17
Emergency Department Thoracotomy in the management of Chest Trauma Sudhir Sundaresan, MD FRCS(C) Division of Thoracic Surgery May 28, 2009
| Date post: | 01-Jan-2016 |
| Category: |
Documents |
| Upload: | ocean-santos |
| View: | 55 times |
| Download: | 7 times |
Emergency Department Thoracotomy in the management
of Chest Trauma
Sudhir Sundaresan, MD FRCS(C)Division of Thoracic SurgeryMay 28, 2009

ED Thoracotomy: Historical
Late 1800’s – cardiac wounds, anesthesia-induced arrest
1874 – Schiff – open cardiac massage Until 1960 – “medical” arrests
– 1960 – CPR
– 1965 – external defibrillation
Late 1960’s – resurgence in trauma Currently – selective approach (Injury,
physiologic status)

Definitions
No V/S = No blood pressure - vs -
No “signs of life” (SOL)– No BP
– No resp effort
– No motor effort
– No cardiac electrical activity
– Fixed / non-reactive pupils
ED Thoracotomy: When?
Post-injury Cardiac arrest– Penetrating: witnessed; < 15mins CPR
– Blunt: witnessed; < 5 mins CPR
Persistent shock (SBP<60)– Hemorrhage
– Tamponade
– Air embolism

ED Thoracotomy: When NOT?
Post-injury Cardiac arrest– Penetrating: > 15mins CPR and NO SOL
– Blunt: > 5 mins CPR and NO SOL
Prior chest surgery (sternotomy, thoracotomy)

ED Thoracotomy: Survival correlates with Injury pattern and status of patient
Injury
Pattern
Shock No V/S No S.O.L Overall
Cardiac 35% 19% 3% 16%
Penetr. 14% 8% 1% 10%
Blunt 2% 1% 0 1.4%

ED Thoracotomy: Technical aspects
Supine, Left arm out of the way Incision: left submammary; clamshell Pericardiotomy

ED Thoracotomy: Technical aspects
Pericardiotomy:– Hemorrhage control– Cardiac repair– Foley technique

ED Thoracotomy: Technical aspects
Open massage and resuscitation:– 2-hand technique– Intracardiac epinephrine– Internal defibrillation

ED Thoracotomy: Technical aspects
Occlude thoracic aorta:– Retract lung superiorly, suction
– Dissect out aorta just above diaphragm

ED Thoracotomy: Purpose
Release tamponade Control exsanguinating intrathoracic
hemorrhage Open cardiac massage
– Closed chest CPR: 25% CO, 20% cerebral perfusion – OK for 15 mins at normothermia
Clamp aorta Deal with broncho-venous air embolism
04/20/23 12
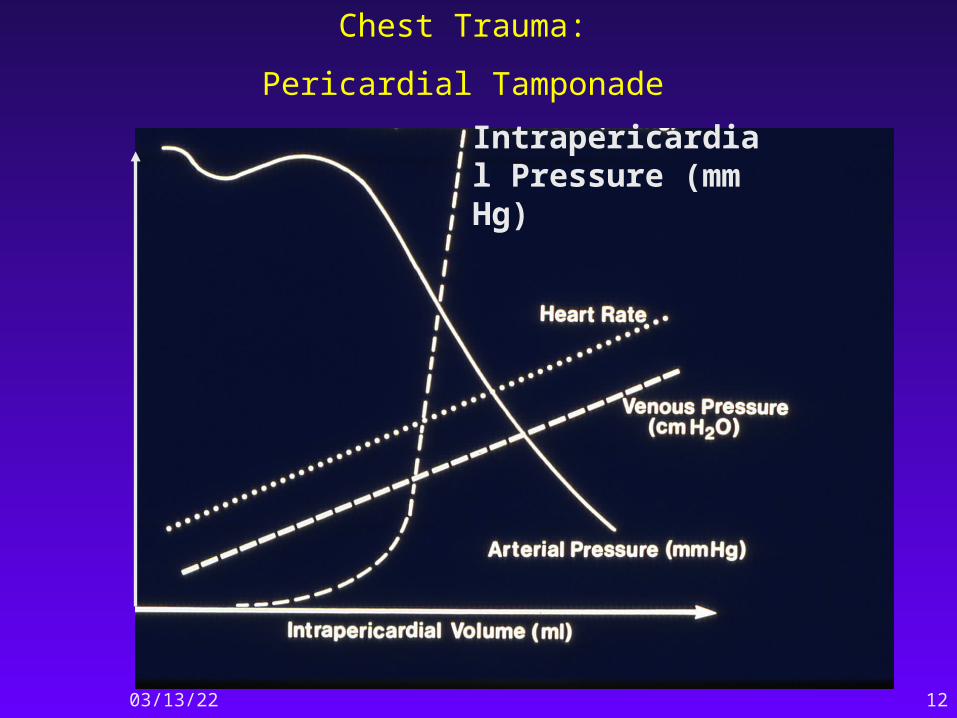
Chest Trauma:
Pericardial Tamponade
Intrapericardial Pressure (mm Hg)
ED Thoracotomy: Aortic clamping
Redistribute blood flow (brain,heart) Address intra-abdominal hemorrhage Extremity injuries Downside (limit to < 30 mins)
– Paraplegia
– Anaerobic gut metabolism massive ischemia/reperfusion injury
ED Thoracotomy: Air embolism
Pulmonary broncho-venous air emolism Penetrating > blunt injuries Scenario: hypotension/arrest after
intubation/PPV Management:
– ED thoracotomy
– Hilar clamping
– Pericardiotomy, de-air the heart
04/20/23 15
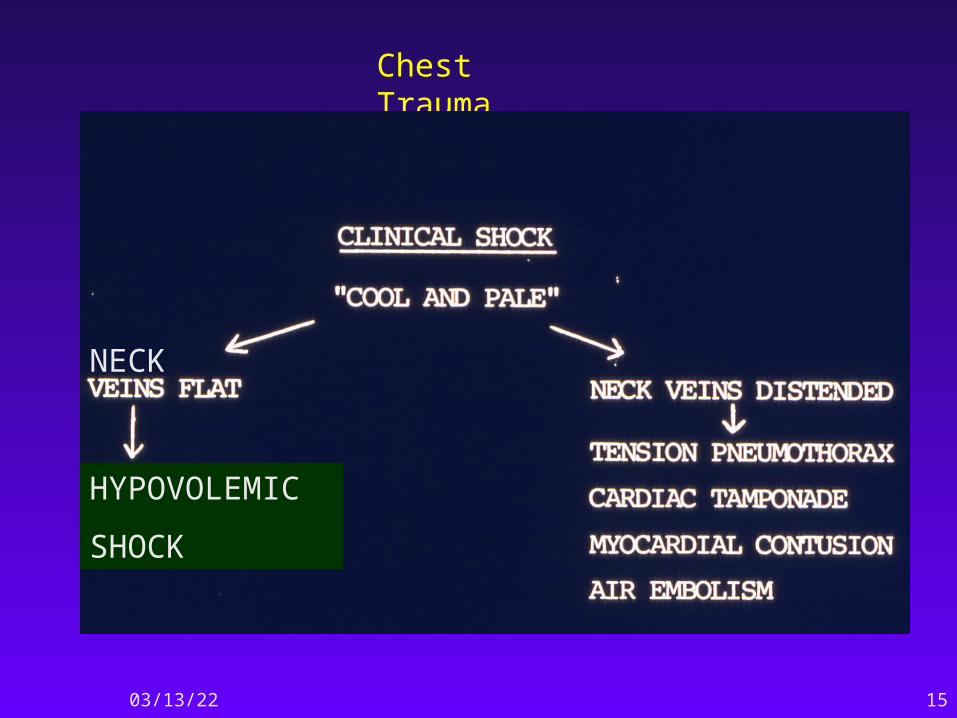
Chest Trauma
NECK
HYPOVOLEMIC
SHOCK

ED Thoracotomy: Downside
Injury to intrathoracic structures Consequences of anaerobic metabolism
– Massive ischemia-reperfusion injury
Post-pericardiotomy syndrome Exposure of HCW’s to blood-borne
pathogens– HIV – 4%
– Hepatitis C – 14%

Reference
Cothren CC, Moore EE. Emergency department thoracotomy for the critically injured patient: Objectives, indications, and outcomes World J Emerg Surg. 2006; 1: 4.

















