40
Endocrine emergencies on the ward • Thyroid • Adrenal • Pituitary • Calcium • Sodium • Neuroendocrine May 2016
Endocrine emergencies on the ward
• Thyroid
• Adrenal
• Pituitary
• Calcium
• Sodium
• Neuroendocrine
May 2016

Hyperthyroid
“Thyroid storm”
Pre-existing hyperthyroidism of any aetiology: graves,
multinodular goitre, amiodarone therapy
Precipitated by
Stress, withdrawal of treatment, radioiodine treatment,
surgery, intercurrent infection, ketoacidosis, tyrosine
kinase inhibitors
Clinical diagnosis: blood tests only helpful to a point
May 2016

Hyperthyroid
Clinical assessment
History:
Fever, sweating
Dehydration
Tachycardia/heart failure
Delirium/psychosis
Headaches
End stage: “apathetic”
May 2016

Thyroid storm
Treatment:
Fluids
Antithyroid drugs (blocks synthesis)
Iodide (blocks release)
Beta-blockers (adrenergic effects)
Steroids (?inhibit T4 to T3 conversion)
Cholestyramine
?plasmaphoresis
May 2016
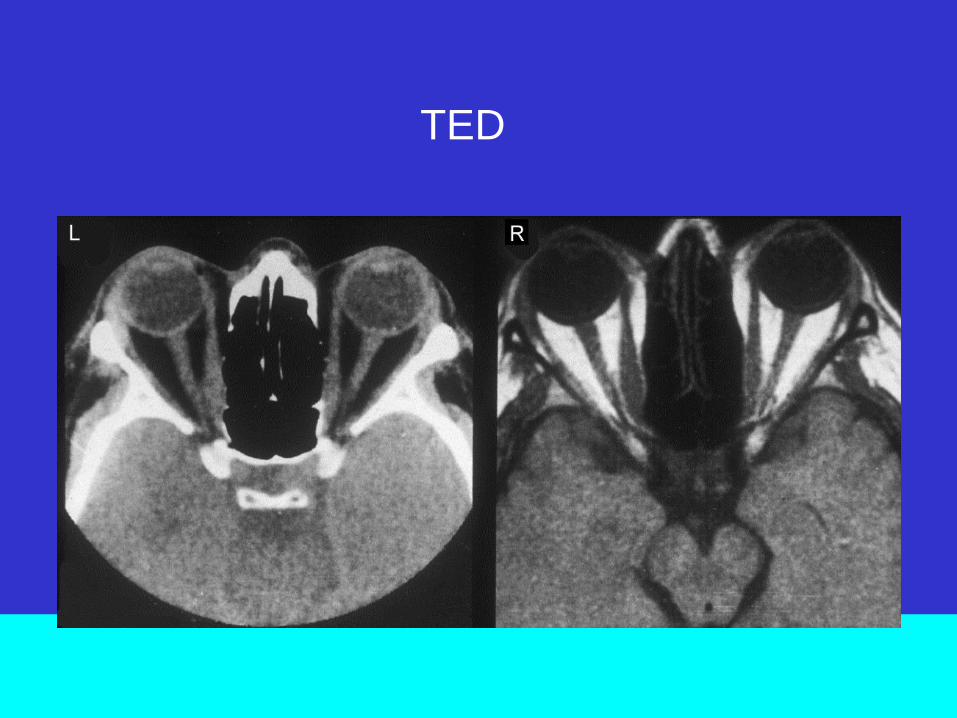
TED

Thyroid eye disease Smokers more at risk/Radioiodine may destabilize
Most patients stabilize or improve
Inflammation the main warning marker
Don’t MRI every case
Colour vision and vision testing may help
Treatment:
stabilize TFTs
anti-inflammatory
radiotherapy/surgery last resort
specialist clinic
May 2016


ECG

Hypothyroidism/myxoedema coma
Precipitating factors
Infection
Other systemic disorder (vascular/respiratory)
Hypothermia
Hypoglycaemia
Drugs eg lithium
Mortality c20% reflecting underlying pathology
May 2016
Hypothyroidism/myxoedema coma
Precipitating factors
Infection
Other systemic disorder (vascular/respiratory)
Hypothermia
Hypoglycaemia
Drugs
May 2016

Hypothyroidism/myxoedema coma
Altered mental status
Reduced thermogenesis – hypothermia –hypoxia
Reduced cardiac output – hypotension – shock
Water retention- hyponatraemia
Differential diagnosis
1) Hypopituitarism: Low T4, Low TSH
2) Sick euthyroid: Low T3 (high rT3), Low/normal T4,
normal TSH
3) Starvation: low T3, low T4, low TSH
May 2016

Myxoedema treatment
Supportive treatment
Fluids
Inotrope support
Steroids
Large loading doses (IV) thyroxine
T4 500ug follwoed by 100ug daily
or T3 50 ug iv followed by 10 10ug qds
Look for atypical history such as weight loss/anorexia
May 2016

Amiodarone and thyroiditis
Amiodarone can cause hyper- or hypothyroidism
Type 1: patients predisposed to thyroid disease
goitre
“hot” gland on isotope scan
treat as for autoimmune hyperthyroidism/thyroid storm
Thyroidectomy last resort
May 2016

Amiodarone and thyroiditis
Type 2: Genuine thyroiditis
Release of stored thyroxine
Antithyroid drugs won’t help
“cold” isotope scan
(interleukin 6 may be elevated)
Supportive and antinflammatory treatment
Antithyroid treatment no use
Thyroidectomy last resort
Try and arrange radioisotope scan before starting treatment
LITHIUM: can also cause hyperthyroidism
May 2016


Addison’s History: c100% anorexia and weight loss
Other clinical clues
Unexplained general ill health
(student life style)
Pyrexia
Nausea
Abdominal pain
Hypoglycaemia
Hyponatraemia/Hyperkalaemia/Hypercalcaemia
Hypotension
May 2016

Addison’s Aetiology
Autoimmune
TB
Malignancy metastasis
Iatrogenic:
enzyme inducers (eg retrovirals)
steroid inhibitors
Sepsis/DIC/Anticoagulant therapy
Compliance/withdrawal of treatment
May 2016
Addison’s Pathophysiology
Glucocorticoids:
dilutional hyponatraemia
hypercalcaemia (loss of one-alpha hydroxylase inhibition)
hypoglycaemia
Mineralcorticoids
Na and water loss
K retention
Dehydration
May 2016

Addison’s Treatment:
Fluids: saline, dextrose
Send off cortisol and give steroids: don’t wait for a
synacthen test
Steroids should precipitate a diuresis
Identify aetiology
Remember sick day rules
May 2016


Severe headache
76 year old female with a longstanding history of non-
functioning pituitary macroadenoma managed
conservatively
Admitted with 2-3 day severe headache, obtunded,
hypotensive and hyponatraemic, vomiting, diplopia/visula
symptoms
Diagnosis? Investigations? Treatment?
May 2016

.
Investigations:
Na 130, K 4.2
MRI scan

Severe headache Aetiology: infarction of preexisting adenoma; haemorrhage
Cause: impaired blood supply via pituitary stalk? Not clear –
may reflect local anatomy and impaction of stalk on
diaphragmatic notch (cf Sheehans)
Management:
Steroids, fluids, assess visual fields
Urgent scanning
Neurosurgical opinion: may need surgery (may not)
May 2016
Hypercalcaemia
71 year old woman
Admitted with confusion, nausea, dehydration
Ca 3.5 mmol/L, PO4 0.72, PTH low normal
Responded to fluids over 4 day period
No need for bisphosphonates
No evidence of underlying malignancy (bloods, scanning)
Gradual improvement
When seen 4 weeks later calcium remains normal
Possible cause?
May 2016

Hyponatraemia assessment How low? –definition <136 mmol/L
Fluid retention/dilutional hyponatraemia (hypotonic): risk of
cerebral oedema
Loss of water from cells to the extracellular fluid (non-
hypotonic) – shift of water from intracellular to
extracellular, risk of cellular dehydration
May 2016

Hyponatraemia assessment Hypotonic hyponatraemia:
An excess of water in relation to existing sodium stores
Either due to inability to excrete water
Or excessive water intake
May 2016

Causes of hypotonic hyponatraemia
Decreased volume extracellular fluid:
diuretics
osmotic diuretics (eg hyperglycaemia)
adrenal insufficiency
nephropathy (salt wasting)
sodium loss (eg sweating)
sequestration (eg pancreatitis)
May 2016

Causes of hypotonic hyponatraemia
Normal volume extracellular fluid
Hypothyroid
Adrenal insufficiency
SIADH
iatrogenic (eg desmopressin, antiepileptics)
Infection (eg pulmonary)
Diet (eg potomania)
May 2016
Causes of hypotonic hyponatraemia
Increased extracellular fluid
CCF
Nephrotic syndrome
Cirrhosis
Renal failure
Pregnancy
May 2016

Causes of hypotonic hyponatraemia
Excessive water intake
Primary polydipsia
Accidental water ingestion
Sodium free irrigants
Tap water enema
May 2016

Consequences of hyponatraemia
Central nervous system dysfunction
Exaggerated by large (eg <125 mmol/L) or rapid decrease
Water gain by brain leads to cerebral oedema
Rapid adaptation: loss of solutes to reduce cerebral oedema
Slow adaptation: loss of organic osmolytes
Rapid correction by any method including fluid deprivation
can lead to shrinkage of the brain leading to osmotic
demyelination (pontine myelinolysis but not just pons)
May 2016

Assessment of the patient How low? <120 mmol/L a warning
How symptomatic (may reflects rapidity of onset)?
Any obvious possible cause : drugs, disease (eg cancer),
lifestyle, surgery, parturition etc., iatrogenic (eg iv
dextrose)
Specifically exclude Hypothyroidism and Adrenal
insufficiency (?hyperkalaemia)
Fluid replete or deplete? Clinical assessment
?SIADH: urine sodium/osmolalaity
May 2016

Options for correction: relatively
asymptomatic
Euvolaemia: check plasma and urine osmolality
Plasma <275, urine >100
Check urine sodium: >20 mmol/L, likely SIADH
Commence fluid restriction eg 1 litre initially
Look for underlying cause
May 2016

Options for correction: relatively
asymptomatic
Hypovolaemic: replace fluids – isotonic saline
Hypervolaemic: treat underlying cause (eg cardiac failure,
cirrhosis)
May 2016

Severe symptomatic hyponatraemia .
*Hypertonic 3% saline can also be administered at 0.5–1 mL/kg/hour with frequent monitoring every 2–4 hours
CNS = central nervous system; GCS = Glasgow Coma Scale; IV = intravenous;
Acute symptomatic hyponatraemia • CNS disturbance • Confusion • Headache • Drowsiness • Coma / altered GCS • Seizures • Encephalopathic
Move to a Level 2 monitored environment
Administration of hypertonic 3% saline* 150 mL IV over 20 min
Repeat after 20 min if no clinical improvement
Recheck serum [Na+] at 6, 12, 24 and 48 h for overcorrection (no more than 10 mmol/L
in 24 h, 18 mmol/L in 48 h)
A 78 year old patient with
liver metastases
• An incidental finding during diaphragmatic hernia repair
• She is on large doses of bisphosphonates for breast cancer mets
• Liver biopsy histology shows features of neuroendocrine tumour
• CT scanning shows a large pancreatic tumour with local lymph nodes
• Post-operatively she develops diarrhoea, hypovolaemia, hypokalaemia
• ?diagnosis

A 78 year old woman with liver mets
(cont)
• Gut hormone screen shows an elevated level of
VIP
• How would you treat?
• How do we know this is not a gastrinoma? (can
also present with diarrhoea)

19year old student
• Has a minor gynaeocological operation
• Hypertensive crisis post-anaesthetic
• Heart failure: resuscitation and transfer to ICU
• Investigations reveal grossly elevated plasma metanephrines
• CT scan shows large pararenal mass 6 cm
• Likely diagnosis paraganglioma
• Responds to alpha blockade but hypotensive, hyperkalaemic, random cortisol <50 nmol/L
• ?explanation

The end

















