87
Endocrine Issues in Critical Endocrine Issues in Critical Illness Illness Illness Illness
| Date post: | 08-Sep-2018 |
| Category: |
Documents |
| Upload: | nguyenthien |
| View: | 217 times |
| Download: | 0 times |

Endocrine Issues in Critical Endocrine Issues in Critical IllnessIllnessIllnessIllness

ObjectivesObjectives
Be able to identify the following:Be able to identify the following:Stress responsePathophysiology of stress hyperglycemiaI d l ti ti f l d i liImmunomodulating properties of glucose and insulinCortisol physiology and biosynthesisHPA and the stress responseEvaluation of HPA in the critically illEvaluation of HPA in the critically illAdrenal physiology in sepsisSteroid replacement in sepsis
The Stress ResponseThe Stress Response
Bi l i h i l h l i t llBi l i h i l h l i t llBiologic, physical, or psychologic stressors generally Biologic, physical, or psychologic stressors generally precipitate similar response precipitate similar response ––“general adaptation syndrome”“general adaptation syndrome”g p yg p y
Selye H. A syndrome produced by diverse nocuous agents. Nature. 1936;138:32.

The Stress ResponseThe Stress Response
A i i f h h h l i i iActivation of the hypothalamic-pituitary (HPA) axis
Activation of the sympatho adrenalActivation of the sympatho-adrenal system
Activation of subset of vagal and sacralActivation of subset of vagal and sacral parasympathetic efferents to GUT

The Stress ResponseThe Stress Response
Activation of HPA axis• Cortisol
Epinephrine
Norepinephrine
Glucagong
Growth hormone
ProlactinProlactin

The Stress ResponseThe Stress Response
Cardiac output increasesp
Respiration increases
Blood flow directed to brain and skeletal muscleBlood flow directed to brain and skeletal muscle
Gluconeogenesis and catabolism• fuel for brain, heart, muscles
Endocrine programs of pleasure, growth, and reproduction shut down

Glucocorticoids and the Stress ResponseGlucocorticoids and the Stress Response
Increase blood glucose↑ hepatic gluconeogenesis↓ adipose tissue glucose uptake
Lipolysis - FFA release
Prototeolysis - AA release
Synthesis of catecholamines
Synthesis of adrenergic and angiotensin II receptors
Cardiac contractility
Vascular tone

Glucagon and Epinephrine Glucagon and Epinephrine MediatedMediated -- GluconeogenesisGluconeogenesisMediated Mediated -- GluconeogenesisGluconeogenesis

Glucagon and Epinephrine Glucagon and Epinephrine MediatedMediated -- GylcolysisGylcolysisMediated Mediated -- GylcolysisGylcolysis

Metabolic Consequence of the Stress Metabolic Consequence of the Stress ResponseResponseResponseResponse
Gluconeogenesis
Gylogenolysis
Proteolysis
LipolysisInsulin Resistance
HYPERGLYCEMIAHYPERGLYCEMIA

Critical illnessCritical illness--state characterized by a state characterized by a pathologically prolonged stress responsepathologically prolonged stress responsepathologically prolonged stress responsepathologically prolonged stress response

Acute StressAcute Stress--Open CholecystectomyOpen Cholecystectomy

The NeuroThe Neuro--endocrine Response to endocrine Response to Prolonged Critical IllnessProlonged Critical IllnessProlonged Critical IllnessProlonged Critical Illness
Van den Berghe G. J Clin End Metab.1998;83:1827.

The NeuroThe Neuro--endocrine Response to endocrine Response to Prolonged Critical IllnessProlonged Critical IllnessProlonged Critical IllnessProlonged Critical Illness
Nocturnal profileNocturnal profile
NormalAcute illnessChronic critical illnessChronic critical illness
Van den Berghe G. J Clin End Metab. 1998;83:1827.
Changes in the GH Axis During Critical Changes in the GH Axis During Critical IllnessIllnessIllnessIllness
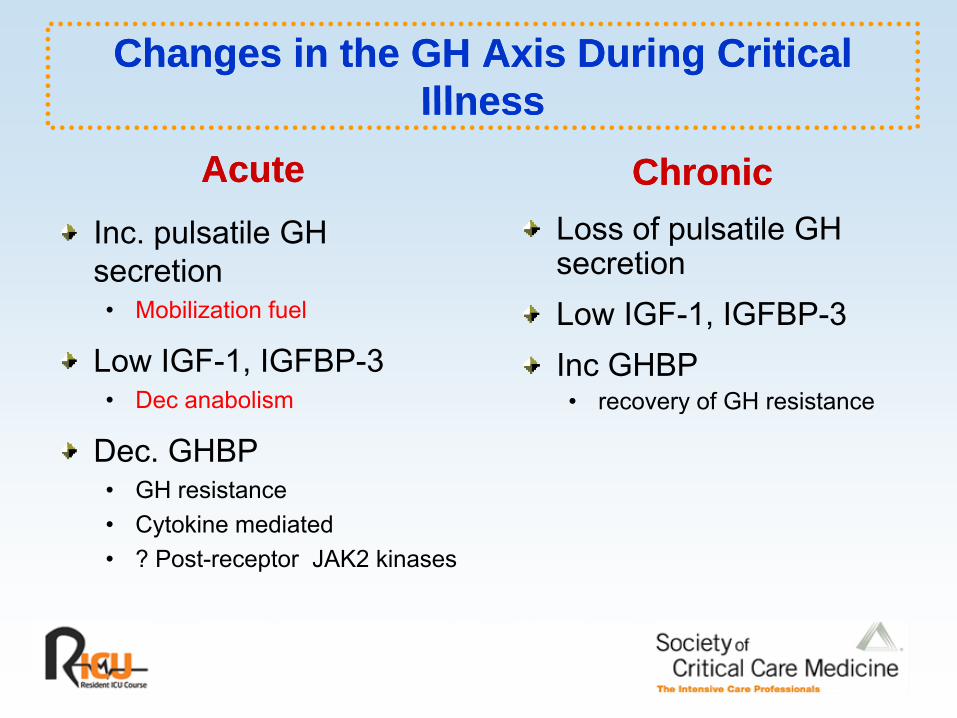
Acute Acute ChronicChronicLoss of pulsatile GH secretionL IGF 1 IGFBP 3
Inc. pulsatile GH secretion• Mobilization fuel Low IGF-1, IGFBP-3
Inc GHBP• recovery of GH resistance
• Mobilization fuel
Low IGF-1, IGFBP-3• Dec anabolism y
Dec. GHBP• GH resistance• Cytokine mediated• ? Post-receptor JAK2 kinases
Stress HyperglycemiaStress Hyperglycemia
D fi itiDefinition• Blood glucose > 200 mg/dl (15 - 20%)• Blood glucose > 110mg/dl (75 - 97%)
Etiology• Increased release of counter-regulatory hormones
- increased hepatic gluconeogenesis• Decreased insulin release• Insulin resistance

Insulin Mediated Glucose UptakeInsulin Mediated Glucose Uptake

Postulated Mechanism of Insulin Resistance Postulated Mechanism of Insulin Resistance in Sepsisin Sepsisin Sepsisin Sepsis

Hyperglycemia and InsulinHyperglycemia and Insulin
Pro-inflammatory Anti-inflammatoryGl I liGlucose Insulin
ROS, NADPH oxidase• Oxidative injury
TNF, IL-8,IL-6
ROS, NADPH oxidaseICAM-1, MCP-1TNF, IL-6
TF, PAI-1CATABOLIC
TF, PAI-1NO synthase
ANABOLIC
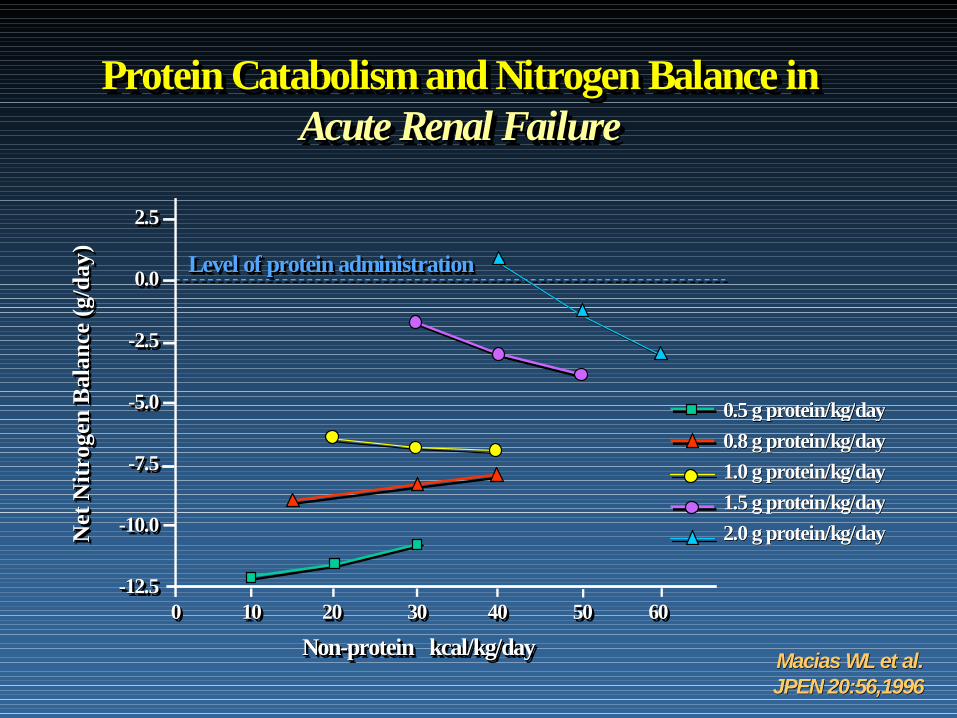
Protein Catabolism and Nitrogen Balance inProtein Catabolism and NitrogenProtein Catabolism and Nitrogen Balance inBalance ingAcute Renal FailureAcuteAcute RenalRenal FailureFailure
g/da
y)g/g/
day
day ))
2.5
0.0
2.52.5
0.00.0 Level of protein administrationLevelLevel ofof protein administrationprotein administration
Bal
ance
(gB
alan
ce (g
Bal
ance
(g
-2.5
-5.0
--2.52.5
--5.05.0 0 5 g0 5 g proteinprotein/kg//kg/dayday
tNitr
ogen
tt Nitr
ogen
Nitr
ogen
5.0
-7.5--7.57.5
0.5 g0.5 g proteinprotein/kg//kg/dayday0.8 g0.8 g proteinprotein/kg//kg/dayday1.0 g1.0 g proteinprotein/kg//kg/dayday1.5 g1.5 g proteinprotein/kg//kg/dayday
NetNet
Net -10.0
-12.5
--10.010.0
--12.512.50 10 20 30 40 50 600 10 20 30 400 10 20 30 40 50 6050 60
gg pp gg yy2.0 g2.0 g proteinprotein/kg//kg/dayday
Non-protein kcal/kg/dayNonNon--protein protein kcal/kg/kcal/kg/dayday0 10 20 30 40 50 600 10 20 30 40 0 10 20 30 40 50 6050 60
Macias WLMacias WL etet al.al.JPEN 20:56,1996JPEN 20:56,1996
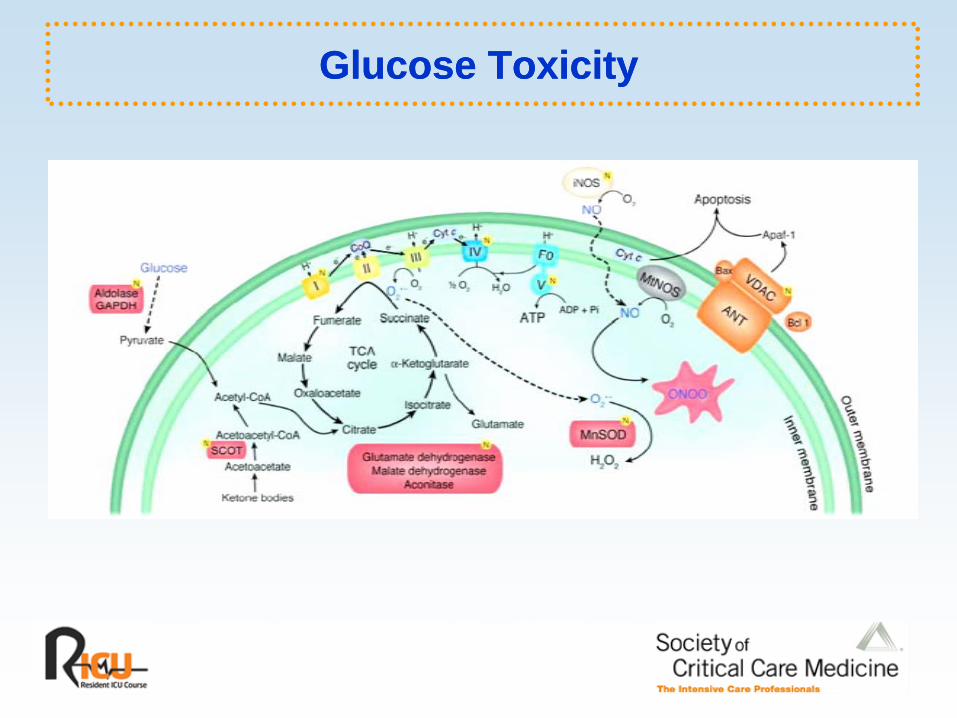
Glucose ToxicityGlucose Toxicity

Conventional - 78% abnormal Intensive - 1% abnormal
Hepatocyte
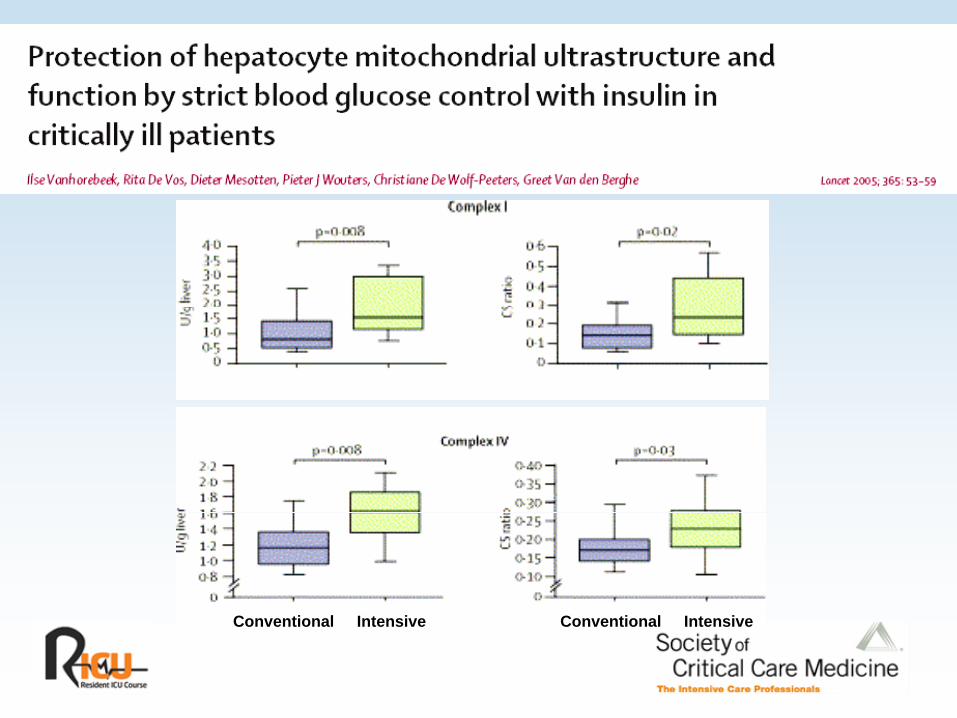
C CConventional Intensive Conventional Intensive

ROSROSICAM-1MCP-1PAI-1


>150 mg/dl
110 -150 mg/dl
< 110 mg/dl

Intensive Insulin TxIntensive Insulin Tx
• More recent studies have not confirmedMore recent studies have not confirmed NEJM findings
Keeping BS 80 110 may not have mortality– Keeping BS 80-110 may not have mortality benefit in all patients
– Keeping BS 80-110 is associated with highKeeping BS 80 110 is associated with high incidence of severe hypoglycemia (BS < 50)

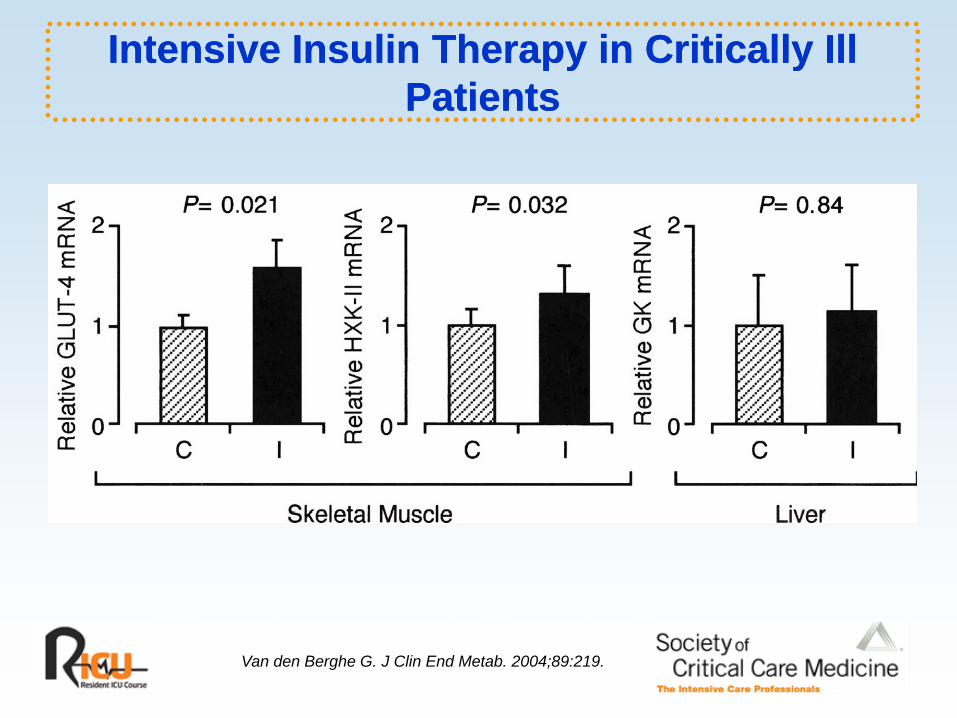
Intensive Insulin Therapy in Critically Ill Intensive Insulin Therapy in Critically Ill PatientsPatientsPatientsPatients

Intensive Insulin Therapy in Critically Ill Intensive Insulin Therapy in Critically Ill PatientsPatientsPatientsPatients
200g Dextrose

Intensive Insulin Therapy in Critically Ill Intensive Insulin Therapy in Critically Ill PatientsPatientsPatientsPatients
Intensive Insulin Therapy in Critically Ill Intensive Insulin Therapy in Critically Ill PatientsPatientsPatientsPatients
Van den Berghe G. J Clin End Metab. 2004;89:219.

Intensive Insulin Therapy in Critically Ill Intensive Insulin Therapy in Critically Ill PatientsPatientsPatientsPatients
Van den Berghe G. J Clin End Metab.2004;89:219.

Intensive Insulin Therapy in Critically Ill Intensive Insulin Therapy in Critically Ill PatientsPatientsPatientsPatients
Van den Berghe G. J Clin End Metab. 2004;89:219.
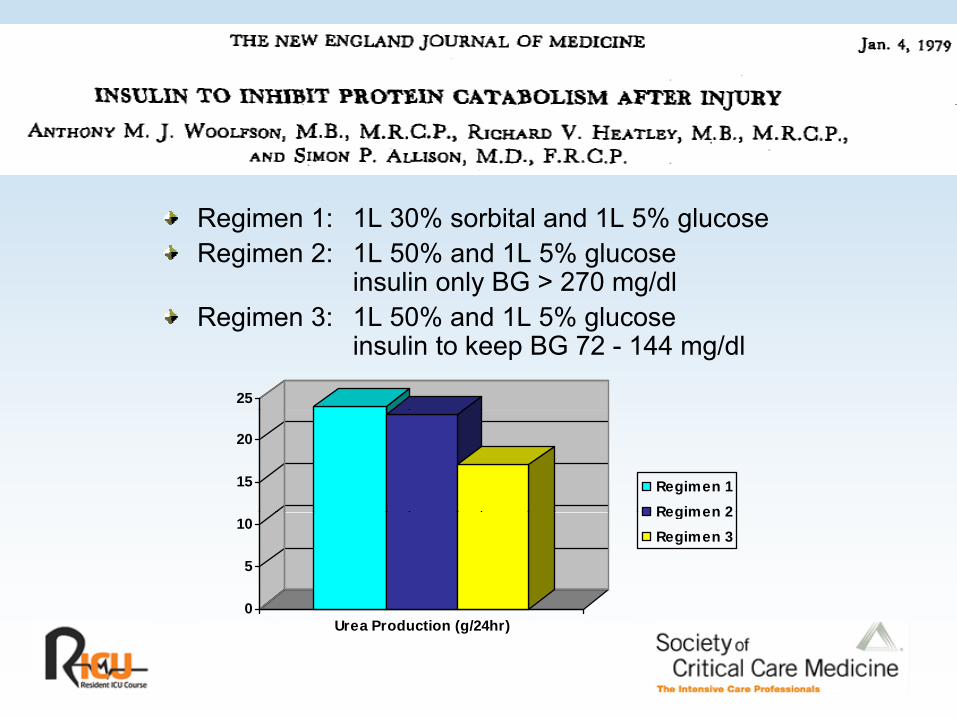
Regimen 1: 1L 30% sorbital and 1L 5% glucoseRegimen 2: 1L 50% and 1L 5% glucose
insulin only BG > 270 mg/dlR i 3 1L 50% d 1L 5% l
25
Regimen 3: 1L 50% and 1L 5% glucose insulin to keep BG 72 - 144 mg/dl
15
20
Regimen 1Regimen 2
0
5
10Regimen 2Regimen 3
Urea Production (g/24hr)

JPEN. 2002;26:271.

7Nitrogen gramsNitrogen grams
5
6
2
3
4 ControlInsulin
0
1
2
JPEN. 1994;18:214.

Hyperglycemia: TEN versus TPNHyperglycemia: TEN versus TPN
230Glucose mg/dl
Trauma meta-analysis
TEN (n = 92) versus TPN 170190210
( )(n = 102)
Similar ATI, ISS, BEE, 110130150
organ injuries
Goal: 0.2 - 0.25 g N/kg/d507090
110
50B MID END
TPN TEN
Moore FA, et al. Ann Surg. 1992;216:172.

Physiologic Effects of Enteral and Physiologic Effects of Enteral and Parenteral Feeding on PancreaticobiliaryParenteral Feeding on PancreaticobiliaryParenteral Feeding on Pancreaticobiliary Parenteral Feeding on Pancreaticobiliary
Secretion in HumansSecretion in Humans
Glucose Insulin
O’Keefe SJ, et al. Am J Physiol. 2003;284:G27.
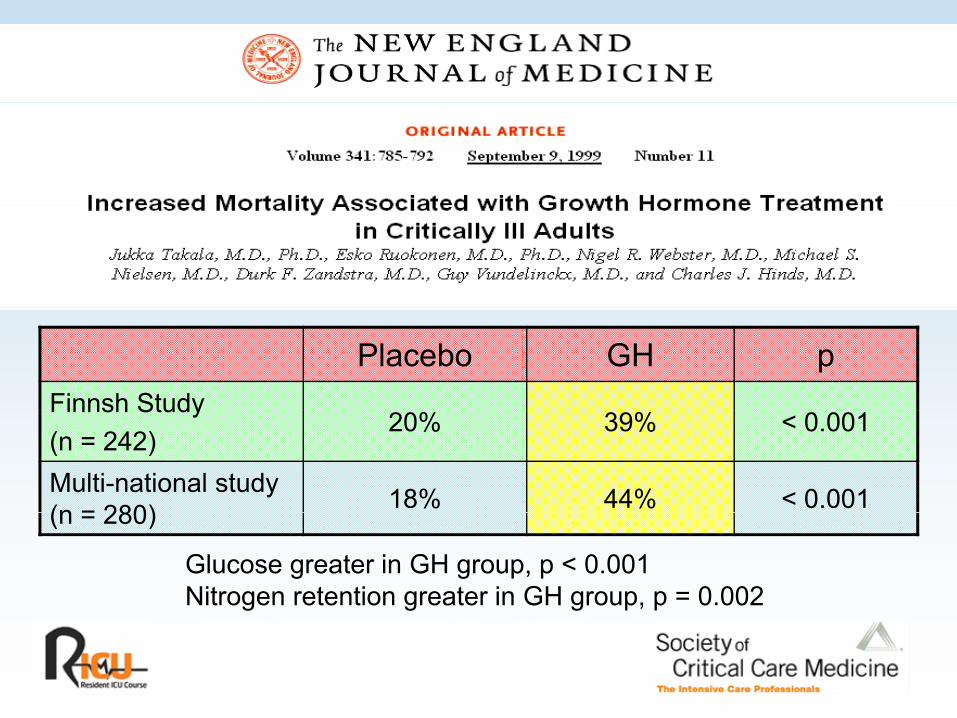
Placebo GH pFinnsh StudyFinnsh Study (n = 242)
20% 39% < 0.001
Multi-national study (n = 280) 18% 44% < 0.001(n = 280)
Glucose greater in GH group, p < 0.001 Nitrogen retention greater in GH group, p = 0.002

Glucose Control in the ICUGlucose Control in the ICU
THE GOOD THE BADGlycemic control• BS < 110-150• Insulin?
High glucose load
High caloric intakeInsulin?
Early enteral nutritionSlowly absorbed CHO
Poor glycemic control
Rapidly absorbed CHOSlowly absorbed CHOPermissive underfeeding
p y
GH
TPNunderfeedingOmega 3 FA
TPN
Low omega 3FA

Adrenal Insufficiency in the Adrenal Insufficiency in the Critically IllCritically IllCritically IllCritically Ill

CortisolCortisol

The HypothalamicThe Hypothalamic--PituitaryPituitary--Adrenal AxisAdrenal Axis
HypothalamusSTRESS
CRH
Hypothalamus
CRH
Pituitary
ACTHCortisol
ACTH
Adrenal

GREGRE

Steroid Hormone Receptor TraffickingSteroid Hormone Receptor TraffickingThrough the Nuclear CompartmentThrough the Nuclear CompartmentThrough the Nuclear CompartmentThrough the Nuclear Compartment
HSP90FKBP51FKBP52Dynein
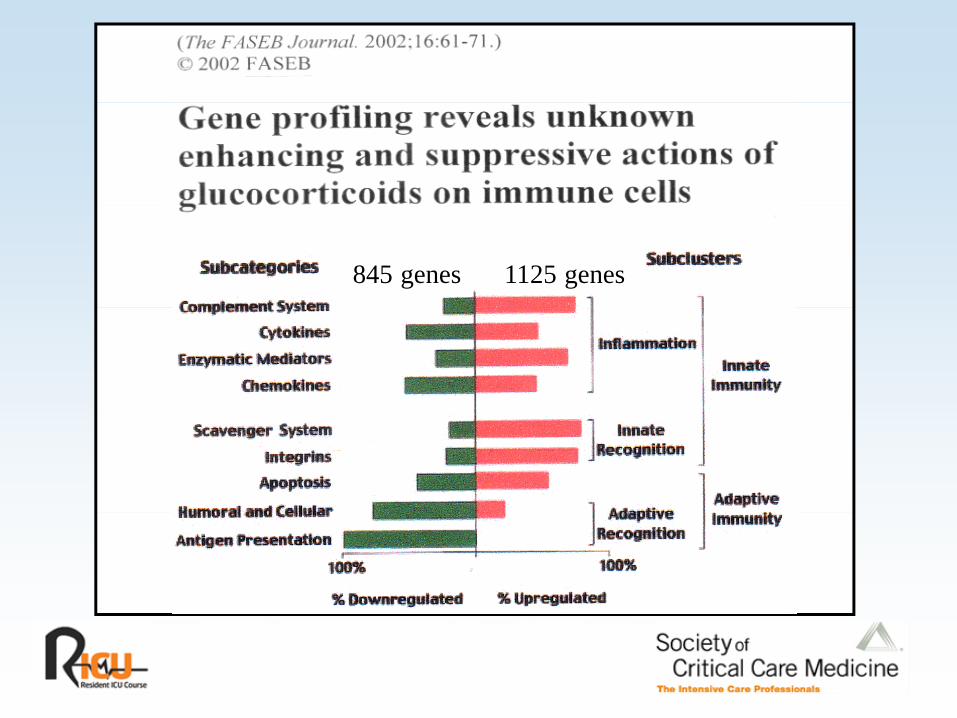
845 genes 1125 genes

Synthesis of CortisolSynthesis of Cortisol
80% exogenous20% endogenous

HDL as Substrate Cholesterol for HDL as Substrate Cholesterol for Steroidogenesis by Bovine Adrenal CellsSteroidogenesis by Bovine Adrenal CellsSteroidogenesis by Bovine Adrenal CellsSteroidogenesis by Bovine Adrenal Cells
Life Sciences. 1998;62:1387.

Scavenger Receptor, Type B, Class 1Scavenger Receptor, Type B, Class 1

Cortisol SynthesisCortisol Synthesis

The NeuroThe Neuro--endocrine Response to endocrine Response to Prolonged Critical IllnessProlonged Critical IllnessProlonged Critical IllnessProlonged Critical Illness
J Clin End Met. 1995;80:1238.

Free Serum Cortisol During the PostFree Serum Cortisol During the Post--op op Period Determined by Mass SpectrometryPeriod Determined by Mass SpectrometryPeriod Determined by Mass SpectrometryPeriod Determined by Mass Spectrometry
25
15
20
10
15
0
5
0BL POD1 POD2 POD3 POD4
Total % free Free
Clin Chem Lab Med. 2003;41:146.

“Normal” Stress Response“Normal” Stress Response
ACTH > 40 pg/dlACTH > 40 pg/dlACTH 40 pg/dlACTH 40 pg/dlCortisol level > 20 ug/dlCortisol level > 20 ug/dlCBGCBG Free cortisol Glucocorticoid receptorGlucocorticoid receptor Androgen synthesis Aldosterone synthesisdoste o e sy t es s
Cortisol and the Stress ResponseCortisol and the Stress Response
S ti t dFight and flight response• Glucose – fuel• Hemodynamic reserve
Suppress activated defense mechanisms• Prevent tissue damage• Prevent excessive inflammation

Adrenalectomy and Survival Following Adrenalectomy and Survival Following HemorrhageHemorrhageHemorrhageHemorrhage
Endocrinology. 1990;127:766.
Evaluation of Adrenal FunctionEvaluation of Adrenal Function
“G ld St d d”“G ld St d d” St C ti lSt C ti l“Gold Standard” “Gold Standard” -- Stress CortisolStress CortisolWhen stress is not adequate: • Provocative testing• Provocative testing
- Insulin hypoglycemia, metyrapone test • CRH stimulation test • ACTH (corticotropin) stimulation test ( p )
- Standard - 250 ug- Low dose - 1 ug

Standard ACTH TestStandard ACTH Test
Baseline cortisol 250 ug cosyntropin1 hour level• 1 hour < 18 ug/dl (AI)• < 9 ug/dl - “Occult AI”< 9 ug/dl Occult AI
Annane - “Non responder”

Problems with Classic ACTH TestProblems with Classic ACTH Test
Bypasses the hypothalamus and pituitary• unphysiological compared to endogenous stressor
Produces supra-physiologic levels of ACTH • serum levels 1000 x1000 x maximal normal stress levels• serum levels 1000 x1000 x maximal normal stress levels
Cutoff of 18 mcg/dl based on response to ACTH in nonstressed patientsp
Severely stressed patients may not increase levels further.CORTICUS Trial suggests ACTH stimulation does not have predictive value in critical illness

Problems with Classic ACTH TestProblems with Classic ACTH Test
~ 50% of healthy volunteers and stressed patients ~ 50% of healthy volunteers and stressed patients without evidence of HPA disease will have awithout evidence of HPA disease will have a cortisol cortisol
< 9ug/dl. < 9ug/dl.

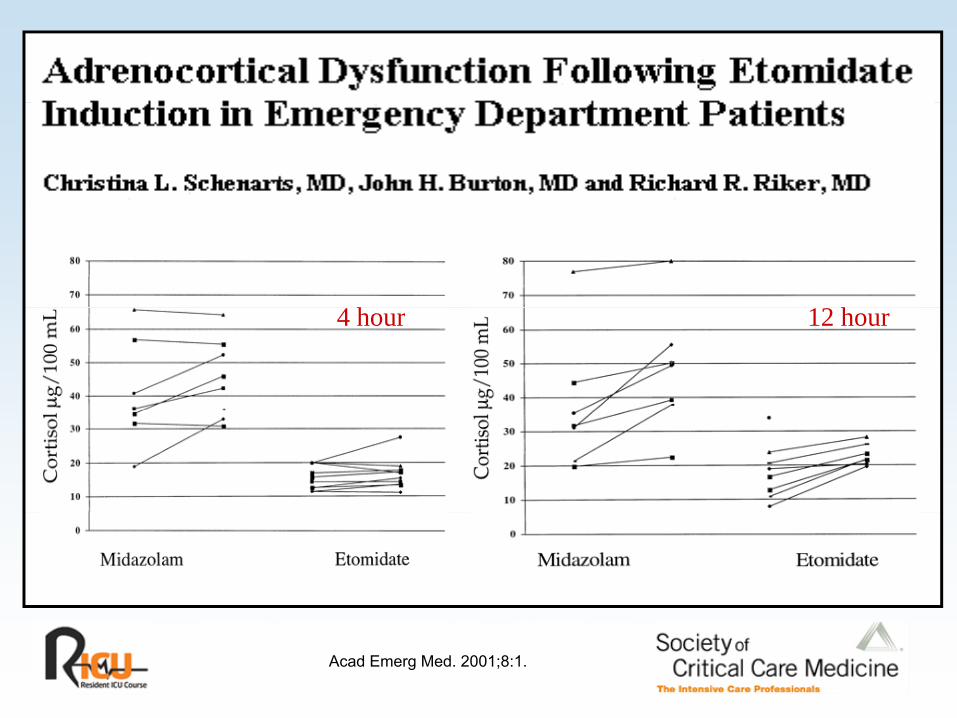
h h4 hour 12 hour
Acad Emerg Med. 2001;8:1.

LowLow--dose Corticotropin Testdose Corticotropin Test
TH
AC
T
J Clin End Metab. 1999;84:3648.

HD
18 ug/dl18 ug/dl
LD
J Clin End Metab. 1995;80:1243.
Diagnosis of HPA FailureDiagnosis of HPA FailureClinicalClinicalHighHigh--dose (250 ug) cosyntropin stimulation testdose (250 ug) cosyntropin stimulation testLow-dose (1ug) cosyntropin stimulation testUrinary cortisol (free)Random “stress” cortisol (total sRandom “stress” cortisol (total s--cortisol)cortisol)Salivary cortisol (free)Free cortisol indexFree cortisolIntraIntra--nuclear cortisolnuclear cortisolGene productGene product
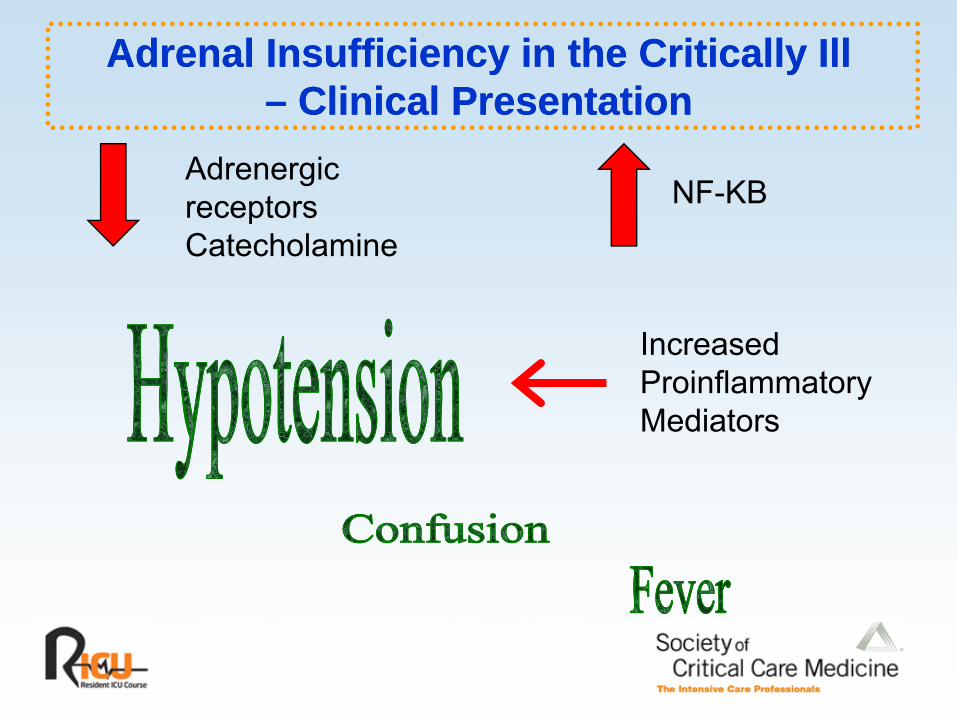
Adrenal Insufficiency in the Critically IllAdrenal Insufficiency in the Critically Ill–– Clinical PresentationClinical Presentation
Adrenergic receptors NF-KB
–– Clinical PresentationClinical Presentation
receptorsCatecholamine
Increased ProinflammatoryM di tMediators
Clinical Diagnosis of HPA FailureClinical Diagnosis of HPA Failure
HypotensionHypotensionHypotensionHypotension
Hemodynamic instabilityHemodynamic instability
Fever
Unexplained confusion
Eosinophilia
Hypoglycemia

Reversible Adrenal Insufficiency Reversible Adrenal Insufficiency of Sepsisof Sepsisof Sepsisof Sepsis

Sepsis and the HPA AxisSepsis and the HPA Axis
Decreased glucocorticoidreceptor synthesis and affinityy

TNF and Cortisol ProductionTNF and Cortisol Production
250Cortisol nmol/l
200
100
150
50
0BL ACTH ACTH + TNF
0.1ACTH TNF
1.0ACTH + TNF
10 ng/ml
Endocrinology. 1991;128:623.


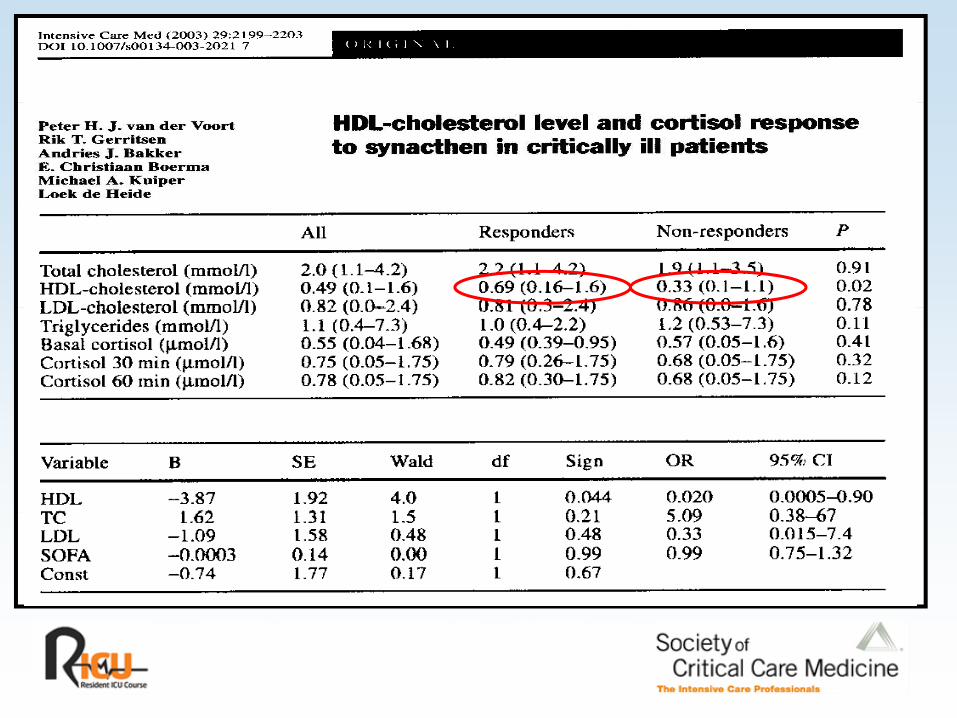
T Ch lT.Chol
LDL
HDL


9
6
7
8
4
5
6
ControlTNFIL-1
1
2
3IL 1IL-6
0
1
Cell Protein, mg Cell APO-A1ug/mg cell proteinug/mg cell protein
Arterioscler Thromb. 1994;14:8.

Cortisol Synthesis in SepsisCortisol Synthesis in SepsisTNF
Endotoxin
TNF

ACTH Response During Septic Shock and ACTH Response During Septic Shock and after Recovery (in patients with HPA failure)after Recovery (in patients with HPA failure)after Recovery (in patients with HPA failure)after Recovery (in patients with HPA failure)
13 of 20 patients BL < 25 mg/dl
30
35
tisol
mg/
dl 25
Cor
t
15
20
ShockRecovery
BL 60 min10
Intensive Care Med. 1996;22:894.

61% patients HPA61% patients HPA failure
Paul Marik & GaryZaloga

Hydrocortisone Infusion in Patients Hydrocortisone Infusion in Patients with Severe CAP: A RCTwith Severe CAP: A RCTwith Severe CAP: A RCTwith Severe CAP: A RCT
Hydron = 46 Placebo Hydro-cortisone P value
D MODS 16 ( 0%) 8 (3 %) 0 04Dev. MODS 16 (70%) 8 (35%) 0.04
Duration ventilation 10 4 0.007ventilation
Hosp LOS 21 13 0.03
Hosp Mortality 7 (30%) 0 0.009
AJRCCM. 2005;171:242.


Study DescriptionStudy Description
DesignR d i d d bl bli d l b t ll d t i l• Randomized, double-blind, placebo-controlled trial
• 19 ICUs France, 1995 - 1999
Population – Septic ShockPopulation Septic Shock• Focus of infection + HR >90/min + fever/hypothermia• SBP < 90 mm Hg for 1 hour despite fluid /pressors• Randomization within 8 hours shockRandomization within 8 hours shock
Treatment Arms• Randomization to hydrocortisone 50mg IV q 6 + 50 ug
fl d ti PO d t hi l bfludrocortisone PO qd or matching placebo
Study DescriptionStudy Description
Adrenal assessmentAdrenal assessment• 250 ug corticotropin test• Responders
increase cortisol > 9 ug/dl– increase cortisol > 9 ug/dl• Non-responders (occult adrenal insufficiency)
– increase cortisol < 9 ug/dl
E d i tEnd-points• 28-day mortality• Time to vasopressor withdrawal

Hydrocortisone Increases Survival in Hydrocortisone Increases Survival in Septic ShockSeptic Shock
30% RRR of death30% RRR of death100100
Septic ShockSeptic Shock
SurvivalSurvival (%)(%)8080
n = 299n = 299
6060 Treatment
2020
4040Placebo
00 77 1414 2121 282800
p = 0.0096
Time (days)Time (days)

CORTICUSCORTICUS
• Larger multinational EuropeanLarger, multinational, European• RCT design
Diff ith A• Differences with Annane– Did not include fludrocortisone– Enrolled patients up to 3 days following onset
of sepsis– Steroids dosed for 11 days with 6 day taper
NEJM 2008; 358 : 111-124

CORTICUSCORTICUS
• ACTH stimulation is not predictive ofACTH stimulation is not predictive of response to exogenous steroid
• Exogenous steroid administration has a• Exogenous steroid administration has a vasopressor sparing effectE t id d i i t ti d t• Exogenous steroid administration does not have mortality benefit
• Steroid group had higher incidence of infection and recurrent severe sepsis/shock
NEJM 2008; 358 : 111-124
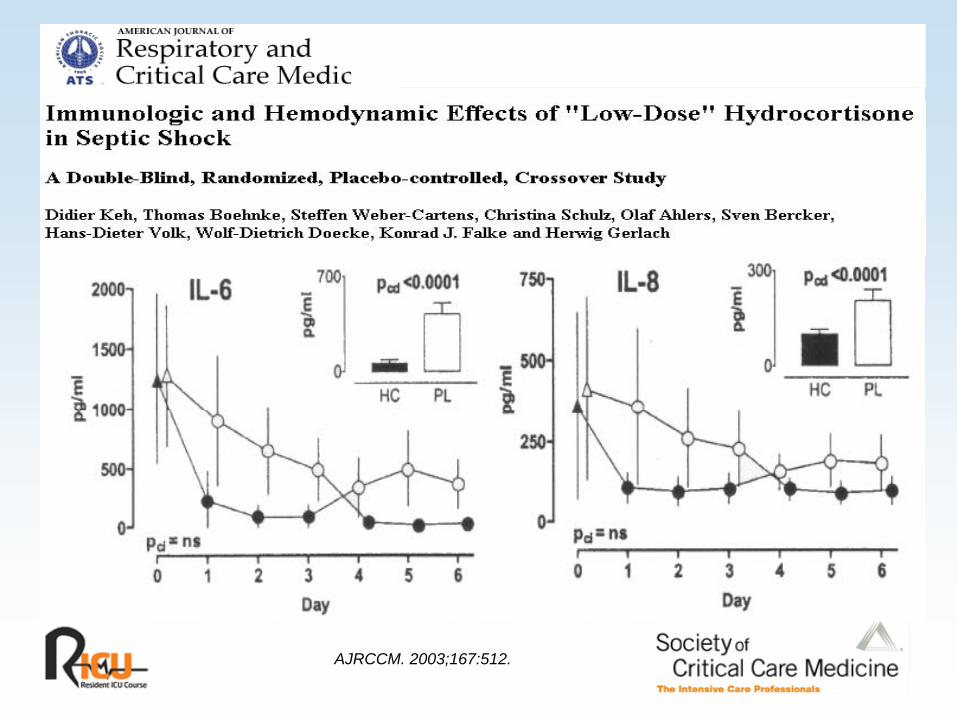
AJRCCM. 2003;167:512.


ConclusionsConclusions
Adrenal insufficiency (AI) common in ICU patients, i ll th ith iespecially those with sepsis.
Decreased synthesis of cortisol and release of ATCHDecreased synthesis of cortisol and release of ATCH mediated by cytokines, endotoxin, low HDL, etc.
Diagnosis of AI controversialDiagnosis of AI controversial
Role for treatment with replacement doses of phydrocortisone (50 - 100 mg q8) remains uncertain.

















