135
Dr Ahmed Esawy Emergency X RAY films Dr. Ahmed Esawy MBBS M.Sc MD
| Date post: | 05-Apr-2017 |
| Category: |
Health & Medicine |
| Upload: | ahmed-esawy |
| View: | 10 times |
| Download: | 7 times |

Dr Ahmed Esawy
Emergency X
RAY films
Dr. Ahmed Esawy
MBBS M.Sc MD

Dr Ahmed Esawy
Plain x- ray
Dr Ahmed Esawy

Dr Ahmed Esawy
• The Elements of a chest x-ray
(CXR)
• The Broncho-vascular markings in
the lung
• The borders of the heart
• The contours of the mediastinum
and pleural space
• The ribs and spine

Dr Ahmed Esawy
• The Elements of a chest x-ray (CXR)
• The Broncho-vascular markings in the lung
• The borders of the heart
• The contours of the mediastinum and pleural space
• The ribs and spine

Dr Ahmed Esawy
• The normal
structures that
account for the
mediastinal contours
seen on chest X-ray
are diagramed below

Dr Ahmed Esawy
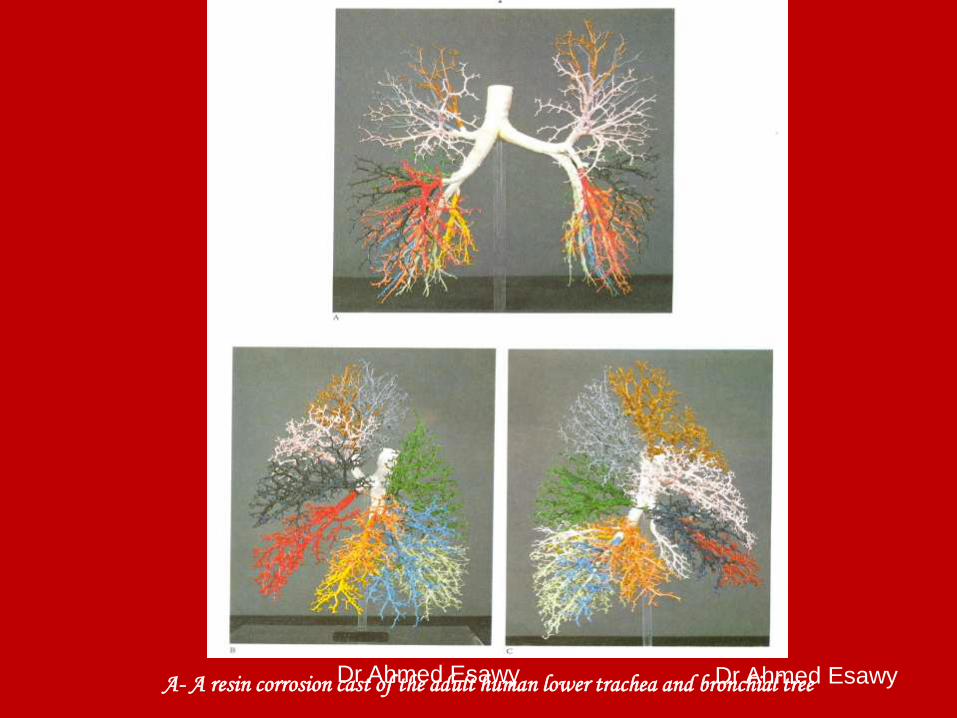
Dr Ahmed Esawy A- A resin corrosion cast of the adult human lower trachea and bronchial tree Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy
• This diagram shows
the appearance of a
bronchogram ( X-ray
dye in the bronchi)
and a schematic
identifying the
bronchial segments.
Note that on the frontal
view there is
considerable overlap
of segments.

Dr Ahmed Esawy
• The diagrams below
show the portion of
the mediastinum
associated with each
of the lobes.

Dr Ahmed Esawy
•ATELECTASIS,
LOBAR

Dr Ahmed Esawy
• COLLAPSE (ATELECTASIS)
• Collapse means partial or complete loss of
volume of a lung.
• Mechanisms of collapse (types):
• 1. Relaxation or passive collapse
• 2. Cicatrization collapse :
• 3. Adhesive collapse :
• 4. Resorption collapse (obstructive):
(causes : outside - inside - lumen)

Dr Ahmed Esawy
A. Direct signs (Lobar signs) of collapse
- Displacement of the interlobar fissures.
The most reliable sign.
• - Loss of aeration or increased density of
the collapsed area.
• - Vascular and bronchial signs

Dr Ahmed Esawy
B. Indirect signs (extra-labor):
• 1. Elevation of the hemidiaphragm:
especially in lower lobes collapse.
• 2. Mediastinal shift:
• 3. Hilar displacement:
• 4. Compensatory hyperinflation of
the normal parts of the lung:
• 5. Rib approximation.

Dr Ahmed Esawy
PATTERNS OF COLLAPSE
• A. Entire lung collapse “complete collapse”:
• B. Lobar collapse:
• C. Multilobar collapse :
• D. Atypical forms of collapse :
• 1. Rounded atalectasis or folded lung:
• 2. Fleischner’s plate atalectasis :

Dr Ahmed Esawy
• Lobar atelectasis.
Lingula collapses
medially.

Dr Ahmed Esawy
• Lobar atelectasis. Complete atelectasis of left lung.

Dr Ahmed Esawy
Lobar atelectasis. Left upper lobe collapses
superiorly and anteriorly.

Dr Ahmed Esawy
• Lobar atelectasis. Left upper lobe collapse. The radiograph shows opacity contiguous with the
aortic knob, a smaller left hemithorax, and a mediastinal shift. The luftsichel sign is
hyperextension of superior segment of the left lower lobe, which then occupies the left apex.

Dr Ahmed Esawy
• Lobar atelectasis. Left upper lobe collapse results in a veil-like opacity extending
upward and outward from the hilum. Additional signs of loss of volume in the left
hemithorax and crowding of the ribs are also evident on this radiograph.

Dr Ahmed Esawy
• Lobar atelectasis. Left upper lobe collapses anteriorly, as shown on
this lateral chest radiograph

Dr Ahmed Esawy
• Lobar atelectasis. Left lower lobe collapses
posteriorly and inferiorly.

Dr Ahmed Esawy
• Lobar atelectasis. Left lower lobe collapse. Radiograph shows volume loss
on left side, an elevated and silhouetted left diaphragm, and an opacity
behind the heart (sail sign).

Dr Ahmed Esawy
• Lobar atelectasis. Right upper lobe collapses posteriorly
and inferiorly.

Dr Ahmed Esawy
• Lobar atelectasis. Complete right lung atelectasis.

Dr Ahmed Esawy
• Lobar atelectasis. Right upper lobe collapse. Radiograph shows volume loss in the upper lobe, upward shifting of the horizontal fissure, and elevation of the right side of the diaphragm.

Dr Ahmed Esawy
• Lobar atelectasis. Left lower lobe collapse. The
opacity is in a posteroinferior location

Dr Ahmed Esawy
• Lobar atelectasis. As the right upper lobe collapses anteriorly and
superiorly, the opacity is seen in anterior and superior locations on this
lateral chest radiograph.

Dr Ahmed Esawy
• Lobar atelectasis. Right middle lobe collapses
medially

Dr Ahmed Esawy
• Lobar atelectasis. Right middle lobe collapse
obliterates the right heart border on a posteroanterior
(PA) image and projects as a wedge-shaped opacity
on a lateral chest radiograph

Dr Ahmed Esawy
• Lobar atelectasis. Right lower lobe collapses medially

Dr Ahmed Esawy
• Lobar atelectasis.
Right lower lobe
collapse results in
volume loss,
obliteration of the
right side of the
diaphragm, and a
posterior opacity on
this lateral chest
radiograph

Dr Ahmed Esawy
• Near drowning in a 46-year-old man. Anteroposterior chest
radiograph obtained in the intensive care unit shows diffuse,
bilateral pulmonary edema.

Dr Ahmed Esawy
• Anteroposterior chest radiograph shows interstitial and alveolar pulmonary edema
Pulmonary Edema, Noncardiogenic

Dr Ahmed Esawy
• Anteroposterior chest radiograph shows bilateral alveolar opacities in a patient with subarachnoid hemorrhage who developed neurogenic pulmonary edema
Pulmonary Edema, Noncardiogenic

Dr Ahmed Esawy
Pneumothorax

Dr Ahmed Esawy
• II. PNEUMOTHORAX
• Definition : Air within the pleural cavity due to defect in parietal or visceral pleura.
• Etiology :
• Spontaneous pneumothorax :
• 2. Traumatic pneumothorax
• Tension pneumothorax (valvular type):

Dr Ahmed Esawy
• A large right-sided pneumothorax has occurred
from a rupture of a subpleural bleb.

Dr Ahmed Esawy
• A true pneumothorax line. Note that the visceral
pleural line is observed clearly, with the absence of
vascular marking beyond the pleural line.

Dr Ahmed Esawy
• Note that although a skin fold can mimic subtle
pneumothorax, lung markings are visible
beyond the skin fold.

Dr Ahmed Esawy
• Deep sulcus sign in a supine patient in the ICU.
The pneumothorax is subpulmonic .

Dr Ahmed Esawy
• An older man admitted to ICU postoperatively. Note the right-sided pneumothorax induced by the incorrectly positioned small bowel feeding tube in the right-sided bronchial tree. Marked depression of the right hemidiaphragm is noted, and mediastinal shift is to the left side, suggestive of tension pneumothorax. The endotracheal tube is in a good position.

Dr Ahmed Esawy
• Right main stem intubation resulting in left-sided
tension pneumothorax, right mediastinal shift,
deep sulcus sign, and subpulmonic
pneumothorax

Dr Ahmed Esawy
• Pneumothorax Injury to the lung, either trauma or iatrogenic, frequently result in air leakage into the pleural space. Spontaneous cases (idiopathic) also occur. Severity and duration of pneumothorax is made worse by increased airway pressure, either by obstructive airway disease or positive pressure ventilation. If a "flap valve" mechanism is present, progressive enlargement of space may compromise cardiac filling and ventilation (tension pneumothorax).
• Below, a left pneumothorax with near complete collapse of the lung. Can you find the lung edge?

Dr Ahmed Esawy
• Below is a lateral view showing the middle lobe as a thin atelectatic band over the heart. Once air and blood volume are lost from atelectatic lung, the remaining structure is remarkably compact, and often hard to identify. In some cases, tracing the vessels to identify a missing segment is the only reliable way to detect complete atelectasis.

Dr Ahmed Esawy

Dr Ahmed Esawy
•Pneumomediastinum
•pneumopericardium

Dr Ahmed Esawy
• Pneumomediastinum
from barotrauma
may result in tension
pneumothorax and
obstructive shock.

Dr Ahmed Esawy
• patient in ICU developed pneumopericardium as
a manifestation of barotrauma .

Dr Ahmed Esawy
• Posteroanterior chest
radiograph demonstrates
a pneumomediastinum
in bronchial asthma.
Mediastinal air is noted
adjacent to the
anteroposterior window
and airtrapping extends
to the neck, especially
on the right side.

Dr Ahmed Esawy
• Lateral chest radiograph
demonstrates a
pneumomediastinum in
bronchial asthma. Air is
noted anterior to the
trachea.

Dr Ahmed Esawy
Esophagus,
Foreign Body

Dr Ahmed Esawy
• Esophagus, foreing body. Chest radiograph depicts deviation of the trachea to the right in an 18-month-old female infant with upper respiratory congestion lasting 3 months

Dr Ahmed Esawy
• Esophagus, foreign
body. Anteroposterior
radiograph of the neck
demonstrates tracheal
deviation to the right.

Dr Ahmed Esawy
• Esophagus, foreign body.
Anteroposterior chest
radiograph depicts a
penny at the thoracic inlet
of a 13-month-old infant
who refused to eat.

Dr Ahmed Esawy
• Esophagus, foreign
body. Radiograph in a
13-year-old girl who was
playing with jacks
recently.

Dr Ahmed Esawy
• Thorax trauma.
Supine chest
radiograph shows a
misplaced Ryle tube
in the left main
bronchus.
Dr Ahmed Esawy
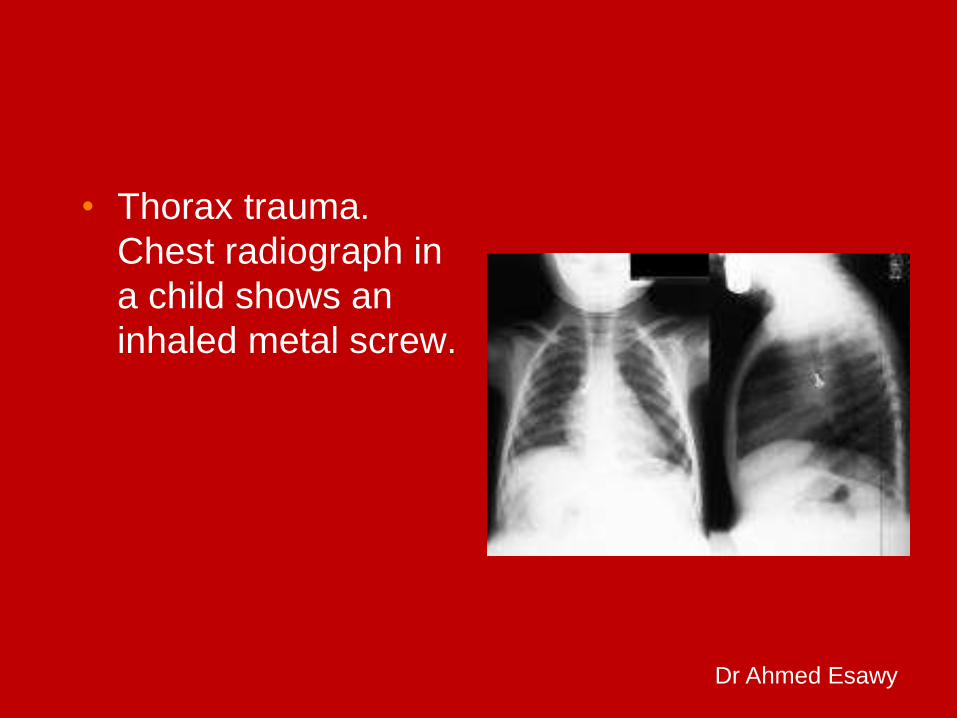
• Thorax trauma.
Chest radiograph in
a child shows an
inhaled metal screw.

Dr Ahmed Esawy

Dr Ahmed Esawy
The viscera

Dr Ahmed Esawy
Retro-peritoneal Structures,
outlined by fat.

Dr Ahmed Esawy
Intra-peritoneal Structures, that
may be outlined by fat

Dr Ahmed Esawy
Normal Gas 'lucency'

Dr Ahmed Esawy

Dr Ahmed Esawy
Complete Abdomen Erect
Looking for
Free air
Air-fluid levels
Substitute – left
lateral decubitus

Dr Ahmed Esawy
Complete Abdomen Erect Chest
Looking for
Free air
Pneumonia at bases
Pleural effusions
Substitute – supine
chest

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy
Normal Fluid Levels
Stomach
Always (except supine film)
Small Bowel
Two or three levels
possible
Large Bowel
None normally

Dr Ahmed Esawy

Dr Ahmed Esawy
Plain Radiographs
1. Bowel obstruction
Small & Large
2. Free intra-
peritoneal air
3. Intra-mural gas
Gas in Rectum &
sigmoid
Gas in few
bowel loops
Gas in
stomach
Normal supine Abdomen
Abnormal gas patterns
Dr Ahmed Esawy

Dr Ahmed Esawy
•Extra-luminal air
•Free intraperitoneal
air

Dr Ahmed Esawy
Free intra-peritoneal air
Perforated diverticulitis
Perforated carcinoma
Trauma
Intussusception
Post operative 5-7 days
Not perforated appendix
Plain Radiographs
Crescent sign:
air beneath
the diaphragm
Erect AP abdomen

Dr Ahmed Esawy
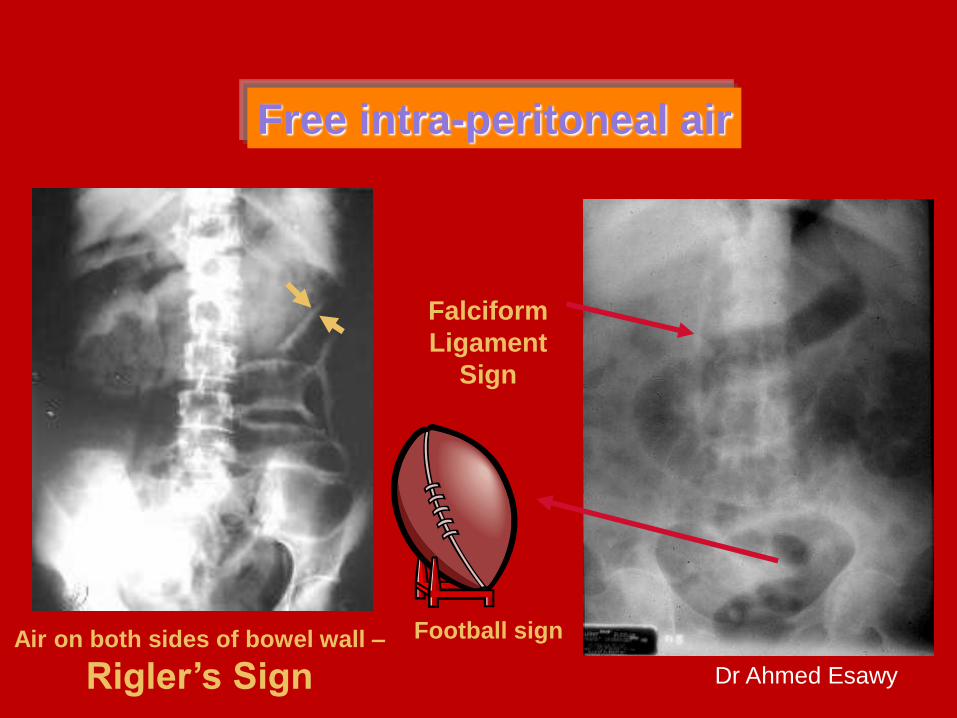
• a.Crescent sign :air beneath the diaphragm
• b.Falciform ligament sign: air delineating the falciform ligament
• c. Football sign: A large air collection beneath that does not conform to any bowel loop
• d.Rigler's sign: If both the serosal and the related mucosal walls of the bowel are delineated it means free air is at that serosal surface
Dr Ahmed Esawy
Falciform
Ligament
Sign
Football sign
Free intra-peritoneal air
Air on both sides of bowel wall –
Rigler’s Sign

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy
Algorithmic approach: Imaging of bowel wall lesions
Plain Radiographs
1. Bowel obstruction
Small & Large
2. Free intra-
peritoneal air
3. Intra-mural gas
Gas in Rectum &
sigmoid
Gas in few
bowel loops
Gas in
stomach
Normal supine Abdomen
Abnormal gas patterns
Dr Ahmed Esawy

Dr Ahmed Esawy
Dilated
Air-fluid levels
Plain Radiographs
Mechanical obstruction
Collapsed

Dr Ahmed Esawy
Bowel gas pattern
Large bowel
obstruction
Small bowel
obstruction
Peripheral Central
Few Multiple
Haustra incomplete Valvulae: complete lines
Diameter }5cm Diameter <5 cm
Dr Ahmed Esawy

Dr Ahmed Esawy
Large vs. Small Bowel
Large Bowel
Peripheral
Haustral markings don't
extend from wall to wall
Small Bowel
Central
Valvulae extend across lumen
Maximum diameter of 2"

Dr Ahmed Esawy
Air in L.
bowel
NO
Distended
loops
Localized
ileus
few
Generalized
ileus
multiple
Air in S.
bowel
LBO SBO
Decompressed
LBO
Air in the
rectum Yes

Dr Ahmed Esawy
LBO decompressed into SB
• in incompetent ileo-caecal valve, gas
in the large bowel may decompress
in the small bowel giving a small
bowel obstruction appearance

Dr Ahmed Esawy
Bowel obstruction
SBO LBO LBO decompressed
into SB
Supine AP
Plain Radiographs
Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy
Intra-mural gas
• pneumatosis coli: Air in the wall of
the bowel with linear areas. It can be
due to obstruction, infection,
ischemia, necrosis, or following
colonoscopy

Dr Ahmed Esawy
Diagnostic Value of plain
radiographs in bowel wall
lesions: • 1. Differentiation between
mechanical obstruction and paralytic
ileus.
2- . Differentiation between small
and large bowel obstruction
3-Diagnosis of perforated viscus

Dr Ahmed Esawy

Dr Ahmed Esawy
Esophagus
, Tear

Dr Ahmed Esawy
• Posteroanterior chest
radiograph shows a right-
sided
hydropneumothorax after
an esophageal rupture.

Dr Ahmed Esawy
Sternum,
Fractures
Dr Ahmed Esawy
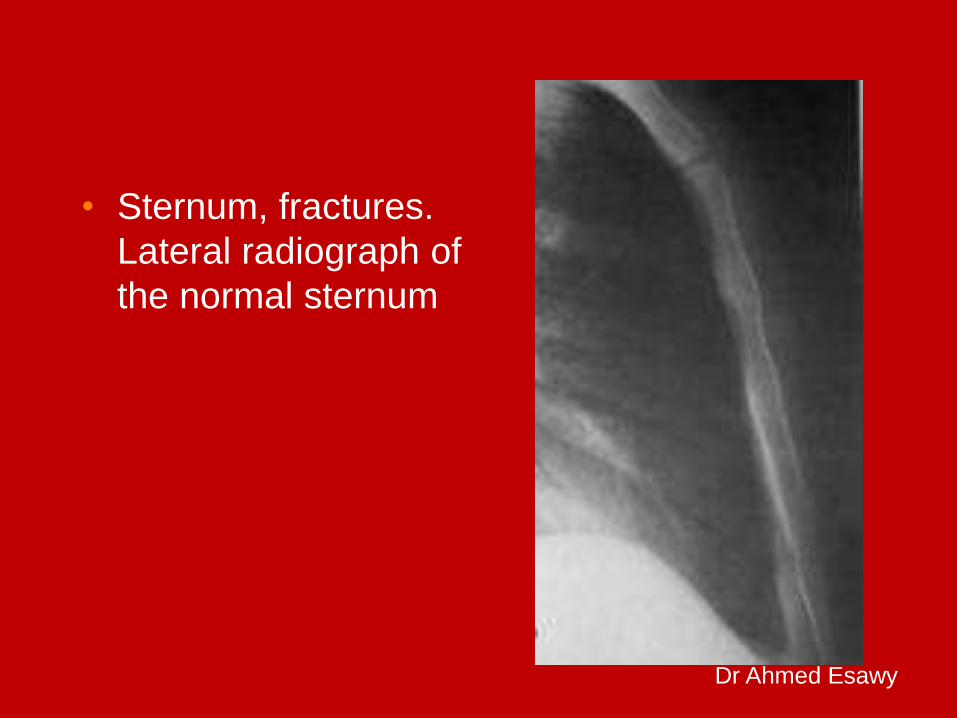
• Sternum, fractures.
Lateral radiograph of
the normal sternum

Dr Ahmed Esawy
• Sternum, fractures.
Posterior surface of
the sternum

Dr Ahmed Esawy
• Sternum, fractures.
Lateral border of the
sternum

Dr Ahmed Esawy
• Sternum, fractures.
Complete dislocation
at the sternal angle

Dr Ahmed Esawy
• Sternum, fractures.
Lateral radiograph in
the same patient as
in Image before
shows a complete
displaced fracture of
the sternum (arrow).

Dr Ahmed Esawy
Thorax
Trauma

Dr Ahmed Esawy
• Thorax trauma. Bilateral pneumothoraces in an infant with a deep costophrenic sulcus
sign, sharp demarcation of the cardiac border, double-diaphragm contour and
depression of left hemidiaphragm and hyperlucency in lower thorax and upper abdomen.

Dr Ahmed Esawy
• Thorax trauma. Left-sided
tension pneumothorax in
an infant.

Dr Ahmed Esawy
• Thorax trauma. 32-year-
old man with gunshot
wounds. Multiple lead
pellets are noted in the
pleura, adjacent to the
thoracic aorta, spleen,
and left kidney. Note the
hemothorax and splenic
laceration.

Dr Ahmed Esawy
• Thorax trauma. 32-year-
old man with gunshot
wounds. Multiple lead
pellets are noted in the
pleura, adjacent to the
thoracic aorta, spleen,
and left kidney. Note the
hemothorax and splenic
laceration.

Dr Ahmed Esawy
• Thorax trauma. Supine
chest radiograph in a
man who was stabbed.
The knife has been left in
the thorax. Note the
associated left
hemothorax and
pulmonary laceration.

Dr Ahmed Esawy
Rupture
daiphragm

Dr Ahmed Esawy
• Chest radiograph in a
patient with a recent
history of thoracic
trauma after a road-
traffic accident. No left
hemidiaphragmatic
dome can be identified.
An air-fluid level is
present at the left lung
base. At surgery, a left
diaphragmatic rupture
was repaired.

Dr Ahmed Esawy
• Scanogram obtained
before CT in a
patient involved in a
road-traffic accident
shows abdominal
visceral herniation
into the left
hemithorax

Dr Ahmed Esawy
• Chest radiograph in a patient
with a previous left phrenic
nerve injury shows an
elevated atrophic left
hemidiaphragm. Note the air-
filled stomach and bowel
loops under the diaphragm.
On fluoroscopy, paradoxical
movement was recorded.

















