134
Electroconvulsive Therapy Dr. Robert Tobiansky Consultant Old Age Psychiatrist & Honorary Senior Clinical Lecturer Lead ECT Consultant Barnet, Enfield & Haringey MH NHS Trust
Electroconvulsive Therapy
Dr. Robert TobianskyConsultant Old Age Psychiatrist& Honorary Senior Clinical LecturerLead ECT Consultant Barnet, Enfield & Haringey MH NHS Trust
Introduction:
Historical reviewIndicationsEvidence of efficacyPhysiological correlatesContra-indications Side - effectsPractical administration
Trainee’s attitudes to ECTc. 1989
24% unsupervised when gave 1st treatment
40% felt training inadequate 30% found it distressing to give treatmentPippard 1990 national audit training not
adequate in NETRH
Historical aspects of ECT•46AD Scribonius Largus- torpedo fish•16th cent. Ethiopians - electric catfish•1933 Von Meduna- “cardiazol”
convulsive therapy•1938 Cerletti & Bini - Electroconvulsive
Therapy•1942/1958- Freeman/Lancaster
unilateral ECT
History of ECT continued c. 1944-51 anaesthesia: barbiturate &
succinylcholine 1957 (Bolam v Friern Hospital Management Committee)
1958 - Hamilton “cuff method” c. 1980s introduction of EEG
monitoring 1970s/ 1980s – real vs. “sham” ECT studies
1985 - dose titration technique (Sackheim & Malitz)
History of ECT continued
2003 NICE HTA2003 RCPsych. ECTAS initiative2005 RCPsych. Handbook 2nd ed2005 MCA2007 amended MHA2009 NICE CG902013 RCPsych. Handbook 3rd ed
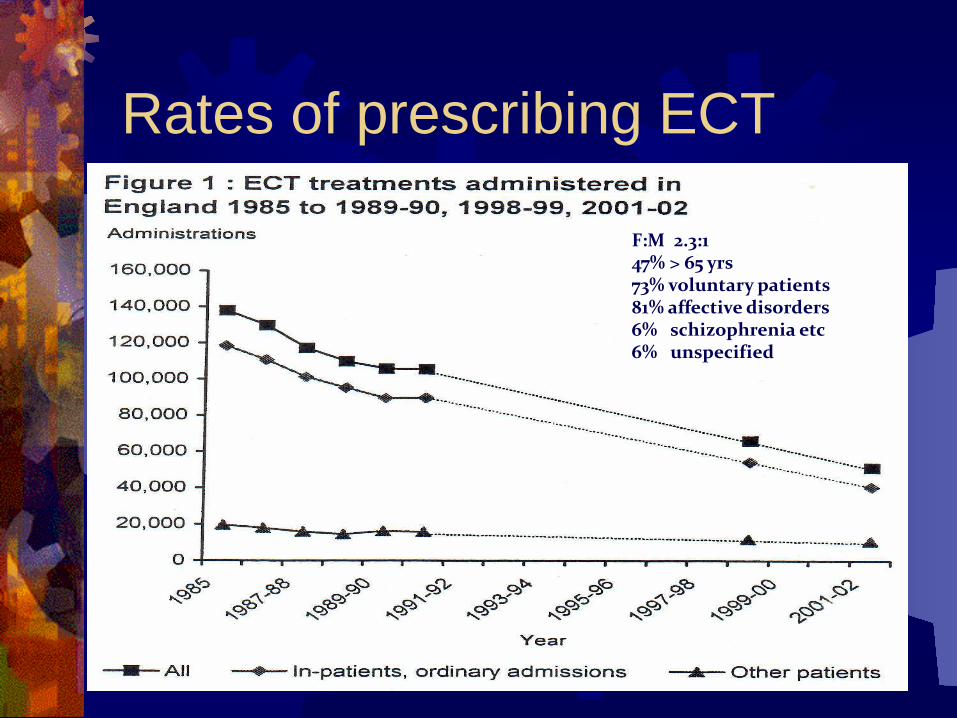
Rates of prescribing ECT
F:M 2.3:147% > 65 yrs73% voluntary patients81% affective disorders6% schizophrenia etc6% unspecified
ECTAS dataset report Sep 2015 2,148 acute courses of ECT were given to 1,969 people Cf 2012 when 2,022 courses of ECT were given to 1,856
people; 18,057 individual treatments 179 people had more than one course during the year 65% patients were female mean age of patients was 61 major depression 84% patients mean number of treatments per course was 9.5 51% patients were informal and had capacity to consent 52% were rated ‘severely ill’ at the start of treatment 92% showed clinical improvement by the end of treatment 155 people undergoing maintenance ECT during March 2015
Why is ECT use declining? International & national variation in practiceEranti & McCloughlin (2003) suggest:
Public and professional concerns Negative and stigmatising perceptions Lack of consensus on useResource limitationsComplacency on the part of psychiatrists
Change in the pattern of treatment of depressionDecreased inpatient treatment of depressionShift to primary care focus for depression Increased number of medication strategiesEmphasis on long-term treatment
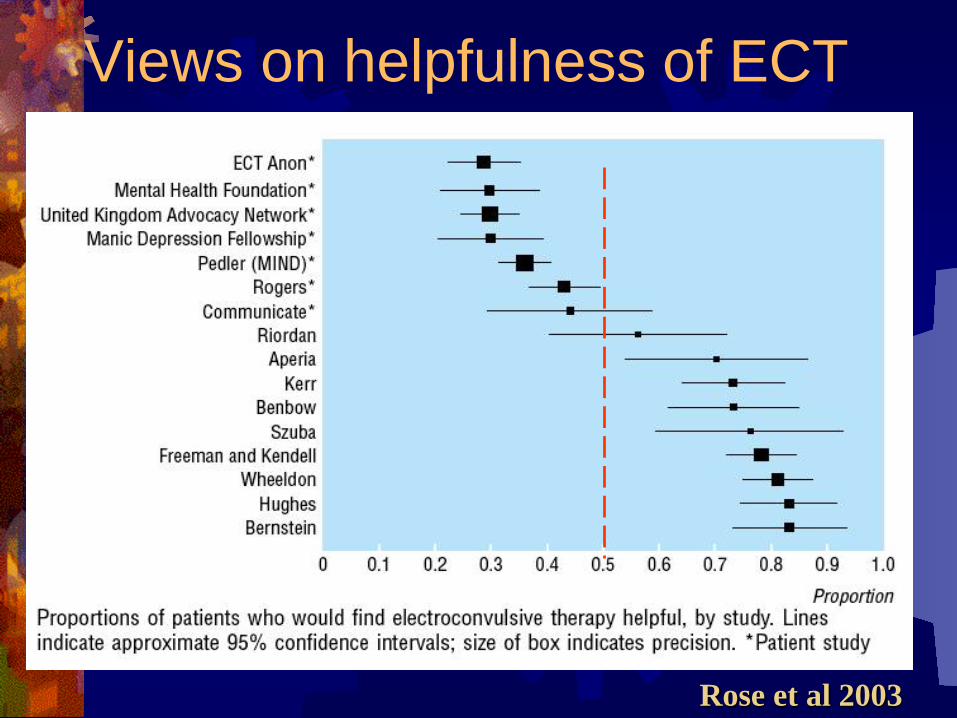
Views on helpfulness of ECT
Rose et al 2003
Indications for ECT
DepressionSchizophrenia - with catatonic features
- with prominent affective symptoms
Mania not responding to medication
ECT Indications: depression
Psychotic depression (delusions & hallucinations)
stupor (akinetic mutism, conscious)suicidal intent/planssevere medical disease failure of drug treatmentpuerperal psychosis
NICE: Guidance on the use of ECT. HTA April 2003 Use only to achieve short term and rapid
improvement in: severe depressive illness, catatonia, prolonged or severe mania
• documented assessment of risks & potential benefits
• Consent must be on-going, based on informed discussion, involving carer/ relatives/ advocate
• Assess clinical status after each treatment, stop when response achieved, sooner if side effects
• Maintenance ECT is not recommended• Use in schizophrenia not recommended
NICE: Clinical Guideline 90 Depression update Oct 2009Consider ECT for severe depression
that is life-threatening & when rapid response or when other treatments fail
Consider ECT in moderate depression if no response to multiple drugs and psychological treatment
NICE: Clinical Guideline 90 Depression update Oct 2009 Fully inform patient of risks & benefit &
document discussion re:Risks associated with GACurrent medical comorbiditiesPotential adverse events esp. cognitive
impairmentRisks associated with not receiving ECT
NICE: Clinical Guideline 90 Depression update Oct 2009 Assess clinical status after each ECT using a
formal valid outcome measure and stop when remission achieved
Assess cognitive function before 1st treatment & after every 3-4 treatments & at end of course
Include orientation, time to reorientation, measures of new learning, retrograde amnesia & subjective memory impairment
Royal College of Psychiatrists
The ECT Handbook, 3rd editionCouncil report CR128April 2013
Revised College guidance on ECT in the treatment of depressive illness, Handbook 2013:
ECT should be a first line treatment for depression in the following situations:
o Emergency treatment of depression where rapid response is needed
o Patients with high suicidal risko Patients with severe psychomotor retardation and
problems of eating and drinkingo Patients with TRD that have responded to ECT
previouslyo Patients who are pregnant where there is concern
about teratogenenic effects of psychotropics
Revised College guidance on ECT in the treatment of depressive illness:
ECT should be a second –line treatment for:
Patients with TRDPatients who experience side effects of
medicationPatients whose psychiatric condition
has deteriorated in spite of other treatments
Revised College guidance on ECT in the treatment of depressive illness:The selection of ECT may be
affected by:o patient preferenceo previous experience of ineffective
and/or intolerable medical treatment
o previous recovery with ECT
Efficacy in depression studies on real vs. sham ECT, 6 RCT 1978 Freeman et al: 40 pts. Given either 2
genuine or sham ECT in first week, depression scores on 3 scales signif. lower in real ECT group
1980 Johnstone et al 70 pts. Half partial sine wave ECT half anaesth. alone: mean HDAS scores signif. lower in real group after 4/52
Efficacy in depression cont. 1981 West: 22 pts. half given 6 real ECT
other half sham. Real group signif. better 1984 Brandon et al 95 depressives given
8 real partial sine wave or sham. Real group signif. better at 2 & 4 /52
1985 Gregory et al 60 pts. Random assigned to partial sine- wave or sham. Signif. change in real group
All included in UK ECT Grp review 2003
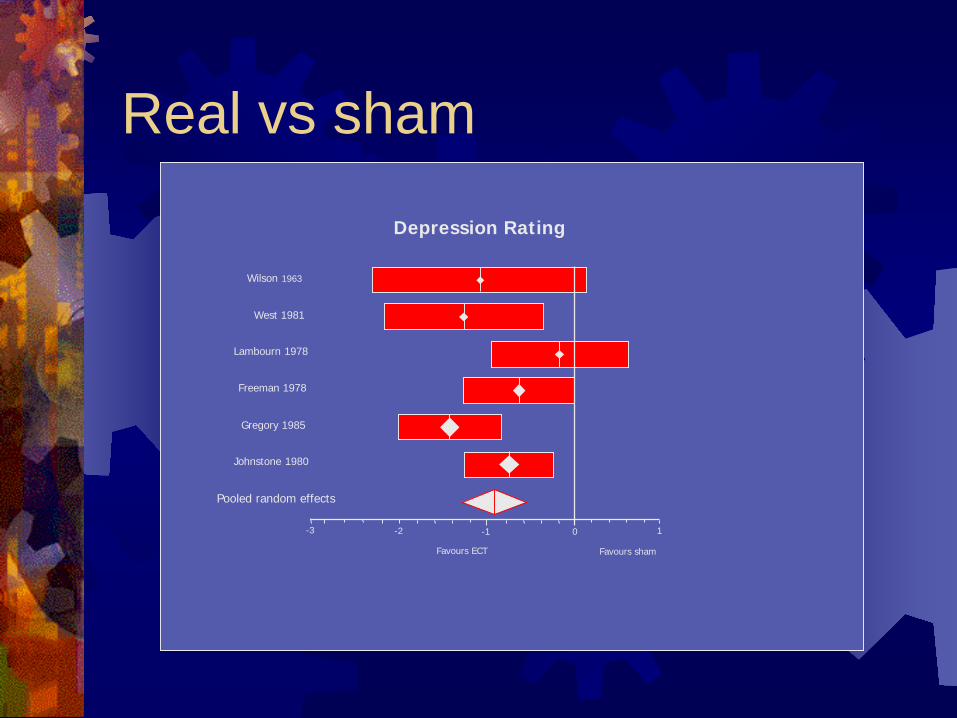
Real vs sham
Depression Rating
Wilson 1963
West 1981
Lambourn 1978
Freeman 1978
Gregory 1985
Johnstone 1980
Pooled random effects
Favours ECT Favours sham
-3 -2 -1 0 1
Efficacy in depression cont’d49 RCTs 1980 – 1989135 RCTs 2000-2009
ECT in treatment resistant depression. Kellner et al Am J Psych. 2012;169:1238-1244
Efficacy in depression cont’dLarge multisite RCTsCORE Kellner et al 2006CUC Sackheim et al 2001684 patients UP depression (TRD)Remission rates 86% (CORE), 55%
(CUC)
Efficacy in depression cont’dcomparison w.antidepressants Early studies: 1965 MRC trial: ECT vs. Imipramine vs. phenelzine
vs. placebo found ECT assoc. with best and most rapid response
Gangadar 1982: 24pts. RCT, real ECT + placebo signif. > effective than sham + imipramine at 1 month
Avery & Lubrano, 1979: ECT> effective than high dose imipramine
NCCMH review 2010: 18 RCTs: ECT more effective than ADs
Efficacy in DepressionAntidepressant pharmacotherapy failure and response to subsequent electroconvulsive therapy: a meta-analysis. DARE 2014, Heijnen et al
Overall remission rates after ECT were 48.0% for patients with previous pharmacotherapy failure and 64.9% for patients without previous pharmacotherapy failure.
Authors' conclusionsECT seemed to be an effective treatment for severely depressed patients as well as for patients with previous pharmacotherapy failure.
Speed of remission in elderly patients withdepression: ECT v. medicationSpaans et al BJPsych Oct 2014
Aims: compare the speed of remission using ECT v. medicationin elderly in-patients.
Method: speed of remission in in-patients with major depression compared between 47 participants (mean age 74.0 years, s.d. = 7.4) from an ECT randomised controlled trial (RCT) and 81 participants (mean age 72.2 years, s.d. = 7.6) from a medication RCT (nortriptyline v. venlafaxine).
Results: Mean time to remission was 3.1 weeks (s.d. = 1.1) for the ECT group and 4.0 weeks (s.d. = 1.0) for the medication group; the adjusted hazard ratio for remission within 5 weeks (ECT v. medication) was 3.4 (95% CI 1.9–6.2).
Conclusions: Considering the substantially higher speed of remission, ECT deserves a more prominent position in treatment
Efficacy in depression cont’d
Kellner et al: relief of expressed suicidal intent by ECT Am. J. Psych May 2005
444 pts. Unipolar depression, multicenter 30% expressed suicidal thoughts / acts at
baseline (score 3 or 4 on item 3 on 24 HDRS) Scores decreased to 0 after 1/52 in 40%,
after 2/52 in 60% and at end of course in 80% if patients at risk do not leave ECT to
last resort
Efficacy in depression cont’d UK ECT review group: Efficacy & safety of
ECT in depressive disorders: a systematic review & meta-analysis. Lancet March 2003
ECT is effective, more so than pharmacotherapy
“the randomised evidence consistently shows that in the short-term ECT is an effective treatment for adult patients with depressive disorders”
Efficacy in depression cont’dOverall efficacy in depression > 80% for
bilateral ECT (1.5 x ST) and high dose(6 x ST or fixed high dose) unilateral ECT (Kellner & Fink, Journal of ECT 2002)
Petrides et al 2001: 253 depressives, overall remission rate with ECT = 87%, remission rates higher & earlier in psychotic depression
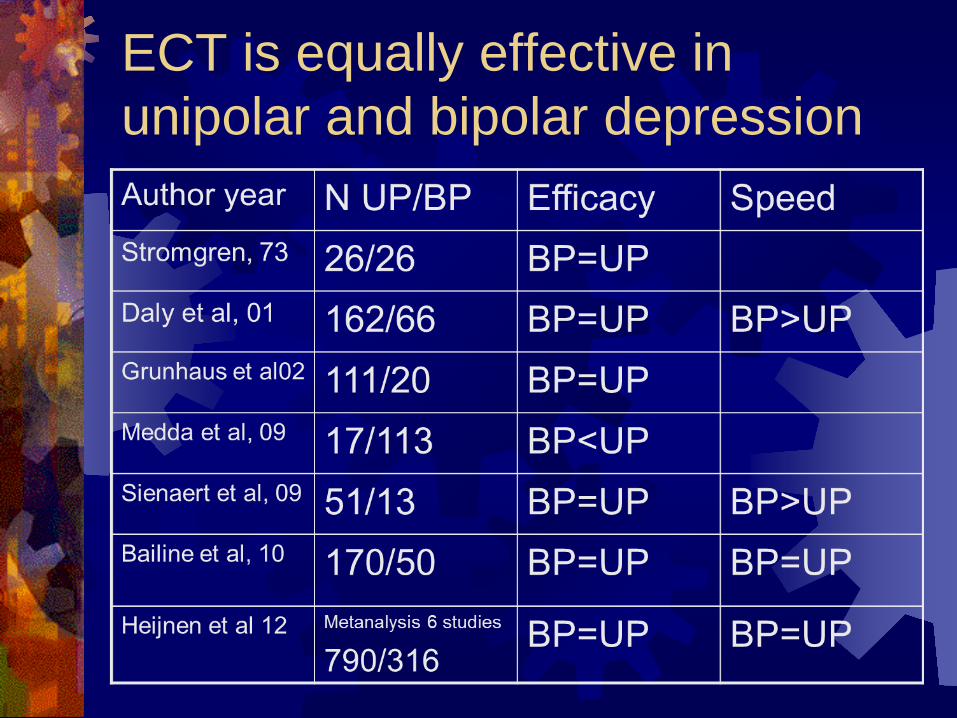
ECT is equally effective inunipolar and bipolar depression
Treatment-resistant bipolar depression: RCT of ECT v algorithm-based pharmacological treatment. Am J Psychiatry. 2015 Jan;172(1):41-51 Schoeyen et al
RCT of ECT in treatment-resistant bipolar depression compared efficacy measures of ECT and algorithm-based pharmacological
treatment in TRD bipolar depression. 7 acute-care psychiatric inpatient clinics throughout Norway 73 bipolar disorder patients with TRD randomly assigned to receive either ECT or
algorithm-based pharmacological treatment. ECT: three sessions per week for up to 6 weeks, right unilateral ECT, brief pulse stimulation.
Linear mixed-effects modeling analysis revealed that ECT was significantly more effective than algorithm-based pharmacological treatment.
mean scores at the end of 6-week treatment period lower for the ECT group than for the pharmacological group: by 6.6 points on the MADRS (SE=2.05, 95% CI=2.5-10.6), by 9.4 points on the 30-item version of the Inventory of Depressive Symptomatology-Clinician-Rated (SE=2.49, 95% CI=4.6-14.3), and by 0.7 points on the Clinical Global Impression for Bipolar Disorder
The response rate was significantly higher in the ECT group (73.9% versus 35.0%), but the remission rate did not differ between the groups (34.8% versus 30.0%).
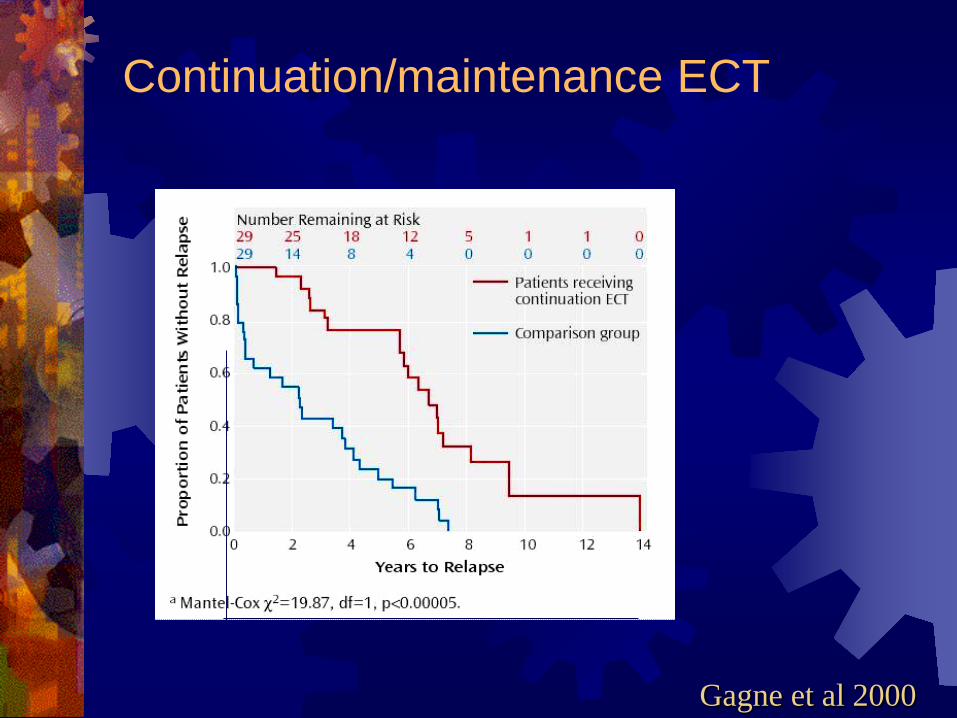
Continuation/maintenance ECT
Continuation/maintenance ECT
Gagne et al 2000
Efficacy of maintenance ECT in recurrent depression: a naturalistic study. Gupta, Tobiansky, Bassett P, Warner J. J ECT. 2008 Sep;24(3):191-4.
retrospective analysis of 19 patients who responded positively to an index and continuation course of ECT and then received mECT. compared number of hospital admissions and duration of hospital stay over 3 time periods: 2 years before ECT, during mECT, and up to 4 years after cessation of mECT. compared the admission rates of this group with a matched sample who received successful index ECT followed by other maintenance therapies (comparison group).Inpatient hospital stay and rate of admissions to an acute psychiatric unit fell significantly during the period of mECT compared with the rates before the initiation of mECT. This reduction in bed use was maintained after termination of mECT. No reduction of service use was observed in the comparison group.CONCLUSIONS: mECT may have a role in reducing the rate and duration of hospital stay of patients with major depressive disorder
CORE Petrides et al: Continuation ECT vs pharmacotherapy forrelapse prevention in major depression. Arch Gen Psych: 2006
• Consortium for Research in ECTMulti-centre study in US, (Columbia University Consortium)531 patients with severe depression HAM-D score 34+/-7Failed to respond to multiple courses of antidepressantsTreated to remission with ECT (BL 150%ST) HAM-D 6+/-3At remission randomised to:
Lithium + NortriptylineContinuation ECT
NO significant difference at six months.
Continuation & Maintenance ECT Continuation electroconvulsive therapy with pharmacotherapy versus
pharmacotherapy alone for prevention of relapse of depression: a randomized controlled trial. J ECT 2013 Nordenskjöld et al
A multicenter, nonblinded, RCT in Sweden 56 patients randomly assigned (1:1) to receiving either 29 treatments of
continuation ECT with pharmacotherapy or pharmacotherapy alone for 1 year. pharmacotherapy consisted of antidepressants (98%), lithium (56%), antipsychotics (30%). Main outcome was relapse of depression within 1 year. Relapse defined as 20 or more points on MÅDRS or inpatient psychiatric care or suicide or suspected suicide
61% of the patients treated with pharmacotherapy versus 32% of the patients treated with ECT plus pharmacotherapy relapsed within 1 year (P = 0.036).
Cox proportional hazard ratio was 2.32 (1.03-5.22).Cognitive function and memory measures were stable for patients without relapse in both groups. One suspected suicide and 3 suicide attempts occurred, all in the pharmacotherapy-alone group.
CONCLUSIONS: The post-ECT relapse rates were substantial in both treatment groups with a statistically significant advantage for combined treatment with pharmacotherapy and continuation ECT.
Journal of ECT: September 2014 Brown et alEfficacy of Continuation/Maintenance Electroconvulsive Therapy for the Prevention of Recurrence of a Major Depressive Episode in Adults With Unipolar Depression: A Systematic Review
A systematic review of 3 databases, including 11 studies of c/m ECT which met the search criteria.Found consistent evidence that c/m ECT was efficacious.“This review suggests that c/mECT is efficacious for the prevention of relapse/recurrence of major depression and that efficacy is increased when c/mECT is provided in combination with antidepressant medication and at flexible treatment intervals, responsive to early signs of recurrence.”
ECT:Efficacy in Schizophrenia
Efficacy in Schizophrenia Friedel 1986: ECT augmentation of
thiothixene resulted in signif. improvement in schizophrenic patients
Klapheke 1993: ECT augmentation of clozapine decreased BPRS score by 40%
Cochrane review, 2, 2005: pooled data from 26 studies, 798 pts. Courses of ECT with antipsychotic medication can, in the short-term, result in global improvement
ECT Augmentation in Clozapine-Resistant Schizophrenia: Prospective RCTPetrides et al Am J Psych August 2014
Objective examine use of ECT as augmentation to clozapine for treatment-refractory schizophrenia.
Method randomized single-blind 8-week study, patients with clozapine-resistant schizophrenia were assigned to treatment as usual (clozapine group) or a course of bilateral ECT plus clozapine (ECT plus clozapine group). Nonresponders from the clozapine group received an 8-week open trial of ECT (crossover phase). Response was defined as ≥40% reduction in symptoms based on the psychotic symptom subscale of the Brief Psychiatric Rating Scale, a Clinical Global Impressions (CGI)-severity rating <3, and a CGI-improvement rating ≤2. Results The intent-to-treat sample included 39 participants (ECT plus clozapine group, N=20; clozapine group, N=19). All 19 patients from the clozapine group received ECT in the crossover phase. Fifty percent of the ECT plus clozapine patients met response criterion. None of the patients in the clozapine group met response criterion. In the crossover phase, response was 47%. There were no discernible differences between groups on global cognition.
Conclusions The augmentation of clozapine with ECT is a safe and effective treatment option. Further research required to determine the persistence of the improvement and the potential need for maintenance treatments.

The place of ECT in the treatment of acute schizophrenia, RCPsych:
The treatment of choice for acute schizophrenia is antipsychotic drug treatment
ECT may be considered as a fourth-line option, that is, an option for treatment-resistant schizophrenia after treatment with two different antipsychotic drugs and then with clozapine has already proven ineffective or intolerable
RCPsych. Handbook: Catatonia & ECT
Catatonia: rigidity, mutism, negativism, stareing, stereotypy, posturing
The treatment of choice is a benzodiazepine drug; most experienceis with lorazepam
ECT may be indicated when treatment with lorazepam has been ineffective
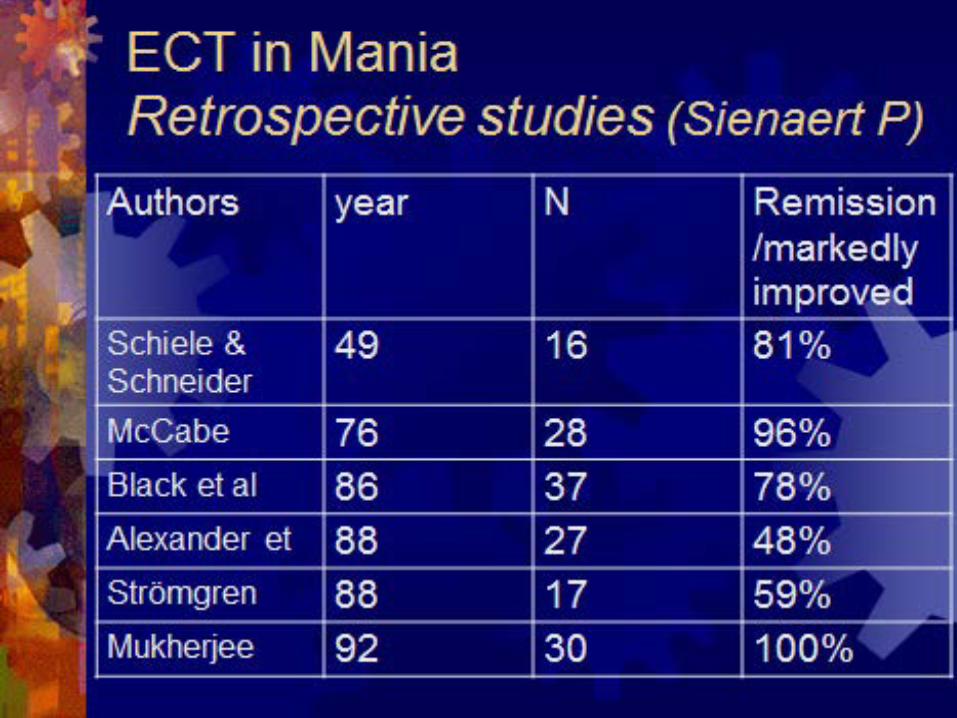
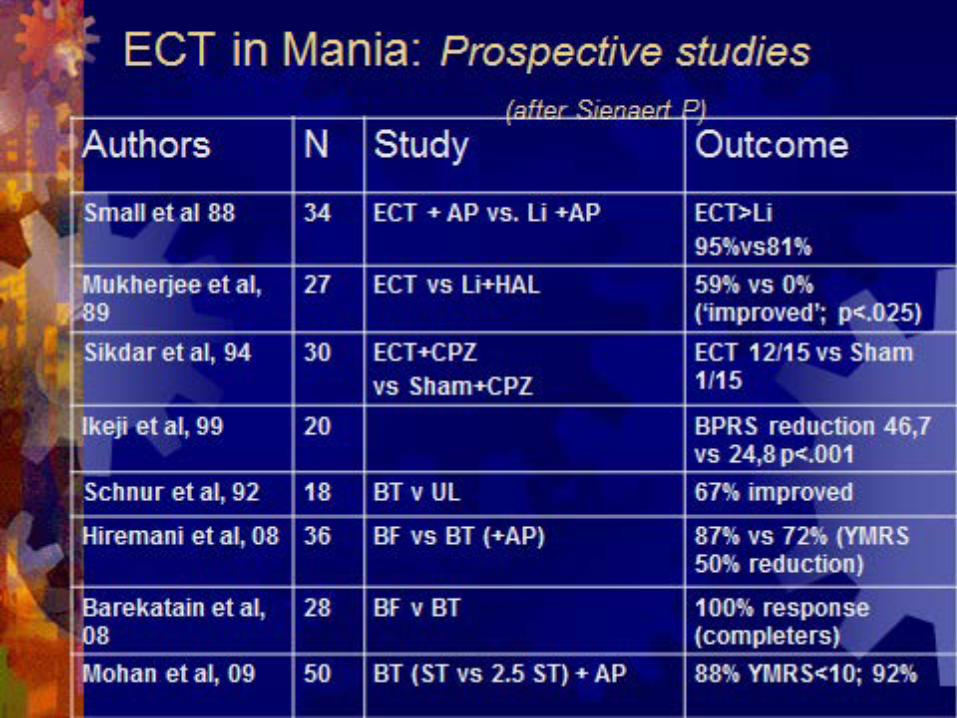
Efficacy in Mania
Small et al 1986 34 manic pts. Either ECT or Lithium, ECT group> outcome at 6 & 8 weeks
Sikdar 1994: 2 groups 15 pts. each. 1 given real ECT + CPZ + PRN, other given sham + CPZ + PRN. Real ECT group improved signif. > and needed half PRN neuroleptics of sham group
RCPsych. Handbook : The place of ECT in the treatment of mania
The treatment of choice for mania is a mood-stabilising drug plus an antipsychotic drug
ECT may be considered for severe mania associated with:
o life-threatening physical exhaustion treatment resistance, that is, mania that has
not responded to the treatment of choice
ECT & Postpartum Psychosis
Focht & Kellner J. ECT: March 2012 review on the phenomenology of postpartum
psychosis and the prevalence of use, safety, and efficacy of ECT a treatment. Studies were searched using CINAHL, EMBASE, MEDLINE, PsycINFO, and PubMed databases. Conclusion: for some patients, ECT should be the treatment of choice
ECT in a pregnant patient NICE CG 192Antenatal and postnatal mental health: clinical management and service guidance December 2014 NICE clinical guideline 192 If a pregnant woman with bipolar disorder develops mania while taking
prophylactic medication: check the dose of the prophylactic medication and adherence increase the dose if the prophylactic medication is an antipsychotic suggest changing to an antipsychotic if taking another medication consider lithium if there is no response to an increase in dose or
change of drug consider ECT if no response to lithium. Electroconvulsive therapy 1.8.22 Consider ECT for pregnant women with severe depression,
severe mixed affective states or mania, or catatonia, whose physical health or that of the foetus is at serious risk. [2014]
ECT in older people Speed of remission in elderly patients with depression:
electroconvulsive therapy v. medication Harm-Pieter Spaans, et al BJPsych Jan 2015
AIMS: To compare the speed of remission using ECT v. medication in elderly in-patients.
Method speed of remission in in-patients with major depression (baseline MADRS score ≥20) was compared between 47 participants (mean age 74.0 years, s.d. = 7.4) from an ECT randomised controlled trial (RCT) and 81 participants (mean age 72.2 years, s.d. = 7.6) from a medication RCT (nortriptyline v. venlafaxine).
Results Mean time to remission was 3.1 weeks (s.d. = 1.1) for the ECT group and 4.0 weeks (s.d. = 1.0) for the medication group
Conclusions: Considering the substantially higher speed of remission, ECT deserves a more prominent position in the treatment of elderly patients with severe depression
….but how does it work?
….but how does it work?
Single mechanism of action highly implausible (Lerer, 1998)
effects on monoamine neurotransmitters 5HT, NA, DA
Increased release GABA (anticonvulsant hypothesis?)
Increased glutamate in anterior cingulate gene expression induction of brain derived neurotrophic factor electrophysiological changes in prefrontal
cortex release of endogenous neuropeptides
….but how does it work? Metabolic correlates of antidepressant and
antipsychotic response in patients with psychotic depression undergoing ECT McCormick L et al. Dec 2007. J ECT;23:265-273.
PET used to assess cerebral glucose metabolism in 10 subjects before and after a course of ECT. Antidepressant efficacy was associated with increased metabolism in the left subgenual anterior cingulate cortex and the hippocampus. Reduction in antipsychotic symptoms was associated with increased metabolism in the left hippocampal region.
….but how does it work? CREB binding and activity in brain: regional
specificity and induction by electroconvulsive seizure. Tanis K, Duman R, Newton S. 2008, Biological Psychiatry
looked at cyclic AMP response element binding (CREB) receptor sites in the rat brain:
CREB is an important mediator of the biological response to ECT seizure.
..how does it work (cont’d)? Duman et al: a molecular & cellular theory of depression Arch Gen Psych 1997
depression arises when structural changes involving decreasing synaptic contacts occurs.
Reversal of depression involves increasing synaptogenesis: increased beta receptor stimulation leads to down regulation of receptors, activation of cAMP responsive binding element and gene activation with induction of neurotrophic factors such as brain derived neurotrophic factor with increased membrane synthesis and increased synaptic contacts
ECT mechanisms of action Jacobs BL et al (2000)Neurogenesis continues into adulthood particularly prominent in the dentate gyrus
of the hippocampal formation stress potently suppresses adult
neurogenesis, probably due to increased glucocorticoid release
increasing brain levels of serotonin enhance the basal rate of dentate gyrus neurogenesis
ECT mechanisms of action Jacobs theory regarding clinical depression:
Stress-induced reduction in dentate gyrus neurogenesis are an important causal factor in precipitating episodes of depression. Reciprocally, therapeutic interventions for depression that increase serotonergic neurotransmission act at least in part by augmenting dentate gyrus neurogenesis and thereby promoting recovery from depression.
Hypothesis: waning and waxing of neurogenesis in the hippocampal formation are important causal factors, respectively, in the precipitation of, and recovery from, episodes of clinical depression.
ECT mechanisms of actionNeurogenesis previously thought only
to occur in dentate gyrus & subventricular zone of the hippocampus
now shown that neurogenesis also occurs in the amygdala & hypothalamus, areas involved in emotional regulation & executive function
ECT mechanisms of action Coplan et al 2007: study of
electroconvulsive shock on normal primates ECS increased proliferation of precursor
cells, a hallmark of neurogenesis ECS specifically increased neurogenesis in
the cingulate cortex, involved in executive function
ECT mechanisms of action ECT is associated with increased hippocampal
precursor cell proliferation, neurogenesis, angiogenesis, anti-apoptosis, BCL2, increased precursor proliferative cells in prefrontal cortex, cingulate cortex. Some cells appear to differentiate into GABAergic interneurons.
This suggests that antidepressant treatments may increase neurogenesis outside the hippocampus
ECT mechanisms of action Depressogenic factors which are associated
with decreased neurogenesis include: Hypercortisolaemic states Alcohol & opiate abuse Sleep deprivation Hypothyroidism (inhibits precursor cell
maturation) Inflammatory disorders (probably through
cytokine cascade, release of interleukin 1 & 6, tumour necrosis factor, interferons)
ECT mechanisms of action Factors that stimulate neurogenesis
include:Neuropeptide Y growth factors eg insulin-like growth factor,
vascular endothelial growth factorExercise in rodents (esp. running)Environmental enrichment
ECT mechanisms of action Mood stabilisers such as lithium & valproate
increase anti-apoptotic gene factors eg B-cell lymphoma gene product 2 (BCl-2)
Lamotragine blocks glutamate All antidepressant treatments, despite diverse
primary actions appear to have effect of stimulating neurogenesis, this may be a unifying mechanism
ECT mechanisms of actionDespite their different mechanisms of
action, all antidepressants appear to share the common property of stimulating neurogenesis. Antidepressant treatment may increase extra-hippocampal GABAergic interneurons.
6-13 ECT treatments in 12 medicated depressed patients
Bilateral c. 5% mean increase in hippocampal volume
Effect of ECT on Hippocampal volume: Nordanskog et al 2010
ECT current theories Bolwig TCan J Psych 2011Generalised seizure theoryNormalisation of neuroendocrine
funxction (Neuroendocrine-diencephalic theory)
Anatomical-Ictal Theory (neurogenesis and neuronal plasticity
ECT reduces frontal cortical connectivity in severe depressive disorder; Perrin, Reid et al PNAS 2012
functional MRI used to examine functional connectivity in the brain before and after ECT treatment in 9 depressed patients
results show that ECT has lasting effects on functional brain architecture
comparison of pre- and post treatment functional connectivity data in 9 patients revealed a significant cluster of voxels in and around the left dorsolateral prefrontal cortical region (Brodmann areas 44, 45, and 46), where the average global functional connectivity was considerably decreased after ECT treatment (P < 0.05)
This decrease in functional connectivity was accompanied by a significant improvement (P < 0.001) in depressive symptoms on MADRS scores pre 36.4 (SD = 4.9) and post 10.7 (SD = 9.6)
The findings reported here add weight to the “hyperconnectivity hypothesis” in depression and support the proposal that increased connectivity may constitute both a biomarker for mood disorder and a potential therapeutic target.
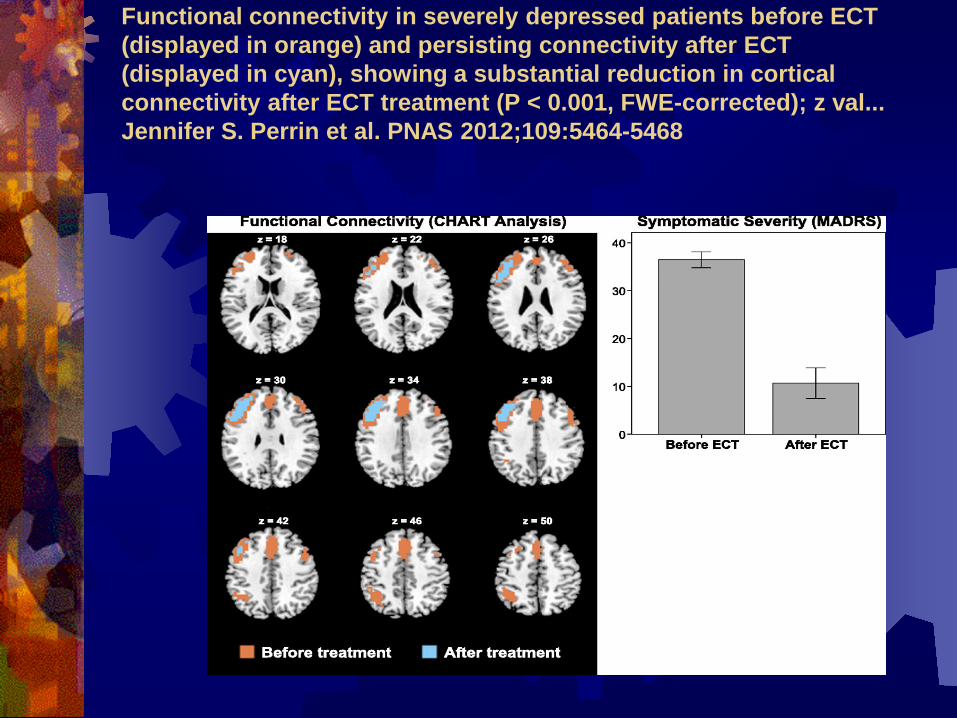
Functional connectivity in severely depressed patients before ECT (displayed in orange) and persisting connectivity after ECT (displayed in cyan), showing a substantial reduction in cortical connectivity after ECT treatment (P < 0.001, FWE-corrected); z val... Jennifer S. Perrin et al. PNAS 2012;109:5464-5468
Predictors of response to ECT
Various studies Hobson 1953, Mendels, Carney et al etc.
Coryell & Zimmerman 1984: most favourable: delusions, older, female
Johnstone et al 1986, Buchan et al 1992 (meta analysis) : delusions & retardation strongest predictors +ve
Predictors of response to ECT Prediction of response to ECT with
routinely collected data in depression. van Vliet et al. J of Affective Disorders 86 (2005) 323-327.
case note study of 53 patients over 4 years to determine factors predicting poor outcome (< 50% reduction in Hamilton RSD)
Predictors of poor response were: personality disorder, age <65years, previous treatment resistance
Predictors of response to ECTPredictors of Response to ECT using
the 3 Factor Structure of MADRS Okazaki et al J ECT 2009
dysphoria retardationvegetative symptoms
Predictors of Response to ECT using 3-Factor Structure of MADRS Okazaki et al Journal of ECT: June 2010
24 depressed patients all MDD or BPD depressed Given 6 sessions of ECT and determined response as being
>50% reduction in MADRS score which started as >21 in all patients. Divided MADRS into
1. Dysphoria factor, 3 items 2. Retardation factor, 4 items3. Vegetative factor, 3 items
17 patients responded, 7 non-responders Responders had significantly higher mean factor 1 score Factor 3 score was significantly lower at one week after
treatment in reponders
Health related quality of life and ECT Rosenquist et al. J of ECT 2006
review of health related quality of life (HRQL) studies following ECT
authors conclude that there is an emerging literature which demonstrates the importance of ECT in restoring function and quality of life in depressed patients.
Health related quality of life following ECT Vaughn McCall et al. J of Affective
Disorders, 2006 naturalistic study of 283 depressed patients
assessed both quality of life and cognitive impairment post ECT and after 24 weeks
Health related factors improved with recovery from depression independent of short term cognitive impairment
at 24 week follow up improvement in cognitive status was associated with better quality of life.
Effect of concomitant antidepressant treatment with ECT Sackheim et al Arch Gen Psych 2009
Treatment with nortriptyline enhanced the efficacy & reduced cognitive s/es vs placebo
High-dosage right unilateral ECT did notdiffer to bilateral ECT in efficacy & resulted in less severe amnesia.
Conclusions: The efficacy of ECT is substantially increased by the addition of an antidepressant medication
Physiological events in ECT
Electrical stimulus depolarisation of neurones low voltage fast activity (recruitment)
suprathreshold stimulus high voltage polyspikes (tonic) polyspike + large amplitude slow wave (clonic) slowing and return to alpha & beta rhythm (Return to baseline in 1- 4 weeks)
Physiological events cont’d
increased cerebral blood flow increased oxygen consumption increased glucose uptakeacross a course seizure threshold
rises by average 65%seizures tend to last longer with
bilat.
Physiological events cont’d
Initial parasympathetic induced bradycardia, periods sinus asystole
sympathetic induced tachycardia 150 - 160 bpm (clonic phase)
initial decrease then increase in BPmyocardial oxygen consumption increases
x2- x4
Contraindications to ECT
No absolute contra-indications, relative only
risk of anaesthesiacauses increased ICP recent MI or CVAaneurysm
Adverse effects of ECT
Mortality: c. 1 in 50 000CVS risk arrhythmia or MICNS: risk of CVA, prolonged seizure,
delirium, retrograde & anterograde amnesia
other: ruptured viscus, fractures
Common side effects of ECT
Headachenauseamyalgia / arthralgia retrograde amnesia (bilateral)anterograde amnesia (bilateral)
ECT: adverse cognitive effectsSemkovsa & McLoughlin 2010 review
84 studies c. 3000pts 70% tests showed decreased cognitive performance
at 0-3 days post ECT Improvement in test results by 4-15 days post ECT By 15 days post last treatment no negative effects on
cognitive function were measurable 60% of tests at 15 days showed improvement over
pre ECT baseline “after 15 days, processing speed, working memory,
anterograde memory, executive function improved beyond baseline”
ECT & Autobiographical memoryFraser et al 2008Autobiographical memory impairment
can occurPredominantly personal events near the
treatment (6 months before)Objective measures found relatively short
term, less than 6/12 after treatmentLess with brief pulse vs. sine wave and
Unilat vs. bilat
Informing patients & relatives regarding risk of cognitive side effects
ECT does not cause brain damage or dementia Depression has marked effects on cognitive function ECT can affect memory Difficulties with everyday memory, learning &
retaining new information will be relatively short-lived Everyday memory function may improve after the
ECT compared with baseline Effects on autobiographical memory can be longer
lasting, can be up to 6 months & some patients may experience more longlasting gaps in memory
ECT Apparatus Older machines: biphasic sinusoidal wave form newer machines uni or bi- phasic brief pulse
stimulus or ultrabrief pulse Various: Thymatron; MECTA; Spectrum V = IR (Voltage = Amps x resistance) Watt = V x I Joule = Watt x sec Coulomb = I x sec
ECT dose & laterality
Electrical dose and STOttosson 1960: compared efficacy of
moderately and markedly suprathreshold ECT, the latter signif. more effective
Robin & de Tissera 1982: high energy brief pulse ECT signif. more effective than low
high stimulus may contribute to therapeutic effect by influencing the intensity or the generalization of seizure activity or both
Electrical dose and Seizure ThresholdDose Titration: Sackheim & Malitz 1985
Dosing methodsDose titration
Age based formula (bilat = half age; unilat = full age for Thymatron percent energy output; alternatively multiply by 2.5mC; eg 50 year old man having bilat ECT= treat at 25% =125mC
For unilateral ECT multiply by 5mC = 250mC

ST vs. Age based formula. Petrides et al. J ECT Dec 2009 multicenter prospective study 402 depressed patients standardized course
bilat ECT ST by dose titration compared with
estimates based on Half Age method (HA) HA estimates 18% above the empirically
determined ST suggests use of HA estimates may result in
fewer stimulations cf DT method.
Methods: sample of ECT patients analysed. Seizure thresholds derived empirically were used to calculate the proportions of patients who would have had a therapeutic stimulus had Half-Age or a fixed-dosing method (200 mC for those <65 years old and 250 mC for those >65 years old) been used.
Results: 62 patients were included. Initial seizure threshold varied 6 fold across the sample. Using the Half Age method 19.4% would have had a therapeutic seizure at first stimulation cf. 61.3% using an age based fixed protocol and 0% using the Royal College recommended dose titration method. Half Age and Fixed Dosing would have significantly (p<.0001) reduced the number of stimulations, the cumulative electrical dose delivered, the complexity of the procedure & number of treatment sessions
ConclusionsAge based fixed-dosing would simplify the ECT process and result in more patients receiving effective treatment at first stimulation.
A comparison of ECT dosing methods using a clinical sample: Bennett et al. J Affective Disorders 2012
Seizure Threshold over a course of ECT
ST over a course of ECT
… tends to increase by c. 60% over a course of ECT
Seizure Threshold over a course of ECTChange in Seizure Threshold During ECT Fink et al. The Journal of ECT: 2008
Only 21% of sample (n=77) showed an increase in ST by end of course.
70% showed NO CHANGE in ST9% of patients (ie 7) had a lowered ST.
but………
Anticonvulsant Mechanisms of ECT and Relation to Therapeutic EfficacyDuthie, Perrin, Bennett et al. J ECT Sep 2015
Background: ECT may confer anticonvulsant effects, although the role of rise in seizure threshold on clinical effect is uncertain. This study investigated the relationship in a large, consecutive, retrospective sample of patients receiving ECT in Aberdeen. Tested the hypotheses of previous authors to further examine the relationship between seizure and therapeutic effect
Methods: All ECT patients at the Royal Cornhill Hospital between 2000 and 2008 identified from the Scottish ECT Accreditation Network. ECT given 2x week; bilateral using routine dosage schedules. Data gathered from SEAN
Results: The seizure threshold increased in 219 (94.4%) patients, stayed the same in 13 (5.6%) patients, and decreased in 0 patient (n = 232). No significant relationship was present between change in seizure threshold and change in Montgomery-Asberg DRS score (P = 0.39; Kendall τ b r = 0.047; n = 182), although responders did display greater increase in ST than nonresponders.
Conclusions: ECT confers anticonvulsant effects in a consecutive sample of real -life patients. Neither initial seizure threshold nor magnitude of seizure threshold increase is a predictor of clinical response to ECT. A rise in ST is not essential for therapeutic effect but may represent an important marker of underlying neuronal state. The evidence reviewed in this article supports a link between neuroplastic effects of ECT and the evidenced rise in seizure threshold
Effectiveness of Ultrabrief R. Uni vs. Bilateral
ECT. McCormick et al . J ECT Dec 2009
Patients having high-dose UB-RUL ECT needed significantly more treatments than those on BL ECT 9.4 [3.3] vs 7.7 [2.8]
findings add to emerging story of reduced efficiency of UB-RUL vs BL electrode placement for an index course of ECT for the treatment of depression.
Practical considerations in the use of Ultra Brief ECT.Galletly, et al. Journal of ECT: March 2014
258 patients over 2 years in a private hospital receiving ECT.
Ultra Brief (UB) 0.3ms PW; Brief PW 1.0ms. All unilateral. UB 10.9 applications vs BPW 8.8 average. LOS for UB was 30.3 days vs 24.7 for BPW. NB In UK we use BPW bilateral at between
0.5ms and 1.0ms with 0.5ms for RUL.
Ultrabrief Pulse width vs Brief Pulse Efficacy of ultrabrief pulse electroconvulsive therapy for depression: A
systematic review Harm-Pieter Spaans J Affective Disorders Sep 2013 studies comparing ultrabrief pulse (UBP) versus brief pulse (BP) ECT in depression 2 RCTs one nonRCT prospective study using unilateral (UL) ECT, 2 RCT and 1
retrospective study using bilateral (BL) ECT comparing UBP with BP ECT. One UL randomized high quality study and one non-randomized study suggest an equal response and remission for both conditions. The number of treatment sessions to achieve remission using UBP is equal in one study and is higher in the second. Both BL studies, one of high quality, point to a lower efficacy for UBP ECT with a lower speed of remission.
Limitations: restricted review to the efficacy of UBP vs. BP ECT in depressed patients and did not address other clinically important issues eg cognitive adverse effects. A statistical meta-analysis was not possible, because of the heterogeneity & small number studies.
Conclusion: The literature shows no clear advantage for the efficacy of ultrabrief pulse over brief pulse ECT using unilateral as well as bilateral electrode placement. The increasing use of unilateral brief pulse ECT as first line method for depression is not supported by the current evidence.
summaryLength of seizure not related to effectSeizure adequacy related to extent to
which dose exceeds ST, especially with unilateral
Use unilateral if need to minimise cognitive adverse effects
Some patients will respond to bilateral but not unilateral ECT
Bifrontal vs bitemporal vs UL placement of electrodes Kellner et al. Bifrontal, bitemporal, and right
unilateral electrode placement in ECT: a randomised trial. B J Psychiatry 2010
RUL n=77(STx6); BF n=81, BT n=72 (STx1.5).
Remission rates: 55%, 61% and 64% respectively.
Not statistically different although BT faster NO difference cognitively across multiple
domains.
Bilateral vs unilateralUK ECT review group: Efficacy & safety
of ECT in depressive disorders: a systematic review & meta-analysis. Lancet March 2003
Bilateral ECT is moderately more effective than unilateral and high dose ECT is more effective than low dose
Bilateral vs unilateral: EFFECT-Dep trialMcLoughlin et al
presented at 28th European College of Neuropsychopharmacology (ECNP) EFFECT-Dep trial - a non-inferiority pragmatic study: 140 patients with depression
randomised to high-dose right unilat ECT (6 x ST) or to standard bitemporal ECT (1.5 x ST) Patients had either unipolar or bipolar depression, 20% had some element of psychosis. The primary outcome was change in the 24-item Ham DRS Secondary outcomes included various measures of cognition. no difference in either response or remission rates nor in relapse rates between two groups The overall response rate was 57%, and the overall remission rate was 44% no significant difference between the two groups in relapse rates at 3 or 6 months' follow-up cognitive side effects- unilateral group quicker immediate recovery of orientation after
individual treatments during the course of ECT at 19 minutes vs 26 minutes for the bitemporal group
No significant differences in other cognitive measures between the two groups with the exception of immediate verbal recall, which was superior in the unilateral group for the first 3 months, after which the difference disappeared.
Suggests that if a patient is referred for treatment-resistant depression start with high-dose unilateral ECT, especially if patients have cognitive issues
Summary: High-dose unilat ECT as effective as bilat & associated with fewer cognitive effects, especially autobiographic memory, the most controversial side effect associated with ECT
The practical administration of ECT
Preparation for ECT Full explanation (written & verbal) Consent - ongoing Physical assessment: History, examination &
investigations Documentation: ECT referral form,
anaesthetic proforma, blood results, ECG Baseline assessment of mood (eg MADRS) Baseline cognitive assessment (eg MMSE)
Prescription of ECTBilateral vs unilateralNumber of treatments - constant review
depending on response and side effectsMonitoring of mental state, mood
cognitive function, side effects, after every treatment
Administering ECT
•consent•physical examination & investigations•prepare patient•anaesthetic: O2, propofol, suxamethonium •mouthguard•Monitoring the seizure- clonus & EEG
Dose Titration: seizure threshold and therapeutic stimulusAim is to stimulate the brain electrically
in order to produce clinical improvementNot sufficient just to induce seizureClinically effective dose has to be
sufficiently suprathresholdBilateral ECT: 1.5 - 2 x STUnilateral ECT: 6 x ST
Effects of General Anesthetic Agents in Adults Receiving ECT:Journal of ECT: September 2008 Hooten et al
SYSTEMATIC REVIEW 41 randomized trials 14 induction agents Weighted mean difference for continuous variables Risk difference for dichotomous variables Crossover and parallel design combined using the inverse variance method Random effects model used throughoutRESULTS: Motor & EEG seizure duration; Emergence time ; Recovery time; Cardiac
arrhythmias ; Nausea and vomiting Motor & EEG seizure duration were longer with thiopentone, methohexitone &
etomidate than propofol. Propofol caused least problems with tachycardia & arrhythmias cf other agents Agents associated with longer seizures have longer emergence & recovery times.CONCLUSION: Using low-dose propofol with opioids such as remifentanil can produce good
seizure length increase.
Administering ECT cont’dStimulus selection/ dose titrationposition electrodesmonitor seizuremonitor recovery (c. 5% delirium) frequency & no. treatments record keeping
Technique in ECTClean scalpAttachment of EEG electrodesElectrode placement – uni vs. bilateralElectrical contact - firm application of
electrodes, rotation
Factors increasing seizure threshold Old Age Male gender Anticonvulsants Baldness Barbiturates Benzodiazepines Bones Recent ECT dehydration
Factors decreasing seizure thresholdCaffeineSSRI’sPhenothiazinesclozapineHypocapnia
Practical tips for EEG monitoring of ECT Prepare prefrontal and mastoid sites for EEG
electrodes Inspect EEG recording while the patient is still
awake, and make any necessary adjustments Record a few seconds of baseline EEG
immediately before electrical stimulation ‘Hands off’ during the termination phase of
EEG recording
Potential applications of ictal EEG, beyond length of seizure Inform optimal electrode placement Inform optimal electrical dosePredict eventual treatment response Inform adjustment of electrical dose
over a course of treatment
Reasons for a missed seizureECT techniqueMuscle relaxant (Hamilton Cuff)Electrical dose too low (subthreshold)All factors that raise threshold
Restimulation after a missed seizureWait 30 - 60 secondsRepeat hyperoxygenation Repeat, increasing the dose by 10-20%Up to maximum of 3 stimulations in one
treatment sessionFully review why the seizure was
difficult to produce
Adjustment of dose during course of ECTwhether generalized+ / - Seizure durationTonic / clonic phaseClinical response Cognitive side effects
ECT & Consent: NICE CG90Fully inform patient of risks & benefit &
document discussion regarding: risks associated with GAcurrent medical comorbiditiespotential adverse events esp. cognitive
impairment risks associated with not receiving ECT
Consent, capacity & ECT: scenariosAn informal patient with capacity
who gives or withholds consentAn informal patient without capacityA detained patient with capacity who
gives or withholds consentA detained patient without capacity
MHA 2007 amendments Section 27 inserts a new section 58A into the
1983 Act. That new section provides that ECT (& any other treatment provided for by regulations under subsection (1)(b)), can only be given when the patient either gives consent, or is incapable of giving consent & a SOAD authorises treatment
A SOAD must also authorise ECT for any patient under 18 years, whether detained or not
Emergency ECT for Detained Patients (S62): Patients who are liable to detention may be given
emergency ECT under section 62 Section 28 of the 2007 Act amended section 62 of
the 1983 Act (urgent treatment) so that, where the treatment is ECT, urgent treatment can only be given where it is immediately necessary to save life or to prevent a serious deterioration in the patient's condition.
This applies to patients with or without capacity there is no statutory limit on the number of ECT
treatments under section 62 (although custom was for max. two treatments)
Informal patient without capacity: MCA 2005 if not appropriate/necessary to use the MHA, can give ECT
under section 5 of the Mental Capacity Act. However, in keeping with the MCA, the “best interests” check-list should be followed and carefully documented, consult with carers, relatives, attorney under LPOA etc). If there is none available must involve an Independent Mental Capacity Advocate (IMCA)
If time allows, a non-statutory second opinion from a Consultant colleague should be sought.
Cannot give ECT if there is a valid & applicable advance decision made by the patient or the treatment would conflict with a decision made by a health & welfare deputy or donee of a LPOA, or there is an order from the COP against treatment
Restriction vs. deprivation of libertySupreme Court March 2014 “…under continuous supervision and
control and not free to leave..”
New Code of Practice MHAApril 2015 Multiple references to ECT in the new Code of Practice: 4.20 Patients must be told … • the circumstances (if any) in which they can be treated without their consent –
and when they have the right to refuse treatment • the role of second opinion appointed doctors (SOADs) and the circumstances
in which they may be involved, the rules on ECT and medication administered as part of ECT (see paragraphs
25.19 – 25.25). Patients who are eligible for IMHA services (qualifying patients): 6.10 Other patients (‘informal patients’) are eligible if they are: • being
considered for a treatment to which section 57 applies (see paragraphs 25.7 –25.10 and for under 18s 19.79), or • under 18 and being considered for ECT or any other treatment to which section 58A applies (see paragraphs 19.80 –19.88).
13.13 A person who has made a valid and applicable advance decision under the MCA, or for whom a decision has been taken by their attorney, to refuse ECT, cannot be given that treatment under section 58A of the Act although treatment can be given in specific emergency situations under section 62(1A).
CoP 2015: ECT MHA & MCA 13.63 ECT cannot be given to an individual who has the capacity to consent
to that treatment but refuses to do so, unless it is immediately necessary to save the patient’s life or to prevent a serious deterioration in the patient’s condition.
13.64 ECT can only be given to individuals who lack capacity if approved by a SOAD (detained patients)
paragraphs 25.19 – 25.25 for further information on ECT 13.65 If ECT is to be given to an individual who lacks capacity and is under
a DoLS authorisation or Court of Protection order, consideration should be given to seeking an independent second medical opinion before treatment which could, in principle, be given under the MCA (remembering that a DoLS authorisation only authorises the deprivation of liberty, not the treatment).
13.66 It is worth noting that ECT is likely to be considered under the MCA to be ‘serious medical treatment’ and that as such, if appropriate, an independent mental capacity advocate (IMCA) may need to be appointed.
Comment: it is implicit from this that ECT can be given under the MCA
CoP: ECT & Children 19.41 parental consent… is this a decision that a parent should reasonably be expected to
make? the more extreme the intervention, the greater the justification that will be required… careful consideration should be given to the appropriateness of relying on parental consent to authorise ECT
19.80 The Act provides specific safeguards in relation to ECT for patients who are under 18. 19.81 As with adults, children detained under MHA cannot be given ECT without their consent,
if they are capable of consenting to the treatment, unless it is emergency treatment (section 62). If they are not capable of consenting, or if it is emergency treatment, ECT may be given without consent in accordance with ch. 25 rules
19.82 Children and young people on a community treatment order (CTO) who are competent (children) or who have capacity (young people) cannot be given ECT without their consent, even in emergencies. If they are recalled to hospital ECT can be given in accordance with provisions under part 4 of the Act.
19.83 Whether or not they are detained under MHA, except where emergency treatment is given under section 62, no child can be given ECT without the approval of a SOAD.
19.84 The legal authority to give ECT to children and young people who are neither detained under the Act, nor subject to a CTO and who lack the capacity (young people) or the competence (children) to consent to ECT will need to be clarified. (The approval of a SOAD is not in itself sufficient authorisation for ECT to be given.) In the case of young people who lack capacity, the MCA could provide the necessary authority to give ECT, so long as this would not involve a deprivation of liberty.
CoPractice: ECT & Children 19.85 Although the Act does not prevent a person with parental responsibility from
consenting to ECT on behalf of a child who lacks competence, or young person who lacks capacity to consent and who not detained nor subject to a CTO, careful consideration should be given as to whether to rely on parental consent. This is because although there is no case law at present directly on this point, given the nature and invasiveness of ECT, it may lie outside the types of decision that parents can make on behalf of their child.
19.86 In cases where ECT cannot be given on the basis of either the child or young person’s consent, or parental consent, or the MCA, consideration should be given to whether the child or young person should be admitted under the Act for ECT, if the criteria are met (or recalled to hospital, in case of a community patient).
19.87 In cases where the Act is not applicable, court authorisation should be sought. Although the application to the court should be made before a SOAD is asked to approve the treatment the views of a SOAD should be sought before making the application as the court is likely to wish to consider a SOAD’s opinion before determining whether to authorise ECT. In practice, the issues the court is likely to address will mirror those that the SOAD is required to consider.
19.88 All children and young people, whether or not they are detained under the Act, are eligible for help from IMHAs if ECT is proposed and must be informed
Code of Practice 2015:ECT under section 58A
25.19 Section 58A applies to ECT and medication administered as part of ECT. It applies to detained patients and to all patients aged under 18 (whether or not detained). The key differences from section 58 are that: • patients who have the capacity to consent to or refuse treatment may not be given treatment under section 58A unless they do consent • no patient aged under 18 can be given treatment under section 58A unless a SOAD has certified that the treatment is appropriate, and • there is no initial three-month period during which a certificate is not needed (even for the medication administered as part of the ECT).
25.21 A patient who is consenting may not be given treatment under section 58A unless the clinician in charge, or a SOAD, has certified that the patient has the capacity to consent and has done so. If the patient under 18, only a SOAD may give the certificate, if appropriate.
25.22 A patient who lacks the capacity to consent may not be given treatment under section 58A unless a SOAD certifies that the patient lacks capacity, that the treatment is appropriate , no valid and applicable advance decision has been made by the patient under the MCA refusing the treatment, no suitably authorised attorney or deputy objects to the treatment on the patient’s behalf, and the treatment would not conflict with a decision of the Court of Protection
25.23 In all cases, SOADs should indicate the maximum number of ECT treatments 25.24 For children and young people under 18, a SOAD certificate by itself is not sufficient to
authorise the treatment, unless they are detained. Clinicians must also have the patient’s own consent or some other legal authority
25.25 Whether or not section 58A applies, patients of all ages who are to be treated with ECT should be given written information before treatment starts which helps them to understand and remember, both during and after the course of ECT, the advice given about its nature, purpose and likely effects.
Care Quality Commission: CQC Considerations
HCC Core Standards (as was) are used to judge Trusts
Given a Colour rating Red Amber or GreenMust be compliant with all but one Core Standard to
gain GreenAll but two: AmberAll but three: red Impacts on
› RMST Grading› Foundation Status as judged by Monitor
CQC Core StandardsWhat relevance to ECT?
Core standard C5a- NICE technology appraisals Core standard 4b- Acquisition & use of Medical
Devices Healthcare organisations keep patients, staff and visitors safe by having systems to ensure that all risks associated with the acquisition and use of medical devices are minimised.
CQC Core Standard C13b – consent Issues related to policies and procedures that ensure
proper consent practice is carried outProper use of MHA 1983 Part IV
ECTAS membership seen as a well evidenced form of adherence to this
ECT clinics & trainingPsychiatric traineesMedical & nursing studentsAMHPsOther members MDT
ECT Competencies: RCPsych.Describes competencies from FY; CT;
ST; Consultant to ECT Consultant
The trainee by year 3 ought to be able to administer ECT without direct supervision, prepare patients for ECT, explain to patients and relatives about ECT, its indications and broad place within psychiatric treatment. Trainees ought to be able to monitor a patient’s mental state and cognitive functioning during a course of ECT.
Acknowledgement: Dr Andrew Easton for use of selected slides
Thank you

















