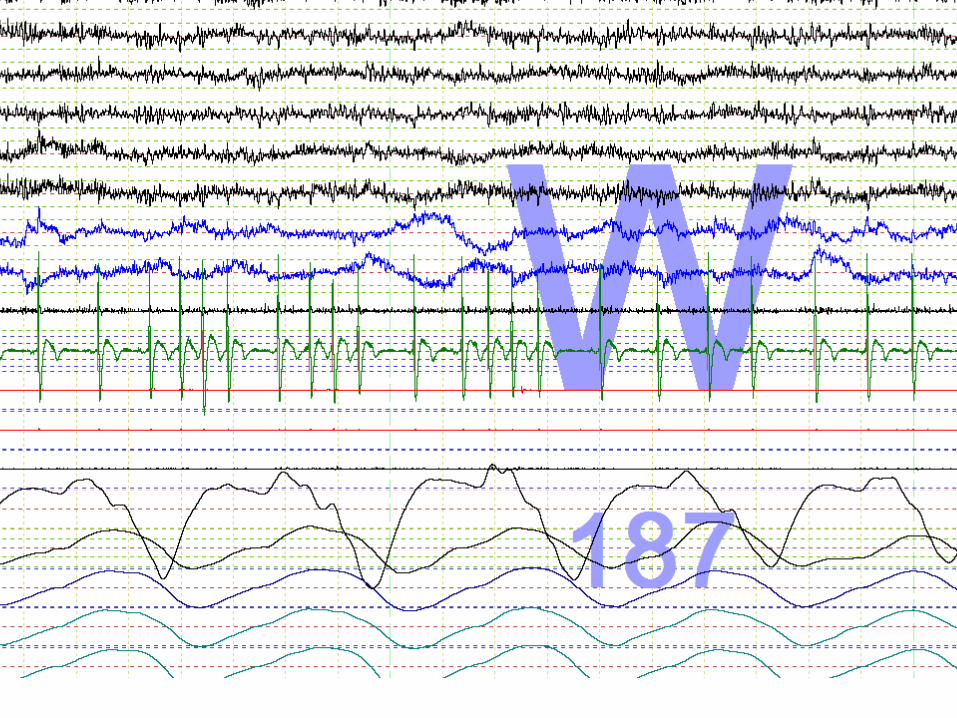
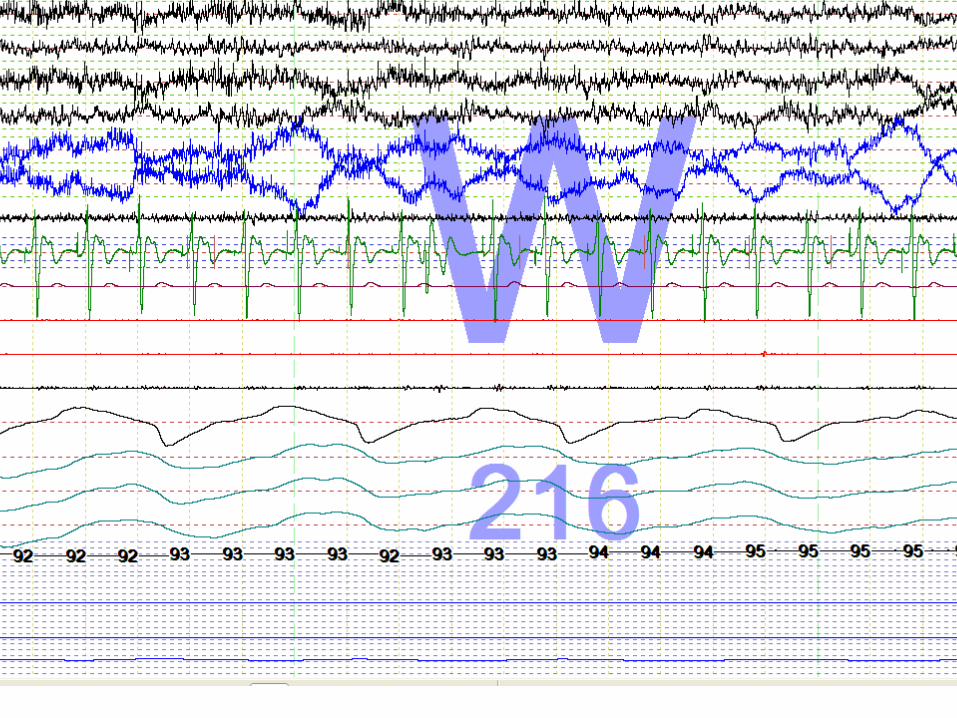
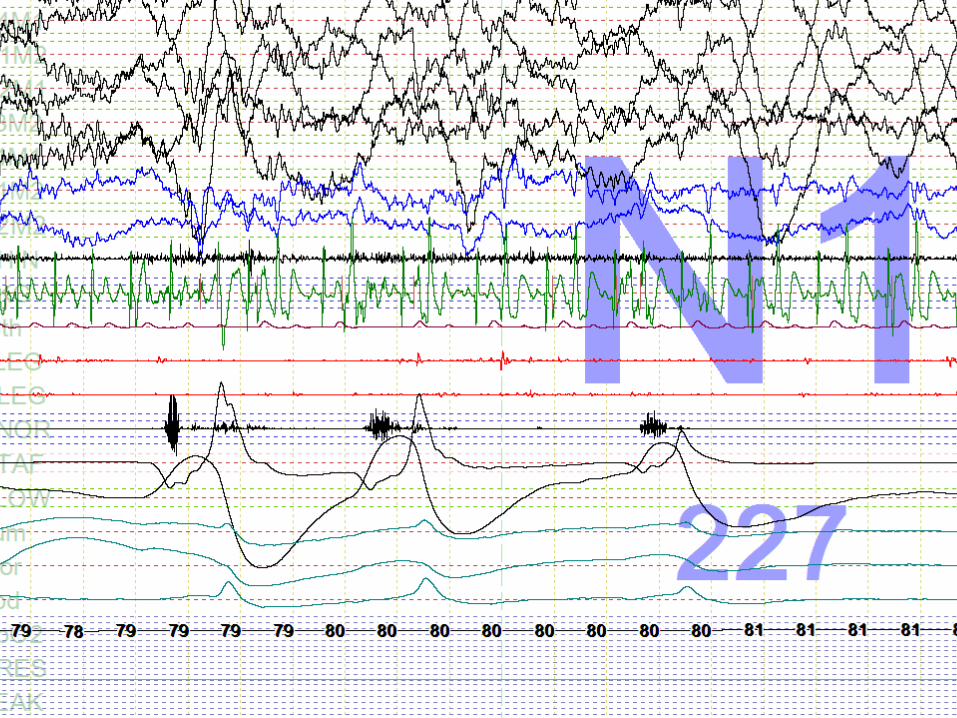
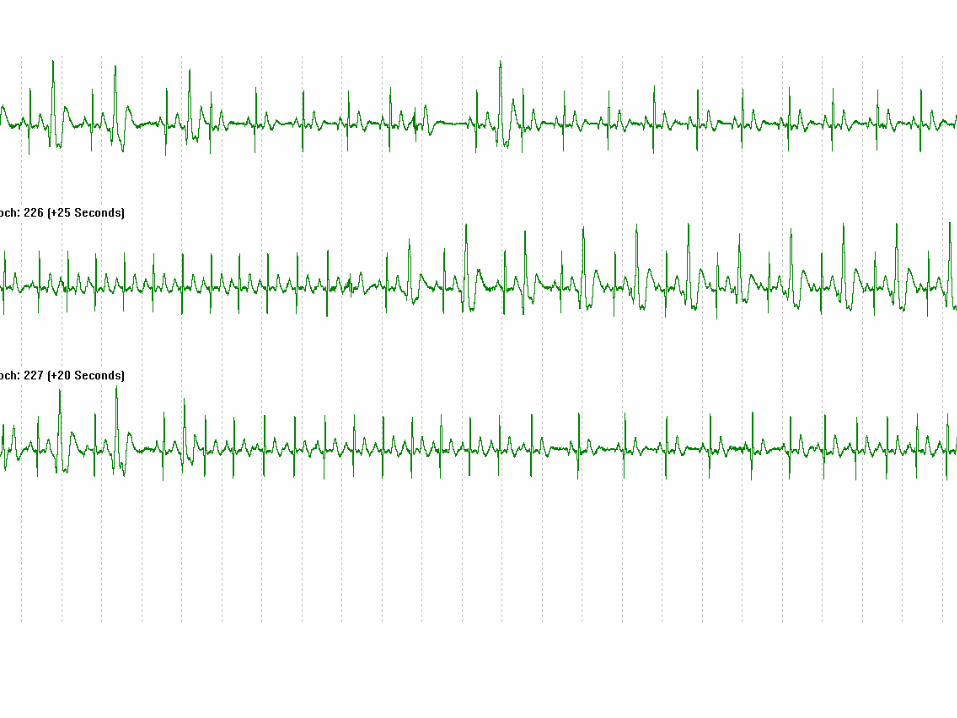
(a) 25 seconds snap shot from sleep study in patient number 2 during wakefulness. White arrows show the beats that were initially reported as non-conducted P-waves. Upper channels (C3-A1) (01-A1): electroencephalogram; third and fourth channel (L-EOG-A1) (R-EOG-A1): oculogram; fifth channel (EMG1) (EMG2): electromyogram; sixth channel (EKG1) (EKG2): electrocardiogram; seventh channel (SaO2): oxygen saturation; eighth channel (LEG1) (LEG2): leg movement; ninth channel: airflow; tenth channel: chest movement; eleventh channel: abdomen movement. (Panel (b)) Amplification of the area under the highlighted rectangle in panel (a). White arrows show the PVCs followed by a post-extrasystolic pause. (Panel (c)) 12-lead ECG shows right bundle branch block. White arrows show PVCs arising probably from the left outflow tract.
Truths and Lies from the Polysomnography ECG Recording: An Electrophysiologist Perspective Case Report Med. 2009 May 4; 2009:675078