39
Old and new methods for detection of emerging resistant organisms Ellen Jo Baron, Ph.D., D(ABMM) Exec. Director of Medical Affairs, Cepheid Prof. Emerita, Stanford University

Old and new methods for detection of emerging resistant organisms
Ellen Jo Baron, Ph.D., D(ABMM) Exec. Director of Medical Affairs, Cepheid Prof. Emerita, Stanford University

Why are some bacteria resistant? Microbes fighting for survival in the environment (soil, human skin, GI tract)

1. Innate (missing mechanism) 2. Prevent uptake; speed exit 3. Modify target site 4. Bind up the antibiotic to prevent activity 6. Inactive the antibiotic (make a new enzyme) 7. Lower importance of target (add new mechanism)
How are bacteria resistant? Rx Target
mecA product

Example: Inactivation - Beta-lactamase
B-lactamase- Serine NCO
H2O
Serine-B-lactamase
O
NCInactive antibiotic
Active ß-lactam antibiotic
Staph aureus (& others)

ACTION OF mecA GENE mecA on transposon
Staph genome Altered genome codes for modified PBP-2a
PBP-1
PBP-2
Meth
PBP-1
PBP-2a
CELL WALL
PBP-1
PBP-2

Methods of detecting resistance 1. Phenotypic
• Agar dilution • Broth dilution (microbroth dilution) • Disk diffusion and variations • Gradient diffusion • Enzymatic detection
2. Genotypic • Mutation or other DNA change detection by PCR
(+ microarray) • Mutation or DNA change detection by line probe • Sequencing
3. Other • Growth and MALDI-TOF facilitated • Growth and Image analysis
Chromogenic cephalosporin disk

Agar Dilution: Detection of VRSA Staphylococcus aureus • Do not trust automated systems – they fail to detect VISA
Some VISA = 2 by Etest and 1 by broth MIC • Use Vanco disk & Vanco screen plate, incubate 24 h • Growth on Vanco plate & no zone = VRSA • Growth on Vanco plate & zone ≥7 mm = possible VISA/VRSA Perform Etest or send isolate to reference lab
• BHI plate with 6 mg/ml Vanco • Inoculate with swab from 0.5
McFarland suspension 30 mcg Vanco disk

Touch 4-5 isolated colonies of the SAME type with a loop or swab to pick up tiny amount from each one. Pure culture required.
Disk diffusion susceptibility testing (Bauer-Kirby method) For staphylococci, Enterobacteriaceae, Pseudomonas aeruginosa, enterococci, and other organisms that grow well on Mueller-Hinton agar in air at 35°C
# 1 Rub colonies on side of 5 ml saline tube to make very thin smooth suspension
# 2 # 3 Check using lined card & add more organisms or dilute the suspension to match McFarland 0.5 turbidity
# 4 Dip new swab into suspension & squeeze out excess liquid on sides of tube
# 5
1
2
3
# 6 Within 15 minutes, add the antibiotic disks
Rub swab over same Mueller-Hinton plate total surface 3 times in 3 different directions to create smooth layer of inoculum
BAP better than Mac to avoid mixed culture
Draw lines on card
# 7 Tap each disk or tap plate upside down to be sure disks do not fall off
# 8 Incubate 16-18 hours in air at 35°C
# 9 Measure in mm diameter of zone of inhibition across center of disks using ruler or calipers
No zone = 6 mm
# 10 Use CLSI tables to interpret zone size results for each organism & drug combination

Factors that influence results and should be monitored as part of QC Program
1. Depth of agar (3-5 mm)
2. pH and cation content of agar
3. Turbidity of organism suspension (0.5 McF)
4. Time between steps (15 min maximum)
5. Incubation temp. (35°C) & time (18-24 h)
6. Incubation atmosphere (usually air)
7. Technologist ability to accurately read zones

Detection of MRSA & MRSE
Oxacillin Cefoxitin
Staphylococcus aureus & S. lugdunensis
• Do not trust automated systems (Vitek, MicroScan) • Use 30 mcg Cefoxitin disk to screen for MRSA & MRSE • Read after 24 hrs incubation at 35° C • Cefoxitin results ≤ 19 mm report as Oxacillin-resistant (Do not
report Cefoxitin)
For all other Coag Neg Staph: Cefoxitin
• ≥ 25 mm = S • ≤ 24 mm = R

Stealth MRSA
Cefoxitin

Inducible MRSA
Before induction After induction
PBP2a Latex agglutination
MRSA Chromagar
Before induction
After induction


Gradient diffusion: Detection of Penicillin Resistance in Streptococcus
pneumoniae • Use Mueller-Hinton + 5% sheep blood agar • Incubate in CO2 instead of air • Report actual MIC
Report both Pen & Cefotaxime or Ceftriaxone & Mero MICs for S. pneumo from CSF
Oxacillin no longer will predict Penicillin susceptibility

Detection of Clindamycin resistance in Staph and Strep
Staphylococcus aureus & S. lugdunensis • Use Erythromycin and Clindamycin disks 15-26 mm apart to detect inducible clindamycin resistance
D-shape = Clinda Resistance
No D shape = Clinda susceptible
20 mm
12 mm E CC
For beta-streptococci place disks 12-15 mm apart

Phenotypic testing of Enterobacteriaceae for some drugs
Amox + Clavulanate
Moxalact
Cefonicid
Cefoperaz
Cefamand
E. coli ATCC 25922
• Cefamandole • Cefoperazone • Cefonicid • Moxalactam

CRO detection: Not so accurate
Meropenem disk
KPC Neg Control
KPC positive organism
Modified Hodge Test Chromogenic agar
P. aeruginosa
K. pneumoniae

Broth dilution methods

Results dictated by guidelines
Disk zones:
EUCAST CLSI
S ≥ R < S ≥ R < Doripenem 22 17 22 19 Ertapenem - - 23 19 Imipenem 20 17 23 19 Meropenem 24 18 23 19

INH RIF
No abx No abx
2.0 µg/mL
0.4 µg/mL
2.5 µg/mL
7.5µg/mL
6.0 µg/mL
Microscopic Observation Drug Susceptibility Assay (MODS) for Mycobacterium tuberculosis; WHO endorsed
EMB
2.0 µg/mL
STREP 0.1 µg/mL
Results usually by Day 15
Day 7 Day 15

1. Add 100 µl of 20 mM Tris-HCl lysis buffer to two 1.5 ml microcentrifuge tubes
(B-PER II (bacterial protein extraction reagent; Thermo Scientific) 2. Pick growth from around carbapenem disk on
Mueller-Hinton plate 3. Add 1/3 of calibrated loop (10 µl) of growth to each
of the lysis buffer tubes and mix very thoroughly with pipette
4. Add phenol-Zinc sulfate to Tube 1 5. Add phenol-Zinc sulfate + 6 mg/ml Imipenem to
Tube 2 6. Incubate at 37ºC for 2 hours
Nordmann/Poirel Rapid Method for Detection of Carbapenemase
Lysis Buffer Buffer + Imipen
No C’pase Red Red Positive C’pase Red Orange/Yellow Indeterminate Yellow Yellow

BioMx Rapidec Carba NP
Not FDA-cleared yet. Many steps. Takes ~ 2 h total

Molecular methods are MOST accurate Development and Evaluation of a Real-Time PCR Assay for Detection of Klebsiella pneumoniae Carbapenemase Genes. Cole et al. 2009; JCM 47:322.
• Only tiny number of labs able to develop such tests (no such commercial assays)
• New enzymes always being characterized, requiring constant modifications of PCR methods

Check-Points Microarray System
KPC VIM NDM OXA 48

Cartridge detects five classes of resistance genes in any genus • Sample: Isolate, perirectal swabs • Time to result: 48 minutes
Xpert Carba-R Assay
– blaKPC – blaNDM – blaVIM – blaOXA-48 & 181 – blaIMP-1
© Cepheid Proprietary and confidential

Xpert Carba-R Assay
© Cepheid Proprietary and confidential

MALDI-TOF and derivatives
Now: Abbott IRIDICA Delivers identification & some
resistant factors (mecA) in 8 hours
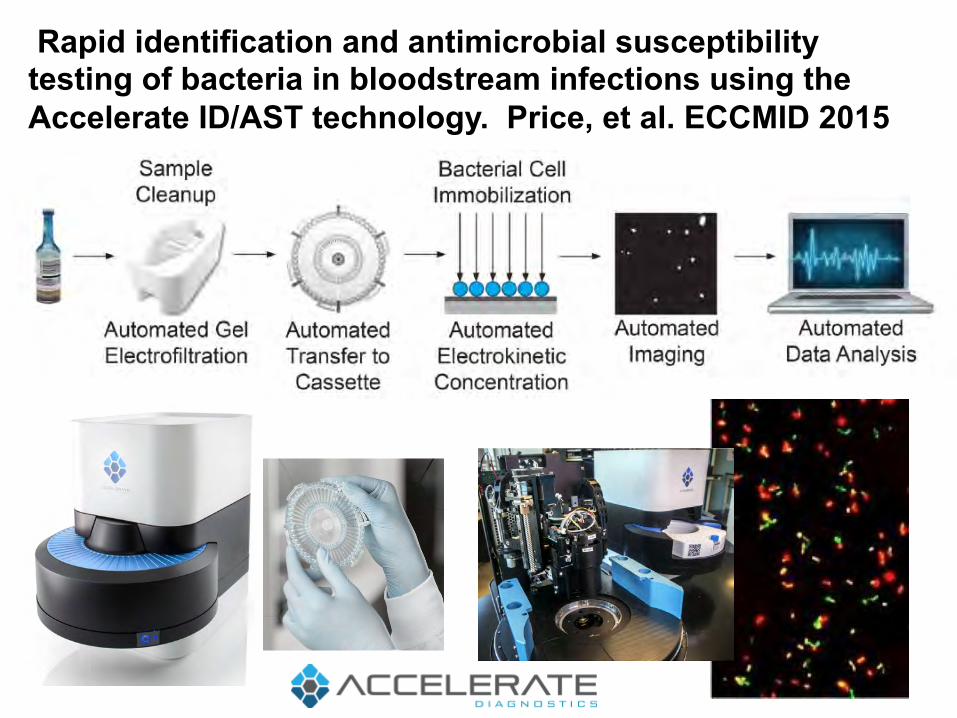
Rapid identification and antimicrobial susceptibility testing of bacteria in bloodstream infections using the Accelerate ID/AST technology. Price, et al. ECCMID 2015

Colorimetric Sensor Array D
iffer
ence
D
rug
C
ontr
ol
Rapid Determination of Antibiotic Influence and Susceptibility by Colorimetric Sensor Array Assessment of Small Molecule Metabolites. Lim et al. ASM GM 2014
K. pneumo in <5 hrs

Controls
rpoB mut’s 96% Sens
katG mut’s 35% Sens
inhA mut’s 35% Sens
HAIN GTMD (~5 hr TAT); WHO endorsed

Hain GenoType® MTBDRplus Assay

WHO endorsed

Example of Rif-Susceptible Profile All 5 probes are positive
Assay design uses RNA polymerase (rpoB) gene targets
Molecular Beacon
Target
Hybrid
Each probe is labeled with a different fluorophore, permitting simultaneous detection of the presence of wild type.
SPC

Improved assay: 4 probes identify rifampin-R mutations in rpoB by shifting their Tm away from a wild type reference value by melt curve analysis
Probes overlap rpoB sequence
A clear change in Tm distinguishes wild type from resistant mutant
Rif S Rif R
rpoB core region. Any mutation = Rifampin resistance
Xpert® MTB/RIF Ultra

July 2011. Vol.8, Issue 7 e1001061
Sequencing includes Mutations in katG, inhA, the inhA locus (inhA regulatory region), the oxyR-ahpC intergenic region (ahpC) and the entire rpoB gene.
• Mutations in rpoB occur in 95-99% of Rif-R strains • Rif-R is a good indicator of MDR-TB • 23 discrepancies between phenotype & genotype

S. aureus genome map of Res SNPs

S. aureus results of Sequencing program (Mykrobe) vs phenotype (3 minute computer run-time)

Sequencing Required: Best method = minION
Potential to reduce
sequencing time from 24 h to 7 h

New technologies are revolutionizing the detection of microbial resistance and improving healthcare worldwide

















