Emergency Medical Services Education Program EMT – AEMT – Paramedic Missouri Bureau of EMS Accreditation #09529T6 Field Preceptor Guide University of Missouri-Kansas City School of Medicine Department of Emergency Medicine Emergency Medical Services Education Program 2411 Holmes Street Kansas City, Missouri 64108 Jay Reich, M.D., FACEP EMS Section Chief, Department of Emergency Medicine Assistant Professor – Emergency Medicine Erica Carney, M.D., ABEM EMS Education Medical Director Assistant Professor – Emergency Medicine Paul Ganss, M.S., NRP, NCEE, CHSE EMS Education Program Director Clinical Assistant Professor – Emergency Medicine
Transcript
Emergency Medical Services
Education Program EMT – AEMT – Paramedic
Missouri Bureau of EMS Accreditation #09529T6
Field Preceptor Guide
University of Missouri-Kansas City School of Medicine Department of Emergency Medicine
Emergency Medical Services Education Program 2411 Holmes Street
Kansas City, Missouri 64108
Jay Reich, M.D., FACEP EMS Section Chief, Department of Emergency Medicine
Assistant Professor – Emergency Medicine
Erica Carney, M.D., ABEM EMS Education Medical Director
Assistant Professor – Emergency Medicine
Paul Ganss, M.S., NRP, NCEE, CHSE EMS Education Program Director
Clinical Assistant Professor – Emergency Medicine
Ver. 11-2015 2
Contents Overview 03 Intern Scoring and Measurement 03 Performance Appraisals 05 Establishing a Positive Learning Environment 05 The Adult Learner 06 Qualities of a good Preceptor/Learner 07 Preceptor Requirements 08 Program Requirements 08 Institutional Flow Chart 09 Field Internship Performance Objectives 10 Field and Clinical Requirements 11 Dress Code and Professional Behavior 13 Punctuality, Preparedness and Absences 13 Scheduling and Changes 13 Injury/Medical Liability 13 Fire Suppression 14 Clinical Review Sessions 14 Area Orientation 14 Paramedic Scope of Practice 15 Performance as a Crew Member 17 Documentation 19 Completing the Clinical/Field Evaluation Form 20 ALS Field Leads 21 Appendix A Program Syllabus Appendix B Program Clinical and Field Forms Appendix C Platinum Planner preceptor user manual
Ver. 11-2015 3
UMKC School of Medicine EMS Education Programs
Preceptor Program
Overview The Paramedic Intern will arrive with two critical elements. Their initial didactic training is provided to them as the basic foundation for their career as a paramedic. Their initial clinical preparation has brought their basic foundation together with a somewhat controlled treatment environment, in order to develop their basic patient interaction, thought processes, and psychomotor abilities. The current phase that they are embarking on is their Field Internship. It is the responsibility of the preceptor to evaluate, critique, and positively influence the new paramedic. The preceptor is their guide to a strong and effective foundation development for a productive and meaningful career in the treatment of the sick and injured.
This manual is provided to assist the preceptor not only in the technicalities of the Emergency Medical Services program, but to guide both the preceptor and the intern through a standard and consistent Field Internship phase. However, it should be noted that one of the major factors (and all too often overlooked) in the development of the new paramedic is the environment that the preceptor and the hosting agency provide on a daily basis. It should be remembered that the culture which surrounds the intern on a daily basis will directly affect their development as a paramedic, and their overall development as a professional EMS provider. It is incumbent upon the preceptor to continually evaluate the social surroundings, and commit to providing a professional and ethically superior environment for intern learning. Only then will this manual provide the best direction and consistency necessary to begin the intern on a sound educational and practical foundation.
Each intern must be treated as an individual, without specific regard to his or her ethnicity, socioeconomic background, gender, disabilities, age, sexual preferences, religious beliefs, political views, or cultural background. Make every effort to garner an atmosphere of mutual respect with interns, eliminating any harassment, exploitation or discriminatory treatment of interns, peers, and patients.
Intern Scores and Measurement How the Intern is measured: The intern is measured against the standard, which is a competent entry-level paramedic.
The definition of a competent entry-level paramedic is an individual who can operate safely within the standard of care. The definition of the standard of care is the degree of care, skill, and judgment that would be expected under like or similar circumstances by a similarly trained, reasonable paramedic in the same community. The intern is NOT measured against another intern, provider, or the preceptor. They are not measured by how well they are doing for a certain time in the field, or by whether the preceptor likes the intern or not. The intern is not measured against past experiences by the preceptor when he or she was an intern. The intern is measured by cognitive, psychomotor and affective skills. The standard does not change through the clinical/ field experience. The standard is not subjective but it is objective.
Ver. 11-2015 4
Performance Appraisals “If you can’t measure it—you can’t manage it”
So often we look at ourselves and ask, “Where are we and where are we going?” A common but accurate response suggests in general terms that we must not and cannot remain constant in a changing environment. As a paramedic preceptor you have answered this question already, now it is your opportunity to help the paramedic intern answer this question.
Performance is and will be vital. Preceptors will be responsible for how paramedic interns perform. One suggestion to this task is a structured, reliable, valid performance appraisal system as well as feedback to the paramedic intern as to his/her position in relation to his/her goals.
Much of the responsibility for the process falls on the shoulders of the preceptor, and the success of the process becomes dependent on two key factors: the preceptor’s commitment to the philosophy of performance appraisals and the preceptor understands the process as well as recognition of its complexity. If commitment and understanding are present, only then can a program lead to performance improvement, increased motivation, enhanced personal development, and greater job satisfaction.
Preceptors must adopt a leadership style to define good performance, recognize it, and reward it. Only positive consequences encourage good future performance. Leadership can be a process of different styles for individuals at different time frames during the development process. Four (4) different leadership styles are:
• Directing
• Coaching
• Supporting
• Delegating
Establishing a Positive Learning Environment It is important to establish and maintain a positive learning environment. This can be accomplished in several ways.
Instruct in the positive. We know from experience this allows interns to learn and respond to directions more quickly and easily. Tell the intern what you want them to do, not what you do not want them to do. This will be difficult in the beginning and will take practice. The results will be amazing. Positive instructions are nurturing, negative instructions are controlling.
Counsel in the positive; in discussions with the intern tell them:
• What went well and what needs work or revision
• Specifically, how to fix the skill or behavior
• When the skill or behavior will be practiced and when it will be evaluated again
• Be the advocate for your intern
• Be the intermediary between your intern and other practitioners
Ver. 11-2015 5
• Praise in public
• Critique in private
• Maintain confidentiality for all interns
• Keep it simple:
• What is the problem?
• Why is it a problem?
• What needs to be done to fix the problem?
• When will the evaluation take place? (Time frame)
Make sure that communication between the preceptor and the intern has taken place by having the intern explain what was just said by the preceptor.
Keep in mind your behaviors have a significant impact of the behavior and attitude of the intern. For example, your silence and distance are perceived by the intern as an indication they have done something wrong. Always be honest with the intern. If you are upset with them and need time to reflect, tell them. If you are angry about something else and need time to reflect, tell them that.
Ver. 11-2015 6
The Adult Learner
• Characteristics
o Self directed
o Usually demanding of knowledge
o Career and goal oriented
o Has competing demands on time from family, employment, and outside stresses
• Positive Attributes of Adult Learners
o Desire to learn
o Desire to succeed
• Difficulties with Adult Learners
o May feel older and wiser than the preceptor
o May have a know-it-all attitude
o Less interested in direct input
o May know more than the preceptor didactically
o The preceptor may feel guilty failing a person with a family who has tried hard to succeed.
Ver. 11-2015 7
Qualities of a Good Learner / Preceptor Many of the qualities that make up a good preceptor are the same as those which make up a good learner. First, the preceptor must be willing to define his or her relationship with the intern. The preceptor is not the intern’s best friend, nor is he or she the intern’s worst enemy. The preceptor should not be too friendly at first as providing critical and objective feedback may be difficult. Being overly friendly can also create confusion with the intern as to his or her relationship with the preceptor and what role that relationship plays in the intern’s education. The preceptor should be supportive and act in the role of advisor, teacher, and mentor. It is very important that the intern can believe and trust his or her preceptor, and the preceptor should never attempt to trick the intern. The preceptor should also watch out for the intern including social interactions around the field site, and making sure that other responders respect the intern’s learning process and don’t step in to help too much.
Beware of micro-managing the intern. The intern must be responsible for his or her actions. Help them plan their learning during the time they are with you. What procedures do they need to learn more about or gain practice at? Are they taking the lead role and being effective? If not, what do they need to improve upon? If they have downtime, the preceptor may be able to facilitate (or suggest) review of didactic materials. The preceptor needs to monitor the intern’s progress and assess their progress, stepping in when necessary to ensure the comfort and safety of the patient. This will require choreography on the part of the preceptor. As the eyes of the program in the field, it is the preceptor who assesses the progress and maturity of the intern. The effective preceptor will time task delegation carefully, gradually adding more responsibility, and pulling responsibility back if additional assistance is required.
The program establishes goals and objectives for the overall completion of the program; however, the preceptor will establish goals and objectives on a shorter term. No intern will go on every single call and perform at 100%. It is expected that the intern will have periods of progression where performance gradually improves, and periods where there is some regression (bad days). The preceptor can help the intern through coaching and setting goals for performance improvement on the next call, or the next shift and communicating these expectations to the intern. Also, the preceptor must document these improvement plans so other preceptors may be aware and build upon them.
The preceptor should have acceptance of self, that is a high degree of self-confidence in his or her knowledge and abilities and the ability to recognize that he or she is human and may make mistakes once in a while. The preceptor should accept interns and patients as being a necessary part of his or her job, and the unique challenges and experiences that these individuals bring. Conversely, a preceptor who does not like interns, or finds him or herself annoyed by patients will probably not contribute very much positive to the intern’s field experience.
Preceptors must be congruent. An effective preceptor is believable to the intern and practices what they teach. If a preceptor advises an intern to communicate with a patient in a specific manner, or advises an intern to perform a procedure in a certain way, then the preceptor should not act differently. From time-to-time the preceptor may take actions or make decisions in his or her head that contradicts what the intern has been taught or told to do. In actuality, the preceptor is doing exactly what the intern was told to do, but is doing it without “thinking out loud” because of experience. In these cases, it is important that the preceptor advise the intern of his or her thought process as to why a decision was made a certain way.
Empathy is a required quality of a good preceptor. The preceptor must be able to see the experience from the intern’s point of view, remembering that we were all interns at one point, starting in a new career field and doing things that we were not familiar with. We must be able to recognize how patients are seeing the situation and how they may feel.
Ver. 11-2015 8
There are times that the preceptor may want to step in because the call is not going well from a patient’s point of view. Having empathy does not mean you must accept the intern or patient’s point of view. A good preceptor, however, will affirm it.
Preceptor Requirements The preceptor should be a Missouri-licensed Paramedic, and have 2 years field experience in pre-hospital care as an ALS provider. Furthermore, he or she must be recommended by the employing agency. The preceptor will work in collaboration with the Clinical Coordinator. Preceptors should be a positive role model for the intern, and not currently under investigation for clinical or patient care issues in the last 24 months.
Training Institution Requirements The training program will enter into a written agreement with any agency involved in intern training. In addition, the following stipulations apply:
• No more than 1 intern assigned at the same time on a unit without the permission of the field agency.
• The intern must never be used as a paid substitute for paid personnel or required team member.
Ver. 11-2015 9
Training Institution Flow Chart
First point of contact should be the Clinical Coordinator then the Program Director.
Program Director Medical Director Paul Ganss, M.S., NRP, NCEE Erica Carney, MD (816) 235-5355 (Office) [email protected] (816) 590-8560 (Mobile) [email protected]
Field Internship Performance Objectives The field internship will offer the intern the opportunity to perform many or all of the skills explored in the didactic and clinical portions of the program. The environment will change from the controlled to the uncontrolled and will afford the intern the environment in which to “put it all together”.
At the end of the field internship, given a real patient or response scenario, the Paramedic Intern will with at least 85% accuracy:
• Determine safety for self, team members, and patient and ensure an adequate work environment in a timely manner (100%).
• Use universal precautions and wear appropriate personal protective equipment specific for patient condition, clean and sanitize equipment in accordance with provider policy and procedures (100%).
• Initiate or delegate appropriate crowd control and deal effectively with family members and bystanders.
• Recognize the need for and request additional assistance or equipment needed in a timely manner.
• Perform an organized primary assessment and intervene appropriately in a timely manner.
• Obtain a relevant and accurate patient history, chief complaint/problem, medications and allergies in a systematic and timely manner.
• Perform a thorough exam with appropriate inquiry and inspection pertinent to the patient’s chief complaint with accurate findings.
• Interpret and correlate assessment information correctly.
• Identify breath sounds and have adequate knowledge of chest auscultation.
• Identify cardiac rhythms in an accurate and timely manner.
• Develop and implement an appropriate plan of action.
• Assure the adequate delivery of oxygen to a patient, including the use of appropriate airway adjuncts and achieving or maintaining patency of the airway in a timely manner.
• Correctly use advanced airways in a timely manner.
• Use all equipment correctly.
• Assess patient response to therapy and interventions.
• Communicate all pertinent information to team members.
• Utilize medical control appropriately, including organized and complete radio reports.
• Complete patient care reports in an accurate, thorough and legible manner.
• Function as a member of the patient care team.
Ver. 11-2015 11
• Assume a leadership role and direct members appropriately.
• Exhibit a professional demeanor.
• Build rapport with patient, family and bystanders, showing consideration and respect for others, and instilling confidence in the patient.
• Participate in the evaluation of self; including accepting feedback and suggestions and taking necessary steps to correct performance.
• Re-supply all inventory per provider policy.
• Demonstrate respect for the dignity of each individual he or she is associated with in the practice of his or her professional duties.
• Respond to the field-learning environment in such a manner to invite confidence of patients, supervisors, peers and other health care professionals.
Field and Clinical Requirements Listed below are the skills and hours goals and requirements of the Paramedic program. Most interns will complete more than the minimum skills required in each skill category. The intern shall document all skills completed even if those skills are above the minimum required. While interns may be required to complete additional hours to meet skills goals, the minimum clinical hours must be met even if the skills goals are met earlier.
Minimum Clinical Hour Requirements Intermediate PHLS Advanced PHLS Total (AEMT) (Paramedic) Critical Care (ICU) 12 48 60 Emergency Department 60 120 180 Burn Unit 12 12 24 Mental Health Unit -- 8 8 Surgery/Recovery -- 24 24 Pediatrics 8 8 16 Family Practice/Primary Care -- 8 8 Labor and Delivery 8 16 24 Nursery/Mother Baby -- 12 12 Respiratory Therapy 8 8 16 Cardiac Catheterization Lab -- 8 8 Medical Director -- 4 4 Total Hospital Hours 108 276 384 Total Field Hours for AEMT 84 (Extra AEMT Field Hours do not carry over to Paramedic)
Clinical Skill Requirements Supraglottic Airway and Intubations (Complete airway competency pathway before going to OR) Venous Access (all ages) 10 50 60 Childbirth (Observe/Perform) 1 5 6 Medication Administration (Total) 30 60 90 Minimum of each of the following required: IM Injection 5 5 SQ Injection 5 5 Inhaled Medication 5 10 IVP Medication 5 20
Ver. 11-2015 12
ECG 3-Lead Interpretations -- 50 50 Requires verification by a preceptor in the clinical or field setting. ECG 12-Lead Interpretations -- 50 50 Requires verification by a preceptor in the clinical or field setting. BVM (non-intubated patients) 5 5 10 Pediatric Assessments 10 30 40 Minimum of each of the following required: Newborn (0-30d) 1 4 Infant (30d-1yr) 1 4 Toddler (1yr-3yr) 1 4 Pre-School (3yr-6yr) 1 4 School-age (6yr-12yr) 1 4 Adolescent (12yr-18yr) 1 4 Assessments 75 200 275 Minimum of each of the following required:
Syncope* -- 10 *Condition-based assessments only apply to patients who have a complaint specific to that subject area (i.e. respiratory distress) and the Paramedic student assessed that body system and planned a course of treatment based upon the exam findings. Students may claim no more than TWO systems-based assessments per patient. Blood Draw 5 10 15
Medication Added to Solution -- 10 10
Field Internship Requirements Paramedic students must complete the didactic portion of the Paramedic program, passing the Didactic Final Exam and Final Psychomotor Exam, plus complete all clinical hours and skill requirements before they may enter the field internship phase of the program. Intermediate PHLS Advanced PHLS Total (AEMT) (Paramedic) Field Observation Hours for AEMT 84 Minimum Internship Hours for Paramedic 276 Total Minimum Field Hours 360 EMS Field Leads (ALL FIELD LEADS) 10 90 100 Note that 100 field leads is the minimum. Eighteen of the last 20 leads in the series must be successful in order to meet this requirement. This is a rolling block of field leads meaning that when the minimum number has been met, the requirement is met when out of the final 20 leads, 18 are successful. Successful is defined as a “2” in the Team Leadership category of the Field Evaluation Worksheet. ALS EMS Field Leads -- 40 40 Note that 40 ALS Field Leads is the minimum required. Eighteen of the last 20 ALS Field Leads must be successful in order to meet this requirement. This is a rolling block of filed leads meaning that when the minimum number has been met, the requirement is met when out of the last 20 ALS Field leads, 18 are successful. Successful is defined as a “2” in the Team Leadership category of the Field Evaluation Worksheet. + A percentage of skill goals may be completed through simulation at the Medical Director’s and Lead Instructor’s discretion. *See Field Lead form for what constitutes a field lead. ** 18 of last 20 leads must be successful.
Ver. 11-2015 13
Dress Code and Professional Behavior As the Paramedic intern is direct reflection of UMKC and the EMS Education program, it is imperative that the intern maintain a clean and professional appearance at all times. Each intern must arrive at their assigned station or workplace on time, appropriately attired, including a school uniform and approved nametag, and a generally professional appearance. Depending on circumstances, you may send any intern arriving late for their shift or without these items home and notify the Clinical Coordinator.
Paramedic interns are expected to follow the dress, grooming, and conduct standards of the field site. This would include items such as visible tattoos, jewelry, and tobacco use or e-cigarette use.
A portion of the intern grade is based upon their professional appearance and behavior. It is important that the preceptor reflects and encourages this behavior and appearance throughout the paramedic intern’s internship. Failure of the intern to fulfill this requirement will count against his/her grade. Situations regarding professional appearance or behavior must be addressed in a timely fashion with the use of written performance evaluation and improvement plans, outlining deficiencies and methods for immediate improvement. These issues should be brought to the Clinical Coordinator’s attention as soon as possible.
Please refer to the Program Syllabus for the rules and regulations.
Punctuality, Preparedness, and Absences Interns are expected to be on time, and an emergency or unavoidable shift holdover (i.e. late run at a full time job) is the only acceptable excuse for being late. If an intern is less than 15 minutes late on shift, they may be allowed to stay. If the intern is more than 15 minutes late on shift, they will need to notify the Clinical Coordinator. Interns are expected to show up for their assigned shifts, and are responsible for notification of the clinical site and Clinical Coordinator if they are unable to attend their shift for any reason.
Schedule Changes The overall internship program is to teach the Paramedic interns’ how to conduct themselves in an appropriate manner for the profession. It is encouraged that they participate in their regular schedule as assigned, and there should be no deviation from that schedule. In the event that they must call in sick, every effort must be made to contact the Clinical Coordinator, prior to the occurrence if possible. The preceptor should be notified as well, especially if the intern must leave a shift early for some reason. Any portion of a shift not completed will not be counted toward the overall required hours, and depending on circumstances, may count against the professional behavior of the intern. In addition to the Clinical Coordinator, the Preceptor (or shift officer/charge nurse) must be notified of the absence by the Clinical Coordinator (Not the intern).
Injury / Medical Liability Any injury or medically related event should be handled appropriately to the event. If the event requires immediate care or treatment, provide care including access to emergency services as you would with any request for EMS. In the event of an injury or communicable disease exposure to the intern, notify the Clinical Coordinator and/or Program Medical Director immediately. While financial responsibility for payment of medical care costs will vary depending upon the intern’s personal situation (i.e. private pay, sponsored by an agency and worker’s comp.), ultimately the intern and not the clinical or field site is responsible for the costs of any medical care.
Ver. 11-2015 14
Fire Suppression As the intern is participating in the field internship as a medically-oriented Paramedic intern, there will be NO FIRE SUPRESSION OR FIRE GROUND ACTIVITIES by the Paramedic intern allowed, regardless of their training or position in their home department. This includes special operations such as extrication, technical rescue, hazardous materials, and water rescue (generally any activity that requires specialized PPE and specialty training). Fire ground rehab activities in the cold zone are acceptable. ANY deviation from this policy by the intern will be grounds for expulsion from the program. In the event that the Preceptor must participate in fire ground activities as part of their normally assigned duties, the Paramedic intern will stay clear of any activity that may put them in jeopardy or danger, preferably in or near their assigned response unit or another area designated by the Incident Commander.
Clinical Review Meetings Interns may be required to attend class meetings that occur during the internship. If a meeting occurs during a scheduled field shift, the intern should be excused from field to attend the meeting and will return to their shift directly after the meeting. The purpose of these meetings is to give the Program first-hand knowledge of how the intern is doing and to counsel the intern and answer any questions.
Area Orientation Checklist We have informed the paramedic intern that he or she is a guest in your facility. As a guest, their behavior should reflect the traits associated with this position. The program encourages the assignment of reasonable station duties, as would be assigned to any other working member, to paramedic interns during their internship phase. Such assignments should help the intern to develop personal and professional responsibility in the EMS environment, and establish a healthy working relationship with the members of the crew. The following checklist is designed to help you orient the intern to your agency’s policies. The site may add or delete items from this list as appropriate to the site.
• Tour of station or department • Introduction to personnel • Specific phone number needed to call in • Station duties/house chores • Agency specific policies • Equipment check and restock • Primary catchment/base hospital • Other catchment hospitals • Other agencies where they may interface • Documentation procedures • Special communication problems • Any necessary financial information • Meal information and/or house dues • Agency-specific dress code and smoking policies
Ver. 11-2015 15
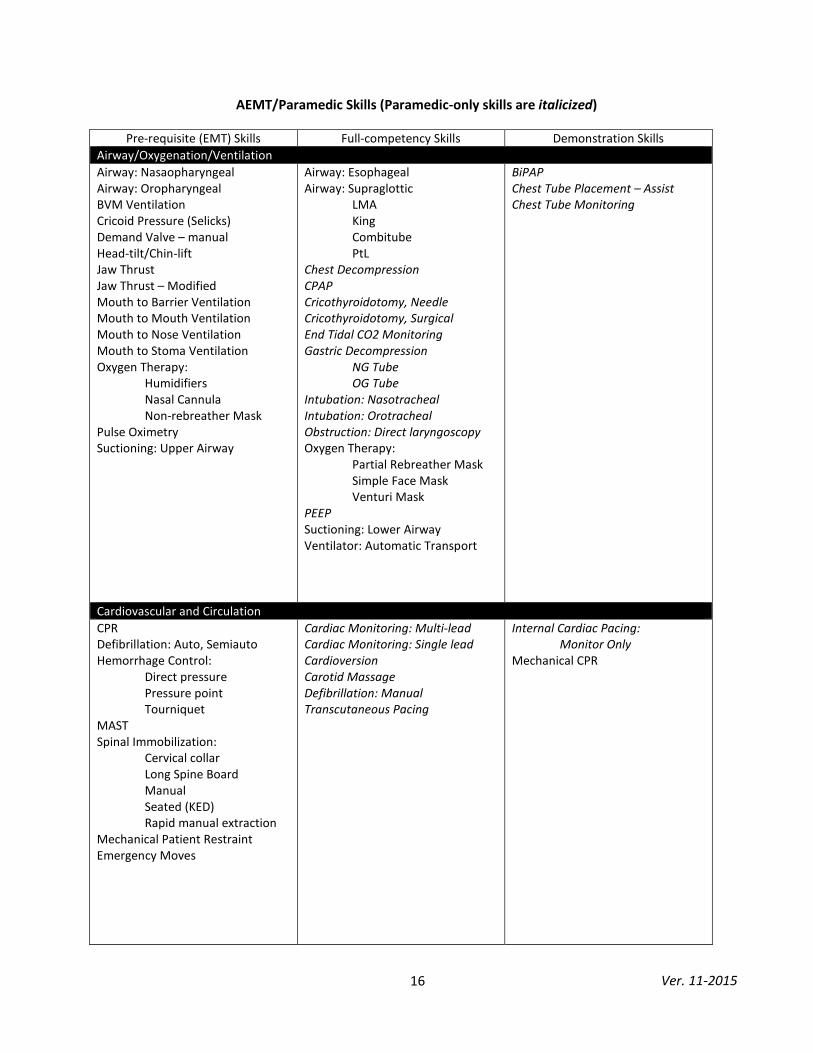
Paramedic Scope of Practice In order to establish the baseline for the required and allowed care to be rendered by the Paramedic intern, both the intern and the Preceptor must be familiar with the guidelines regarding the Paramedic’s scope of practice. From time-to-time, Advanced EMT interns or Paramedic interns in the intermediate phase of their training may be in the field setting. Paramedic-only skills are denoted in italics on the following chart of skills.
Without direct supervision of the preceptor (direct defined as line-of-sight and ability to verbally communicate) the intern must act as a BLS (EMT) provider and work within that scope of practice.
In the event that an EMS crewmember becomes a patient, they cease to be an EMS provider and cannot provide direct supervision.
In addition to these regulations, it should be clearly understood that any intern who falsifies documentation in any manner, or who performs outside the direct supervision of their preceptor for any reason will be immediately dropped from the program. Any incidents of this nature should be reported to the program as soon as possible.
Ver. 11-2015 16
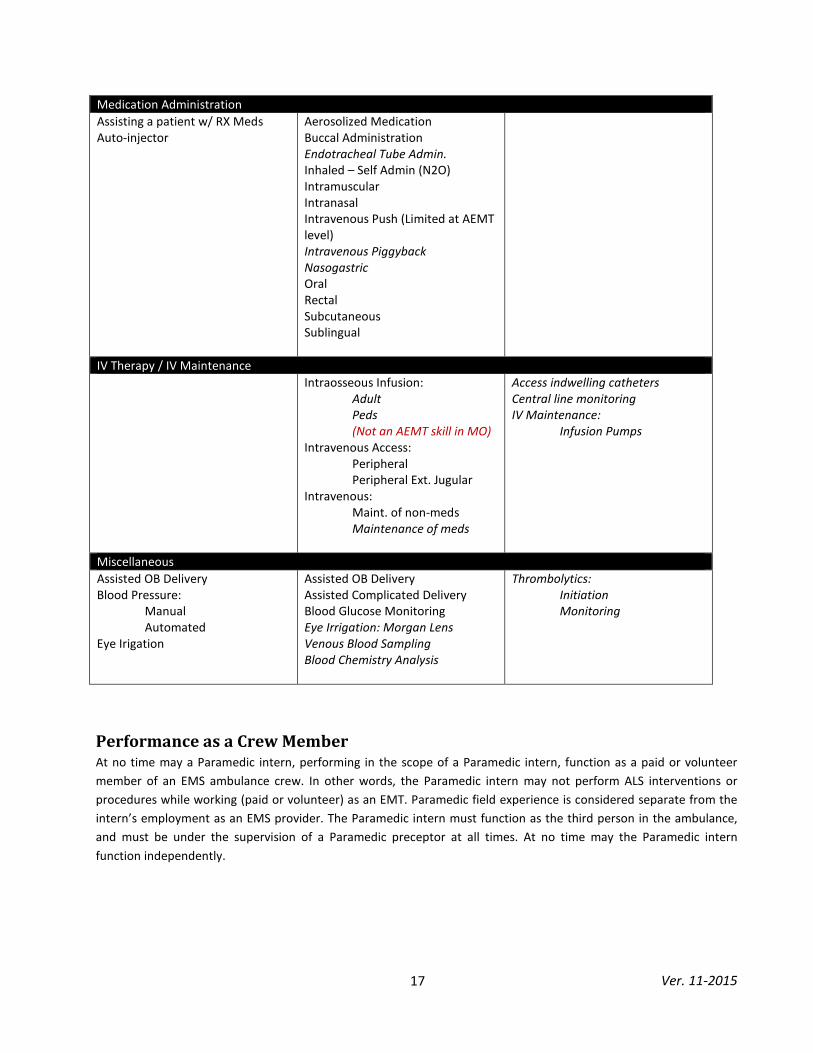
AEMT/Paramedic Skills (Paramedic-only skills are italicized)
IV Therapy / IV Maintenance Intraosseous Infusion:
Adult Peds (Not an AEMT skill in MO)
Intravenous Access: Peripheral Peripheral Ext. Jugular Intravenous: Maint. of non-meds Maintenance of meds
Access indwelling catheters Central line monitoring IV Maintenance: Infusion Pumps
Miscellaneous Assisted OB Delivery Blood Pressure: Manual Automated Eye Irigation
Assisted OB Delivery Assisted Complicated Delivery Blood Glucose Monitoring Eye Irrigation: Morgan Lens Venous Blood Sampling Blood Chemistry Analysis
Thrombolytics: Initiation Monitoring
Performance as a Crew Member At no time may a Paramedic intern, performing in the scope of a Paramedic intern, function as a paid or volunteer member of an EMS ambulance crew. In other words, the Paramedic intern may not perform ALS interventions or procedures while working (paid or volunteer) as an EMT. Paramedic field experience is considered separate from the intern’s employment as an EMS provider. The Paramedic intern must function as the third person in the ambulance, and must be under the supervision of a Paramedic preceptor at all times. At no time may the Paramedic intern function independently.
Ver. 11-2015 18
The following information is excerpted from a Missouri Bureau of EMS memorandum. Please direct any questions regarding this information to the Missouri DHSS, Bureau of EMS.
With the passage of the Comprehensive EMS Act of 1998, regulations were written to accredit training entities. In 19CSR 30-40.331, there are specific sections regarding clinical experience by Paramedic interns. (2) Specific Requirements for EMS Training Entities Offering Initial EMT-P Courses
(B) EMT-P interns are only authorized to perform skills and practice in accordance with the national standard curriculum for EMT-P and approved by the training entity medical director. The skills and practice performed by the intern must be under the direct supervision of a clinical preceptor and cannot be performed while being employed as an EMT-B. (H) Clinical Requirements.
1. Each EMS training entity that provides EMT-P programs shall document and demonstrate a supervised clinical experience for all interns. 2. Clinical affiliations shall be established and confirmed in current written affiliation agreements with institutions and agencies that provide clinical experience under appropriate medical direction and clinical supervision.
3. Interns shall be assigned in clinical settings where experiences are clinically and educationally effective in achieving the program’s objectives.
4. When participating in clinicals, interns will be clearly identified by name and intern status using nameplate, uniform, or other apparent means to distinguish them from other personnel. 5. Field internship shall occur only in association with an Advanced Life Support ambulance service, which demonstrates medical accountability and employs preceptors who meet the training entity requirements.
This regulation was written to prohibit EMT-P interns from performing skills during the course of their employment as an EMT-B. It also would prevent interns from, for example, riding on a rescue truck as an EMT and performing skills at the scene. It also prohibits an EMT-Basic, during the course of a scheduled shift as an EMT-B, from performing any ALS skills since they are present to work as an EMT-B, not as intern in a clinical setting. It has been brought to our attention that some interns have been attempting to circumvent this regulation. It has been documented that interns working as an EMT-B, when presented with an opportunity to perform a skill, will clock out to perform the skill, and then clock back in. It has also occurred where a intern tells a paramedic on a call they “can do their skills at their service”. The phrase “while being employed as an EMT-B” includes both paid and volunteer EMT-B’s. This does not prohibit a department or service from paying a intern while in training. For example, a Fire Department continues to pay a intern while they are in clinicals. This is allowed only if the intern is in assigned clinicals and are not working in their capacity as an EMT-Basic for the their employer on a call or scheduled shift. The same policy also pertains to ambulance services, ALS or BLS EMRA’s, Fire Departments, or any other location that the EMT works for as an EMT, both paid and volunteer. This does not prohibit a intern from completing clinicals at their place of employment. There needs to be a clear distinction between intern and employee status. The purpose of clinicals is to provide an environment for a intern to learn. They are present not as a member of the service or the crew, but as a intern of the training entity, observing and performing skills under the supervision of a preceptor. The preceptor is there to teach and observe and if necessary, step in and take over for the intern if there is a problem. During clinicals each person, the intern and preceptor, have different roles than if they were a Paramedic and EMT on shift. While in clinicals at an ambulance service there is also a third person present, licensed at a minimum, as an EMT-B or EMT-P as required by law. It is the responsibility of training entities, and licensed ambulance services that are approved clinical sites to inform their interns of the statutes and regulations regarding EMS. Recently there has been licensure action taken against both preceptors and interns. Activity like this could lead to disciplinary action against the intern, the training entity, the preceptor, crewmembers and the service that allowed this activity to take place. Clear written policies must be given to each intern, preferably the intern should sign a receipt upon receiving the policies. These same policies should be distributed to clinical sites and preceptors. Before an EMT-Basic can perform ALS skills, the following components must have been fulfilled:
The intern is in an accredited Paramedic program; they have been trained in the skills to be accomplished; are approved by the training entity to enter into the clinical phase. The clinicals must be pre-arranged and approved by the training entity. The clinicals must be at a location where there is an agreement already in place and signed by both the training entity and the service or clinical site. The preceptor must be approved by the training entity. The Intern is currently licensed as an EMT-B by Missouri DHSS/EMS
In the past it has been said that the Unit of EMS prohibits clinicals at night. This is incorrect. In the regulation it states “Interns shall be assigned in clinical settings where experiences are clinically and educationally effective in achieving the program’s objectives”. If a service and a training entity mutually agree that clinicals can be done during the night, they must have provisions in place for this to occur, such as addressing the scenario of clinical hours while sleeping. If a person is sleeping, it only makes sense that this cannot be counted towards hours performed. There are many operational differences with night work as well as physiological and psychological changes in both patients and crews. This must be investigated thoroughly and as stated earlier, mutually agreed upon.
Ver. 11-2015 19
Documentation The documentation completed by the preceptor is one of the most important tools the program has to guide interns in helping them improve their performance and in creating a repeat intern contract.
Documentation should be completed daily, throughout, and at the end of each shift. Out of fairness to the intern, it is not appropriate to leave evaluations not completed. Interns need to be able to review in writing what was done well and what needed to improve on calls. A good approach is to plan time prior to the end of the shift to sit and review the evaluation points with the intern, and come to consensus on the evaluation and its contents. Documentation should include the what, when, how and why method, so interns have a clear picture of the steps they need to take to correct any problem(s). Interns are required to document some details of their shifts in an online database, and the program requires the intern to have this information uploaded within 24 hours of the end of the shift. Where internet access is available, or the intern has a mobile computing device, the interns should be encouraged to keep this documentation current.
WARNING!! DO NOT sign evaluation forms prior to the end of the shift, and never sign a blank evaluation form for an intern. If an intern needs to re-create an evaluation for a shift, they should enter all of the pertinent information for that shift prior to the preceptor signing the form. The preceptor should verify that the intern was actually at the site on the dates and times listed, and that the logged calls did occur at that time.
Verbal communication and written documentation should match. For example, an intern should not hear the run went well and then see poor scores on the evaluation. If the intern performs in a competent manner on a call, or on portions of a call, they should receive a competent score. This does not mean that their performance will be the same on every subsequent call.
Ver. 11-2015 20
Criteria for Evaluating Intern Performance
Field Evaluation Form In the early stages of learning, performance can be inconsistent. It is impossible to predict when the student will begin to show consistent achievement so it is imperative that each attempt be evaluated and documented. Since competency must be documented and tracked over multiple attempts, monitoring student performance, achievement of set goals and the response to your coaching is essential.
This daily formative evaluation has been simplified to provide a streamlined single-sheet-of- paper method of documentation. You are encouraged to document additional notes and attach additional documentation if necessary.
Directions on how to complete the evaluation form (instrument):
Each contact must be documented and rated by the student first. Students should mark their self-evaluation ratings in row “S.” You should document your rating of the student in row “P.” You should continue to document all shaded sections after the student has completed all of the sections required. Please comment on any discrepancies at the end of the row or on the back of the form. If you have concerns that you do not want to discuss with the student or write on the form, please check the box in the reverse of the form to be contacted and leave a method of contact. You are also welcome to contact the Clinical Coordinator or Program Director directly by phone or email.
Student Name: Name of student
Date: Date the field shift began
Educational Program: Name of the paramedic program the student is attending
Clinical Site: Name of the ambulance service or other clinical site
Page ___of___: If additional forms are necessary due to additional contacts, document the total number of additional forms.
TIME IN and OUT: Time of arrival and departure from clinical site
Preceptor: Name of preceptor
Unit or Station: Radio call sign or “report to work” location
Patient Age/Gender: Patient's age and gender
Impression and/or Differential Diagnosis: A list of the possible diagnoses for patient
LOC/Complaints/Event/Circumstances: Level of consciousness, the stated complaint or the observed condition of the patient.
Summary of Treatments: The student lists any psychomotor skills performed successfully.
Ver. 11-2015 21
Ratings:
2 = Successful/Competent – no prompting necessary. The student performed at the entry-level of competency as judged by the preceptor. Entry-level of competency takes into account the amount of education the Paramedic student has undergone at the time of the clinical interface with the patient.
0 = Unsuccessful – required excessive or critical prompting; this includes “Not attempted” when student was expected to try; this is an unsatisfactory rating.
1 = Marginal – inconsistent, not yet competent; this includes partial attempts.
NA = Not Applicable – not needed or expected; this is a neutral rating. (Example: Student expected to only observe, or the patient did not need intervention).
*NOTE: Ideally, students will progress their role from observation to participation in simple skills, to more complex assessments and formulating treatment plans. Students will progress at different rates and case difficulty will vary. Students should be active and ATTEMPT to perform skills and assess/treat patients early even if this results in frequent prompting and unsuccessful ratings. Unsuccessful ratings are normal and are expected in the early stages of the clinical learning process when student needs prompting. Consistent successful ratings in the early stages of the clinical and field experience cast doubt on the reliability of the overall evaluation. Improvement plans MUST follow any unsuccessful or inconsistent ratings.
All interns must be evaluated equally and against the set standard!
ALS Field Leads To qualify for an ALS call, two ALS interventions must be attempted (by someone on the crew). A simple IV start or cardiac monitoring does not constitute an ALS call, yet both together do constitute an ALS call. Likewise, an albuterol treatment and cardiac monitoring would also constitute an ALS call. If a patient presents with a critical condition, and ALS would have been carried out but was not due to extenuating circumstances or proximity to a hospital (i.e. scene safety, multiple trauma), then the preceptor may count that as an ALS call at their discretion. ALS transfers also qualify if two or more ALS procedures are carried out (i.e. IV maintenance, med drip monitoring, and cardiac monitoring). An IV attempt should never be performed simply to add to the total number of ALS calls. ALS should only be initiated if it is in the best interest of the patient.
Patient Information should include an age, sex and chief complaint. Treatment rendered should include all treatment given the patient.
Plan for improvement must include the specific things the intern and / or preceptor will do to improve the intern’s performance. This is an informal improvement plan and should be clear and concise in outlining what is to be done and when it will be evaluated again.
The form below is carried by Paramedic interns and should be completed for each ALS field lead. The preceptor must verify the information in order for the intern to receive credit for the lead.
YES NO I. SECTION I TO BE COMPLETED BY THE PARAMEDIC INTERN #1 I handled this call from start to finish. (If YES, go to #2, If NO – NOT a field lead) #2 This patient had indications for two or more ALS interventions. (If YES, go to #3, if
NO – NOT a field lead) #3 The ALS interventions were: (Check all that apply and go to #4)
[ ] Vascular Access – IV or IO [ ] Advanced Airway (ETI, King/LMA, Cric) [ ] CPAP or Mechanical Ventilation [ ] IV Medication Push [ ] IM, SQ, SL, or IN Medication Administration [ ] Nebulized Medication Administration [ ] Medicated IV Drip [ ] 12-Lead ECG and Interpretation
#4 The above checked interventions were attempted by myself or another provider at my request. (If YES, go to #6, if NO go to #5)
#5 The interventions were not attempted or completed for the following reason: #6 The above checked interventions were performed successfully. (If YES, go to Section
II, if NO go to #7) #7 Which interventions were unsuccessful and why. (i.e. three IV attempts by myself and medic were not successful, patient had allergy to medication, multiple providers could not visualize airway, proximity to hospital, etc.): SECTION II – TO BE COMPLETED BY PRECEPTOR The student led this call from start to finish. The intern required [ ]NO [ ]MINIMAL [ ]SOME [ ]MUCH assistance from me. I concur with the information above Signed:
Printed Name:
Note to Intern: 1. Attach this completed form to your Field Evaluation Form and submit it to the Clinical Coordinator with your paperwork. 2. Enter your Field Lead: ALS in Platinum. 3. You will be notified if the field lead is rejected for any reason.
Ver. 11-2015 23
Platinum Planner Each intern will report their skills data to Platinum Planner (www.platinumplanner.com).
The information is to be completed within 24 hours of the shift and the information will be reviewed at all meetings with the Clinical Coordinator. Failure to complete the forms correctly and completely will result in the intern losing credit for the clinical experience.
The intern will enter a preceptor along with the data for the shift. In participating departments, after the report is submitted for grading by the Clinical Coordinator, an email will be sent to the preceptor. The preceptor is asked to click on the link to review the intern’s entered information and complete a brief evaluation of the intern electronically. This serves as a validation process for the intern’s hard copy paperwork and assists the program with data management.
The full instructions to the Platinum Planner site are provided in the Appendix.
Ver. 11-2015 24
INTERN NAME: DATE: PROGRAM: UMKC SCHOOL OF MEDICINE
FIELD SITE:
Page _____ of ______
TIME IN: OUT: PRECEPTOR: UNIT/STATION:
DIRECTIONS: Each contact must be rated by the intern FIRST, and rated by the preceptor SECOND. Mark intern ratings in the row marked “S” and preceptors in row “P”. Comment on any discrepancies on back. Preceptors complete shaded sections.
RATINGS: NA – Not applicable, not needed or expected. 0 = Unsuccessful – required excessive or critical prompting. Includes rating of not attempted when the intern was expected to try. 1 = Marginal – inconsistent, not yet competent. 2 – Successful/Competent – no prompting required.
Patient Age Gender
Impression and/or Differential Diagnosis
LOC, Complaints, Events/Circumstances
Summary of Treatments Rendered Successfully by Intern
Circle Patient Type
RATE
R
CLINICAL OBJECTIVES
Lead
ersh
ip
Prec
epto
r In
itial
s
Comments and Immediate Plan for Improvement for Next Contact
Pt In
terv
iew
Phys
Exa
m
Impr
essio
n
Skill
Per
f.
Com
ms.
Prof
. Beh
av.
ALS BLS
S
P
ALS BLS
S
P
ALS BLS
S
P
ALS BLS
S
P
ALS BLS
S
P
ALS BLS
S
P
ALS BLS
S
P
ALS BLS
S
P
ALS BLS
S
P
Ver. 11-2015 26
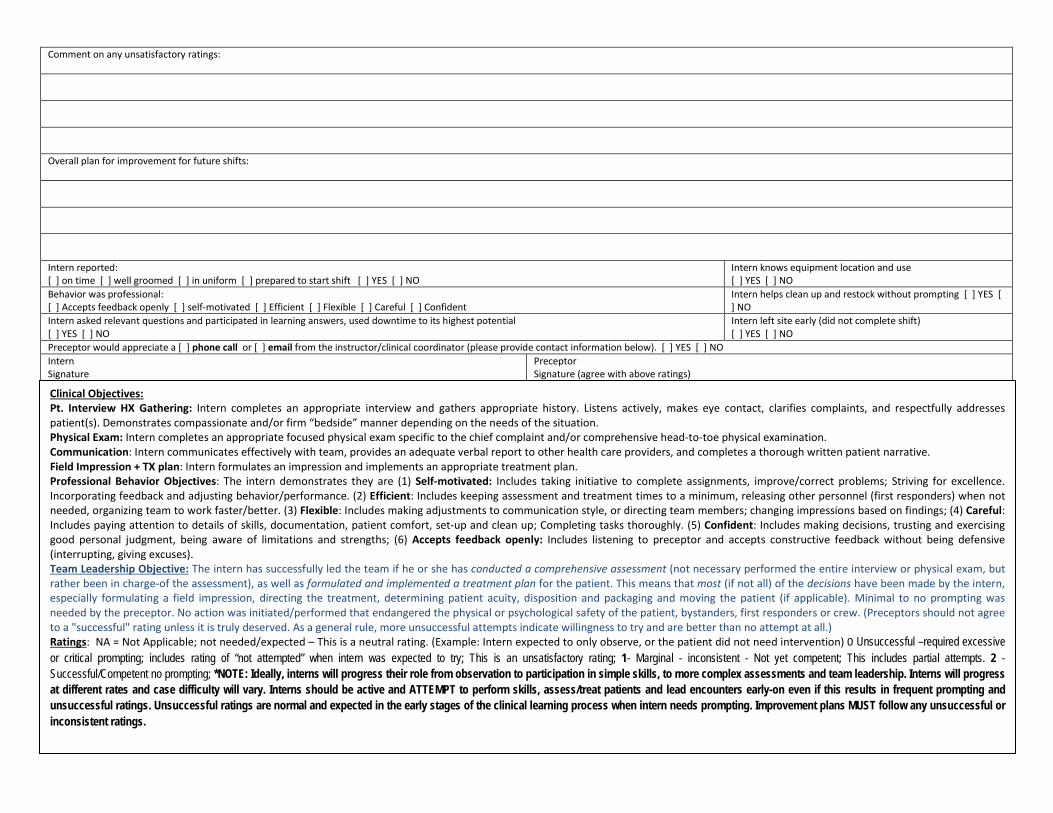
Comment on any unsatisfactory ratings: Overall plan for improvement for future shifts: Intern reported: [ ] on time [ ] well groomed [ ] in uniform [ ] prepared to start shift [ ] YES [ ] NO
Intern knows equipment location and use [ ] YES [ ] NO
Intern helps clean up and restock without prompting [ ] YES [ ] NO
Intern asked relevant questions and participated in learning answers, used downtime to its highest potential [ ] YES [ ] NO
Intern left site early (did not complete shift) [ ] YES [ ] NO
Preceptor would appreciate a [ ] phone call or [ ] email from the instructor/clinical coordinator (please provide contact information below). [ ] YES [ ] NO Intern Signature
Preceptor Signature (agree with above ratings)
Clinical Objectives: Pt. Interview HX Gathering: Intern completes an appropriate interview and gathers appropriate history. Listens actively, makes eye contact, clarifies complaints, and respectfully addresses patient(s). Demonstrates compassionate and/or firm “bedside” manner depending on the needs of the situation. Physical Exam: Intern completes an appropriate focused physical exam specific to the chief complaint and/or comprehensive head-to-toe physical examination. Communication: Intern communicates effectively with team, provides an adequate verbal report to other health care providers, and completes a thorough written patient narrative. Field Impression + TX plan: Intern formulates an impression and implements an appropriate treatment plan. Professional Behavior Objectives: The intern demonstrates they are (1) Self-motivated: Includes taking initiative to complete assignments, improve/correct problems; Striving for excellence. Incorporating feedback and adjusting behavior/performance. (2) Efficient: Includes keeping assessment and treatment times to a minimum, releasing other personnel (first responders) when not needed, organizing team to work faster/better. (3) Flexible: Includes making adjustments to communication style, or directing team members; changing impressions based on findings; (4) Careful: Includes paying attention to details of skills, documentation, patient comfort, set-up and clean up; Completing tasks thoroughly. (5) Confident: Includes making decisions, trusting and exercising good personal judgment, being aware of limitations and strengths; (6) Accepts feedback openly: Includes listening to preceptor and accepts constructive feedback without being defensive (interrupting, giving excuses). Team Leadership Objective: The intern has successfully led the team if he or she has conducted a comprehensive assessment (not necessary performed the entire interview or physical exam, but rather been in charge-of the assessment), as well as formulated and implemented a treatment plan for the patient. This means that most (if not all) of the decisions have been made by the intern, especially formulating a field impression, directing the treatment, determining patient acuity, disposition and packaging and moving the patient (if applicable). Minimal to no prompting was needed by the preceptor. No action was initiated/performed that endangered the physical or psychological safety of the patient, bystanders, first responders or crew. (Preceptors should not agree to a "successful" rating unless it is truly deserved. As a general rule, more unsuccessful attempts indicate willingness to try and are better than no attempt at all.) Ratings: NA = Not Applicable; not needed/expected – This is a neutral rating. (Example: Intern expected to only observe, or the patient did not need intervention) 0 Unsuccessful –required excessive or critical prompting; includes rating of “not attempted” when intern was expected to try; This is an unsatisfactory rating; 1- Marginal - inconsistent - Not yet competent; This includes partial attempts. 2 - Successful/Competent no prompting; *NOTE: Ideally, interns will progress their role from observation to participation in simple skills, to more complex assessments and team leadership. Interns will progress at different rates and case difficulty will vary. Interns should be active and ATTEMPT to perform skills, assess/treat patients and lead encounters early-on even if this results in frequent prompting and unsuccessful ratings. Unsuccessful ratings are normal and expected in the early stages of the clinical learning process when intern needs prompting. Improvement plans MUST follow any unsuccessful or inconsistent ratings.
Paramedic Student Required Checklists Paramedic interns in the UMKC program are taught to use certain checklists during their didactic and laboratory phases. Currently, the two mandatory checklists that the program requires are the Medication Administration Cross-Check (MACC) and the Airway Script for Endotracheal Intubation. While it is not the intent of the program to mandate or modify the operating procedures at field agencies, requiring paramedic interns to utilize these tool when they are doing the procedure will not only enhance their learning and reliability in critical situations, but will increase patient safety.
Ver. 11-2015 28
Advanced Airway Script
“Gloves, Gown, Goggles” • Place head into head-tilt position • Measure and insert an oral airway • Using an E/C hand placement, properly position mask • Evaluate SpO2 • Quickly squeeze the BVM and count aloud:
seven-one thousand, breathe” • Ask partner to take over BVM and begin pre-oxygenation (not hyperventilation) • Set-up ETI equipment
o Correct size ETT o Stylet placed into ET o Syringe with 10cc MAX air into balloon to test, removing syringe during test o Re-set syringe onto ET o Correct size and type blade - Check bulb is tight and bright o ET CO2 Detector o EDD o Suction o Stethoscope o Commercial ET holder o C-Collar o Flex guide o Pulse OX
• Engage blade on handle “Please stop ventilations.”
• Hold your breath • Remove oral airway • Position the head properly • Place blade into mouth SLOWLY starting at right of mouth while sweeping to the left • Point handle at corner of room • Use suction and visualization techniques (ELM, BURP, Hook) as needed
Ver. 11-2015 29
• Visualize the vocal cords and say aloud, “I see the cords.”
• Place the tube 1cm beyond the cords and say aloud, “The tube is passing through the cords.”
• Remove the blade SLOWLY and close handle • Remove stylette SLOWLY while maintaining control of the ETT • Push in plunger of syringe and remove from pilot balloon • Ask partner to place EDD.
“The EDD indicates correct placement.” • Connect BVM, ventilate and verbalize,
“Equal chest rise.” • Auscultate first at epigastric and then bilaterally at mid axillary and lastly bilaterally at
mid clavicular region. “No air over the epigastrum and clear lung sounds bilaterally.”
“The ETCO2 monitor is showing _____”(color change or waveform). “The tube is ___cm at the teeth.”
• Assess for hypoxia during ET attempt – SpO2, heart rate • Secure ETT with commercial tube holder • Place C-Collar on patient • Assess need for suction and suction if needed
If patient begins to regain consciousness: • “I would have the suction equipment ready.” • “I would monitor the patient’s VS.” • Verbalize two possible medications you could administer to sedate the patient.
“I would administer (#) mg of (medication) (route)” If patient is unable to tolerate ETT:
• Oxygenate the patient for 30 sec (if time permits) • Suction the oropharynx • Tilt patient or backboard to side • Attach syringe and deflate cuff • Quickly withdraw the ETT.
“When the patient exhales.” • Reassess respiratory status • Provide high concentration O2