85
The Art and Science of Electrosurgery and Argon Plasma Coagulation in Endoscopy Rhonda Delcampo BSN, RN, CGRN
The Art and Science of Electrosurgery and Argon Plasma Coagulation in
Endoscopy
Rhonda Delcampo BSN RN CGRN
Electrosurgical Procedures An Art and Sciencehellip
3
My MotherhellipMy MentorhellipMy Teacher
Disclosureother pertinent facts
4
Employed full-time with ERBE-USA as a Clinical Education Manager Program has been approved as a GI-Specific contact hour program for 10 hours by the American Board for Certification of Gastroenterology Nurses (ABCGN) Separate sign-in evaluation and certificate
Objectives
1 Discuss the basics of electricity and how itrsquos adapted for use in the human body
2 Describe how Electrosurgery is used therapeutically and the variables that affect it
3 Discuss how to provide safe electrosurgical care to patients 4 Describe the basic principles and components of Argon Plasma Coagulation (APC) and how itrsquos applied safely in clinical applications
How cauterization all started
Various tools were heated with fire -17th century
History - Hemostasis by cauterization
1848 Galvanocautery
Christian Heinrich Erbe
von Bruns MD
These devices were comprised of a metal wire heated by means of an electrical galvanic (direct) current - used for coagulation and separation of biological tissue and was referred to as galvanocautery
History of Electrosurgery
In 1978 Dr Glover published an article on the use of thermal knives in comparison to other modalities and stated ldquoThere is no group of instruments in the surgical armamentarium that is used as frequently and understood as poorly as Electrosurgery unitshelliprdquo
1923 Electrosurgical Unit (ESU) in
Europe
Christian Otto Erbe
1926 Electrosurgical Unit in the
US
William T Bovie PhD
Harvey Cushing MD
1971 ldquoplasma scalpelrdquo for
surgery
JL Glover MD
1991 APC probes for flexible
endoscopy
ERBE GmbH
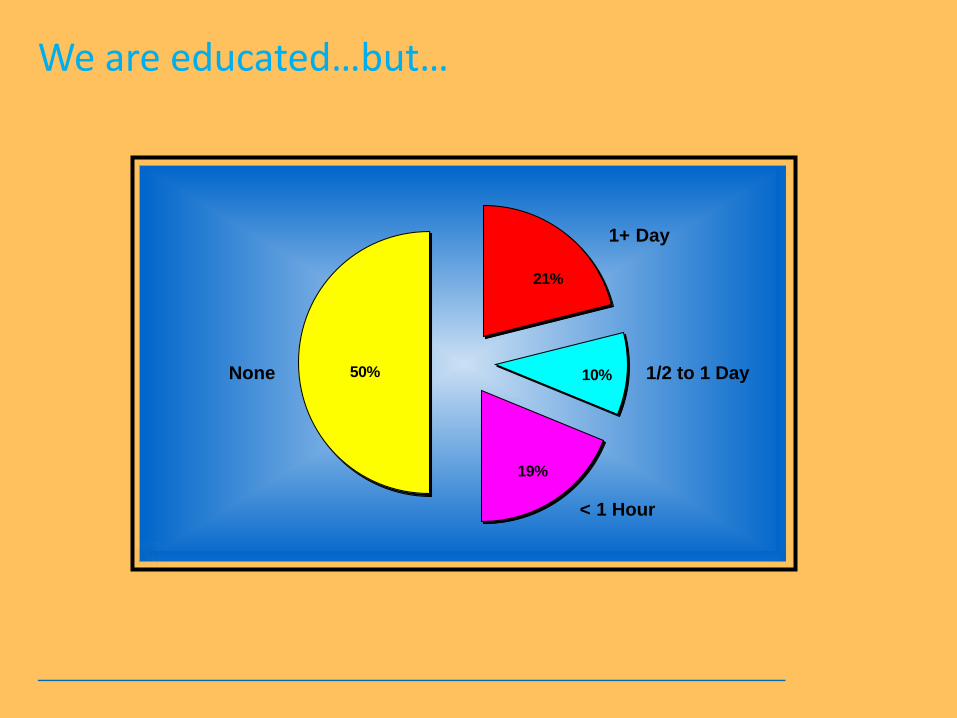
We are educatedhellipbuthellip
50
21
10
19
None 12 to 1 Day
1+ Day
lt 1 Hour
Electrosurgical Procedures An Art and Sciencehellip
3
My MotherhellipMy MentorhellipMy Teacher
Disclosureother pertinent facts
4
Employed full-time with ERBE-USA as a Clinical Education Manager Program has been approved as a GI-Specific contact hour program for 10 hours by the American Board for Certification of Gastroenterology Nurses (ABCGN) Separate sign-in evaluation and certificate
Objectives
1 Discuss the basics of electricity and how itrsquos adapted for use in the human body
2 Describe how Electrosurgery is used therapeutically and the variables that affect it
3 Discuss how to provide safe electrosurgical care to patients 4 Describe the basic principles and components of Argon Plasma Coagulation (APC) and how itrsquos applied safely in clinical applications
How cauterization all started
Various tools were heated with fire -17th century
History - Hemostasis by cauterization
1848 Galvanocautery
Christian Heinrich Erbe
von Bruns MD
These devices were comprised of a metal wire heated by means of an electrical galvanic (direct) current - used for coagulation and separation of biological tissue and was referred to as galvanocautery
History of Electrosurgery
In 1978 Dr Glover published an article on the use of thermal knives in comparison to other modalities and stated ldquoThere is no group of instruments in the surgical armamentarium that is used as frequently and understood as poorly as Electrosurgery unitshelliprdquo
1923 Electrosurgical Unit (ESU) in
Europe
Christian Otto Erbe
1926 Electrosurgical Unit in the
US
William T Bovie PhD
Harvey Cushing MD
1971 ldquoplasma scalpelrdquo for
surgery
JL Glover MD
1991 APC probes for flexible
endoscopy
ERBE GmbH
We are educatedhellipbuthellip
50
21
10
19
None 12 to 1 Day
1+ Day
lt 1 Hour
3
My MotherhellipMy MentorhellipMy Teacher
Disclosureother pertinent facts
4
Employed full-time with ERBE-USA as a Clinical Education Manager Program has been approved as a GI-Specific contact hour program for 10 hours by the American Board for Certification of Gastroenterology Nurses (ABCGN) Separate sign-in evaluation and certificate
Objectives
1 Discuss the basics of electricity and how itrsquos adapted for use in the human body
2 Describe how Electrosurgery is used therapeutically and the variables that affect it
3 Discuss how to provide safe electrosurgical care to patients 4 Describe the basic principles and components of Argon Plasma Coagulation (APC) and how itrsquos applied safely in clinical applications
How cauterization all started
Various tools were heated with fire -17th century
History - Hemostasis by cauterization
1848 Galvanocautery
Christian Heinrich Erbe
von Bruns MD
These devices were comprised of a metal wire heated by means of an electrical galvanic (direct) current - used for coagulation and separation of biological tissue and was referred to as galvanocautery
History of Electrosurgery
In 1978 Dr Glover published an article on the use of thermal knives in comparison to other modalities and stated ldquoThere is no group of instruments in the surgical armamentarium that is used as frequently and understood as poorly as Electrosurgery unitshelliprdquo
1923 Electrosurgical Unit (ESU) in
Europe
Christian Otto Erbe
1926 Electrosurgical Unit in the
US
William T Bovie PhD
Harvey Cushing MD
1971 ldquoplasma scalpelrdquo for
surgery
JL Glover MD
1991 APC probes for flexible
endoscopy
ERBE GmbH
We are educatedhellipbuthellip
50
21
10
19
None 12 to 1 Day
1+ Day
lt 1 Hour

Disclosureother pertinent facts
4
Employed full-time with ERBE-USA as a Clinical Education Manager Program has been approved as a GI-Specific contact hour program for 10 hours by the American Board for Certification of Gastroenterology Nurses (ABCGN) Separate sign-in evaluation and certificate
Objectives
1 Discuss the basics of electricity and how itrsquos adapted for use in the human body
2 Describe how Electrosurgery is used therapeutically and the variables that affect it
3 Discuss how to provide safe electrosurgical care to patients 4 Describe the basic principles and components of Argon Plasma Coagulation (APC) and how itrsquos applied safely in clinical applications
How cauterization all started
Various tools were heated with fire -17th century
History - Hemostasis by cauterization
1848 Galvanocautery
Christian Heinrich Erbe
von Bruns MD
These devices were comprised of a metal wire heated by means of an electrical galvanic (direct) current - used for coagulation and separation of biological tissue and was referred to as galvanocautery
History of Electrosurgery
In 1978 Dr Glover published an article on the use of thermal knives in comparison to other modalities and stated ldquoThere is no group of instruments in the surgical armamentarium that is used as frequently and understood as poorly as Electrosurgery unitshelliprdquo
1923 Electrosurgical Unit (ESU) in
Europe
Christian Otto Erbe
1926 Electrosurgical Unit in the
US
William T Bovie PhD
Harvey Cushing MD
1971 ldquoplasma scalpelrdquo for
surgery
JL Glover MD
1991 APC probes for flexible
endoscopy
ERBE GmbH
We are educatedhellipbuthellip
50
21
10
19
None 12 to 1 Day
1+ Day
lt 1 Hour

Objectives
1 Discuss the basics of electricity and how itrsquos adapted for use in the human body
2 Describe how Electrosurgery is used therapeutically and the variables that affect it
3 Discuss how to provide safe electrosurgical care to patients 4 Describe the basic principles and components of Argon Plasma Coagulation (APC) and how itrsquos applied safely in clinical applications
How cauterization all started
Various tools were heated with fire -17th century
History - Hemostasis by cauterization
1848 Galvanocautery
Christian Heinrich Erbe
von Bruns MD
These devices were comprised of a metal wire heated by means of an electrical galvanic (direct) current - used for coagulation and separation of biological tissue and was referred to as galvanocautery
History of Electrosurgery
In 1978 Dr Glover published an article on the use of thermal knives in comparison to other modalities and stated ldquoThere is no group of instruments in the surgical armamentarium that is used as frequently and understood as poorly as Electrosurgery unitshelliprdquo
1923 Electrosurgical Unit (ESU) in
Europe
Christian Otto Erbe
1926 Electrosurgical Unit in the
US
William T Bovie PhD
Harvey Cushing MD
1971 ldquoplasma scalpelrdquo for
surgery
JL Glover MD
1991 APC probes for flexible
endoscopy
ERBE GmbH
We are educatedhellipbuthellip
50
21
10
19
None 12 to 1 Day
1+ Day
lt 1 Hour

How cauterization all started
Various tools were heated with fire -17th century
History - Hemostasis by cauterization
1848 Galvanocautery
Christian Heinrich Erbe
von Bruns MD
These devices were comprised of a metal wire heated by means of an electrical galvanic (direct) current - used for coagulation and separation of biological tissue and was referred to as galvanocautery
History of Electrosurgery
In 1978 Dr Glover published an article on the use of thermal knives in comparison to other modalities and stated ldquoThere is no group of instruments in the surgical armamentarium that is used as frequently and understood as poorly as Electrosurgery unitshelliprdquo
1923 Electrosurgical Unit (ESU) in
Europe
Christian Otto Erbe
1926 Electrosurgical Unit in the
US
William T Bovie PhD
Harvey Cushing MD
1971 ldquoplasma scalpelrdquo for
surgery
JL Glover MD
1991 APC probes for flexible
endoscopy
ERBE GmbH
We are educatedhellipbuthellip
50
21
10
19
None 12 to 1 Day
1+ Day
lt 1 Hour
History - Hemostasis by cauterization
1848 Galvanocautery
Christian Heinrich Erbe
von Bruns MD
These devices were comprised of a metal wire heated by means of an electrical galvanic (direct) current - used for coagulation and separation of biological tissue and was referred to as galvanocautery
History of Electrosurgery
In 1978 Dr Glover published an article on the use of thermal knives in comparison to other modalities and stated ldquoThere is no group of instruments in the surgical armamentarium that is used as frequently and understood as poorly as Electrosurgery unitshelliprdquo
1923 Electrosurgical Unit (ESU) in
Europe
Christian Otto Erbe
1926 Electrosurgical Unit in the
US
William T Bovie PhD
Harvey Cushing MD
1971 ldquoplasma scalpelrdquo for
surgery
JL Glover MD
1991 APC probes for flexible
endoscopy
ERBE GmbH
We are educatedhellipbuthellip
50
21
10
19
None 12 to 1 Day
1+ Day
lt 1 Hour

History of Electrosurgery
In 1978 Dr Glover published an article on the use of thermal knives in comparison to other modalities and stated ldquoThere is no group of instruments in the surgical armamentarium that is used as frequently and understood as poorly as Electrosurgery unitshelliprdquo
1923 Electrosurgical Unit (ESU) in
Europe
Christian Otto Erbe
1926 Electrosurgical Unit in the
US
William T Bovie PhD
Harvey Cushing MD
1971 ldquoplasma scalpelrdquo for
surgery
JL Glover MD
1991 APC probes for flexible
endoscopy
ERBE GmbH
We are educatedhellipbuthellip
50
21
10
19
None 12 to 1 Day
1+ Day
lt 1 Hour
We are educatedhellipbuthellip
50
21
10
19
None 12 to 1 Day
1+ Day
lt 1 Hour

Electrocautery vs Electrosurgeryhellip
350 kHz
Direct Current (Electrocautery)
Alternating Current (Electrosurgery)
Electrocautery bull Uses direct current bull Often used inaccurately to describe ldquoElectrosurgeryrdquo bull Current does not enter the patientrsquos body ndash only the heated wire tip comes in contact with tissue Electrosurgery bull Uses High-Frequency Alternating Current (AC) bull The AC Circuit must be completed includes the electrosurgical generator active electrode the patient and return electrode
hellipthere is a difference
Using High-Frequency Alternating Current
54-880 MHz
60 Hz 100000 Hz 350000 Hz
ESUrsquos
Therapeutic Effect
550-1550 kHz
Household Neuromuscular stimulation
AM Radio
TV
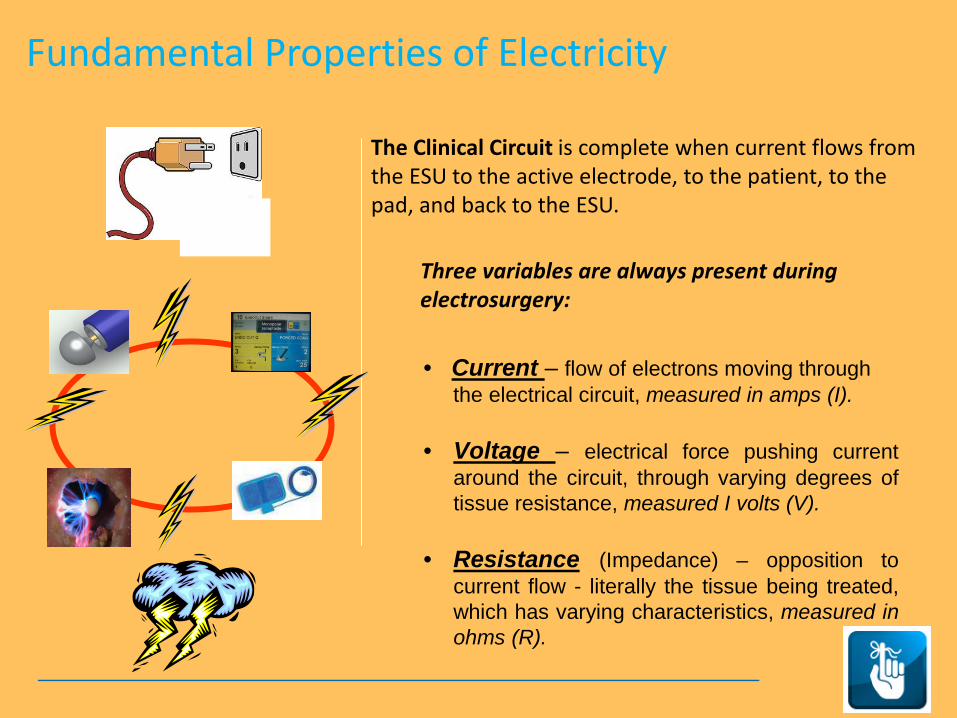
Three variables are always present during electrosurgery
Fundamental Properties of Electricity
bull Current ndash flow of electrons moving through the electrical circuit measured in amps (I) bull Voltage ndash electrical force pushing current
around the circuit through varying degrees of tissue resistance measured I volts (V)
bull Resistance (Impedance) ndash opposition to current flow - literally the tissue being treated which has varying characteristics measured in ohms (R)
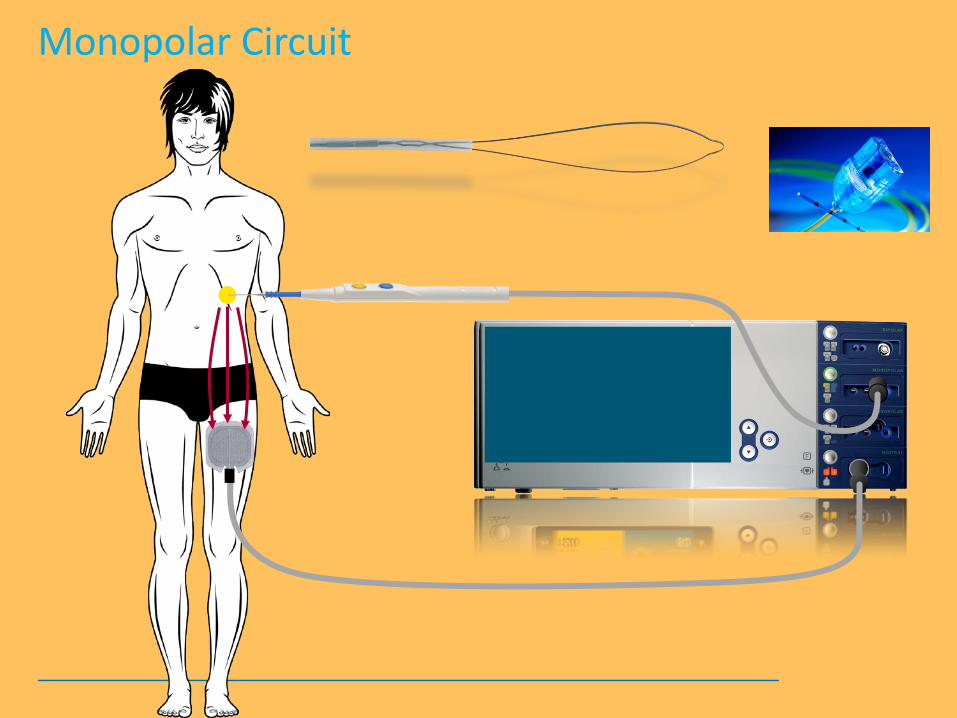
The Clinical Circuit is complete when current flows from the ESU to the active electrode to the patient to the pad and back to the ESU
Volunteers
13
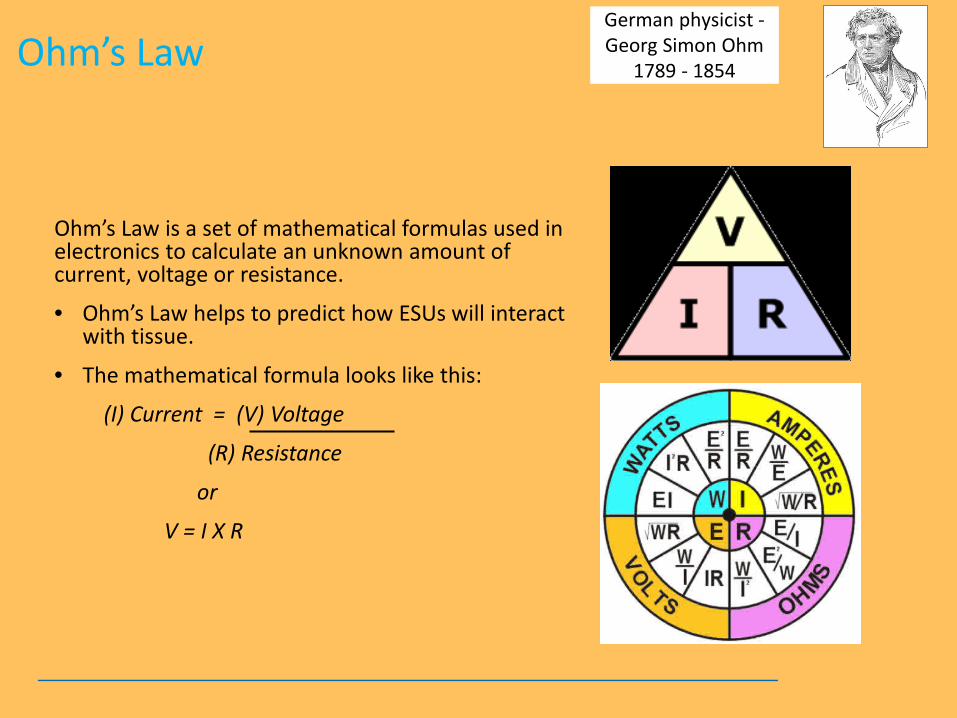
Ohmrsquos Law
Ohmrsquos Law is a set of mathematical formulas used in electronics to calculate an unknown amount of current voltage or resistance
bull Ohmrsquos Law helps to predict how ESUs will interact with tissue
bull The mathematical formula looks like this
(I) Current = (V) Voltage
(R) Resistance
or
V = I X R
German physicist - Georg Simon Ohm
1789 - 1854
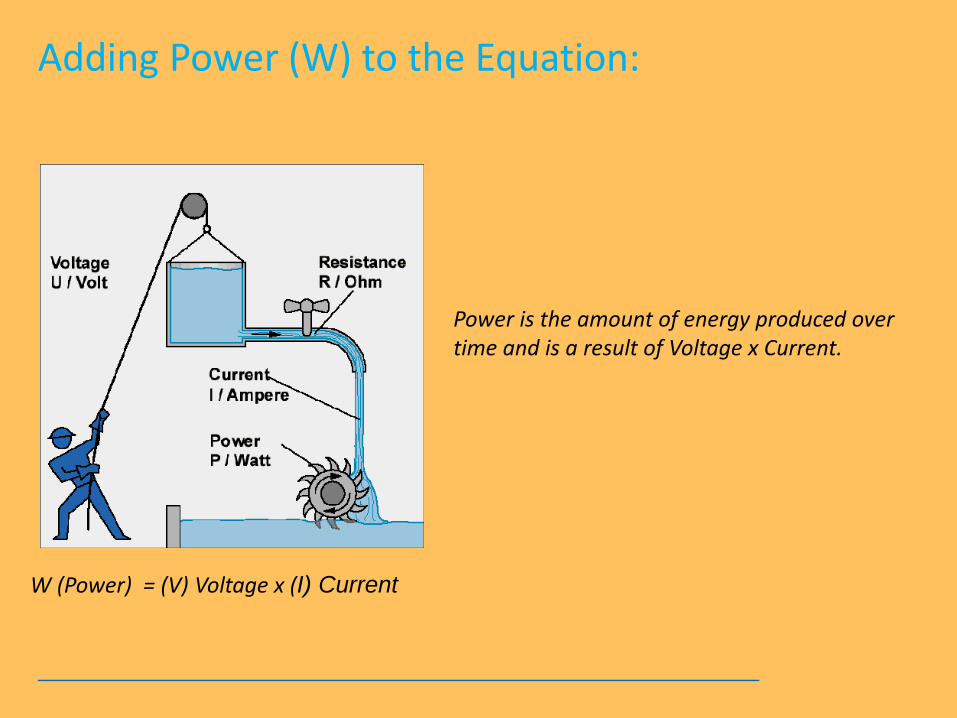
Adding Power (W) to the Equation
Power is the amount of energy produced over time and is a result of Voltage x Current
W (Power) = (V) Voltage x (I) Current
Types of Electrosurgical Generators
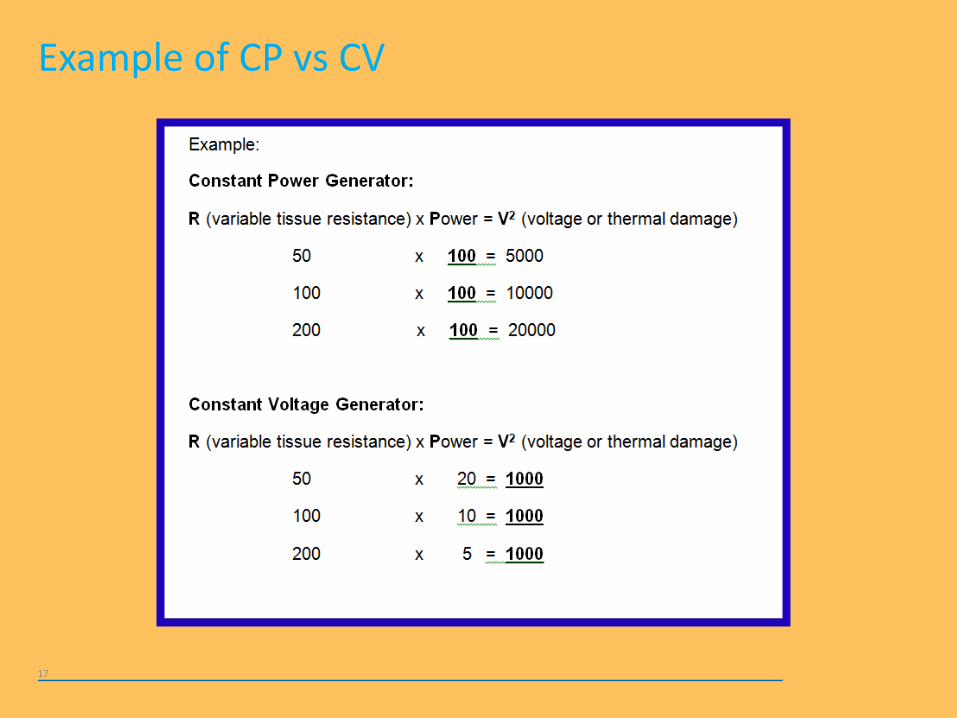
bull The voltage remains constant to maintain consistent tissue effect regardless of changes in tissue resistance (muscle fatty tissue)
bull The power (watts) automatically adjusts in response to the tissue impedancecircuit variables
Constant Voltage
bull Watts (power) setting is chosen bull The Watts remain constant bull Voltage varies to maintain Watts bull All tissue is treated with same Wattage
Constant Power
Example of CP vs CV
17
Monopolar Circuit
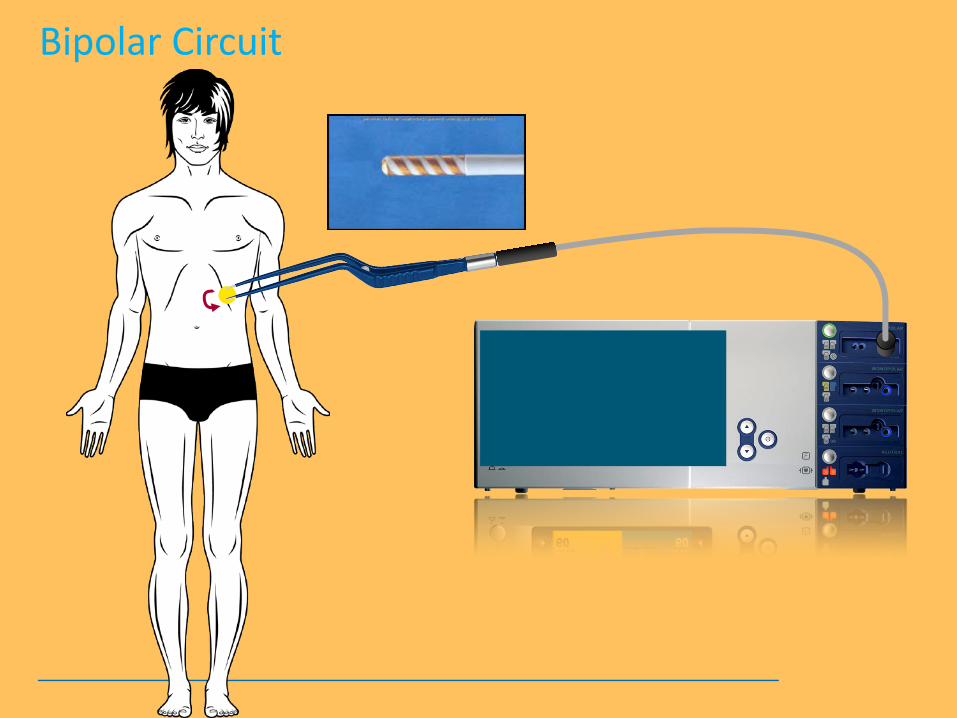
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
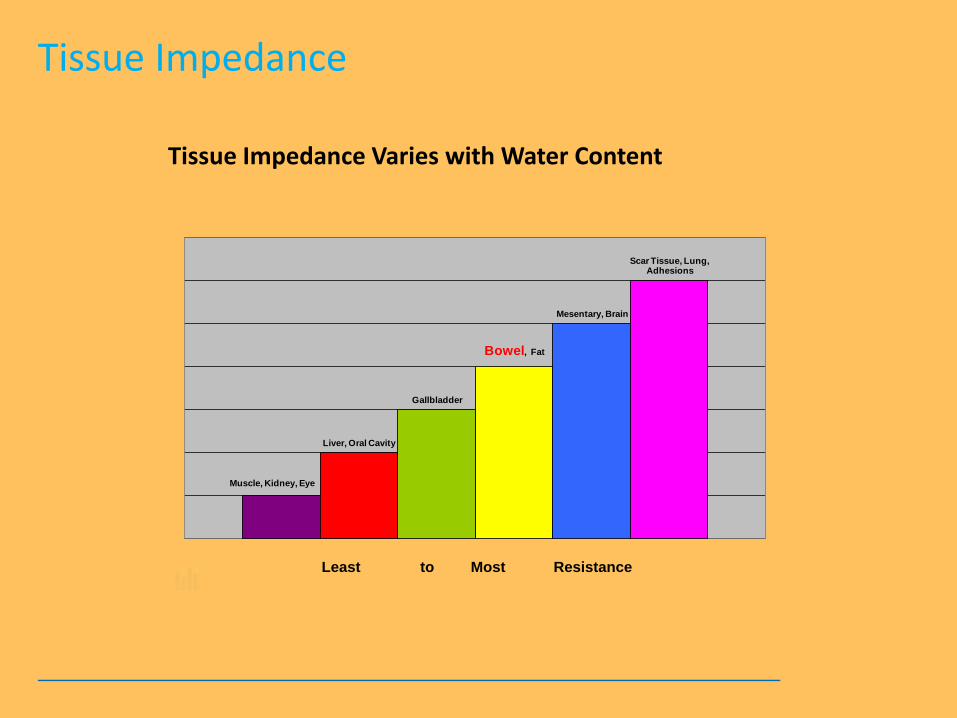
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance
| 21 | 10 | 19 | 50 |
| 021 | |
| 01 | |
| 019 | |
| 05 |

Electrocautery vs Electrosurgeryhellip
350 kHz
Direct Current (Electrocautery)
Alternating Current (Electrosurgery)
Electrocautery bull Uses direct current bull Often used inaccurately to describe ldquoElectrosurgeryrdquo bull Current does not enter the patientrsquos body ndash only the heated wire tip comes in contact with tissue Electrosurgery bull Uses High-Frequency Alternating Current (AC) bull The AC Circuit must be completed includes the electrosurgical generator active electrode the patient and return electrode
hellipthere is a difference
Using High-Frequency Alternating Current
54-880 MHz
60 Hz 100000 Hz 350000 Hz
ESUrsquos
Therapeutic Effect
550-1550 kHz
Household Neuromuscular stimulation
AM Radio
TV
Three variables are always present during electrosurgery
Fundamental Properties of Electricity
bull Current ndash flow of electrons moving through the electrical circuit measured in amps (I) bull Voltage ndash electrical force pushing current
around the circuit through varying degrees of tissue resistance measured I volts (V)
bull Resistance (Impedance) ndash opposition to current flow - literally the tissue being treated which has varying characteristics measured in ohms (R)
The Clinical Circuit is complete when current flows from the ESU to the active electrode to the patient to the pad and back to the ESU
Volunteers
13
Ohmrsquos Law
Ohmrsquos Law is a set of mathematical formulas used in electronics to calculate an unknown amount of current voltage or resistance
bull Ohmrsquos Law helps to predict how ESUs will interact with tissue
bull The mathematical formula looks like this
(I) Current = (V) Voltage
(R) Resistance
or
V = I X R
German physicist - Georg Simon Ohm
1789 - 1854
Adding Power (W) to the Equation
Power is the amount of energy produced over time and is a result of Voltage x Current
W (Power) = (V) Voltage x (I) Current
Types of Electrosurgical Generators
bull The voltage remains constant to maintain consistent tissue effect regardless of changes in tissue resistance (muscle fatty tissue)
bull The power (watts) automatically adjusts in response to the tissue impedancecircuit variables
Constant Voltage
bull Watts (power) setting is chosen bull The Watts remain constant bull Voltage varies to maintain Watts bull All tissue is treated with same Wattage
Constant Power
Example of CP vs CV
17
Monopolar Circuit
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance
| 21 | 10 | 19 | 50 |
Electrocautery vs Electrosurgeryhellip
350 kHz
Direct Current (Electrocautery)
Alternating Current (Electrosurgery)
Electrocautery bull Uses direct current bull Often used inaccurately to describe ldquoElectrosurgeryrdquo bull Current does not enter the patientrsquos body ndash only the heated wire tip comes in contact with tissue Electrosurgery bull Uses High-Frequency Alternating Current (AC) bull The AC Circuit must be completed includes the electrosurgical generator active electrode the patient and return electrode
hellipthere is a difference
Using High-Frequency Alternating Current
54-880 MHz
60 Hz 100000 Hz 350000 Hz
ESUrsquos
Therapeutic Effect
550-1550 kHz
Household Neuromuscular stimulation
AM Radio
TV
Three variables are always present during electrosurgery
Fundamental Properties of Electricity
bull Current ndash flow of electrons moving through the electrical circuit measured in amps (I) bull Voltage ndash electrical force pushing current
around the circuit through varying degrees of tissue resistance measured I volts (V)
bull Resistance (Impedance) ndash opposition to current flow - literally the tissue being treated which has varying characteristics measured in ohms (R)
The Clinical Circuit is complete when current flows from the ESU to the active electrode to the patient to the pad and back to the ESU
Volunteers
13
Ohmrsquos Law
Ohmrsquos Law is a set of mathematical formulas used in electronics to calculate an unknown amount of current voltage or resistance
bull Ohmrsquos Law helps to predict how ESUs will interact with tissue
bull The mathematical formula looks like this
(I) Current = (V) Voltage
(R) Resistance
or
V = I X R
German physicist - Georg Simon Ohm
1789 - 1854
Adding Power (W) to the Equation
Power is the amount of energy produced over time and is a result of Voltage x Current
W (Power) = (V) Voltage x (I) Current
Types of Electrosurgical Generators
bull The voltage remains constant to maintain consistent tissue effect regardless of changes in tissue resistance (muscle fatty tissue)
bull The power (watts) automatically adjusts in response to the tissue impedancecircuit variables
Constant Voltage
bull Watts (power) setting is chosen bull The Watts remain constant bull Voltage varies to maintain Watts bull All tissue is treated with same Wattage
Constant Power
Example of CP vs CV
17
Monopolar Circuit
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance
Electrocautery vs Electrosurgeryhellip
350 kHz
Direct Current (Electrocautery)
Alternating Current (Electrosurgery)
Electrocautery bull Uses direct current bull Often used inaccurately to describe ldquoElectrosurgeryrdquo bull Current does not enter the patientrsquos body ndash only the heated wire tip comes in contact with tissue Electrosurgery bull Uses High-Frequency Alternating Current (AC) bull The AC Circuit must be completed includes the electrosurgical generator active electrode the patient and return electrode
hellipthere is a difference
Using High-Frequency Alternating Current
54-880 MHz
60 Hz 100000 Hz 350000 Hz
ESUrsquos
Therapeutic Effect
550-1550 kHz
Household Neuromuscular stimulation
AM Radio
TV
Three variables are always present during electrosurgery
Fundamental Properties of Electricity
bull Current ndash flow of electrons moving through the electrical circuit measured in amps (I) bull Voltage ndash electrical force pushing current
around the circuit through varying degrees of tissue resistance measured I volts (V)
bull Resistance (Impedance) ndash opposition to current flow - literally the tissue being treated which has varying characteristics measured in ohms (R)
The Clinical Circuit is complete when current flows from the ESU to the active electrode to the patient to the pad and back to the ESU
Volunteers
13
Ohmrsquos Law
Ohmrsquos Law is a set of mathematical formulas used in electronics to calculate an unknown amount of current voltage or resistance
bull Ohmrsquos Law helps to predict how ESUs will interact with tissue
bull The mathematical formula looks like this
(I) Current = (V) Voltage
(R) Resistance
or
V = I X R
German physicist - Georg Simon Ohm
1789 - 1854
Adding Power (W) to the Equation
Power is the amount of energy produced over time and is a result of Voltage x Current
W (Power) = (V) Voltage x (I) Current
Types of Electrosurgical Generators
bull The voltage remains constant to maintain consistent tissue effect regardless of changes in tissue resistance (muscle fatty tissue)
bull The power (watts) automatically adjusts in response to the tissue impedancecircuit variables
Constant Voltage
bull Watts (power) setting is chosen bull The Watts remain constant bull Voltage varies to maintain Watts bull All tissue is treated with same Wattage
Constant Power
Example of CP vs CV
17
Monopolar Circuit
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance
Electrocautery vs Electrosurgeryhellip
350 kHz
Direct Current (Electrocautery)
Alternating Current (Electrosurgery)
Electrocautery bull Uses direct current bull Often used inaccurately to describe ldquoElectrosurgeryrdquo bull Current does not enter the patientrsquos body ndash only the heated wire tip comes in contact with tissue Electrosurgery bull Uses High-Frequency Alternating Current (AC) bull The AC Circuit must be completed includes the electrosurgical generator active electrode the patient and return electrode
hellipthere is a difference
Using High-Frequency Alternating Current
54-880 MHz
60 Hz 100000 Hz 350000 Hz
ESUrsquos
Therapeutic Effect
550-1550 kHz
Household Neuromuscular stimulation
AM Radio
TV
Three variables are always present during electrosurgery
Fundamental Properties of Electricity
bull Current ndash flow of electrons moving through the electrical circuit measured in amps (I) bull Voltage ndash electrical force pushing current
around the circuit through varying degrees of tissue resistance measured I volts (V)
bull Resistance (Impedance) ndash opposition to current flow - literally the tissue being treated which has varying characteristics measured in ohms (R)
The Clinical Circuit is complete when current flows from the ESU to the active electrode to the patient to the pad and back to the ESU
Volunteers
13
Ohmrsquos Law
Ohmrsquos Law is a set of mathematical formulas used in electronics to calculate an unknown amount of current voltage or resistance
bull Ohmrsquos Law helps to predict how ESUs will interact with tissue
bull The mathematical formula looks like this
(I) Current = (V) Voltage
(R) Resistance
or
V = I X R
German physicist - Georg Simon Ohm
1789 - 1854
Adding Power (W) to the Equation
Power is the amount of energy produced over time and is a result of Voltage x Current
W (Power) = (V) Voltage x (I) Current
Types of Electrosurgical Generators
bull The voltage remains constant to maintain consistent tissue effect regardless of changes in tissue resistance (muscle fatty tissue)
bull The power (watts) automatically adjusts in response to the tissue impedancecircuit variables
Constant Voltage
bull Watts (power) setting is chosen bull The Watts remain constant bull Voltage varies to maintain Watts bull All tissue is treated with same Wattage
Constant Power
Example of CP vs CV
17
Monopolar Circuit
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance
Electrocautery vs Electrosurgeryhellip
350 kHz
Direct Current (Electrocautery)
Alternating Current (Electrosurgery)
Electrocautery bull Uses direct current bull Often used inaccurately to describe ldquoElectrosurgeryrdquo bull Current does not enter the patientrsquos body ndash only the heated wire tip comes in contact with tissue Electrosurgery bull Uses High-Frequency Alternating Current (AC) bull The AC Circuit must be completed includes the electrosurgical generator active electrode the patient and return electrode
hellipthere is a difference
Using High-Frequency Alternating Current
54-880 MHz
60 Hz 100000 Hz 350000 Hz
ESUrsquos
Therapeutic Effect
550-1550 kHz
Household Neuromuscular stimulation
AM Radio
TV
Three variables are always present during electrosurgery
Fundamental Properties of Electricity
bull Current ndash flow of electrons moving through the electrical circuit measured in amps (I) bull Voltage ndash electrical force pushing current
around the circuit through varying degrees of tissue resistance measured I volts (V)
bull Resistance (Impedance) ndash opposition to current flow - literally the tissue being treated which has varying characteristics measured in ohms (R)
The Clinical Circuit is complete when current flows from the ESU to the active electrode to the patient to the pad and back to the ESU
Volunteers
13
Ohmrsquos Law
Ohmrsquos Law is a set of mathematical formulas used in electronics to calculate an unknown amount of current voltage or resistance
bull Ohmrsquos Law helps to predict how ESUs will interact with tissue
bull The mathematical formula looks like this
(I) Current = (V) Voltage
(R) Resistance
or
V = I X R
German physicist - Georg Simon Ohm
1789 - 1854
Adding Power (W) to the Equation
Power is the amount of energy produced over time and is a result of Voltage x Current
W (Power) = (V) Voltage x (I) Current
Types of Electrosurgical Generators
bull The voltage remains constant to maintain consistent tissue effect regardless of changes in tissue resistance (muscle fatty tissue)
bull The power (watts) automatically adjusts in response to the tissue impedancecircuit variables
Constant Voltage
bull Watts (power) setting is chosen bull The Watts remain constant bull Voltage varies to maintain Watts bull All tissue is treated with same Wattage
Constant Power
Example of CP vs CV
17
Monopolar Circuit
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance

Using High-Frequency Alternating Current
54-880 MHz
60 Hz 100000 Hz 350000 Hz
ESUrsquos
Therapeutic Effect
550-1550 kHz
Household Neuromuscular stimulation
AM Radio
TV
Three variables are always present during electrosurgery
Fundamental Properties of Electricity
bull Current ndash flow of electrons moving through the electrical circuit measured in amps (I) bull Voltage ndash electrical force pushing current
around the circuit through varying degrees of tissue resistance measured I volts (V)
bull Resistance (Impedance) ndash opposition to current flow - literally the tissue being treated which has varying characteristics measured in ohms (R)
The Clinical Circuit is complete when current flows from the ESU to the active electrode to the patient to the pad and back to the ESU
Volunteers
13
Ohmrsquos Law
Ohmrsquos Law is a set of mathematical formulas used in electronics to calculate an unknown amount of current voltage or resistance
bull Ohmrsquos Law helps to predict how ESUs will interact with tissue
bull The mathematical formula looks like this
(I) Current = (V) Voltage
(R) Resistance
or
V = I X R
German physicist - Georg Simon Ohm
1789 - 1854
Adding Power (W) to the Equation
Power is the amount of energy produced over time and is a result of Voltage x Current
W (Power) = (V) Voltage x (I) Current
Types of Electrosurgical Generators
bull The voltage remains constant to maintain consistent tissue effect regardless of changes in tissue resistance (muscle fatty tissue)
bull The power (watts) automatically adjusts in response to the tissue impedancecircuit variables
Constant Voltage
bull Watts (power) setting is chosen bull The Watts remain constant bull Voltage varies to maintain Watts bull All tissue is treated with same Wattage
Constant Power
Example of CP vs CV
17
Monopolar Circuit
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance
Three variables are always present during electrosurgery
Fundamental Properties of Electricity
bull Current ndash flow of electrons moving through the electrical circuit measured in amps (I) bull Voltage ndash electrical force pushing current
around the circuit through varying degrees of tissue resistance measured I volts (V)
bull Resistance (Impedance) ndash opposition to current flow - literally the tissue being treated which has varying characteristics measured in ohms (R)
The Clinical Circuit is complete when current flows from the ESU to the active electrode to the patient to the pad and back to the ESU
Volunteers
13
Ohmrsquos Law
Ohmrsquos Law is a set of mathematical formulas used in electronics to calculate an unknown amount of current voltage or resistance
bull Ohmrsquos Law helps to predict how ESUs will interact with tissue
bull The mathematical formula looks like this
(I) Current = (V) Voltage
(R) Resistance
or
V = I X R
German physicist - Georg Simon Ohm
1789 - 1854
Adding Power (W) to the Equation
Power is the amount of energy produced over time and is a result of Voltage x Current
W (Power) = (V) Voltage x (I) Current
Types of Electrosurgical Generators
bull The voltage remains constant to maintain consistent tissue effect regardless of changes in tissue resistance (muscle fatty tissue)
bull The power (watts) automatically adjusts in response to the tissue impedancecircuit variables
Constant Voltage
bull Watts (power) setting is chosen bull The Watts remain constant bull Voltage varies to maintain Watts bull All tissue is treated with same Wattage
Constant Power
Example of CP vs CV
17
Monopolar Circuit
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance
Volunteers
13
Ohmrsquos Law
Ohmrsquos Law is a set of mathematical formulas used in electronics to calculate an unknown amount of current voltage or resistance
bull Ohmrsquos Law helps to predict how ESUs will interact with tissue
bull The mathematical formula looks like this
(I) Current = (V) Voltage
(R) Resistance
or
V = I X R
German physicist - Georg Simon Ohm
1789 - 1854
Adding Power (W) to the Equation
Power is the amount of energy produced over time and is a result of Voltage x Current
W (Power) = (V) Voltage x (I) Current
Types of Electrosurgical Generators
bull The voltage remains constant to maintain consistent tissue effect regardless of changes in tissue resistance (muscle fatty tissue)
bull The power (watts) automatically adjusts in response to the tissue impedancecircuit variables
Constant Voltage
bull Watts (power) setting is chosen bull The Watts remain constant bull Voltage varies to maintain Watts bull All tissue is treated with same Wattage
Constant Power
Example of CP vs CV
17
Monopolar Circuit
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance
Ohmrsquos Law
Ohmrsquos Law is a set of mathematical formulas used in electronics to calculate an unknown amount of current voltage or resistance
bull Ohmrsquos Law helps to predict how ESUs will interact with tissue
bull The mathematical formula looks like this
(I) Current = (V) Voltage
(R) Resistance
or
V = I X R
German physicist - Georg Simon Ohm
1789 - 1854
Adding Power (W) to the Equation
Power is the amount of energy produced over time and is a result of Voltage x Current
W (Power) = (V) Voltage x (I) Current
Types of Electrosurgical Generators
bull The voltage remains constant to maintain consistent tissue effect regardless of changes in tissue resistance (muscle fatty tissue)
bull The power (watts) automatically adjusts in response to the tissue impedancecircuit variables
Constant Voltage
bull Watts (power) setting is chosen bull The Watts remain constant bull Voltage varies to maintain Watts bull All tissue is treated with same Wattage
Constant Power
Example of CP vs CV
17
Monopolar Circuit
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance
Adding Power (W) to the Equation
Power is the amount of energy produced over time and is a result of Voltage x Current
W (Power) = (V) Voltage x (I) Current
Types of Electrosurgical Generators
bull The voltage remains constant to maintain consistent tissue effect regardless of changes in tissue resistance (muscle fatty tissue)
bull The power (watts) automatically adjusts in response to the tissue impedancecircuit variables
Constant Voltage
bull Watts (power) setting is chosen bull The Watts remain constant bull Voltage varies to maintain Watts bull All tissue is treated with same Wattage
Constant Power
Example of CP vs CV
17
Monopolar Circuit
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance
Types of Electrosurgical Generators
bull The voltage remains constant to maintain consistent tissue effect regardless of changes in tissue resistance (muscle fatty tissue)
bull The power (watts) automatically adjusts in response to the tissue impedancecircuit variables
Constant Voltage
bull Watts (power) setting is chosen bull The Watts remain constant bull Voltage varies to maintain Watts bull All tissue is treated with same Wattage
Constant Power
Example of CP vs CV
17
Monopolar Circuit
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance
Example of CP vs CV
17
Monopolar Circuit
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance
Monopolar Circuit
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance
Bipolar Circuit
Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance

Basic Principles of
bull Always seeks ground
bull Always seeks the path of least resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance
Tissue Impedance
Tissue Impedance Varies with Water Content
Muscle Kidney Eye
Liver Oral Cavity
Gallbladder
Bowel Fat
Mesentary Brain
Scar Tissue Lung Adhesions
Least to Most Resistance

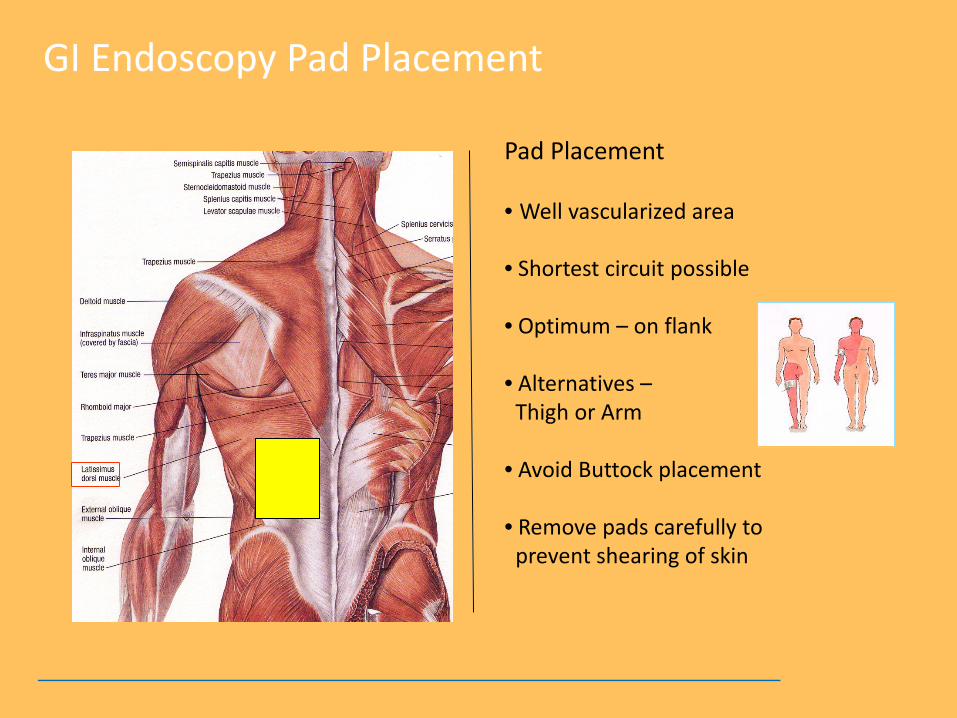
Pad Placement
bull Well vascularized area bull Shortest circuit possible bull Optimum ndash on flank bull Alternatives ndash Thigh or Arm bull Avoid Buttock placement bull Remove pads carefully to prevent shearing of skin
GI Endoscopy Pad Placement
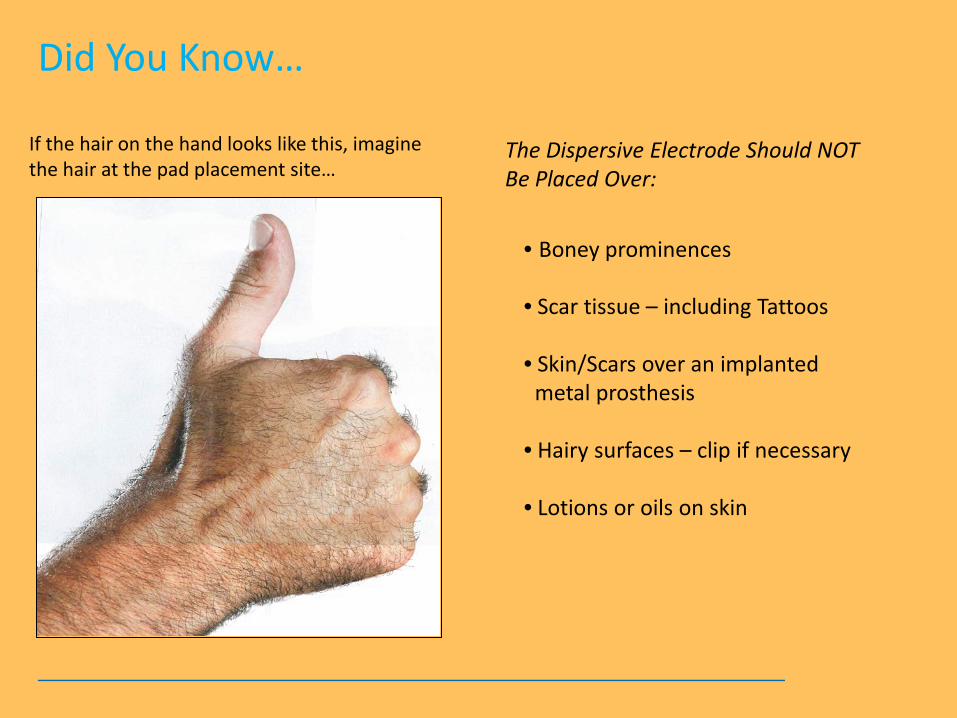
Did You Knowhellip
If the hair on the hand looks like this imagine the hair at the pad placement sitehellip
bull Boney prominences bull Scar tissue ndash including Tattoos bull SkinScars over an implanted metal prosthesis bull Hairy surfaces ndash clip if necessary bull Lotions or oils on skin
The Dispersive Electrode Should NOT Be Placed Over
24
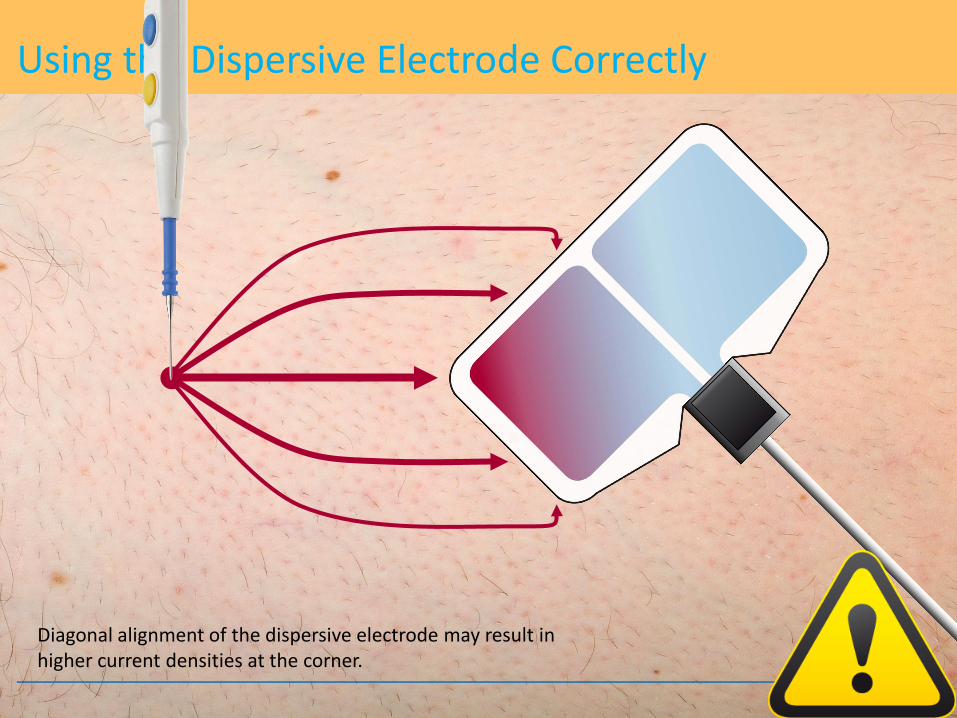
Using the Dispersive Electrode Correctly
Diagonal alignment of the dispersive electrode may result in higher current densities at the corner
25
Using the Dispersive Electrode Correctly
The long side of the dispersive electrode must face the operating field
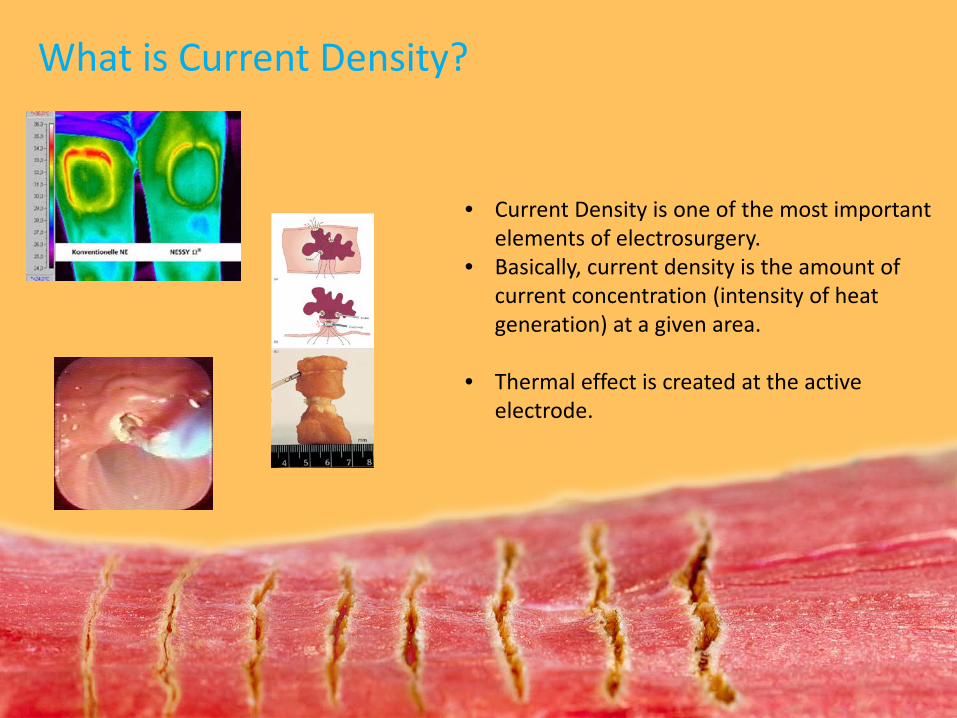
What is Current Density
bull Current Density is one of the most important elements of electrosurgery
bull Basically current density is the amount of current concentration (intensity of heat generation) at a given area
bull Thermal effect is created at the active electrode
Current Density
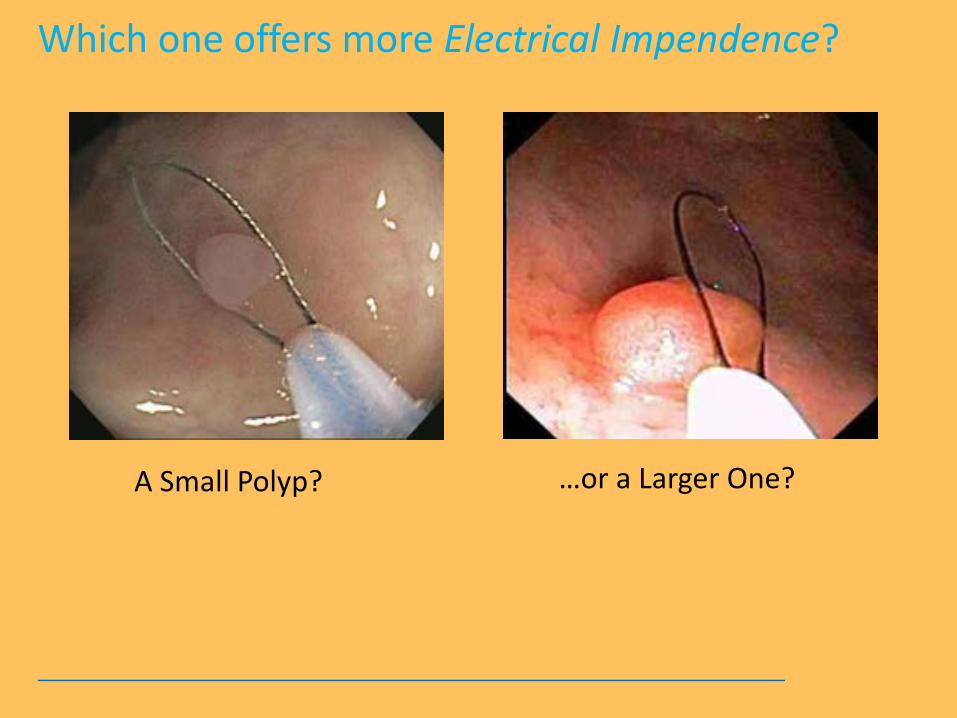
A Small Polyp hellipor a Larger One
Which one offers more Electrical Impendence
hellipall shapes and sizeshellipmany variables
Endoscopy Polypectomy Techniques
Cold Biopsy
Hot Biopsy
Cold Snare
Hot Snare
Saline Assisted Polypectomy
Piecemeal Resection
En bloc Resection
Variables Impacting Tissue Effect
Variables Impacting
Tissue Effect
Type of Generator Constant voltage vs
constant power
Type (size) of Electrode
Waveform Cut vs Coag
Physician technique
Pad placement
Patient variables age body type
hydration tissue IEDrsquos etc
Length of activation
Anatomical location
Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
| 5 | Muscle Kidney Eye | ||
| 10 | Liver Oral Cavity | ||
| 15 | Gallbladder | ||
| 20 | Bowel Brain Adipose | ||
| 25 | Mesentary | ||
| 30 | Scar Tissue Lung Adhesions |
| 5 | 10 | 15 | 20 | 25 | 30 |
Pad Placement
bull Well vascularized area bull Shortest circuit possible bull Optimum ndash on flank bull Alternatives ndash Thigh or Arm bull Avoid Buttock placement bull Remove pads carefully to prevent shearing of skin
GI Endoscopy Pad Placement
Did You Knowhellip
If the hair on the hand looks like this imagine the hair at the pad placement sitehellip
bull Boney prominences bull Scar tissue ndash including Tattoos bull SkinScars over an implanted metal prosthesis bull Hairy surfaces ndash clip if necessary bull Lotions or oils on skin
The Dispersive Electrode Should NOT Be Placed Over
24
Using the Dispersive Electrode Correctly
Diagonal alignment of the dispersive electrode may result in higher current densities at the corner
25
Using the Dispersive Electrode Correctly
The long side of the dispersive electrode must face the operating field
What is Current Density
bull Current Density is one of the most important elements of electrosurgery
bull Basically current density is the amount of current concentration (intensity of heat generation) at a given area
bull Thermal effect is created at the active electrode
Current Density
A Small Polyp hellipor a Larger One
Which one offers more Electrical Impendence
hellipall shapes and sizeshellipmany variables
Endoscopy Polypectomy Techniques
Cold Biopsy
Hot Biopsy
Cold Snare
Hot Snare
Saline Assisted Polypectomy
Piecemeal Resection
En bloc Resection
Variables Impacting Tissue Effect
Variables Impacting
Tissue Effect
Type of Generator Constant voltage vs
constant power
Type (size) of Electrode
Waveform Cut vs Coag
Physician technique
Pad placement
Patient variables age body type
hydration tissue IEDrsquos etc
Length of activation
Anatomical location
Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
| 5 | Muscle Kidney Eye | ||
| 10 | Liver Oral Cavity | ||
| 15 | Gallbladder | ||
| 20 | Bowel Brain Adipose | ||
| 25 | Mesentary | ||
| 30 | Scar Tissue Lung Adhesions |

Pad Placement
bull Well vascularized area bull Shortest circuit possible bull Optimum ndash on flank bull Alternatives ndash Thigh or Arm bull Avoid Buttock placement bull Remove pads carefully to prevent shearing of skin
GI Endoscopy Pad Placement
Did You Knowhellip
If the hair on the hand looks like this imagine the hair at the pad placement sitehellip
bull Boney prominences bull Scar tissue ndash including Tattoos bull SkinScars over an implanted metal prosthesis bull Hairy surfaces ndash clip if necessary bull Lotions or oils on skin
The Dispersive Electrode Should NOT Be Placed Over
24
Using the Dispersive Electrode Correctly
Diagonal alignment of the dispersive electrode may result in higher current densities at the corner
25
Using the Dispersive Electrode Correctly
The long side of the dispersive electrode must face the operating field
What is Current Density
bull Current Density is one of the most important elements of electrosurgery
bull Basically current density is the amount of current concentration (intensity of heat generation) at a given area
bull Thermal effect is created at the active electrode
Current Density
A Small Polyp hellipor a Larger One
Which one offers more Electrical Impendence
hellipall shapes and sizeshellipmany variables
Endoscopy Polypectomy Techniques
Cold Biopsy
Hot Biopsy
Cold Snare
Hot Snare
Saline Assisted Polypectomy
Piecemeal Resection
En bloc Resection
Variables Impacting Tissue Effect
Variables Impacting
Tissue Effect
Type of Generator Constant voltage vs
constant power
Type (size) of Electrode
Waveform Cut vs Coag
Physician technique
Pad placement
Patient variables age body type
hydration tissue IEDrsquos etc
Length of activation
Anatomical location
Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Pad Placement
bull Well vascularized area bull Shortest circuit possible bull Optimum ndash on flank bull Alternatives ndash Thigh or Arm bull Avoid Buttock placement bull Remove pads carefully to prevent shearing of skin
GI Endoscopy Pad Placement
Did You Knowhellip
If the hair on the hand looks like this imagine the hair at the pad placement sitehellip
bull Boney prominences bull Scar tissue ndash including Tattoos bull SkinScars over an implanted metal prosthesis bull Hairy surfaces ndash clip if necessary bull Lotions or oils on skin
The Dispersive Electrode Should NOT Be Placed Over
24
Using the Dispersive Electrode Correctly
Diagonal alignment of the dispersive electrode may result in higher current densities at the corner
25
Using the Dispersive Electrode Correctly
The long side of the dispersive electrode must face the operating field
What is Current Density
bull Current Density is one of the most important elements of electrosurgery
bull Basically current density is the amount of current concentration (intensity of heat generation) at a given area
bull Thermal effect is created at the active electrode
Current Density
A Small Polyp hellipor a Larger One
Which one offers more Electrical Impendence
hellipall shapes and sizeshellipmany variables
Endoscopy Polypectomy Techniques
Cold Biopsy
Hot Biopsy
Cold Snare
Hot Snare
Saline Assisted Polypectomy
Piecemeal Resection
En bloc Resection
Variables Impacting Tissue Effect
Variables Impacting
Tissue Effect
Type of Generator Constant voltage vs
constant power
Type (size) of Electrode
Waveform Cut vs Coag
Physician technique
Pad placement
Patient variables age body type
hydration tissue IEDrsquos etc
Length of activation
Anatomical location
Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
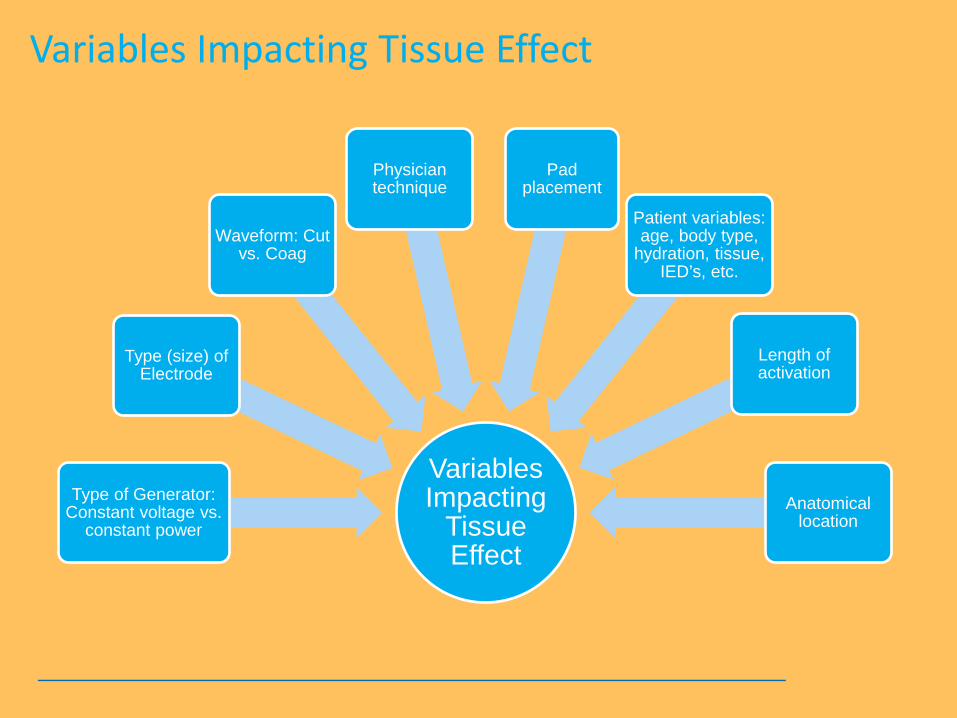
Pad Placement
bull Well vascularized area bull Shortest circuit possible bull Optimum ndash on flank bull Alternatives ndash Thigh or Arm bull Avoid Buttock placement bull Remove pads carefully to prevent shearing of skin
GI Endoscopy Pad Placement
Did You Knowhellip
If the hair on the hand looks like this imagine the hair at the pad placement sitehellip
bull Boney prominences bull Scar tissue ndash including Tattoos bull SkinScars over an implanted metal prosthesis bull Hairy surfaces ndash clip if necessary bull Lotions or oils on skin
The Dispersive Electrode Should NOT Be Placed Over
24
Using the Dispersive Electrode Correctly
Diagonal alignment of the dispersive electrode may result in higher current densities at the corner
25
Using the Dispersive Electrode Correctly
The long side of the dispersive electrode must face the operating field
What is Current Density
bull Current Density is one of the most important elements of electrosurgery
bull Basically current density is the amount of current concentration (intensity of heat generation) at a given area
bull Thermal effect is created at the active electrode
Current Density
A Small Polyp hellipor a Larger One
Which one offers more Electrical Impendence
hellipall shapes and sizeshellipmany variables
Endoscopy Polypectomy Techniques
Cold Biopsy
Hot Biopsy
Cold Snare
Hot Snare
Saline Assisted Polypectomy
Piecemeal Resection
En bloc Resection
Variables Impacting Tissue Effect
Variables Impacting
Tissue Effect
Type of Generator Constant voltage vs
constant power
Type (size) of Electrode
Waveform Cut vs Coag
Physician technique
Pad placement
Patient variables age body type
hydration tissue IEDrsquos etc
Length of activation
Anatomical location
Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Did You Knowhellip
If the hair on the hand looks like this imagine the hair at the pad placement sitehellip
bull Boney prominences bull Scar tissue ndash including Tattoos bull SkinScars over an implanted metal prosthesis bull Hairy surfaces ndash clip if necessary bull Lotions or oils on skin
The Dispersive Electrode Should NOT Be Placed Over
24
Using the Dispersive Electrode Correctly
Diagonal alignment of the dispersive electrode may result in higher current densities at the corner
25
Using the Dispersive Electrode Correctly
The long side of the dispersive electrode must face the operating field
What is Current Density
bull Current Density is one of the most important elements of electrosurgery
bull Basically current density is the amount of current concentration (intensity of heat generation) at a given area
bull Thermal effect is created at the active electrode
Current Density
A Small Polyp hellipor a Larger One
Which one offers more Electrical Impendence
hellipall shapes and sizeshellipmany variables
Endoscopy Polypectomy Techniques
Cold Biopsy
Hot Biopsy
Cold Snare
Hot Snare
Saline Assisted Polypectomy
Piecemeal Resection
En bloc Resection
Variables Impacting Tissue Effect
Variables Impacting
Tissue Effect
Type of Generator Constant voltage vs
constant power
Type (size) of Electrode
Waveform Cut vs Coag
Physician technique
Pad placement
Patient variables age body type
hydration tissue IEDrsquos etc
Length of activation
Anatomical location
Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

24
Using the Dispersive Electrode Correctly
Diagonal alignment of the dispersive electrode may result in higher current densities at the corner
25
Using the Dispersive Electrode Correctly
The long side of the dispersive electrode must face the operating field
What is Current Density
bull Current Density is one of the most important elements of electrosurgery
bull Basically current density is the amount of current concentration (intensity of heat generation) at a given area
bull Thermal effect is created at the active electrode
Current Density
A Small Polyp hellipor a Larger One
Which one offers more Electrical Impendence
hellipall shapes and sizeshellipmany variables
Endoscopy Polypectomy Techniques
Cold Biopsy
Hot Biopsy
Cold Snare
Hot Snare
Saline Assisted Polypectomy
Piecemeal Resection
En bloc Resection
Variables Impacting Tissue Effect
Variables Impacting
Tissue Effect
Type of Generator Constant voltage vs
constant power
Type (size) of Electrode
Waveform Cut vs Coag
Physician technique
Pad placement
Patient variables age body type
hydration tissue IEDrsquos etc
Length of activation
Anatomical location
Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

25
Using the Dispersive Electrode Correctly
The long side of the dispersive electrode must face the operating field
What is Current Density
bull Current Density is one of the most important elements of electrosurgery
bull Basically current density is the amount of current concentration (intensity of heat generation) at a given area
bull Thermal effect is created at the active electrode
Current Density
A Small Polyp hellipor a Larger One
Which one offers more Electrical Impendence
hellipall shapes and sizeshellipmany variables
Endoscopy Polypectomy Techniques
Cold Biopsy
Hot Biopsy
Cold Snare
Hot Snare
Saline Assisted Polypectomy
Piecemeal Resection
En bloc Resection
Variables Impacting Tissue Effect
Variables Impacting
Tissue Effect
Type of Generator Constant voltage vs
constant power
Type (size) of Electrode
Waveform Cut vs Coag
Physician technique
Pad placement
Patient variables age body type
hydration tissue IEDrsquos etc
Length of activation
Anatomical location
Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
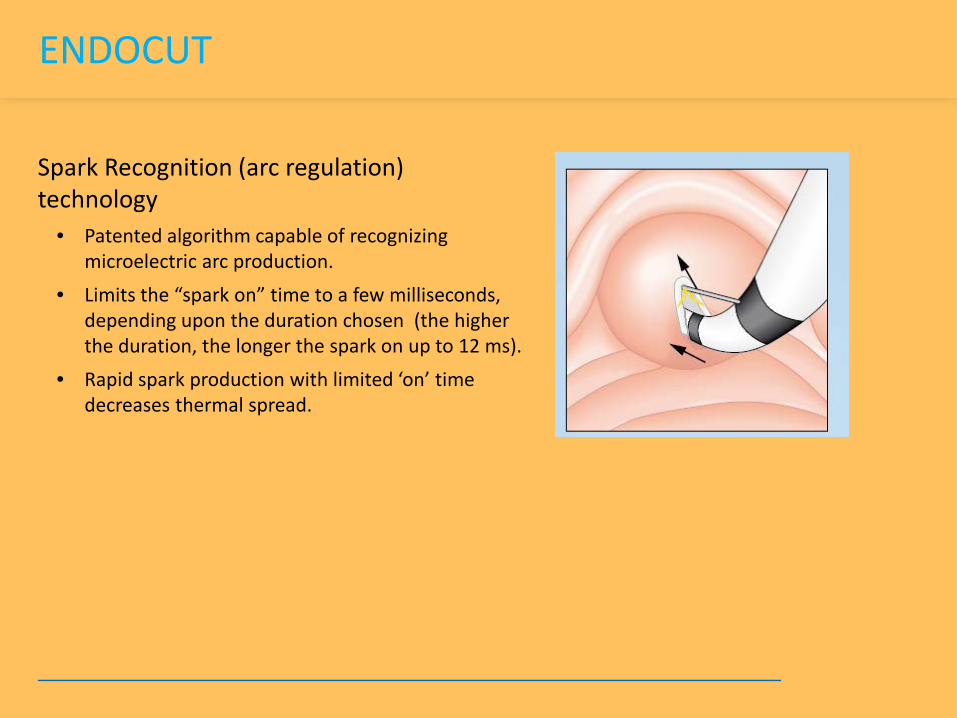
What is Current Density
bull Current Density is one of the most important elements of electrosurgery
bull Basically current density is the amount of current concentration (intensity of heat generation) at a given area
bull Thermal effect is created at the active electrode
Current Density
A Small Polyp hellipor a Larger One
Which one offers more Electrical Impendence
hellipall shapes and sizeshellipmany variables
Endoscopy Polypectomy Techniques
Cold Biopsy
Hot Biopsy
Cold Snare
Hot Snare
Saline Assisted Polypectomy
Piecemeal Resection
En bloc Resection
Variables Impacting Tissue Effect
Variables Impacting
Tissue Effect
Type of Generator Constant voltage vs
constant power
Type (size) of Electrode
Waveform Cut vs Coag
Physician technique
Pad placement
Patient variables age body type
hydration tissue IEDrsquos etc
Length of activation
Anatomical location
Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Current Density
A Small Polyp hellipor a Larger One
Which one offers more Electrical Impendence
hellipall shapes and sizeshellipmany variables
Endoscopy Polypectomy Techniques
Cold Biopsy
Hot Biopsy
Cold Snare
Hot Snare
Saline Assisted Polypectomy
Piecemeal Resection
En bloc Resection
Variables Impacting Tissue Effect
Variables Impacting
Tissue Effect
Type of Generator Constant voltage vs
constant power
Type (size) of Electrode
Waveform Cut vs Coag
Physician technique
Pad placement
Patient variables age body type
hydration tissue IEDrsquos etc
Length of activation
Anatomical location
Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
A Small Polyp hellipor a Larger One
Which one offers more Electrical Impendence
hellipall shapes and sizeshellipmany variables
Endoscopy Polypectomy Techniques
Cold Biopsy
Hot Biopsy
Cold Snare
Hot Snare
Saline Assisted Polypectomy
Piecemeal Resection
En bloc Resection
Variables Impacting Tissue Effect
Variables Impacting
Tissue Effect
Type of Generator Constant voltage vs
constant power
Type (size) of Electrode
Waveform Cut vs Coag
Physician technique
Pad placement
Patient variables age body type
hydration tissue IEDrsquos etc
Length of activation
Anatomical location
Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
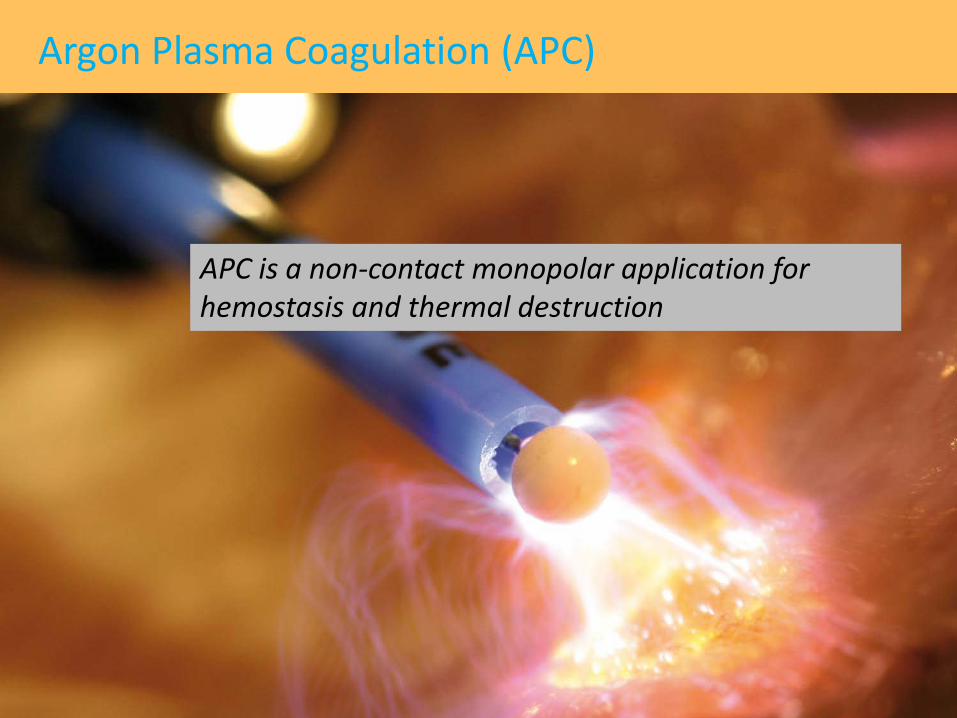
hellipall shapes and sizeshellipmany variables
Endoscopy Polypectomy Techniques
Cold Biopsy
Hot Biopsy
Cold Snare
Hot Snare
Saline Assisted Polypectomy
Piecemeal Resection
En bloc Resection
Variables Impacting Tissue Effect
Variables Impacting
Tissue Effect
Type of Generator Constant voltage vs
constant power
Type (size) of Electrode
Waveform Cut vs Coag
Physician technique
Pad placement
Patient variables age body type
hydration tissue IEDrsquos etc
Length of activation
Anatomical location
Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
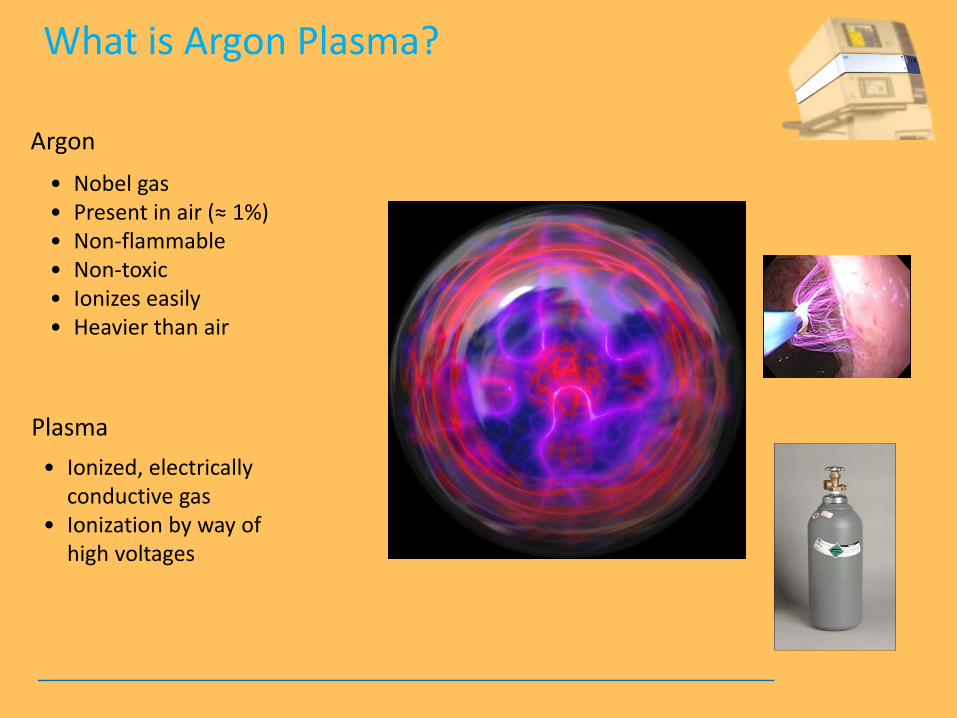
Endoscopy Polypectomy Techniques
Cold Biopsy
Hot Biopsy
Cold Snare
Hot Snare
Saline Assisted Polypectomy
Piecemeal Resection
En bloc Resection
Variables Impacting Tissue Effect
Variables Impacting
Tissue Effect
Type of Generator Constant voltage vs
constant power
Type (size) of Electrode
Waveform Cut vs Coag
Physician technique
Pad placement
Patient variables age body type
hydration tissue IEDrsquos etc
Length of activation
Anatomical location
Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Variables Impacting Tissue Effect
Variables Impacting
Tissue Effect
Type of Generator Constant voltage vs
constant power
Type (size) of Electrode
Waveform Cut vs Coag
Physician technique
Pad placement
Patient variables age body type
hydration tissue IEDrsquos etc
Length of activation
Anatomical location
Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Electrosurgical Thermal Effects on Cells
Temperature Tissue Effect
104degF Reversible cellular trauma
120degF Irreversible cellular trauma
158degF Coagulation (Desiccation)
212degF Cutting
392degF Carbonization
33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

33
Cutting bull Voltage quickly raises cell water temperature to the boiling
point bull Cell water turns to steam bull Cell explodes separating from adjoining cells bull Cleavage plane is created = clinical ldquoCUTrdquo Note For cutting to occur a minimum of 200 Vp is required to get a spark
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
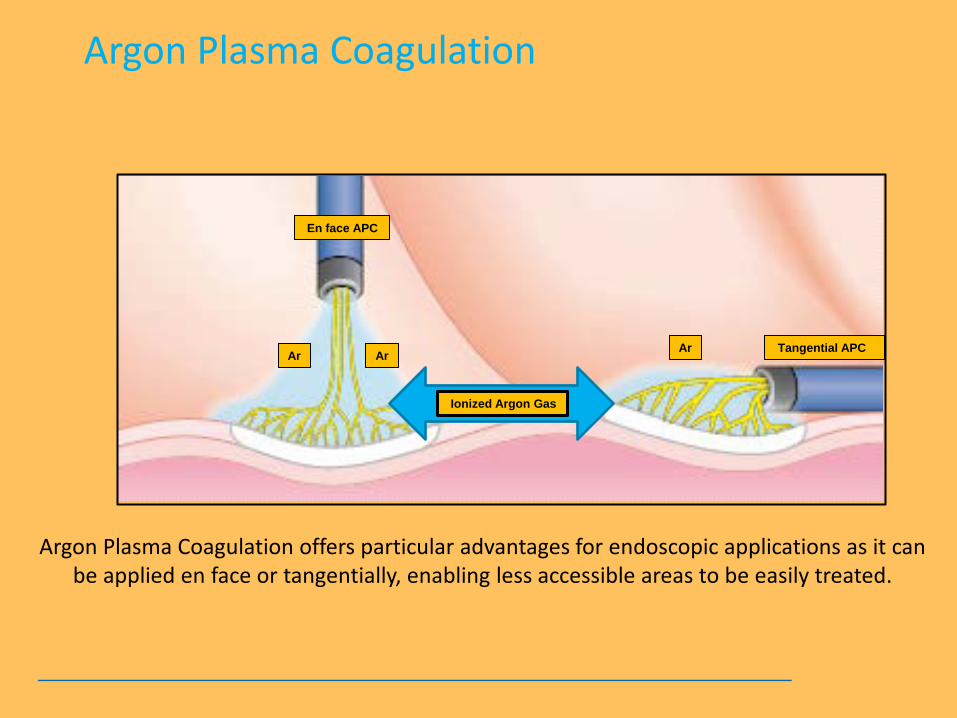
ENDO CUT
bull ENDO CUT is a specialized waveform which involves a fractionated cutting mode with patented spark recognition technology characterized by alternating cutting and coagulation cycles
bull Constant VoltagePower Dosing Technology
bull Yellow Pedal
Akiho H et al Safety Advantage of Endocut Mode over Endoscopic Sphincterotomy for Choledocholelithasis World Journal Gastroenterolgy 2006122086-8
Monkemuller K et al State of the Art Clinical Gastroenterology and Hepatology 20097641-652
Frye L et al Quality of Polyps Resected by Snare Polypectomy Does the Type of Electrosurgical Current Used Matter American Journal of Gastroenterology 20061012123-27
Perini R et al Post sphincterotomy bleeding after microprocessor controlled electrosurgery Gastrointestinal Endoscopy 20056153-7
Hopper A et al Giant laterally spreading tumors of the papilla endoscopic features resection technique and outcome Gastrointest Endosc 201071967-75 Fanning S et al Giant laterally spreading tumors of the duodenum endoscopic resection outcomes limitations and caveats Gastrointest Endosc 201275805-12)
Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Spark Recognition (arc regulation) technology
bull Patented algorithm capable of recognizing microelectric arc production
bull Limits the ldquospark onrdquo time to a few milliseconds depending upon the duration chosen (the higher the duration the longer the spark on up to 12 ms)
bull Rapid spark production with limited lsquoonrsquo time decreases thermal spread
ENDOCUT
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
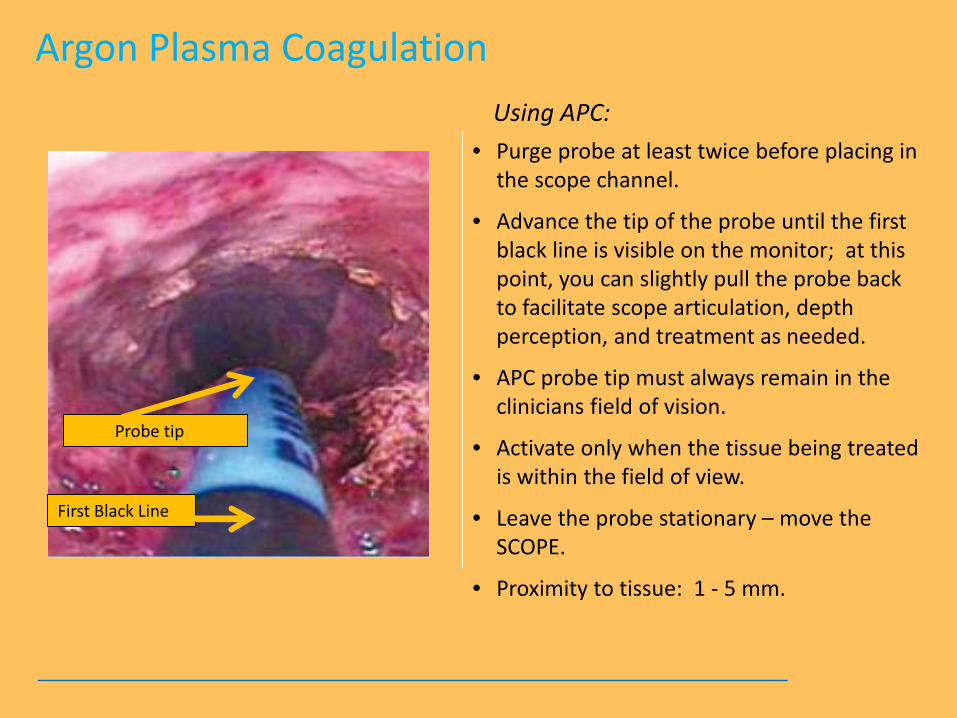
36
Coagulation Hemostasis due to shrinking tissue
bull Waveform with spikes of high voltage followed by rest periods
bull This allows the cellular proteins to slowly denature (dehydrate)
bull Coagulation occurs
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
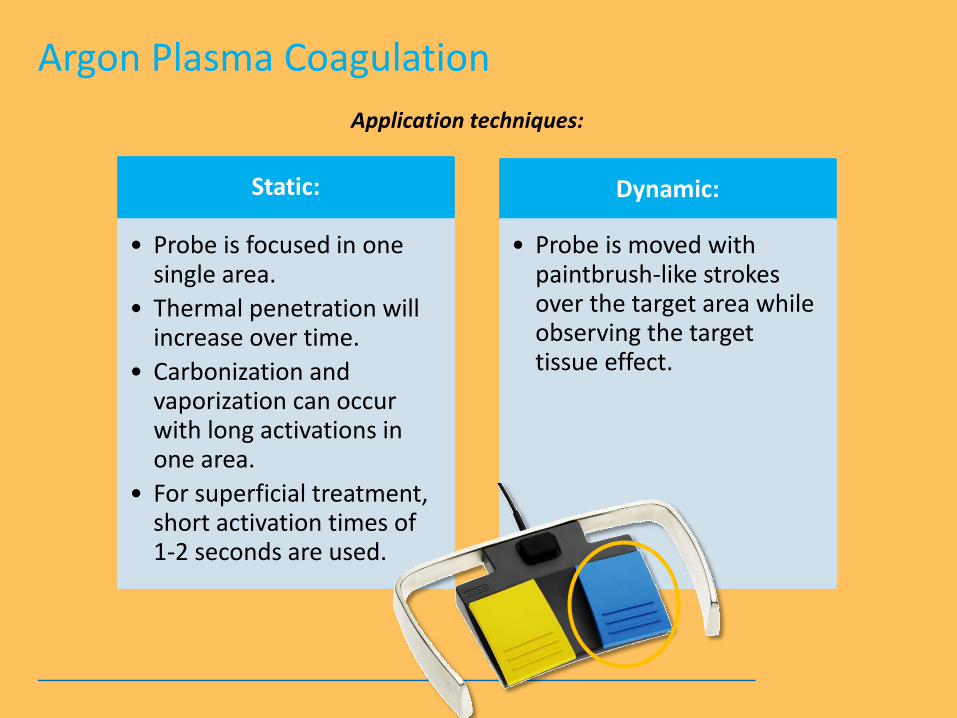
Yellow + Blue IS NOT Green in electrosurgeryhellip
bull COAGULATION (Blue) is completely independent of CUT (Yellow)
bull BLEND-CUT or ENDO CUT is a CUT feature (Always Yellow)
bull Settings on one side do not effect the other
Like a set of rail tracks running into infinityhellip they never meet
Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Argon Plasma Coagulation (APC)
38
APC is a non-contact monopolar application for hemostasis and thermal destruction
bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

bull Nobel gas bull Present in air (asymp 1) bull Non-flammable bull Non-toxic bull Ionizes easily bull Heavier than air
Argon
What is Argon Plasma
bull Ionized electrically conductive gas
bull Ionization by way of high voltages
Plasma
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
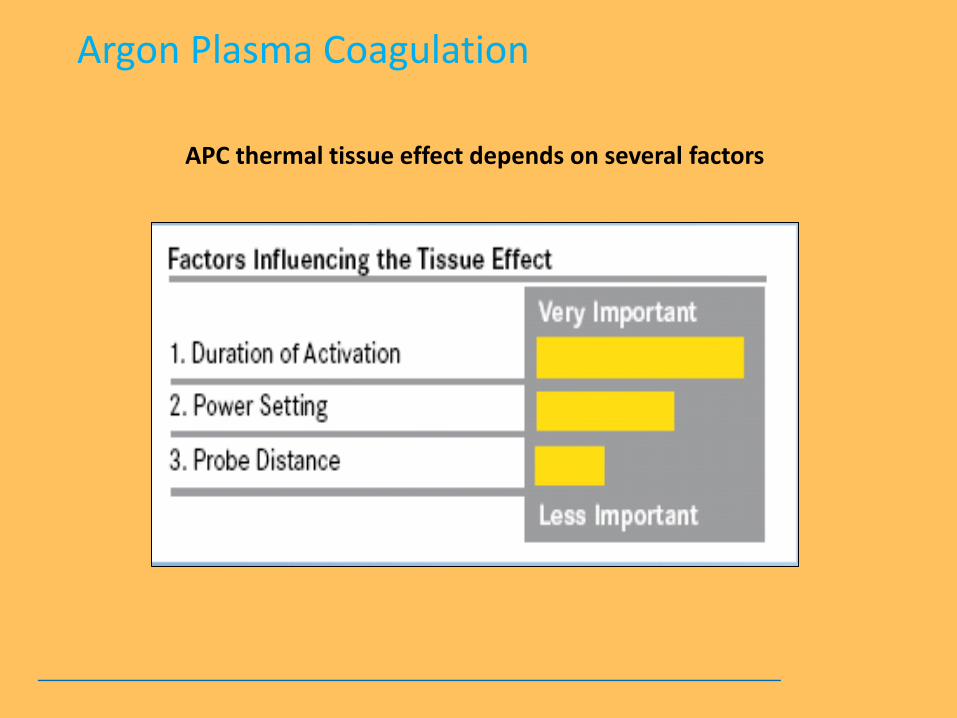
Argon-one of the Nobel gases
40
IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

IF A QUEEN PASSES GAS IS IT CONSIDERED A NOBEL GAS
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
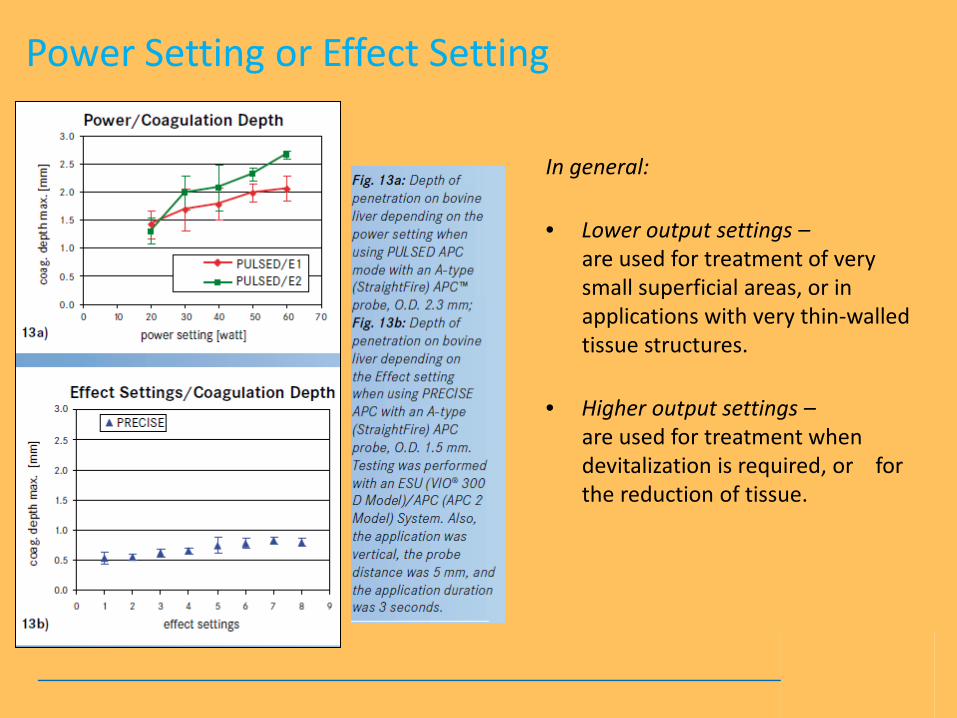
The voltage required for ionization of gas is asymp 4000
volts
Argon gas Argon plasma with arc beam
APC is a monopolar application in which HF electrical energy is transferred to the target tissue using ionized (conductive) argon gas (plasma) without the
electrode coming in contact with the target tissue
Argon Plasma Coagulation - APC
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
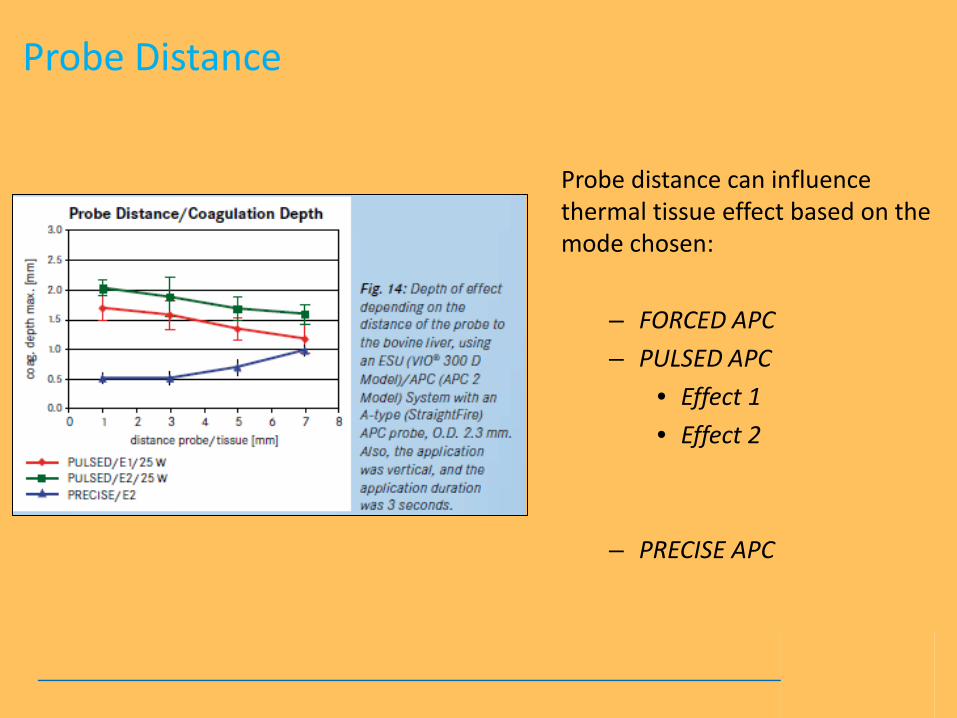
Argon Plasma Coagulation offers particular advantages for endoscopic applications as it can be applied en face or tangentially enabling less accessible areas to be easily treated
En face APC
Tangential APC
Argon Plasma Coagulation
Ar
Ionized Argon Gas
Ar Ar
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
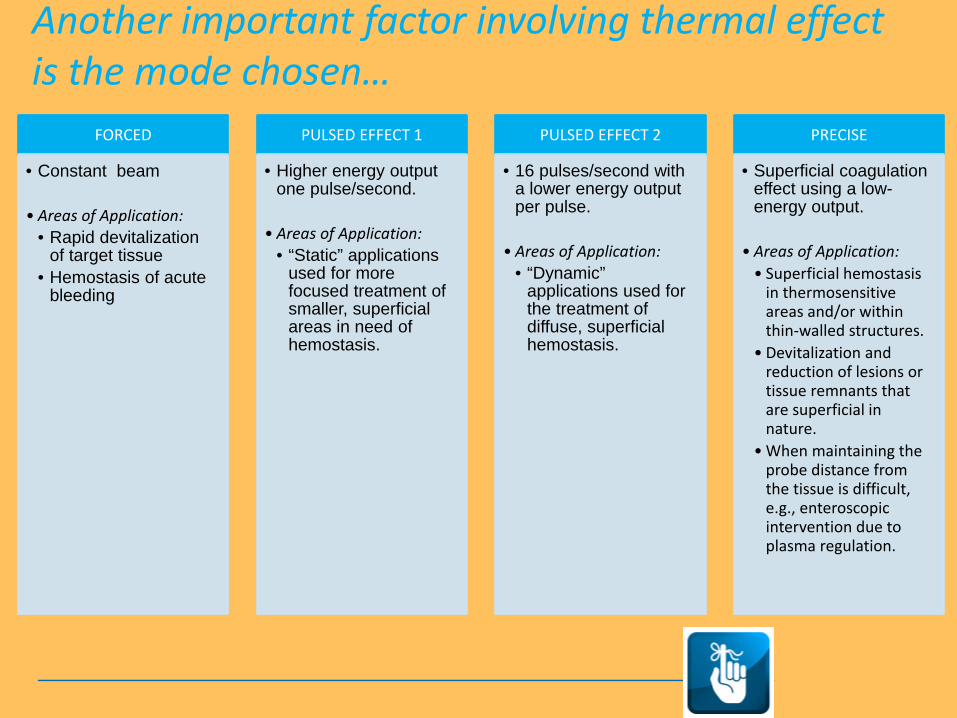
APC Advantages
Argon Plasma Coagulation
bull Non-contact application
bull Smoke is reduced bull Thinner more flexible eschar
bull Widespread areas can be treated
bull Applications can be ndash
bull Axial bull Radial bull Retroflexed bull Circumferential
Non-contact No sticking to delicate tissue
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
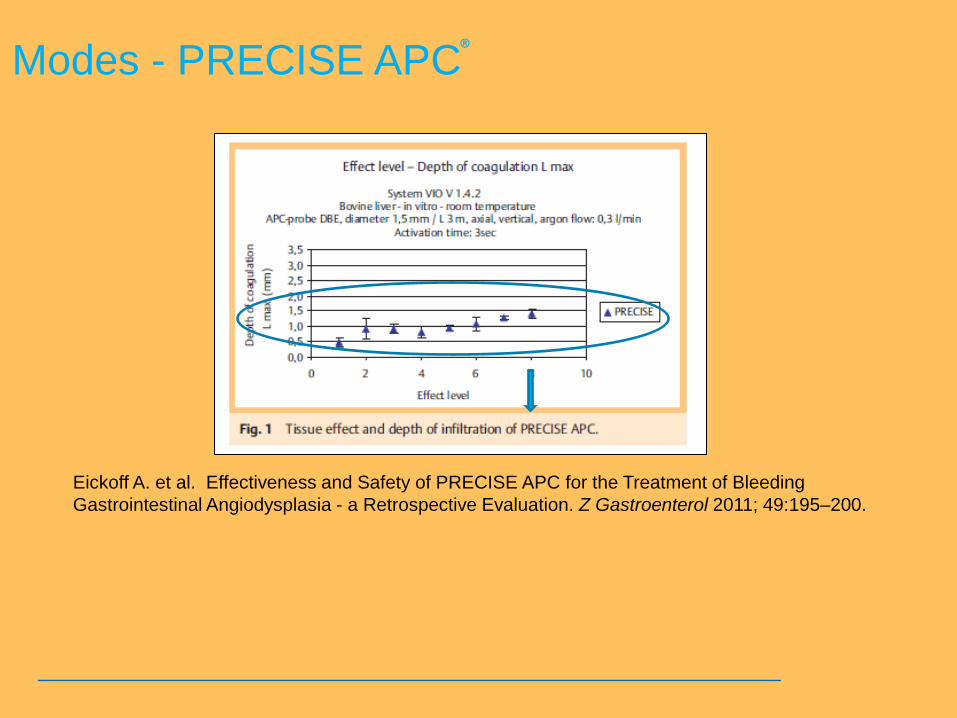
bull Purge probe at least twice before placing in the scope channel
bull Advance the tip of the probe until the first black line is visible on the monitor at this point you can slightly pull the probe back to facilitate scope articulation depth perception and treatment as needed
bull APC probe tip must always remain in the clinicians field of vision
bull Activate only when the tissue being treated is within the field of view
bull Leave the probe stationary ndash move the SCOPE
bull Proximity to tissue 1 - 5 mm
Argon Plasma Coagulation Using APC
Probe tip
First Black Line
Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Argon Plasma Coagulation Application techniques
Static
bull Probe is focused in one single area
bull Thermal penetration will increase over time
bull Carbonization and vaporization can occur with long activations in one area
bull For superficial treatment short activation times of 1-2 seconds are used
Dynamic
bull Probe is moved with paintbrush-like strokes over the target area while observing the target tissue effect
Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Proper Technique
Clinical Video
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
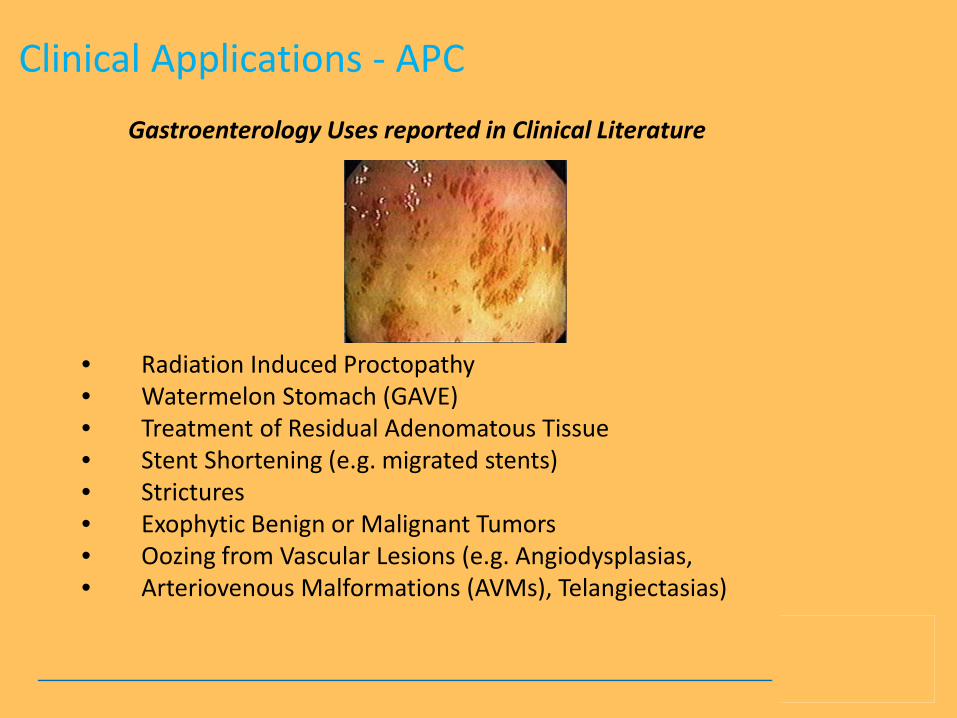
ERBEVIOTOMMYGUNGAVEmpg
48
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
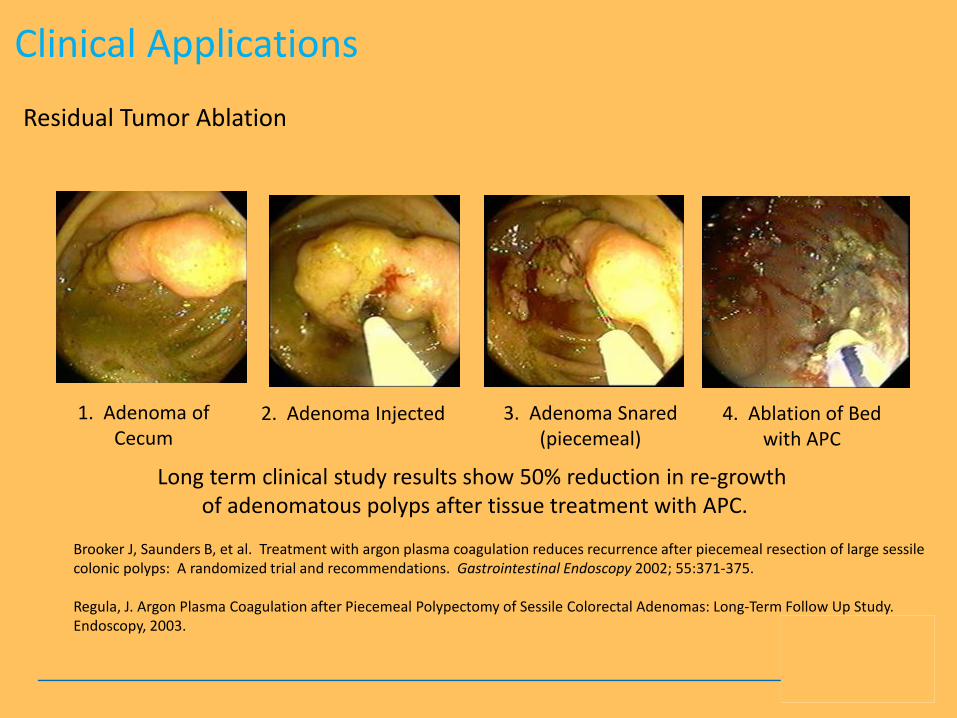
Argon Plasma Coagulation
APC thermal tissue effect depends on several factors
Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Duration of Activation
bull When the application time over the same area is increased the depth of the tissue being affected will increase
bull The physician should treat with an activation time to correspond with the desired thermal effect and anatomical location
Fig 12 Depth effect depending on the duration of activation with the APC modes in a bovine liver Testing was performed with an ESU (VIOreg 300 D Model)APC (APCtrade 2 Model) System along with an A-type (Straight Fire) APC probe OD 23 mm Also the application was vertical and the probe distance was 5 mm
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
Power Setting or Effect Setting
In general bull Lower output settings ndash
are used for treatment of very small superficial areas or in applications with very thin-walled tissue structures
bull Higher output settings ndash
are used for treatment when devitalization is required or for the reduction of tissue
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
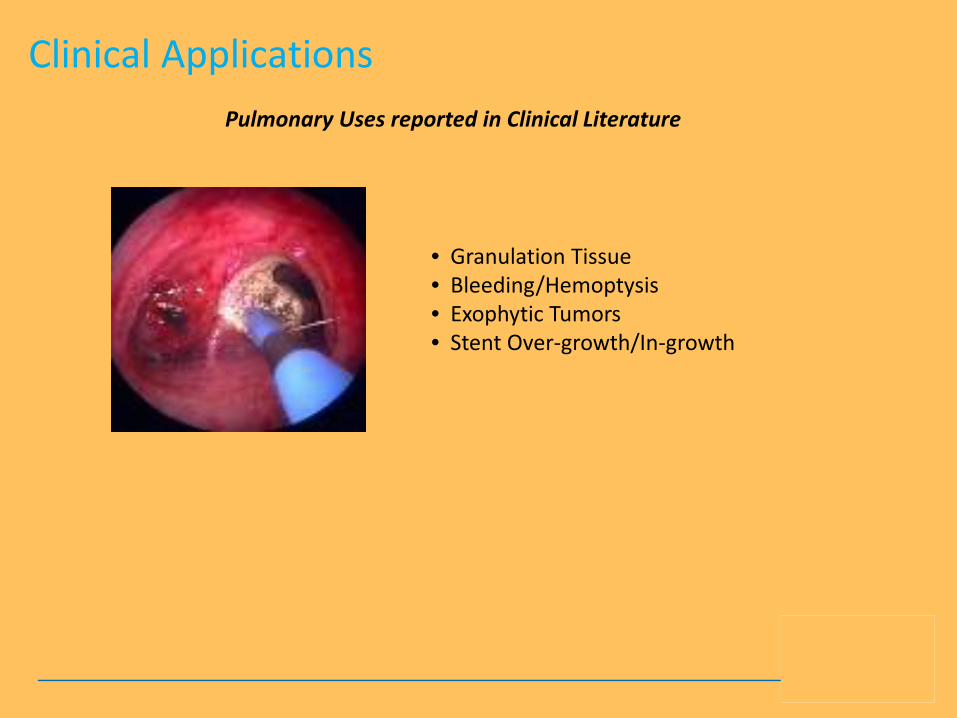
Probe Distance
Probe distance can influence thermal tissue effect based on the mode chosen
ndash FORCED APC ndash PULSED APC
bull Effect 1 bull Effect 2
ndash PRECISE APC
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
Another important factor involving thermal effect is the mode chosenhellip
FORCED
bull Constant beam
bull Areas of Application bull Rapid devitalization
of target tissue bull Hemostasis of acute
bleeding
PULSED EFFECT 1
bull Higher energy output one pulsesecond
bull Areas of Application bull ldquoStaticrdquo applications
used for more focused treatment of smaller superficial areas in need of hemostasis
PULSED EFFECT 2
bull 16 pulsessecond with a lower energy output per pulse
bull Areas of Application bull ldquoDynamicrdquo
applications used for the treatment of diffuse superficial hemostasis
PRECISE
bull Superficial coagulation effect using a low-energy output
bull Areas of Application bull Superficial hemostasis
in thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull When maintaining the probe distance from the tissue is difficult eg enteroscopic intervention due to plasma regulation
Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Modes - PRECISE APC
Eickoff A et al Effectiveness and Safety of PRECISE APC for the Treatment of Bleeding Gastrointestinal Angiodysplasia - a Retrospective Evaluation Z Gastroenterol 2011 49195ndash200
reg
Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Modes - PRECISE APC
Areas of Application
bull Superficial hemostasis
bull Thermosensitive areas andor within thin-walled structures
bull Devitalization and reduction of lesions or tissue remnants that are superficial in nature
bull In situations where maintaining the probe distance from the tissue is difficult eg enteroscopic intervention
Angiodysplasia
PRECISE APC Effect 5
reg
Clinical Video
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
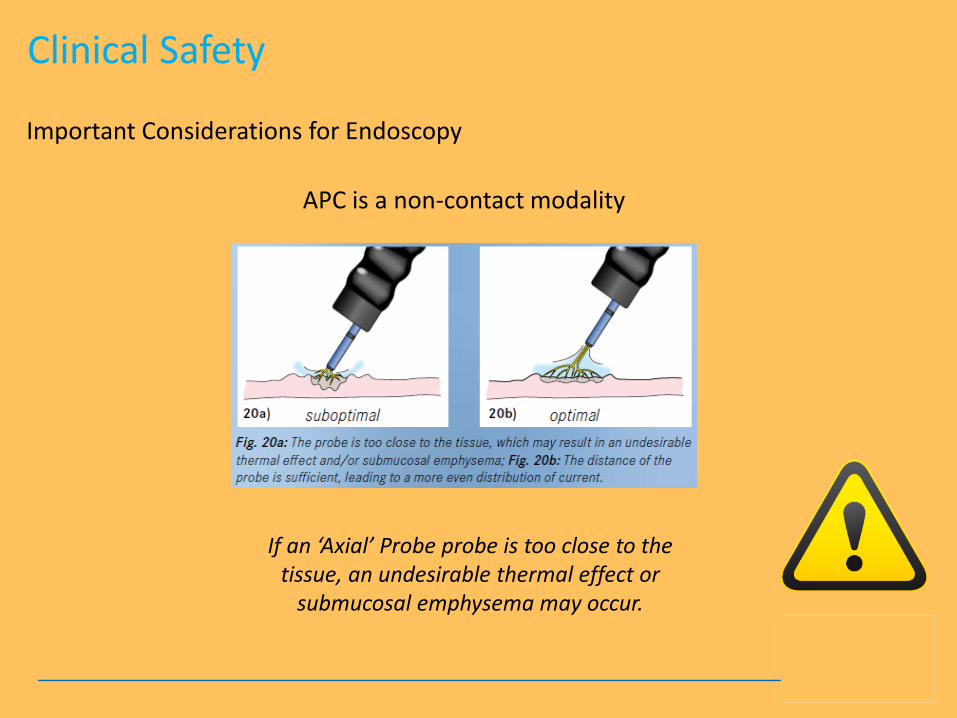
There are differences bull Diameter bull Length bull Shape of the probersquos outlet
bull Axial direction bull Side fire bull Circumferential
Black rings bull 1cm apart (10mm)
APC Probes
1cm
Connector
Marking rings
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
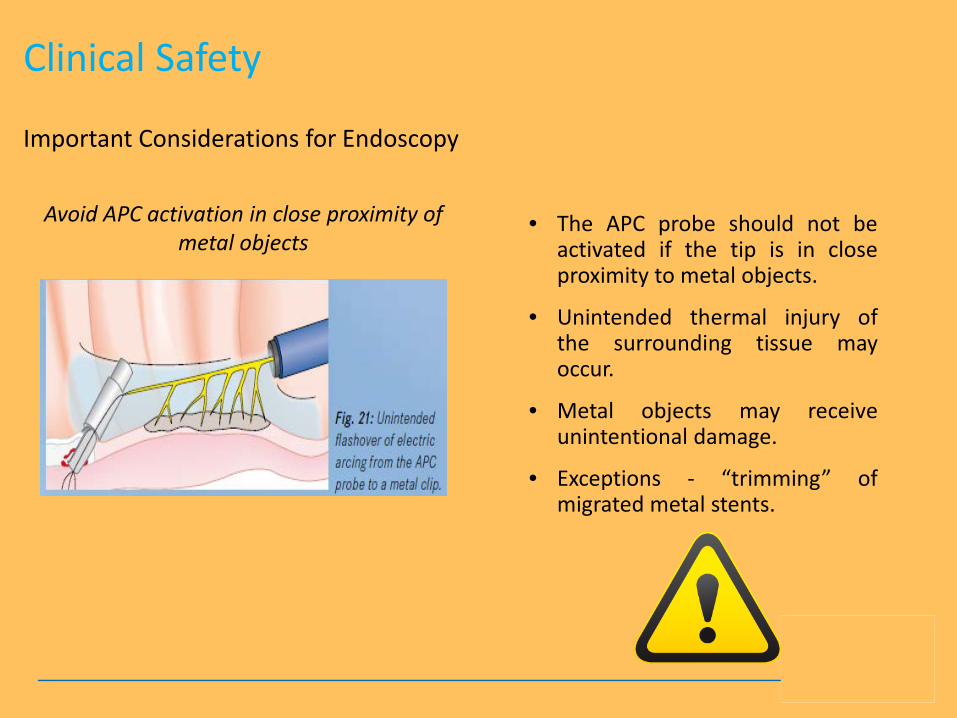
Clinical Applications - APC
bull Radiation Induced Proctopathy bull Watermelon Stomach (GAVE) bull Treatment of Residual Adenomatous Tissue bull Stent Shortening (eg migrated stents) bull Strictures bull Exophytic Benign or Malignant Tumors bull Oozing from Vascular Lesions (eg Angiodysplasias bull Arteriovenous Malformations (AVMs) Telangiectasias)
Gastroenterology Uses reported in Clinical Literature
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
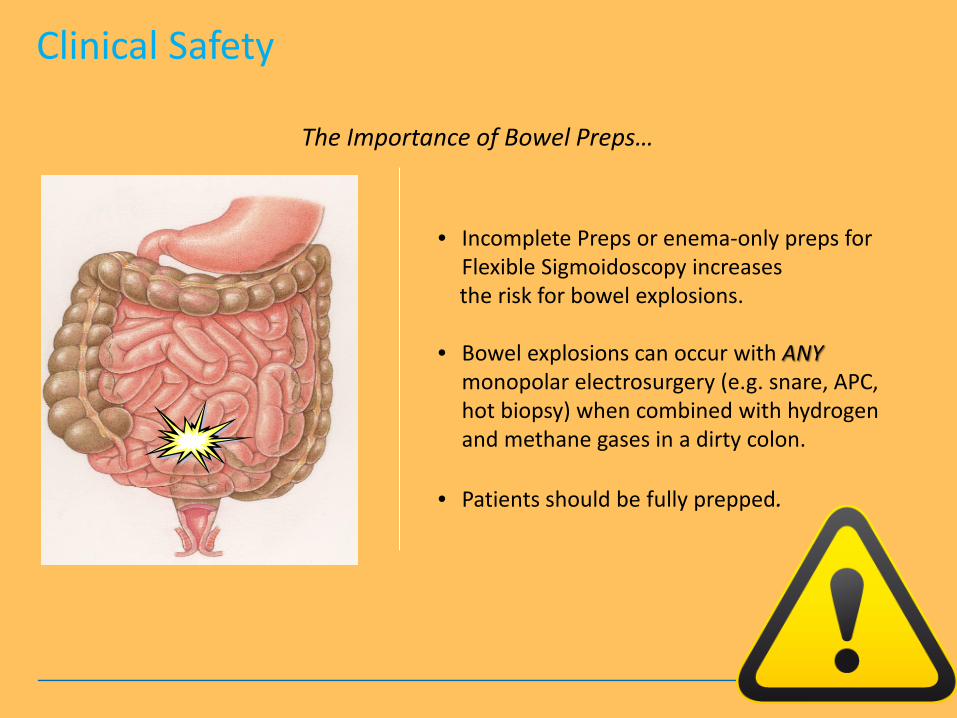
Clinical Applications
1 Adenoma of Cecum
3 Adenoma Snared (piecemeal)
2 Adenoma Injected 4 Ablation of Bed with APC
Long term clinical study results show 50 reduction in re-growth of adenomatous polyps after tissue treatment with APC
Brooker J Saunders B et al Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps A randomized trial and recommendations Gastrointestinal Endoscopy 2002 55371-375 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow Up Study Endoscopy 2003
Residual Tumor Ablation
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
References 1 ldquoThe role of endoscopy in ampullary and duodenal adenomasrdquo Gastrointestinal Endoscopy 2006 Vol 64 No 6 2 Brooker J Treatment with APC reduces recurrence after piecemeal resection of large sessile colonic polyps a randomized trial and
recommendations Gastrointestinal Endoscopy 2002 3 Buyukberber Mehmet APC in the treatment of hemorrhagic radiation proctitis Turk J Gastroenterol 2005 4 Dulai Gareth Treatment of Water Melon Stomach Current Treatment Options in Gastroenterology 2006 5 Eickhoff A et al Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction effectiveness of the new
pulsed APC versus forced APC Endoscopy 2007 39 637-642 Ferreira L et al Post-Sphincterotomy Bleeding Who What When and How American Journal of Gastroenterology 2007
6 Eickhoff A et al Pain sensation and neuromuscular stimulation during argon plasma coagulation in gastrointestinal endoscopy Surg Endosc 2007
7 Fujishiro M Safety of Argon Plasma Coagulation for Hemostasis During Endoscopic Mucosal Resection Surg Laparosc Endosc Percutan Tech 2006
8 Fukami N Endoscopic treatment of large sessile and flat colorectal lesions Current Opinions in Gastroenterology 20062254-59 9 Fukatsu H et al Evaluation of needle-knife precut papillotomy after unsuccessful biliary cannulation especially with regard to postoperative
anatomic factors Surg Endosc 200822717-23 10 Garcia A et al Safety and efficacy of argon plasma coagulator ablation therapy for flat colorectal adenomas Rev Esp Enferm Dig 200496315-
321 11 Herrera S et al The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in
patients admitted for GI hemorrhage Gastrointestinal Endoscopy 2008 12 Horiuchi A et al Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla Clin
Gastroenterol Hepatol 200751113-8 13 Ifadhli A et al Efficacy of argon plasma coagulation compared with topical formalin application for chronic radiation proctopathy Can J
Gastroenterol 200822129-132 14 Kitamura Tadashi Argon plasma coagulation for early gastric cancer technique and outcome Gastrointestinal Endoscopy 2006 15 Kwan V APC in the Management of Symptomatic GI Vascular Lesions American Journal of Gastroenterology 2006 16 Lecleire S et al Bleeding gastric vascular ectasia treated by argon plasma coagulation a comparison between patients with and without
cirrhosis Gastrointestinal Endoscopy 200867
Gastroenterology Uses found in Clinical Literature
Clinical Applications - APC
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
References 17 Manner H et al Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract
Digestive and Liver Disease 2006 18 Norton I et al A Randomized Trial of Endoscopic Biliary Sphincterotomy Using Pure-Cut Versus Combined Cut and Coagulation Waveforms
Clinical Gastroenterology and Hepatology 2005 31029-1033 19 Norton I et al Efficacy of colonic submucosal saline solution injection for the reduction of iatrogenic thermal injury Gastrointestinal Endoscopy
2002Vol 56 No 1 20 Olmos Jorge APC for prevention of recurrent bleeding from GI angiodysplasias Gastrointestinal Endoscopy 2004 21 Ortner M et al Endoscopic Interventions for Preneoplastic and Neoplastic Lesions Mucosectomy Argon Plasma Coagulation and Photodynamic
Therapy Digestive Diseases 200220 167-172 22 Perini Rafael Post-sphincterotomy bleeding after microprocessor-controlled electrosurgery Gastrointestinal Endoscopy 2005 23 Regula J Argon Plasma Coagulation after Piecemeal Polypectomy of Sessile Colorectal Adenomas Long-Term Follow-Up Study Endoscopy 2003 24 Repici A Endoscopic polypectomy techniques complications and follow-up Tech Coloproctol 2004 8 S283-S290 25 Rerknimitr R Trimming a Metallic Biliary Stent Using an Argon Plasma Coagulator Cardio Vascular and Interventional Radiology 2006 26 Ross A Flat and Depressed Neoplasms of the Colon in the Western World American Journal of Gastroenterology 2006 27 Schubert D Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with
diathermy Surg Endosc 2003171579-1582 28 Soctikno R et al Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults JAMA 2008
Vol 299 No 9 29 Vargo John Clinical Applications of APC Gastrointestinal Endoscopy 2004 30 Zlatanic J et al Large sessile colonic adenomas use of argon plasma coagulator to supplement piecemeal snare polypectomy Gastrointestinal
Endoscopy 1999 Vol 49 No 6
Clinical Applications - APC Gastroenterology Uses found in Clinical Literature
Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Clinical Applications Pulmonary Uses reported in Clinical Literature
bull Granulation Tissue bull BleedingHemoptysis bull Exophytic Tumors bull Stent Over-growthIn-growth
Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Clinical Applications - APC
Pulmonary Uses found in Clinical Literature References
1 Bergler Wolfgang Treatment of recurrent respiratory papillomatosis with argon Plasma coagulation Journal of Laryngology and Otology 1997
2 Bolligner CT et al Therapeutic bronchoscopy with immediate effect laser electrocautery argon plasma coagulation and stents European Respirartory Journal 2006 271258-1271
3 Capaccio P et al Flexible Argon Coagulation Treatment of Obstructive Tracheal Metastatic Melanoma American Journal of Otolarynogology 2002 Vol 23 No 4
4 Crosta C et al Endoscopic argon plasma for palliative treatment of malignant airway obstructions early results in 47 cases Lung Cancer 2001 33 75-80
5 Lee P et al Advances in Bronchoscopy-Therapeutic Bronchoscopy JAPI 2004 Vol 52 6 Morice Roldofo Endobronchial Argon Plasma Coagulation for Treatment of Hemoptysis and Neoplastic Airway
Obstruction Chest 2001 7 Orino K et al Bronchoscopic Treatment with Argon Plasma Coagulation for Recurrent Typical Carcinoids Report of a
Case Anticancer Research 2004 244073-4078 8 Sheski F Endobronchial Electrosurgery Seminars in Respiratory and Critical Care Medicine 2004 Vol 25 No 4 9 Sohrab S Management of Central Airway Obstruction Clinical Lung Cancer 2007 10 Sutedja G Endobronchial Electrocautery and Argon Plasma Coagulation Prog Respir 2000 Vol 30 11 Tremblay A Endobronchial electrocautery and Argon Plasma Coagulation A Practical Approach Can Respir 2004
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
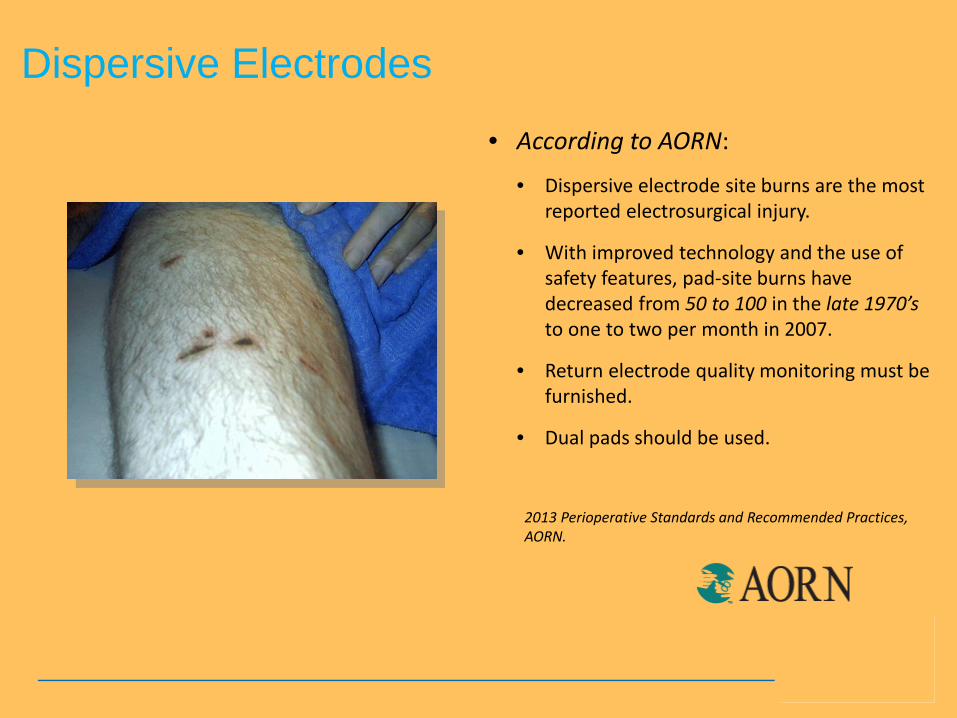
63
Clinical Safety Considerationshellip
hellipletrsquos discuss further
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
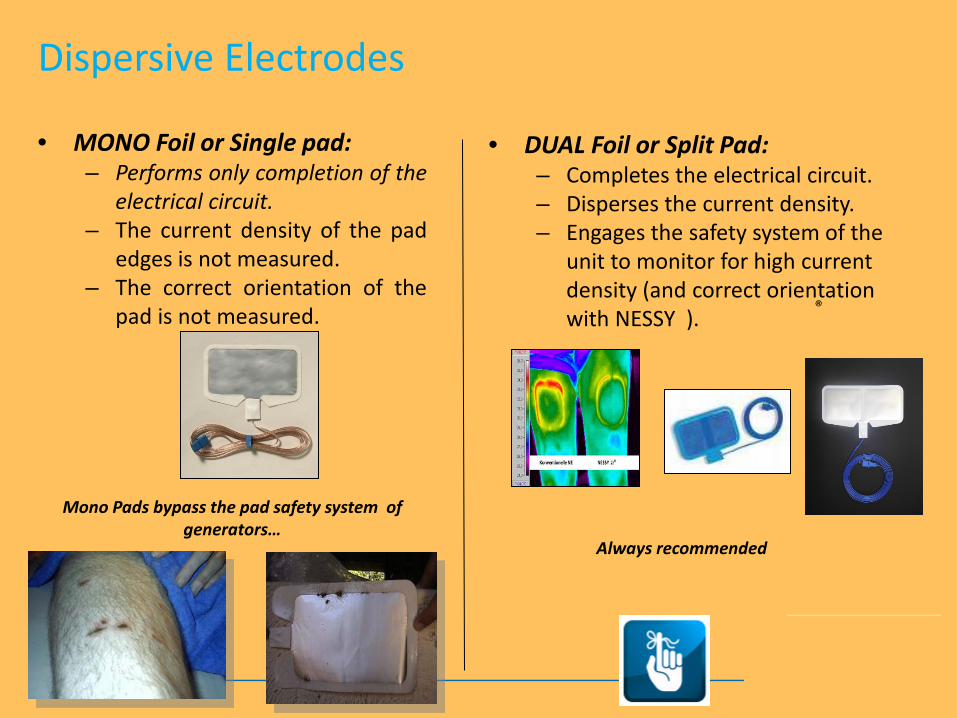
Clinical Safety
bull Use the lowest possible output settings as well as the shortest activation times
bull Confirm gas flow (with APC use) and settings prior to activation
bull Continuously monitor for signs of over-distention
bull Brief and repeated aspirations should be routinely performed throughout the procedure
Important Considerations for Endoscopy
APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

APC is a non-contact modality
If an lsquoAxialrsquo Probe probe is too close to the tissue an undesirable thermal effect or
submucosal emphysema may occur
Clinical Safety
Important Considerations for Endoscopy
Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Avoid APC activation in close proximity of metal objects
bull The APC probe should not be activated if the tip is in close proximity to metal objects
bull Unintended thermal injury of the surrounding tissue may occur
bull Metal objects may receive unintentional damage
bull Exceptions - ldquotrimmingrdquo of migrated metal stents
Clinical Safety
Important Considerations for Endoscopy
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
bull Incomplete Preps or enema-only preps for Flexible Sigmoidoscopy increases
the risk for bowel explosions bull Bowel explosions can occur with ANY
monopolar electrosurgery (eg snare APC hot biopsy) when combined with hydrogen and methane gases in a dirty colon
bull Patients should be fully prepped
The Importance of Bowel Prepshellip
Clinical Safety
Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Quiz Whorsquos has the most gas Hint Not the female
68
122408-073116
Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Clinical Safety - Oxygen Management
Combustion requires a heat source fuel and oxygen all components of the fire triangle
bull Conscious Sedation Patient Supplemental nasal cannula O2 at 3 LM or LOWER Mask delivery is considered high risk
bull Intubated Vent Patient FiO2 Concentration should be reduced to 40 or less
bull Activation Activate APC during the patientrsquos exhalation phase or during apnea
Maintain oxygen concentration at safe levels
Preventative Measures to Avoid Combustion
Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Patient Return Electrode Monitoring
bull Introduced in the 1980rsquos
ndash Return Electrode Monitoring (REM)
ndash Aspen Return Monitoring (ARM)
bull Introduced in the early 1990rsquos
ndash Neutral Electrode Safety System (NESSY)
bull Introduced in 2012
ndash Neonatal Monitoring
According to AORN guidelines return-electrode contact quality monitoring (RECQM) should be furnished on general purpose electrosurgical units
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
Dispersive Electrodes
bull According to AORN
bull Dispersive electrode site burns are the most reported electrosurgical injury
bull With improved technology and the use of safety features pad-site burns have decreased from 50 to 100 in the late 1970rsquos to one to two per month in 2007
bull Return electrode quality monitoring must be furnished
bull Dual pads should be used
2013 Perioperative Standards and Recommended Practices AORN
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
Dispersive Electrodes
bull MONO Foil or Single pad ndash Performs only completion of the
electrical circuit ndash The current density of the pad
edges is not measured ndash The correct orientation of the
pad is not measured
Mono Pads bypass the pad safety system of generatorshellip
bull DUAL Foil or Split Pad ndash Completes the electrical circuit ndash Disperses the current density ndash Engages the safety system of the
unit to monitor for high current density (and correct orientation with NESSY )
Always recommended
reg
Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Dispersive Electrode Reminders
bull Open the pad only when ready to use
bull Pads cannot be repositioned always replace the pad bull Remove pad SLOWLY to prevent skin shearing bull Always check the pad placement before activation of the ESU
bull Do not ldquotestrdquo instruments on the pad eg snares hot forceps
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
Clinical Safety
Navel and genital jewelry can be in the circuit increasing risk of burns
bull ESU Manufacturers and Clinical Guidelines recommend removal of ALL pierced and non-pierced jewelry due to the risk of burn if within the electrical circuit bull Removal helps to
minus Avoid Burns minus Avoid accidental injury minus Lower staff liability
Jewelry Removal
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
Challenge
76
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom
Clinical Safety ndash Additional Challenges
Body modifications require special attention for maintenance of the patients skin integrityhellip
Sub-dermal implants Trans-dermal and micro-dermal implants ndash
thin metal posts protruding through skin
Additional risks are posed due to - Patient positioning - Patient transfers - Electrosurgery use and pad placement
Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Implanted Electronic Devices Implanted Electronic Devices (IEDs) are battery operated devices placed within a patientrsquos body to treat a physiological defect or to replace a sensory function bull Cardiac
ndash Pacemakers ndash Internal Cardiac Defibrillators (ICDs) ndash Ventricular Assistive Devices (VADs)
bull Neurostimulators ndash Deep brain stimulators ndash Spinal cord stimulators ndash Vagal nerve stimulators ndash Programmable ventricular shunts
bull Implantable Hearing Devices Cochlear Implants Auditory Brainstem Implant (ABI) Bone-conduction stimulators
bull Implanted Infusion Pumps bull Osteogenic (Bone-growth) Stimulators bull Gastric Electronic Pumps
Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Safety Considerations ndash IEDrsquos Pre-planning is crucialhellip bull Pre-procedure knowledge of IED patients allows time
for adequate planning bull Determine the type and location of the device bull Contact the implanting physician to determine -
bull Last device evaluation bull Any specific pre-oppost-op orders for the device
bull Consider having a policy in place specific to IED patients
bull Utilize anesthesia and manufacturer device-specific guidelines as warranted to assist with establishing facility protocols and guidelines for care of IED patients
bull Contact appropriate device representatives and arrange presence during procedures based on protocols
bull Notify the physician anesthesia and other team members in advance of an IED patient
Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Implanted Electronic Devices
ldquoAORN Guidance Statement Care of the Perioperative Patient With an Implanted Electronic Devicerdquo
AORN offers guidelines for Implanted Electronic Devices
bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

bull Use Bipolar when possible
bull Keep 15 cm between the active electrode and any EKG electrode
bull Have resuscitation equipment at the ready ndash DOCUMENT
bull Have the device clinical support line available
bull Contact the IED manufacturer for specific deactivation recommendations
Electrosurgical Safety for Patients with IEDrsquos
Safety Considerations ndash IEDrsquos
Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Safety Considerations ndash IEDrsquos
If the physician must use Monopolar current bull Apply the dispersive electrode close to the
operative site but as far away from the IED as possible (eg for patients with pacemakersICDrsquos place on the opposite lower extremity to draw current away from the device)
bull Use the lowest settings possible
bull Use the shortest possible activations
bull If the ICD is deactivated re-establish integrity of the device post-procedure
Electrosurgical Safety for Patients with IEDrsquos
Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Summary
bull The ldquoartrdquo of therapeutically utilizing high-frequency (HF) electricityelectrosurgery within the hollow lumen of the GI tract requires a fundamental working knowledge of the scientific principles involved in order to optimize clinical outcomes while minimizing risks
bull It is important for the clinician to understand the basic principles and properties of electrosurgery and APC and how itrsquos adapted for clinical use
bull In addition staying well-informed on the current standards and recommended practices for clinical safety eg SGNA and AORN enhances our ability to make critical decisions and to promote optimal patient outcomes
84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

84
Gratitude to my family
122408=073116
Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom

Copyright copy 2016 Erbe USA Inc
Erbe USA Inc 2225 Northwest Pkwy Marietta GA 30067 Tel 800778ERBE wwwerbe-usacom










![Hybrid technology - ERBE Elektromedizin GmbH€¦ · [electrosurgery] technology for ablation with controlled cutting and coagulation technique. The HybridKnife® enables submucosal](https://static.documents.pub/doc/80x56/5fa0a2b90917f561bc2e3c8a/hybrid-technology-erbe-elektromedizin-gmbh-electrosurgery-technology-for-ablation.jpg)






