Endocrine neoplasms – searching for new forms of targeted therapy Alicja Hubalewska-Dydejczyk, Agata Jabrocka-Hybel, Aleksandra Gilis-Januszewska Jagiellonian University, Medical College, Department of Endocrinology 24 th of June, 2008, Krakow, Poland COST BM0607 Working Group Meeting
Transcript
Endocrine neoplasms – searching for new forms of targeted therapy
Alicja Hubalewska-Dydejczyk, Agata Jabrocka-Hybel, Aleksandra Gilis-Januszewska
Jagiellonian University, Medical College, Department of Endocrinology
24th of June, 2008, Krakow, Poland
COST BM0607 Working Group Meeting
99mTc-Octreotate99mTc-Octreotate90Y-DOTA TATE
VI 2005 X 2006
CgA – 47,1U/lCgA – 206,8U/l
Currently known targeted therapy in endocrinology
As a standard therapy:
131I therapy of differentiated carcinoma of thyroid gland
131I MIBG therapy as complementary and palliative therapy of malignant pheochromocytomas and NETs
Somatostatin analogues radiolabelled (90Y/177Lu-DOTATOC/DOTATATE) – in nonoperative or disseminated NETs
Currently known targeted therapy in endocrinology
In clinical trials:
Medullary carcinoma:
131I-MIBG (positive response in 35-40% cases)
90Y/177Lu-DOTATOC/DOTATATE
radiolabelled gastrin e.g. 131I (in experimental studies)
preliminary reports with 90Y-minigastrin
malignant pheochromocytoma, GEP-NET
radiolabelled VIP
radiolabelled ligands for glukagon like peptides’ (GLP-1) receptors – in malignant insulinoma treatment as well as in malignant pheochromocytomas and in brain npls
“Sensitizers” as possible improvement of targeted therapy
Retinoid acid (retinoids): up to one-third of metastasized or recurrent thyroid carcinomas may dedifferentiate over time, dediferentation is characterized by a loss of growth-regulating mechanisms mediated by TSH and/or a decline in iodine avidity. Various groups of “redifferentiating” agents such as retinoid acids were investigated in vivo studies
131 I-MIBG with topotecan as topoisomerase I inhibitor in malignant pheochromocytoma treatment
an inhibitor of DNA methylation or histone deacetylaseincreases the expression of natrium iodide symporter in tumor cells and also inhibits tumor growth – this inhibitor was found in in vitro studies
New possibilities of targeted therapy
Tyrosin kinase inhibitors RAF kinase inhibitors (serine/threonine protein kinases)
Inhibitors of RAS farnesylation (correct functioning of Ras proteins requires post-translational modification)
Chaperone inhibitors Histon deacetylase inhibitors (inhibition of
proliferation and induction of differentiation and apoptosis of tumor cells)
Proteosoms inhibitors (inhibition of NF-κB, inflammatory cytokine expression, induction apoptosis)
Proposed targeted therapy:Inhibitor of the IGF-I receptor (currently known agents: NVP-
AEW541-A and NVP-ADW742)
Explanation: Inactivating mutations at the 17p13 locus including the TP53
tumour suppressor gene and alterations of the 11p15 locus leading to IGF-II overexpression are frequently observed in adrenocortical carcinoma. In vitro experiments suggest that overexpressed IGF-II acting via the IGFI receptor is relevant for adrenal cancer cell proliferation. Thus, the IGF-II IGF-I receptor pathway is a promising target for future therapies in ACC.
Potential combined therapy:mitotan plus radiolabelled inhibitor of IGF-I receptor
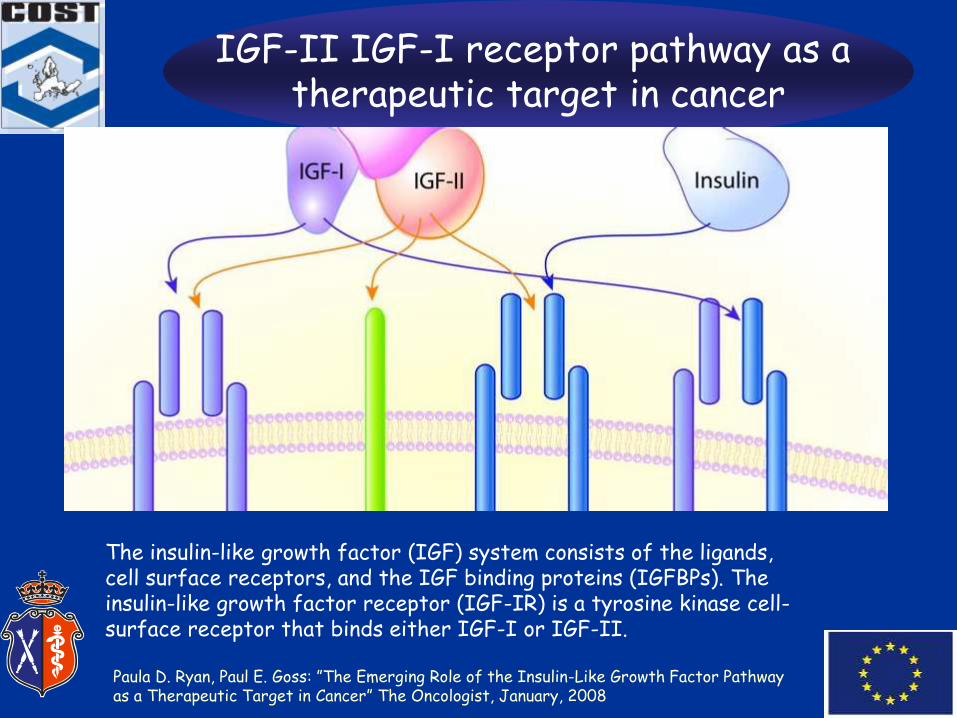
IGF-II IGF-I receptor pathway as a therapeutic target in cancer
The insulin-like growth factor (IGF) system consists of the ligands, cell surface receptors, and the IGF binding proteins (IGFBPs). The insulin-like growth factor receptor (IGF-IR) is a tyrosine kinase cell-surface receptor that binds either IGF-I or IGF-II.
Paula D. Ryan, Paul E. Goss: ”The Emerging Role of the Insulin-Like Growth Factor Pathway as a Therapeutic Target in Cancer” The Oncologist, January, 2008
IGF-II IGF-I receptor pathway as a therapeutic target in cancer
Binding of the ligands IGF-I and IGF-II to IGF-IR activates its intrinsic tyrosine kinase activity resulting in signaling through cellular pathways that stimulates proliferation and inhibits apoptosis. Therapeutic approaches that target the IGF-I R are being tested clinically and include antibodies directed at the extracellular portion of the receptor and small molecule tyrosine kinase inhibitors with specificity for IGF-IR.
Paula D. Ryan, Paul E. Goss: ”The Emerging Role of the Insulin-Like Growth Factor Pathway as a Therapeutic Target in Cancer” The Oncologist, January, 2008
Adrenocortical carcinoma
Proposed targeted therapy:Inhibitor of the IGF-I receptor (currently known agents: NVP-
AEW541-A and NVP-ADW742)
Explanation: Inactivating mutations at the 17p13 locus including the TP53
tumour suppressor gene and alterations of the 11p15 locus leading to IGF-II overexpression are frequently observed in adrenocortical carcinoma. In vitro experiments suggest that overexpressed IGF-II acting via the IGF-I receptor is relevant for adrenal cancer cell proliferation. Thus, the IGF-II IGF-I receptor pathway is a promising target for future therapies in ACC.
Potential combined therapy:mitotan plus radiolabelled inhibitor of IGF-I receptor
Vascular targeted therapies in ACC
Proposed targeted therapy- antiangiogenic agents:
antibodies against VEGF (bevacizumab) or inhibitors of the VEGFR kinases
Explanation:
VEGF is the predominant signal for both endothelial cells proliferation and migration into sites of neovascularization, and blockade of this signal has been a major goal of research in this field (by VEGFR2)
Potential combined therapy:
mitotan plus radilabelled bevacizumab
- would such therapy be more effective than mitotane treatment only?
- would possible side-effects make this therapy useless?
Vascular targeted therapies in ACC
Proposed targeted therapy:• Inhibitors of matrix metalloproteinases• Inhibitors of other angiogenic molecules such as angipoietin• Monoclonal antibodies against tumour endothelial markers
Explanation:Expression of matrix metalloproteinase type 2 was discovered
in malignant adrenocortical tumours (75%)Additionally, serial analysis of gene expression of tumour
endothelium led to the identification of anonymous genes known as tumour endothelial markers (TEMs), of which TEM1 (endosialin), TEM5, and TEM8 have been shown to be specific for tumour vasculature. These proteins, all of which are cell surface antigens, provide potential targets for the development of agents that influence them directly
Other possible targets in ACC
Proposed targeted therapy:Inhibitors directed against enzymes specific for steroidogenesis or
antibodies against such enzymes/steroid hormones precursors; for example HSD3ß2 (hydroxy-steroid dehydrogenase) enzyme
Explanation:characteristic steroidogenesis enzyme in adrenal carcinoma is
HSD3ß2, responsible for conversion of pregnenolon to progesterone, it is expressed especially in granulosa and reticular stratum and it is very specific for adrenocortical carcinoma (high expression of this enzyme in hormonally active tumours).
Potential combined therpy:inhibitor of HSD3ß2 only (?) plus radiolabelled inhibitor of 11beta
hydroxylase (metyrapone)
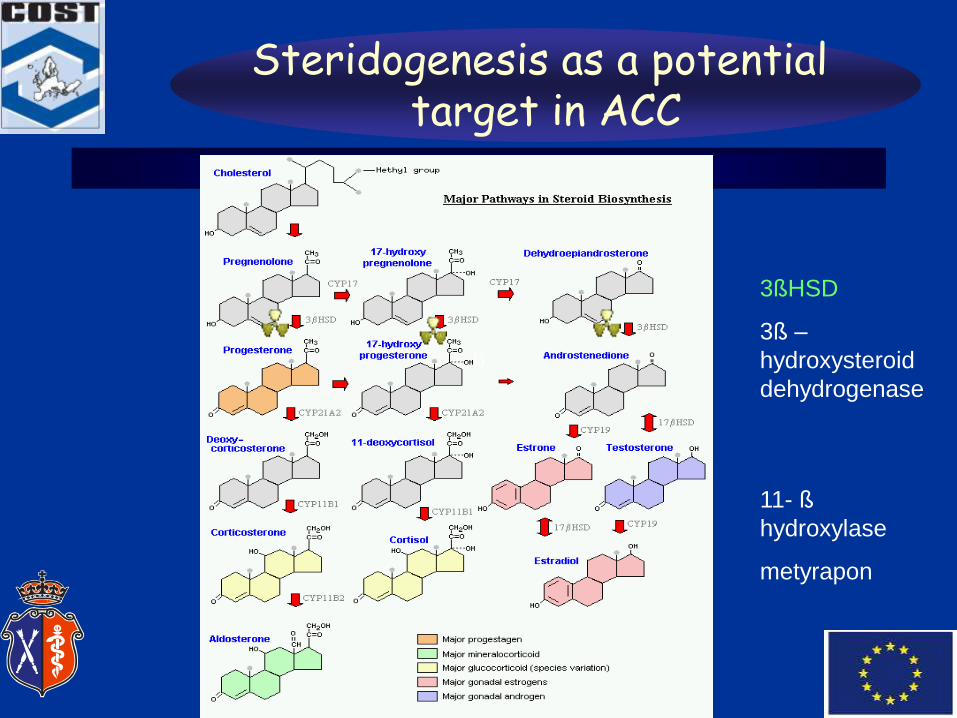
Steridogenesis as a potential target in ACC
3ßHSD
3ß –
hydroxysteroid
dehydrogenase
11- ß
hydroxylase
metyrapon
ß
Other possible targets in ACC
Proposed targeted therapy:Inhibitors directed against enzymes specific for steroidogenesis or
antibodies against such enzymes/steroid hormones precursors; for example HSD3ß2 (hydroxy-steroid dehydrogenase) enzyme
Explanation:characteristic steroidogenesis enzyme in adrenal carcinoma is
HSD3ß2, responsible for conversion of pregnenolon to progesterone, it is expressed especially in granulosa and reticular stratum and it is very specific for adrenocortical carcinoma (high expression of this enzyme in hormonally active tumours).
Potential combined therpy:inhibitor of HSD3ß2 only (?) plus radiolabelled inhibitor of 11beta
hydroxylase (metyrapone)
Mutations in papillary thyroid cancer
RET (5-30%)
RAS (10%)
BRAF (40%)
RET and RAS are tyrosine kinases
Genetic factors in medullary thyroid carcinoma
MEN2A – 16%
MEN2B – 3%
Simply familial medullary thyroid carcinoma – 5%
Familial MTC is caused by germinal RET proto-oncogene mutation.
i.e. approximately 98% of all MEN2B patients carry a missense mutation in codon 918 of RET proto-oncogene.
Known tyrosine kinase inhibitors
Axitinib - renal cell carcinoma (RCC), pancreatic cancerBosutinibCediranib – non-small cell lung cancer, colorectal cancer tumors of
central nervous system in childrenDasatinib – chronic myelogenous leukemia (CML), Philadelphia
Chemical structures of small molecule kinase inhibitors
Inhibitors of the kinase activity of RET
Proposed targeted therapy:The RET kinase inhibitor NVP-AST487
Explanation:It inhibits the growth of human thyroid cancer cell lines with
activating mutations of RET but not the lines without RET mutations (for example with BRAF mutations).
Can RET kinase inhibitor be a ligand?
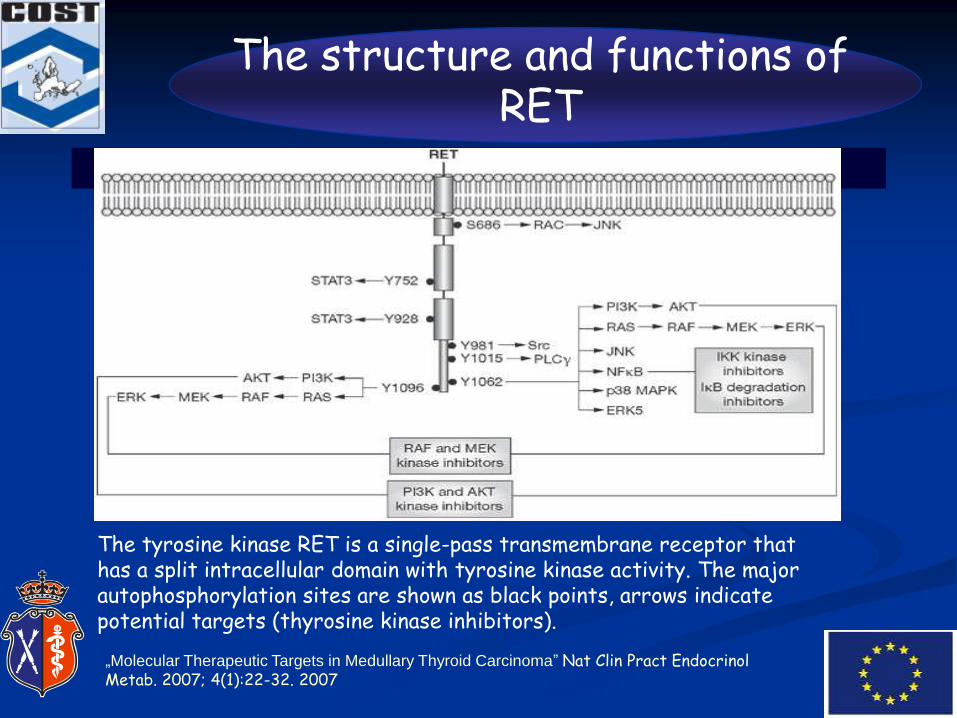
The structure and functions of RET
The tyrosine kinase RET is a single-pass transmembrane receptor that has a split intracellular domain with tyrosine kinase activity. The major autophosphorylation sites are shown as black points, arrows indicate potential targets (thyrosine kinase inhibitors).
the ligand binds to membrane-bound glycosylphosphatidylinositol-anchored GDNF-family coreceptors (GFR ) that are distributed within lipid rafts. Activation of RET leads to dimerization of RET, which consequently signals to the nucleus.
the ligand binds to the soluble form of its coreceptor (sGFR ) and the ligand-sGFR complex brings together two inactive RET monomers.
J. W. B. de Groot et al. Endocrine Reviews 27 (5): 535-560
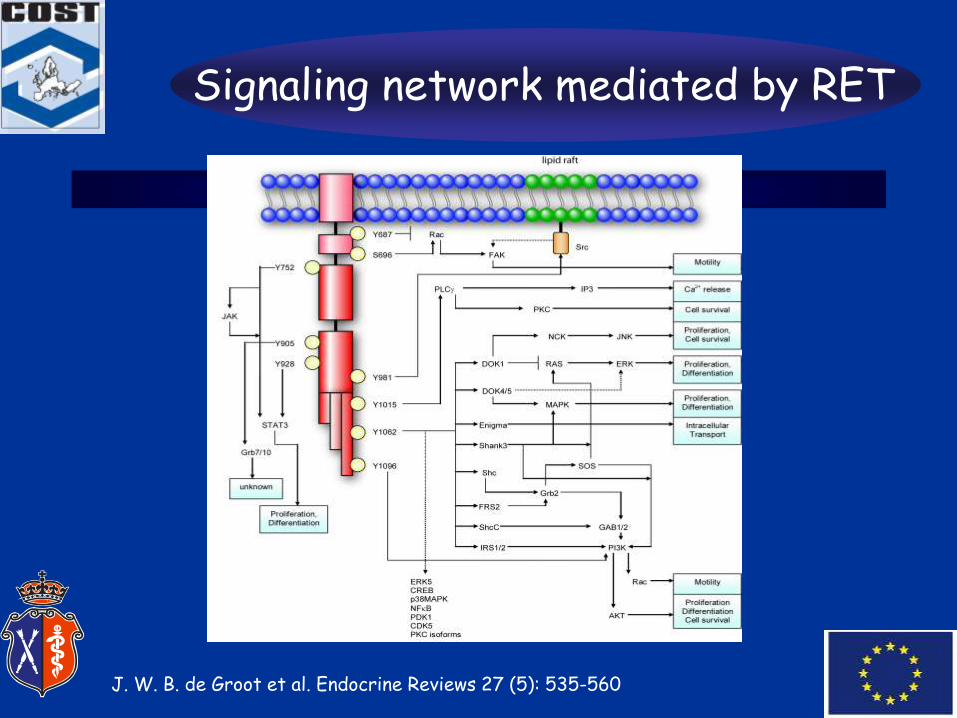
Signaling network mediated by RET
J. W. B. de Groot et al. Endocrine Reviews 27 (5): 535-560
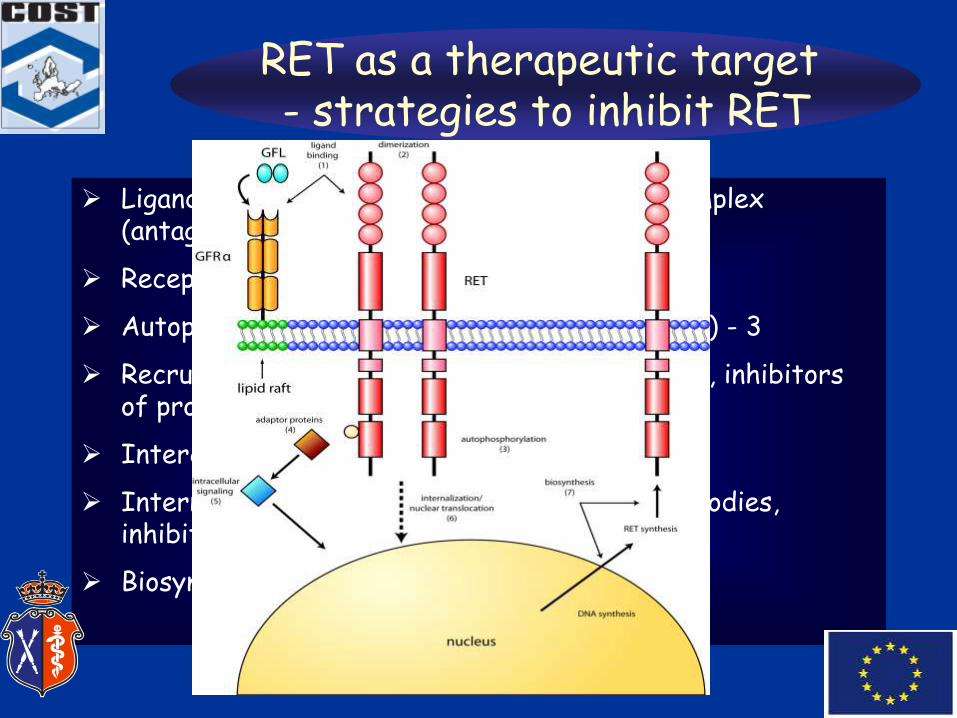
RET as a therapeutic target - strategies to inhibit RET
Ligand binding and formation of ligand-GFR complex (antagonists, antibodies) - 1
Activator of tyrosine kinases receptor (Trk B) –is it possible to find?
Explanation:
In medullary carcinoma, reduction in receptor TrkB expression isfound in the later stages of tumor progression. In a cell culture model, TrkB expression led to reduced VEGF concentrations and reduced tumorigenicity, suggesting that TrkB may inhibit medullary thyroid carcinoma angiogenesis and tumor growth.
Possible combined therapy:
TrkB activator with radiolabelled agents against VEGF pathway. The positive effect is uncertain.
Inhibitors of BRAF kinase
Proposed targeted therapy:
Using BAY 43-9006 – BRAF kinase inhibitor
Explanation:
gene BRAF mutation is the most frequent mutation in PTC (44%)
BRAF kinase inhibitor blocks the growth of thyroid cancer cells(more aggressive and less differentiated papillary tumours) that have RET/PTC or BRAF mutations
Hurthle cell carcinoma
Potential therapy:radiolabelled somatostatin analogues in disseminated Hurthle
cell carcinomas
Explanation:Hurthle cell carcinomas express the somatostatin receptor
type 2
Inhibition of HSP
Potential targeted therapy:Family of the ansamycin antibiotics acting through the heat
shock protein pathway
Explanation:Many oncogenic protein kinase depend on the molecular
chaperone HSP 90 – HSP90 inhibition
Malignant pheochromocytoma
Potential targeted therapy: inhibitors or/and monoclonal antibodies against pituitary
adenylate cyclase-activating peptide receptor
Explanation:Expression of PACAP – peptide structurally similar to
vasoactive intestinal peptide (VIP) acting by G protein-coupled receptor – found in neuroblastomas, non-functioning pituitary adenomas, somatotroph pituitary adenomas (PAC1) and in pheochromocytoma and paraganglioma (PAC2)
Malignant pheochromocytoma– other possibilities
• SSR 2,3,5 radiolabelled somatosatin analoques therapy combained with D 2 receptors agonist could be promising
• Inhibition of VEGF pathway – related to very high neoangiogenesis
GEP-NET – using kinase inhibitors
Potential targeted therapy:
Erlotinib (also gefitinib) as a small-molecule HER-1/EGFR tyrosine kinase inhibitor, acting on the intracellular domain of the receptor, preventing receptor activation and inhibiting downstream signal transduction and cell proliferation
Explanation:
HER-1/EGFR has a role in carcinogenesis in many types of cancer. This coexpression has been shown to stimulate tumor cell proliferation, and elevated HER-1/EGFR levels are linked to poor disease outcomes and lower sensitivity to chemotherapy. Blocking HER-1/EGFR should therefore help to stabilize tumor growth and improve prognosis via the inhibition of multiple HER-1/EGFR downstream signaling pathways. HER-1/EGFR expression has been found in the pulmonary NET.
Potential combined therapy:
Combination of radiolabelled erlotinib plus standard chemotherapy
GEP-NET – other possibilities Matrix metalloproteinase inhibitor marimastat or talomastat
Combined therapy: radiolabelled marimastat plus gemcitabine
Cetuximab – anti-HER-1/EGFR monoclonal antibody. This agent blocks the extracellular domain of HER-1/EGFR to prevent receptor activation.
Combined therapy: Cetuximab with radiolabelled somatostatin analogues in GEP NET therapy.
Labelled trastuzumab (monoclonal antibody against HER2-receptor)in HER-2 positive NET (intestinal, not gastric)
Gastrin releasing peptide (GRP) – brain-gut peptides including bombezin. Four different types of receptors are currently known. BB3 receptor is expressed in bronchial carcinoids. Neuromedin receptor is presented in ileal carcinoids, GRP receptors in gastrinomas.
Newly introduced NET therapy with SOM230 could be also used as the radiolabelled agent therapy.
Role of dopamine receptors
Potential targeted (combined) therapy: Using D2 receptor agonists and radiolabelled somatostatin
receptor analogues or combination of D2 receptor agonist with antiangiogenetic factors seem to be promising targeted therapy.
Explanation: Dopamine receptors are found in all types of neuroendocrine
tumors. Dopamine receptors – mostly D2 could mediate the inhibitory effect of dopaminergic drugs in these tumors, since cabergoline has been found to induce normalization of ACTH and consequently cortisol secretion.
The previous finding of dopamine receptors in GEP-NETcell lines and the recent finding of D2 receptors in GEP-NETsuggests a role for these receptors, and possibly a role of dopaminergic drugs in this category of neuroendocrine tumors.