101
Endocrine Review 2014 Ashley Inman (T. Davis)

Endocrine Review 2014
Ashley Inman(T. Davis)

Physiology Review
• Hypothalamic-pituitary axis
• Controls multiple end products via negative feedback loops:
• Cortisol• T3/T4• Testosterone• Estradiol, Progesterone• IGF-1
Cushing’s Syndrome(Hypercorticism regardless of cause)
• Laboratory Evaluation:– Overnight dexamethasone suppression test recommended as
initial screening test• Plasma cortisol at 8 am >50 nmol/L (2 microg/dl) after 1 mg
dexamethasone at midnight– OR use 24 hr urine-free cortisol in obese or depressed pts
• Urine free cortisol level >140 nmol/d (50 microg/d)– Confirm with failure of plasma cortisol to fall to <140 nmol/L (5
g/dL) or urinary cortisol to fall to <25 nmol/d (10 g/d) after standard dexamethasone suppression test (0.5 mg every 6 h for 48 h)
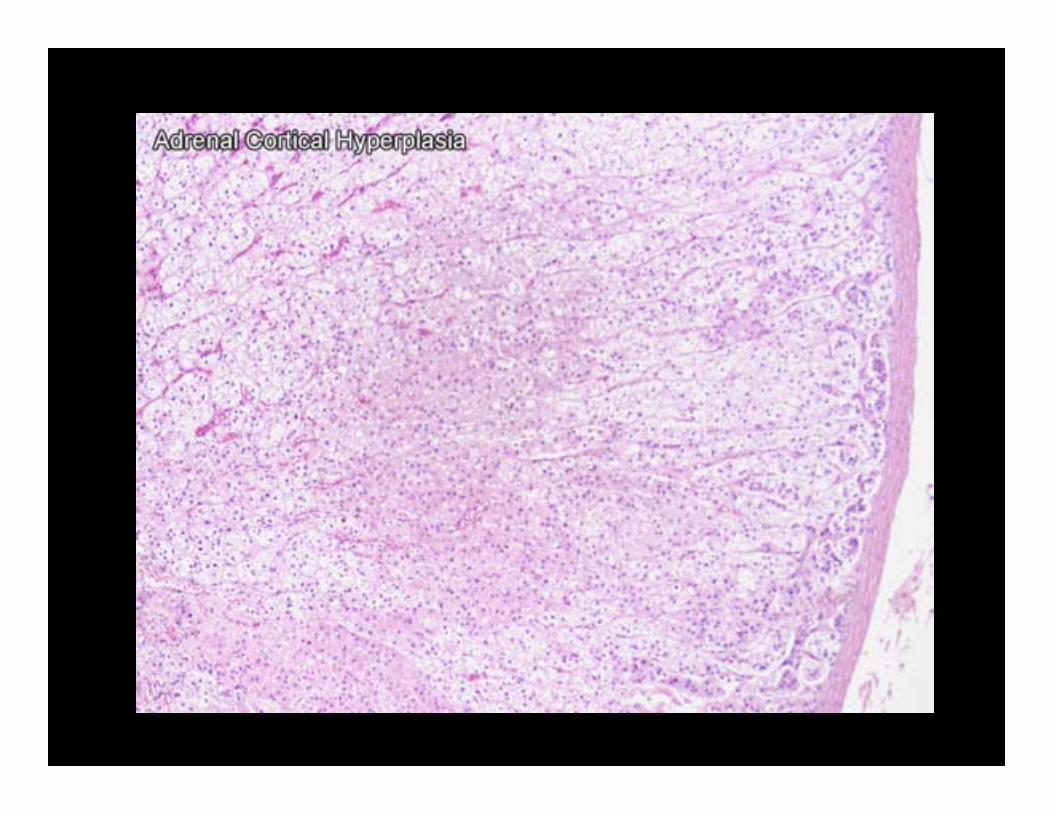
• CT of abdomen to identify adrenal hyperplasia/adenomas
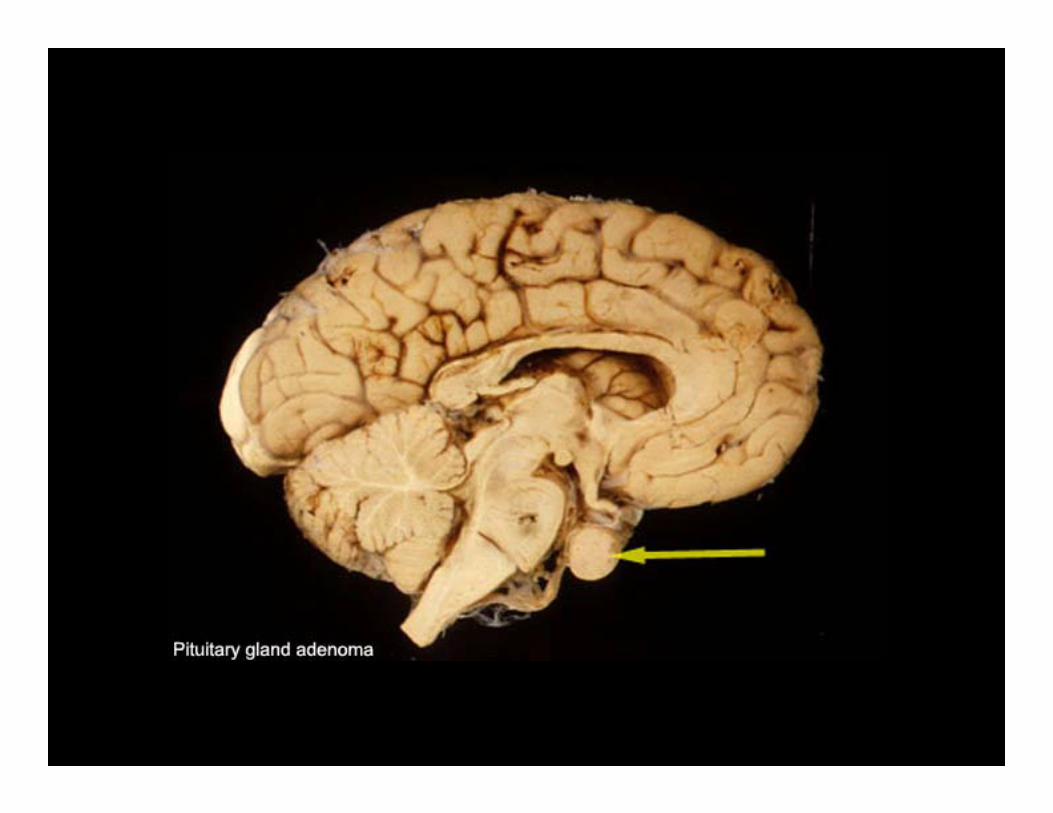
• CT head to identify pituitary adenomas

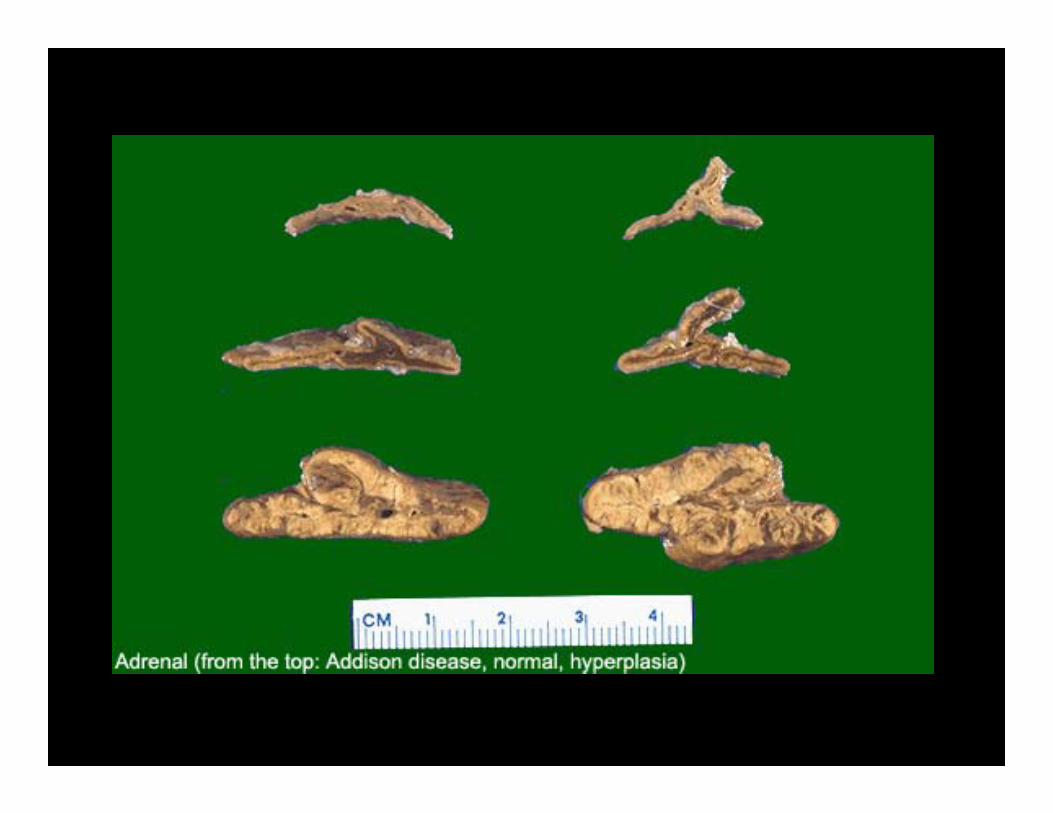
Addison’s Disease
• Laboratory Evaluation– May be normal in early stages except when under stress– More advanced stages, may have decreased levels of
Na+, Cl-, and bicarbonate and increased K+– ACTH Stimulation Test abnormal at all stages of disease
• Subnormal increase in cortisol or no increase at all (normal increase >495 nmol/L
• If abnormal, then measure aldosterone levels from the same blood samples (low in primary)


Aldosteronism
• Diagnostic criteria:1. Diastolic hypertension without edema2. Hyposecretion of renin3. Hypersecretion of aldosterone
• If positive, follow with abdominal CT– May identify aldosteronomas <1cm in size– If CT negative, follow with percutaneous transfemoral
bilateral adrenal vein catheterization with adrenal vein– May demonstrate a two- to threefold increase in plasma
aldosterone concentration on the involved side





Case 128 y.o. female, 8 months postpartum with
amenorrhea, loss of pubic hair and hypotension. She will need:
• A. Iron supplements• B. Iron, B12 and Folate supplements• C. RBC transfusion• D. Life-long hormone replacement• E. A psychiatric consultation

Case 232 y.o. female with breast discharge,
amenorrhea and bitemporal hemianopsia. You order:
• A. Serum prolactin and brain MRI• B. Urine FSH and LH• C. Adrenal and kidney ultrasound• D. Chest xray and sputum cytology• E. Pelvic examination and ovary ultrasound

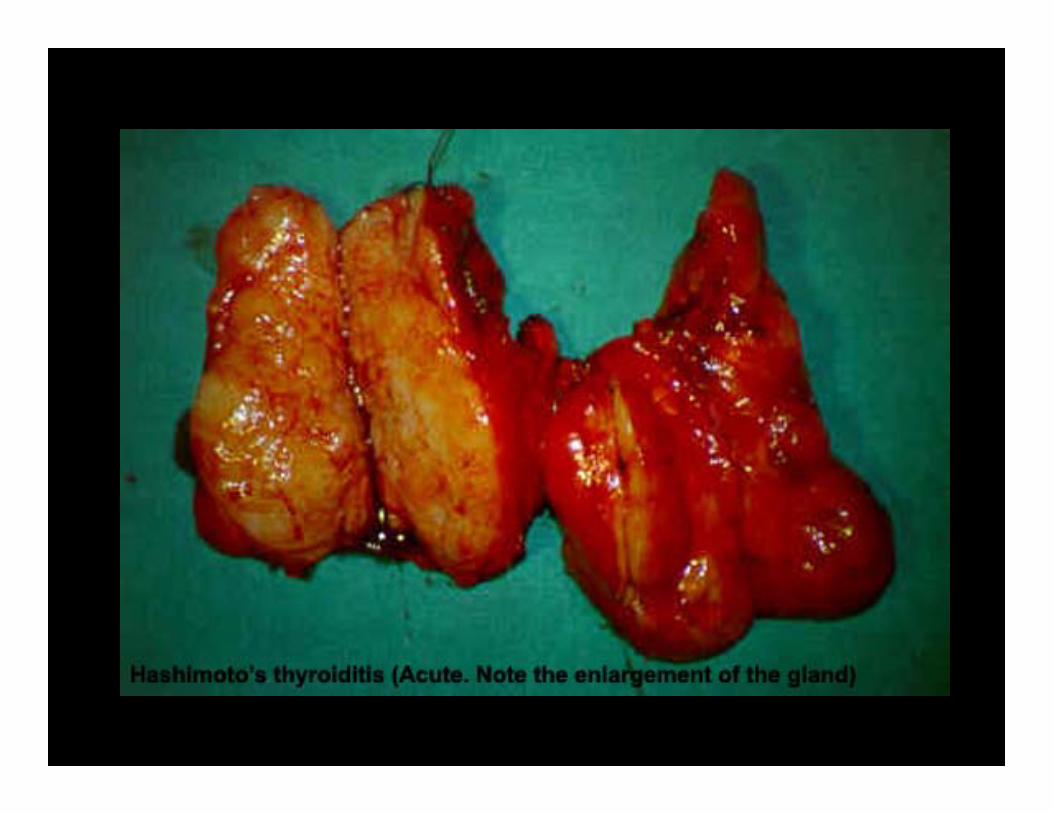
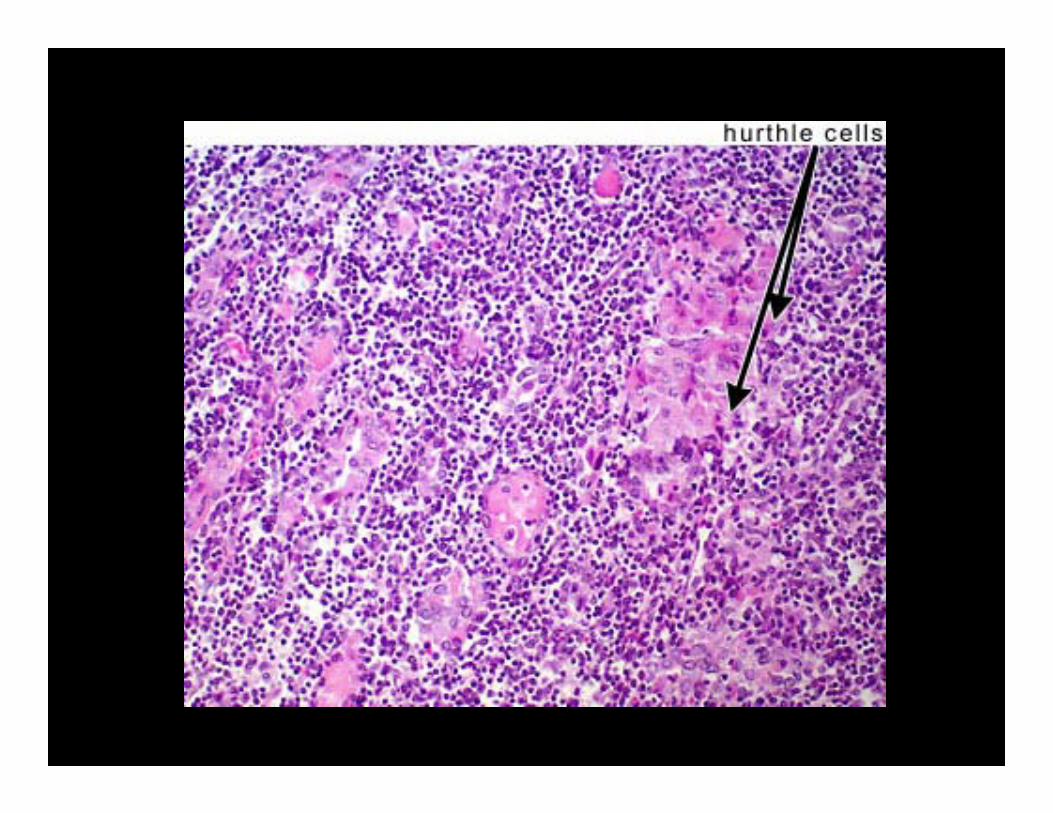
Case 348 y.o. female with lethargy, weight gain and loss of lateral eyebrows. Thyroid histology?
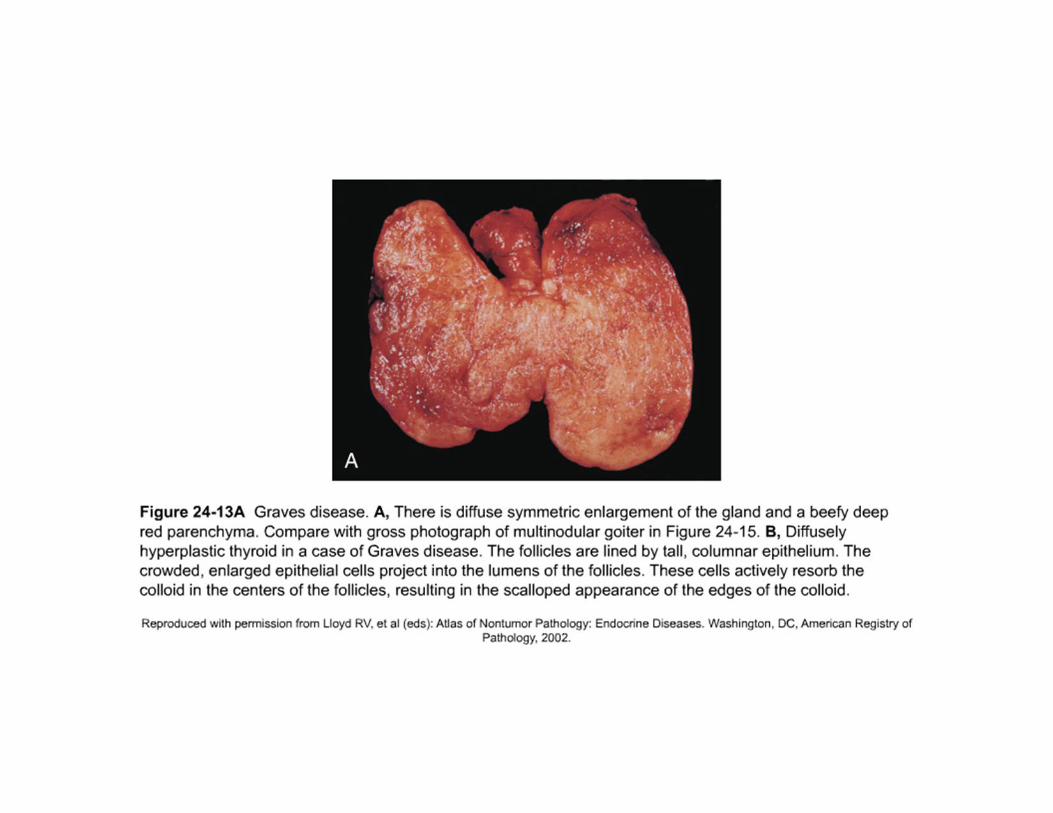
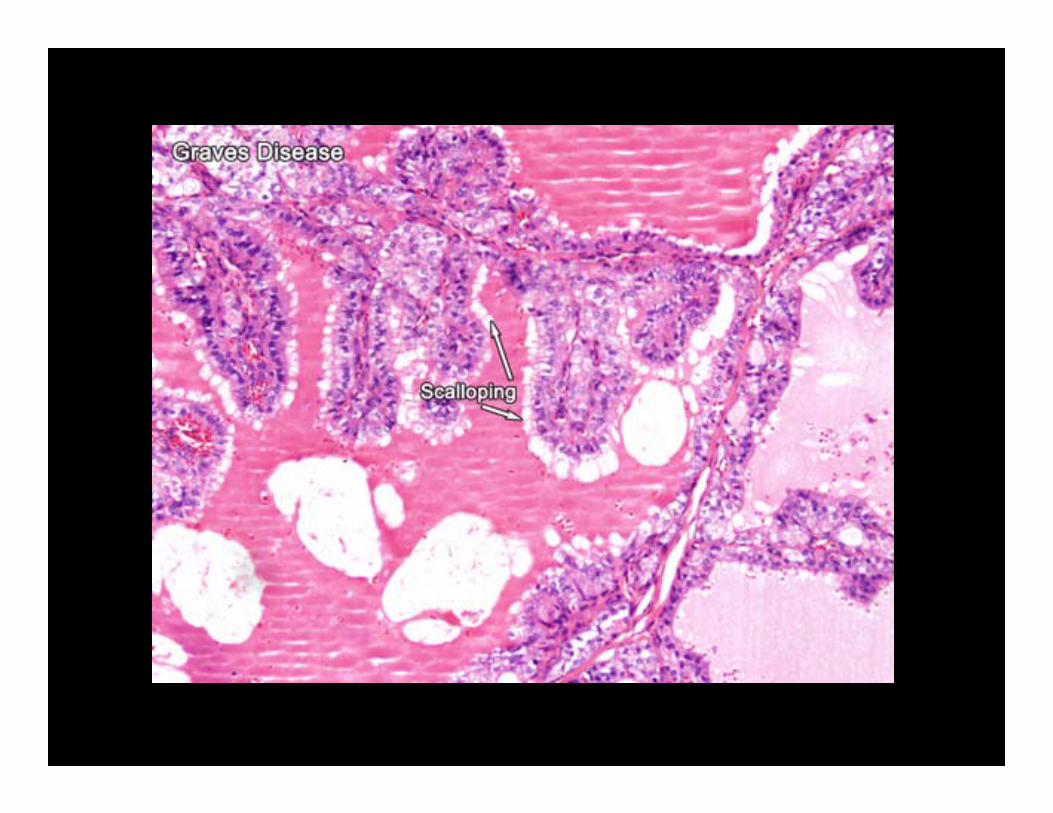
• A. Papillary hyperplasia• B. Tall columnar epithelium• C. Colloid scalloping• D. Lymphoid nodules• E. Neuroendocrine cells with amyloid


Case “4”Also Case 3 patient- You would expect to find
autoantibodies directed against all the following EXCEPT___?
• A. Thyroglobulin • B. Microsomes (peroxidases)• C. TSH receptors• D. Iodine

Case 545 y.o. male with heat intolerance,
palpitations and an diffusely enlarged thyroid.
Expected labs:
A. High TSH, High T4B. High TSH, Low T4C. Low TSH, High T4D. Low TSH, Low T4E. Normal TSH and T4
Papillary hyperplasia
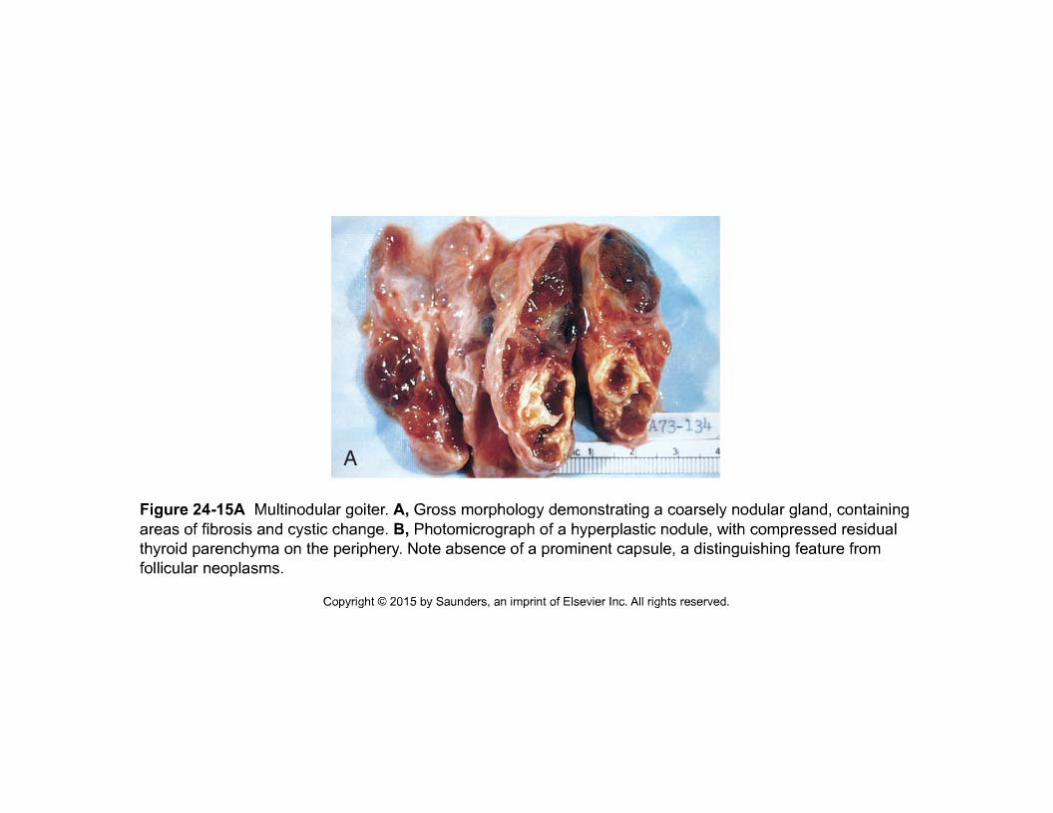
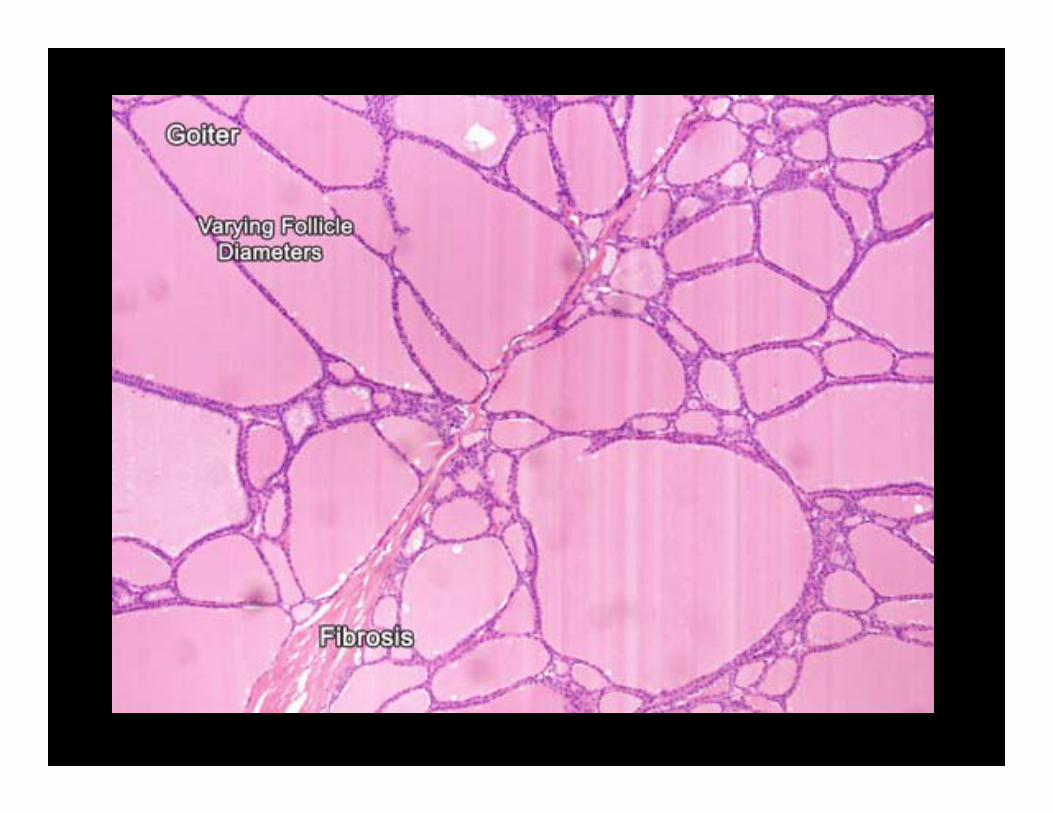
Case 660 y.o. female with small lumps in neck. Thyroid is irregularly enlarged and the gland is “toxic”.
The patient is:
A. HyperthyroidB. HypothyroidC. EuthyroidD. Infected



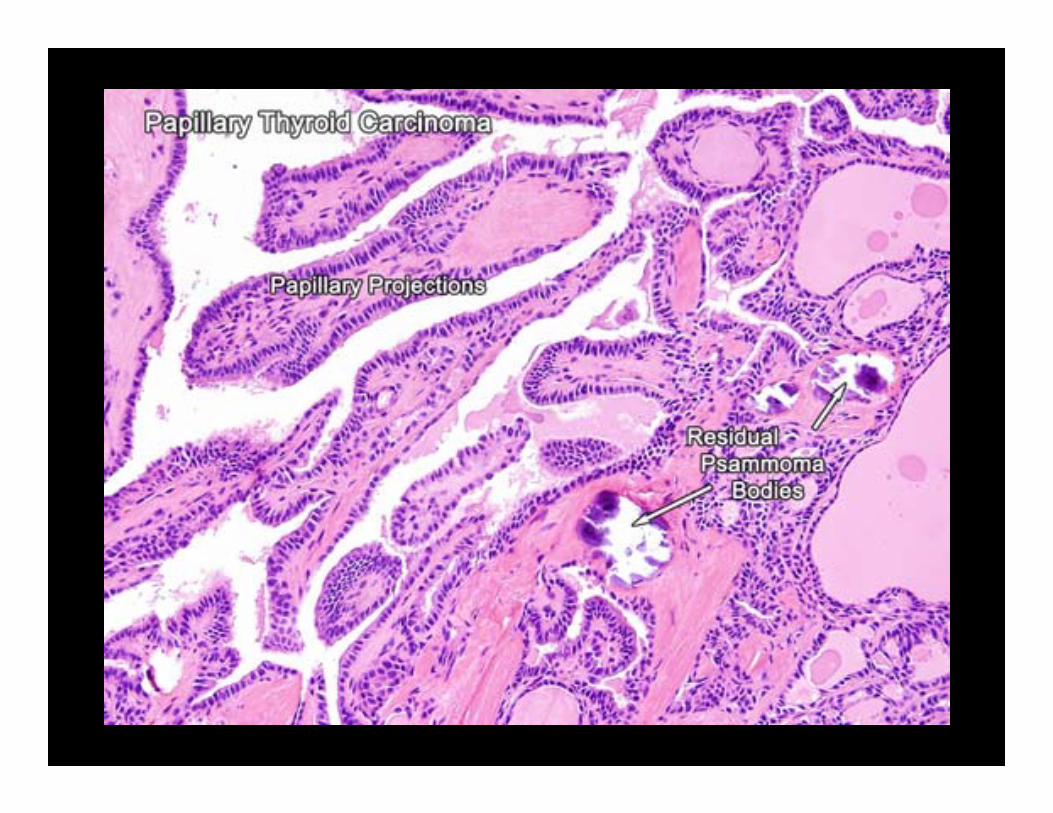
Case 729 y.o. female has thyroid biopsy. Histology
shows malignant follicles and vesicular nuclei with “grooves”. Dx?
• A. Papillary CA• B. Follicular CA• C. Medullary CA• D. Anaplastic CA
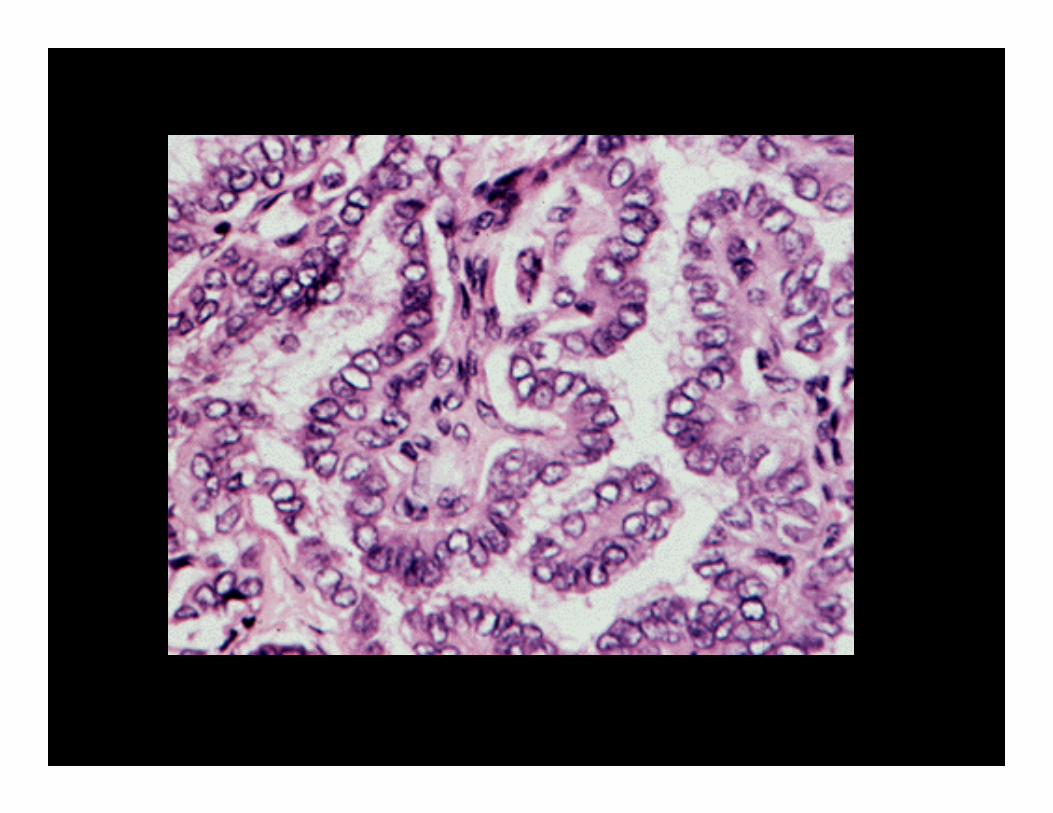
Vesicular nuclei- sometimes “grooved”
“Orphan Annie Eyes”



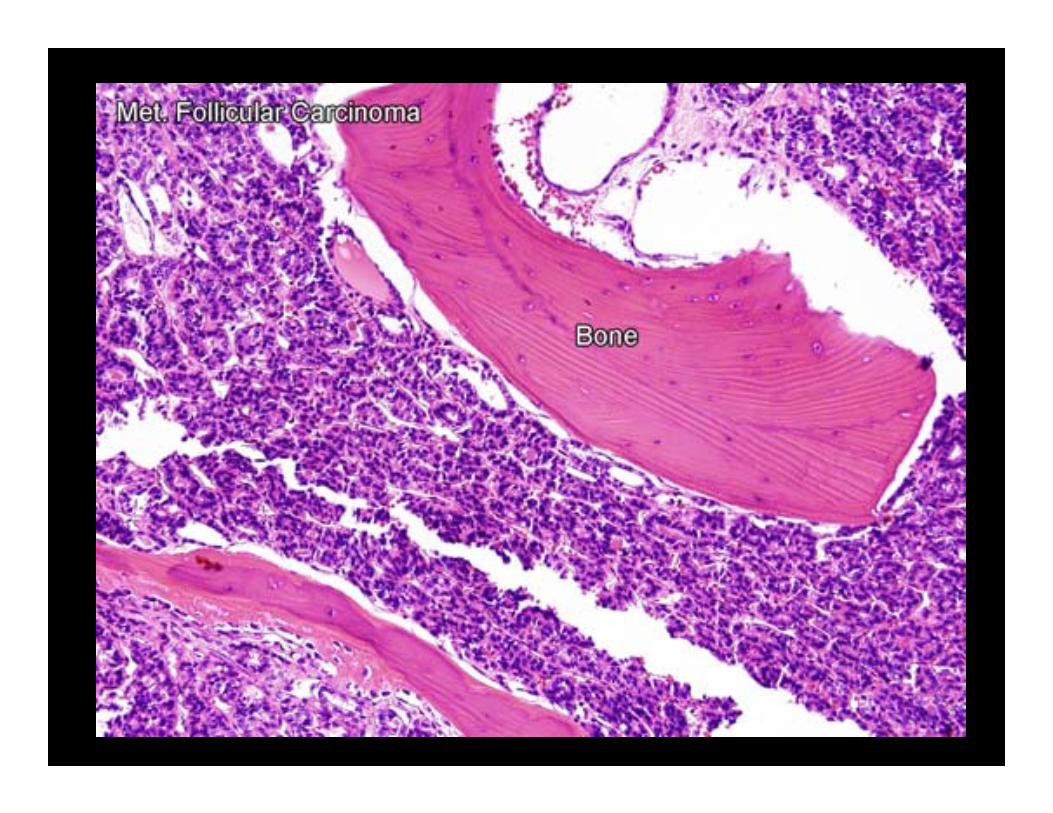
Case 8What identifies a follicular thyroid tumor
as malignant?
• A. Increased mitoses• B. Production of thyroxine• C. Anti-TSH receptor antibodies• D. Irregular follicle shapes• E. Vascular invasion



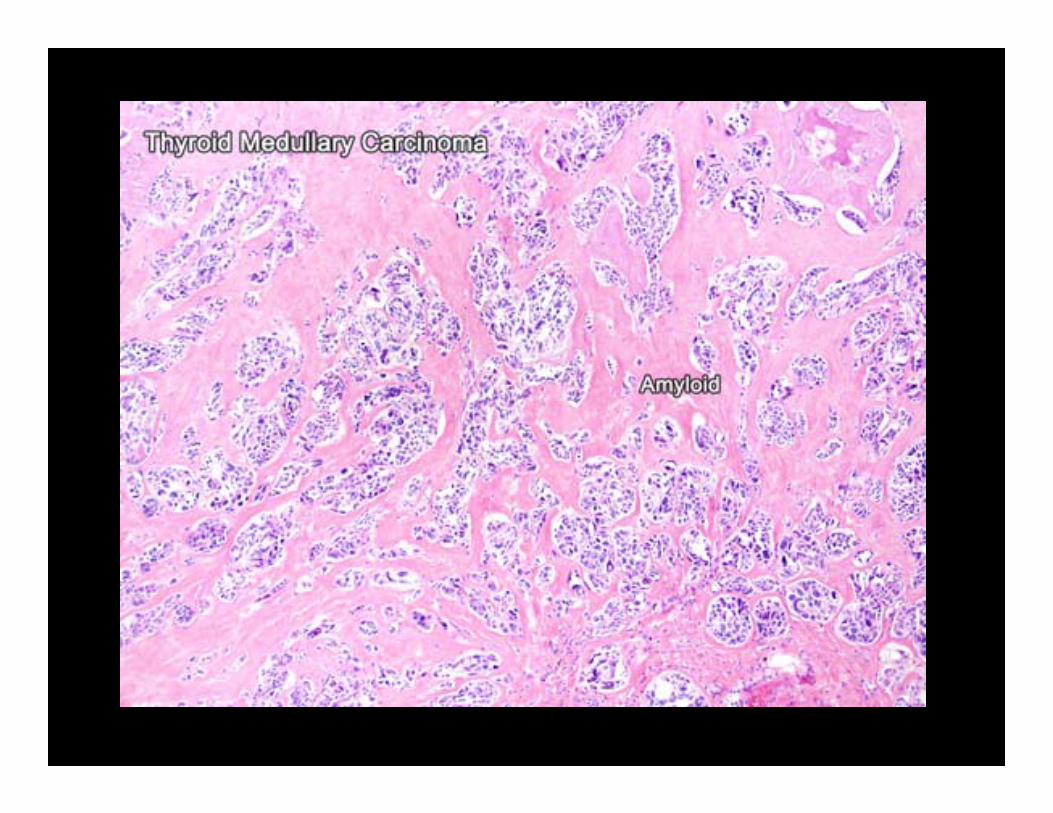
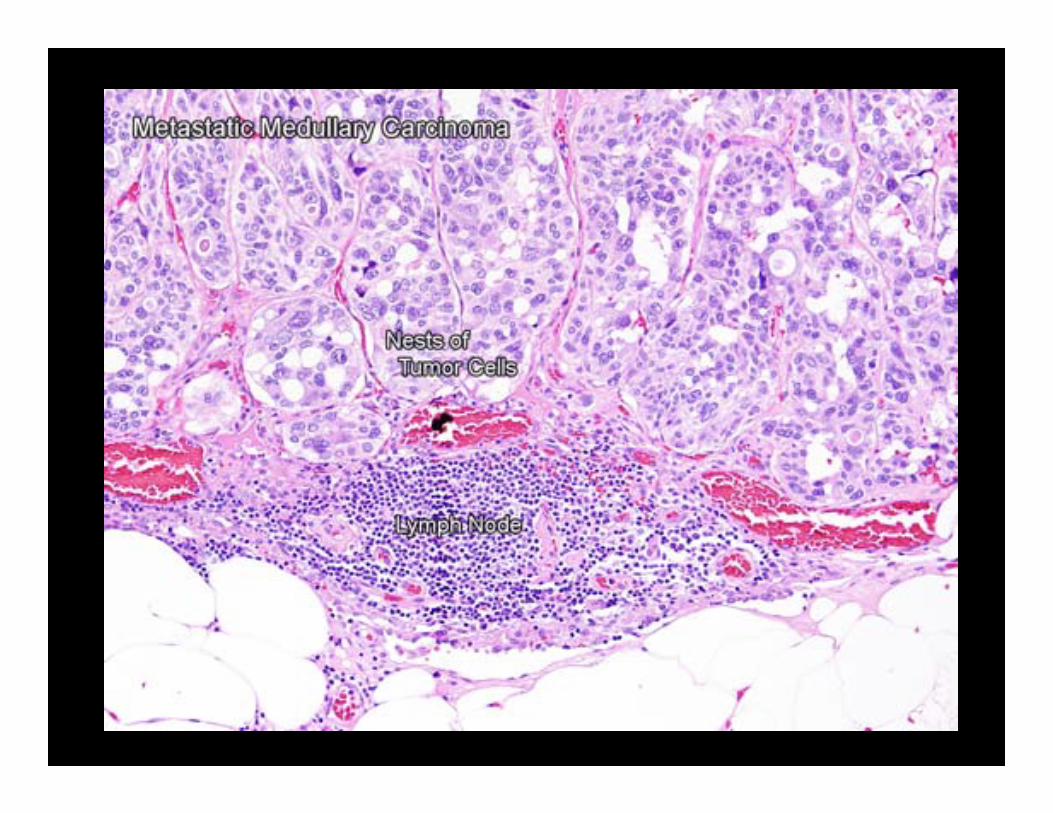
Case 9A 42 y.o. female has medullary CA of the
thyroid. Serum Ca++ is:
• A. Elevated• B. Decreased• C. Normal• D. Not detectable• E. A, B, or C

Case 1045 y.o. female, post-thyroidectomy has
carpal spasm and facial twitching if you tap her facial nerve. Labs expected?
A. Hypercalcemia, low serum phosphateB. Hypercalcemia, high serum phosphateC. Hypocalcemia, hypophosphatemiaD. Hypocalcemia, hyperphosphatemiaE. Elevated PTH levels
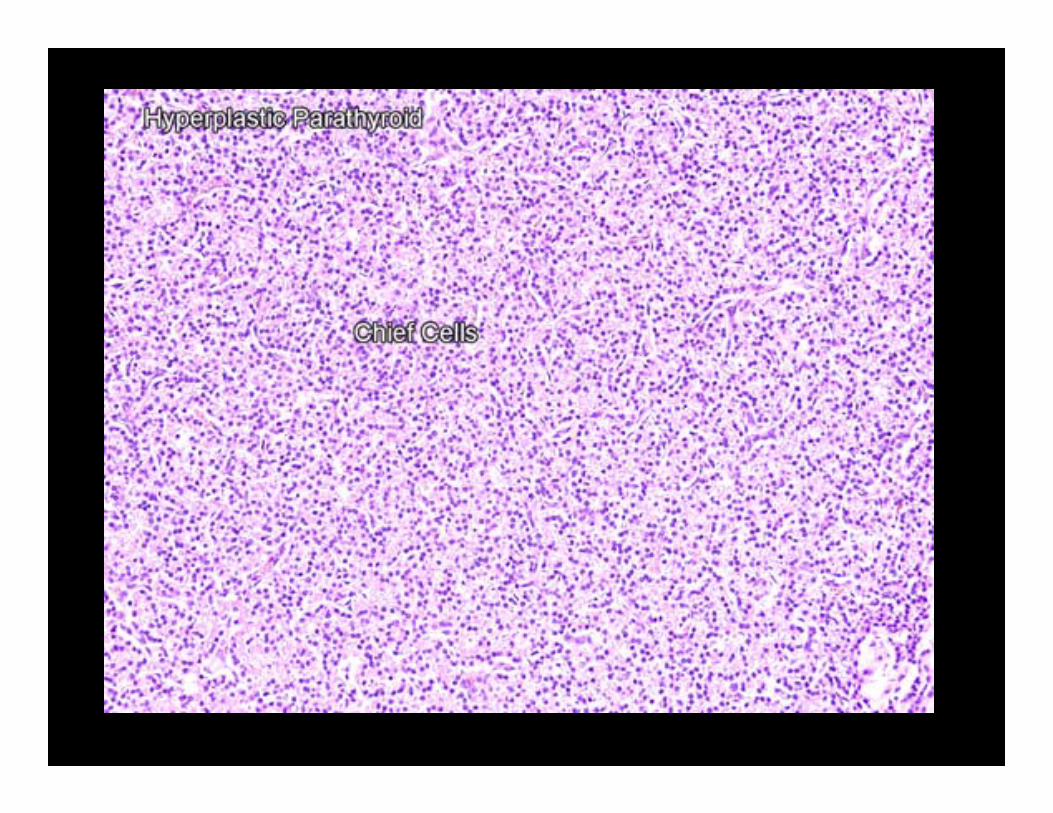
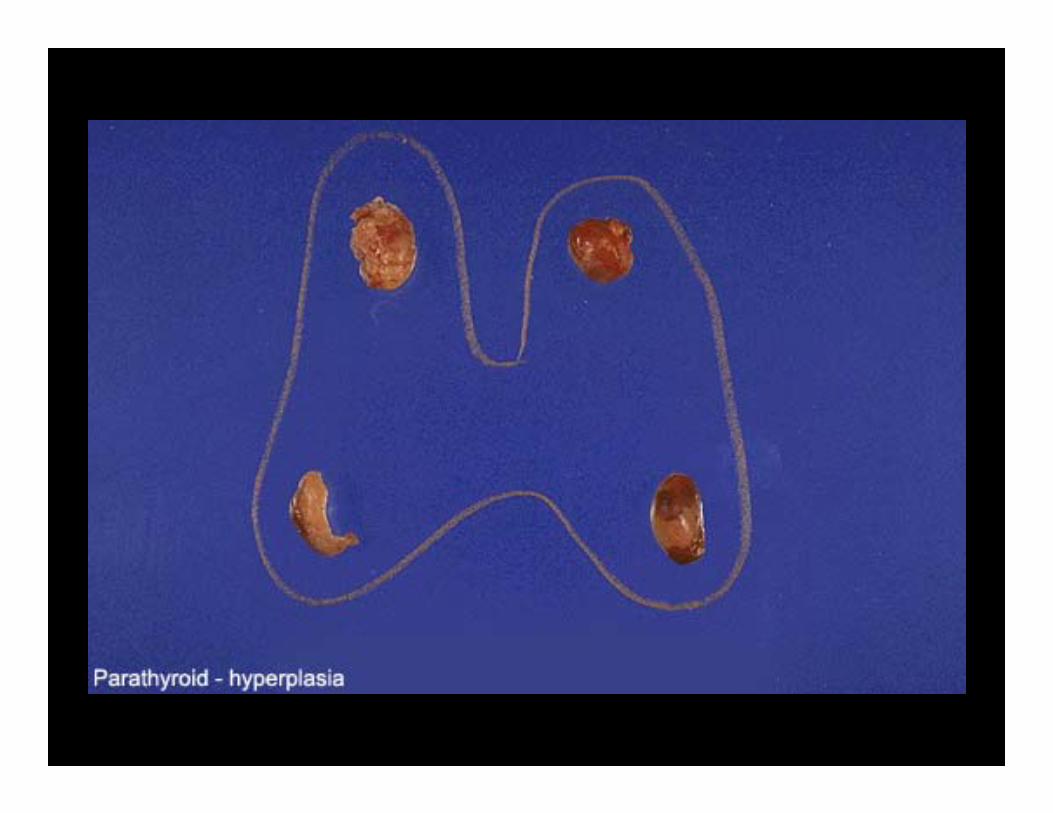
Case 11Patient has high serum Ca++. Surgeon
removes 2 parathyroids, both have no fat. Dx?
• A. Double adenoma• B. Hyperplasia• C. Normal, biopsy more glands• D. Carcinoma, remove thyroid and all 4
parathyroids


Case 12 High Ca++ patient. Surgeon removes 4 parathyroids all with fat. There is no 5th
gland detected in the thyroid. Dx?
A. HyperplasiaB. Quadruple adenomaC. Normal, do total thyroidectomy to remove all
possible parathyroid tissueD. Rule out lung cancer


Case 1360 y.o. female with hypercalcemia, kidney stones, bone pain, polyuria, weakness and constipation and low serum phosphate. A
bone biopsy reveals?
• A. Metastatic parathyroid carcinoma• B. Metastatic thyroid carcinoma• C. Metastatic prostate carcinoma• D. Osteitis fibrosa cystica• E. DiGeorge syndrome

Osteitis Fibrosa Cystica with “Brown tumors”
Case 145 y.o. short, “overprotected” boy has bowed
legs, broad sternum and square head. You should:
A. Order a CT of the headB. Order TSH and T4C. Prescribe synthroidD. Prescribe vitamin supplementsE. Tell the parents to avoid sun exposure


Case 1510 y.o. girl is confused with rapid
breathing. She has fruity breath. Parents say she eats a lot, but has lost weight.
You expect:
A. HypoglycemiaB. KetonemiaC. Low TSHD. High TSHE. Possible hyperosmolar coma

Insulitis

Case 1648 y.o. obese man with increased thirst and urinary volume. You expect to find:
A. Increased sensation in fingers and toesB. Increased dorsalis pedis pulsesC. HypoglycemiaD. Proliferative retinopathyE. High risk for ketoacidosis


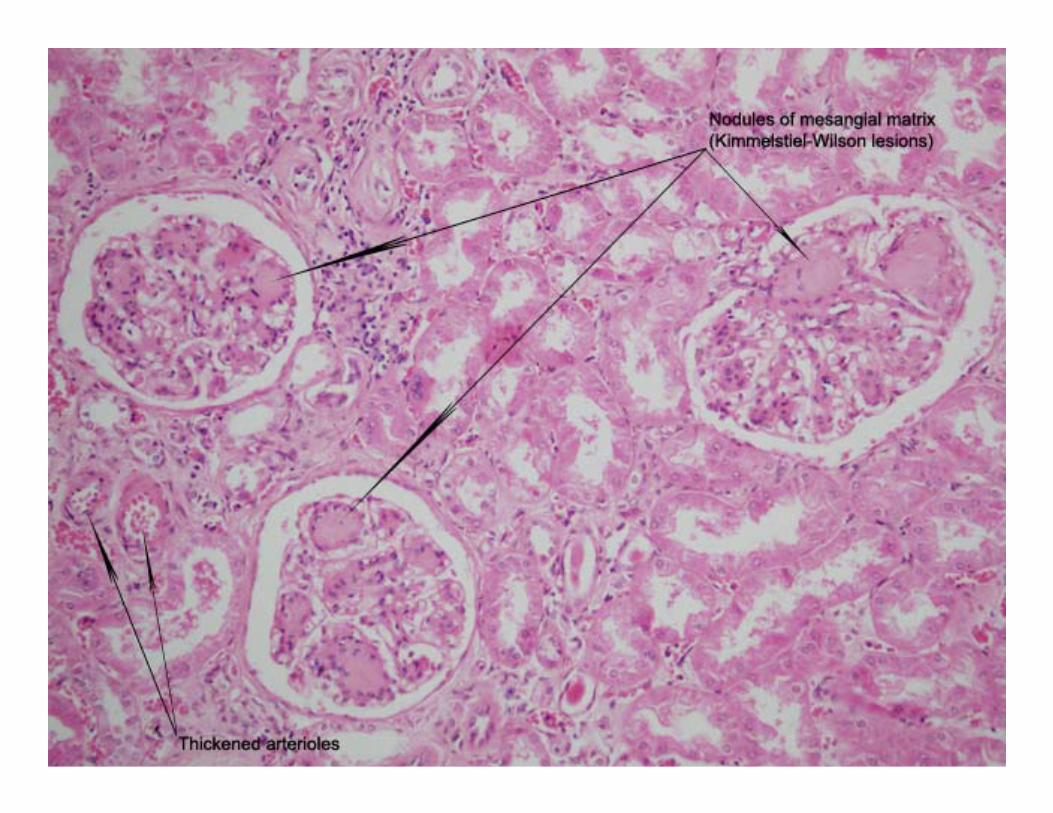
Case 1760 y.o. male with 20 year history of type II
DM. Labs show proteinuria, hyperlipidemia and hypercholesterolemia. Renal Bx ?
A. Lymphocytic infiltrate in glomeruliB. Granulomatous inflammationC. Micronodular glomerulosclerosisD. Aschoff bodiesE. Normal glomeruli


Case 1840 y.o. female has watery diarrhea,
midepigastric pain and shallow ulcers in the duodenum. Antacids and cimetidine give no
relief. What test is likely to be elevated?
A. InsulinB. SomatostatinC. GlucagonD. Vasoactive intestinal peptide (VIP)E. Gastrin

Case 19Male Cushings pt.; 1 mg Dm = no
suppression; 8 mg Dm = suppression. Cause?
A. Pituitary adenomaB. Adrenal adenomaC. AdrenocorticocarcinomaD. Ectopic ACTH (lung cancer)E. Germ cell tumor of testis


Case 20Male Cushings pt.; 1 and 8 mg fail to
suppress. What next?
A. Give 16 mg dexamethasoneB. Measure serum cortisolC. Measure urine cortisolD. Measure serum ACTHE. Ultrasound of testes

Case 2135 y.o. male with diarrhea, skin flushing,
cyanosis and heart murmur. Dx?
A. Cushing SyndromeB. Addison SyndromeC. Hashimoto SyndromeD. Graves diseaseE. Carcinoid syndrome


Case 2247 y.o. female with nausea and fatigue.
Knees and elbows are hyperpigmented. BP is low. ??
A. Acanthosis nigricansB. Type I DMC. Type II DMD. Autoimmune diseaseE. Adrenocorticocarcinoma
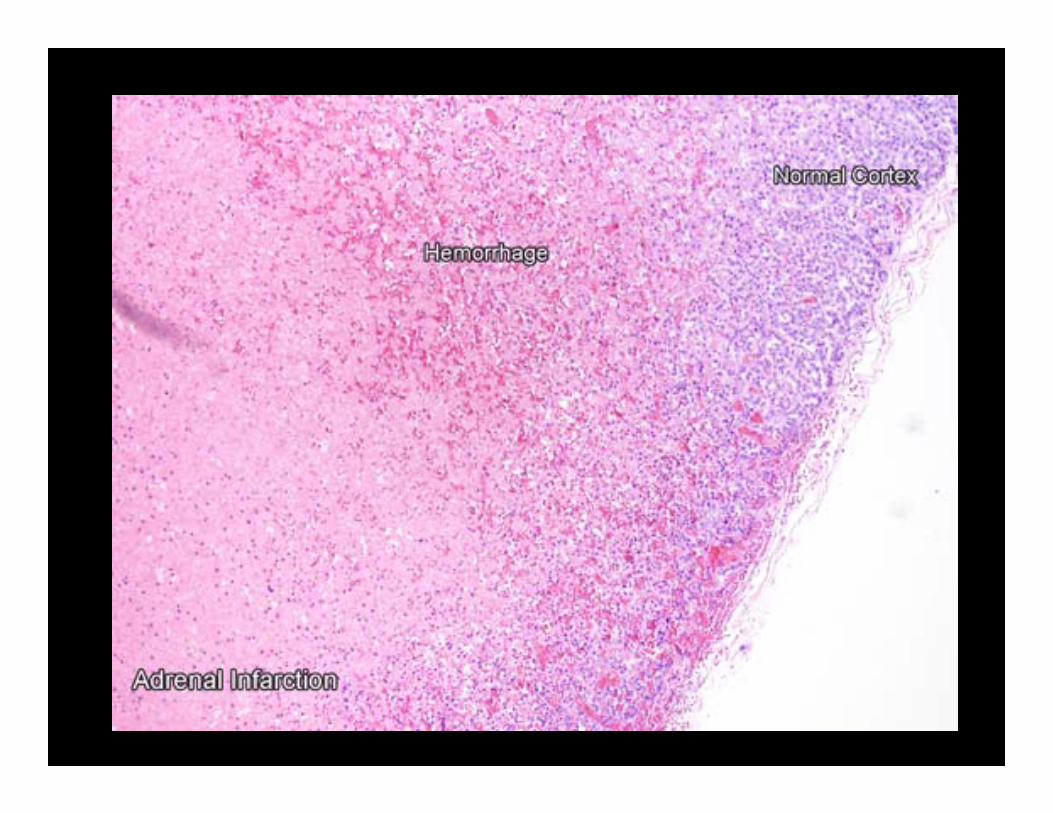


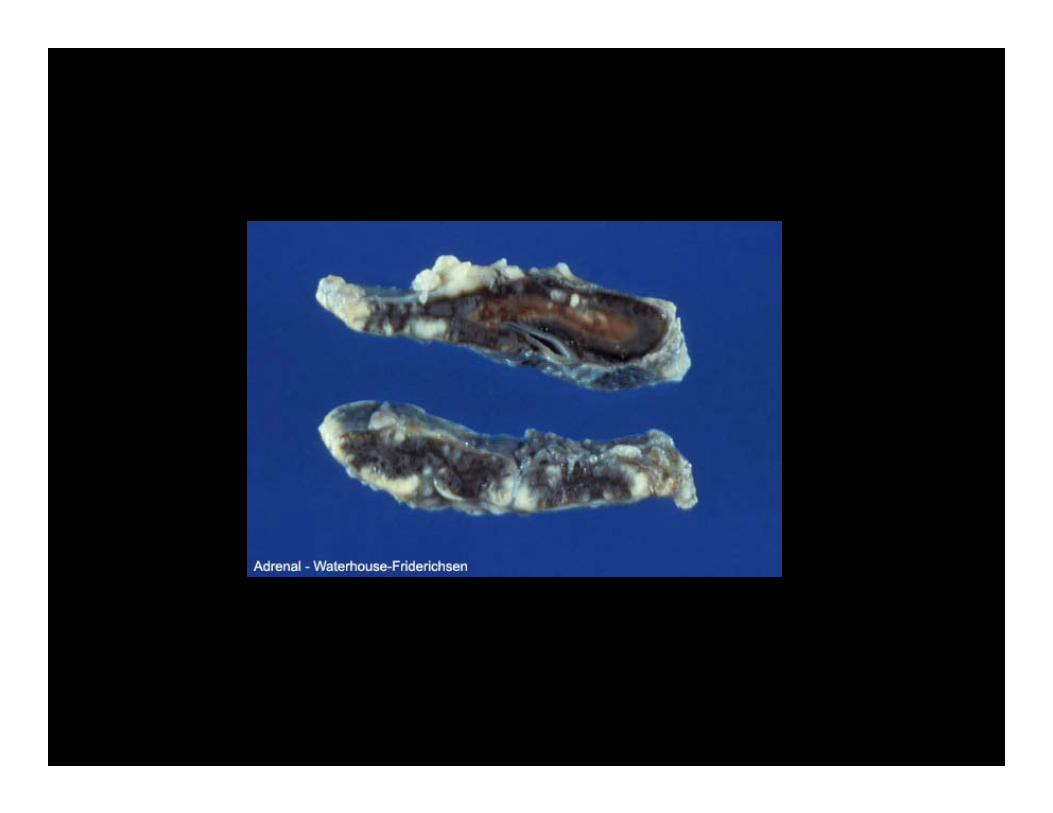
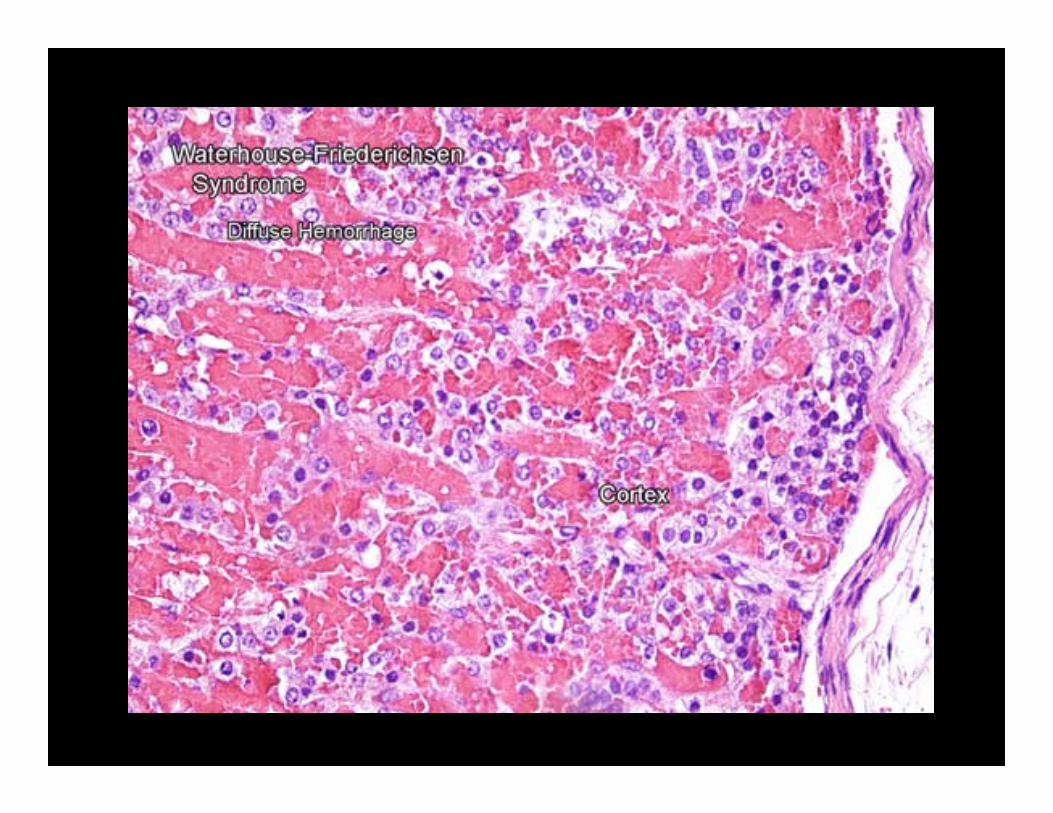
Case 23What are causes/etiologies of Waterhouse-
Friderichsen Syndrome
A. N. meningitidis and N. gonorrhoeaeB. N. meningitidis and H. influenzaeC. S. aureus and S. epidermadisD. Salmonella and ShigellaE. Cryptococcus neoformans

Case 2425 y.o. male (not obese or diabetic) with
headache and palpitations. BP is 200/110. Which of the following correct?
A. 90% of these patients are MEN II or IIIB. Most of these cases are sporadicC. The most sensitive test is urine VMAD. The most sensitive test is urine metanephrines
(TOTAL)E. The most specific test is urinary metanephrines
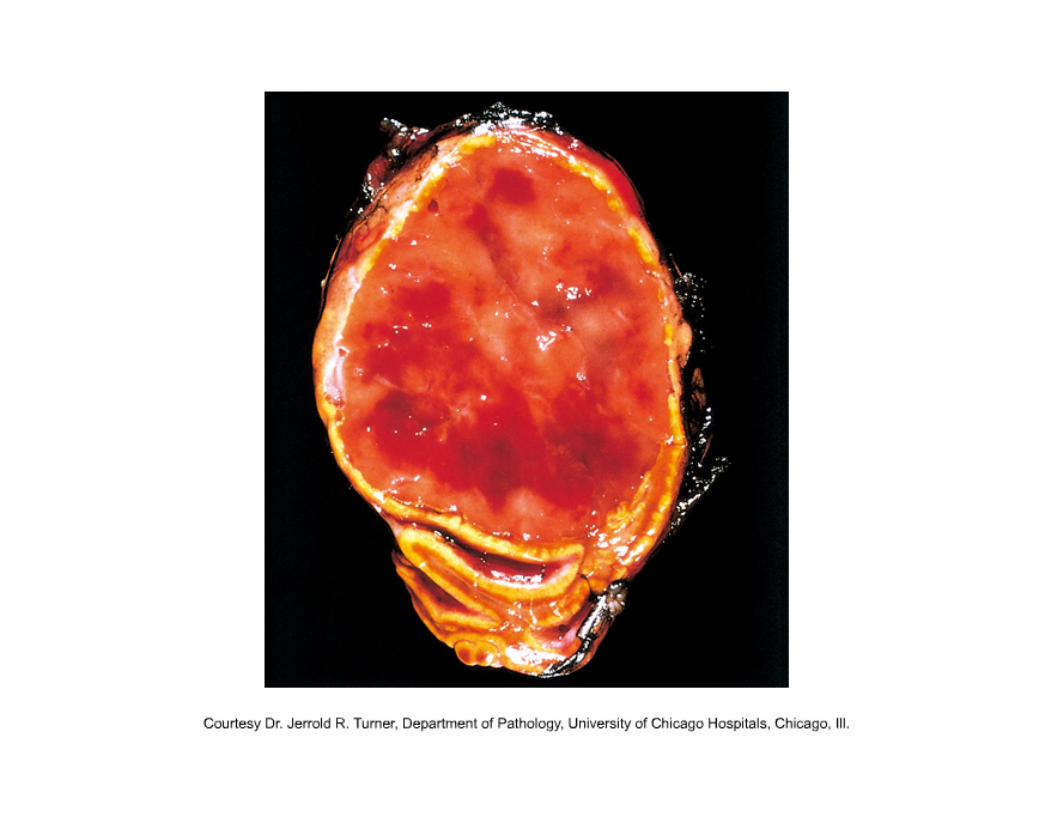




Case 25A2 m.o. child with calcified abdominal mass
(that crosses midline) suddenly shrinks before Rx. ?
A. Wilm’s tumorB. NeuroblastomaC. Burkitt lymphomaD. Renal Cell carcinoma
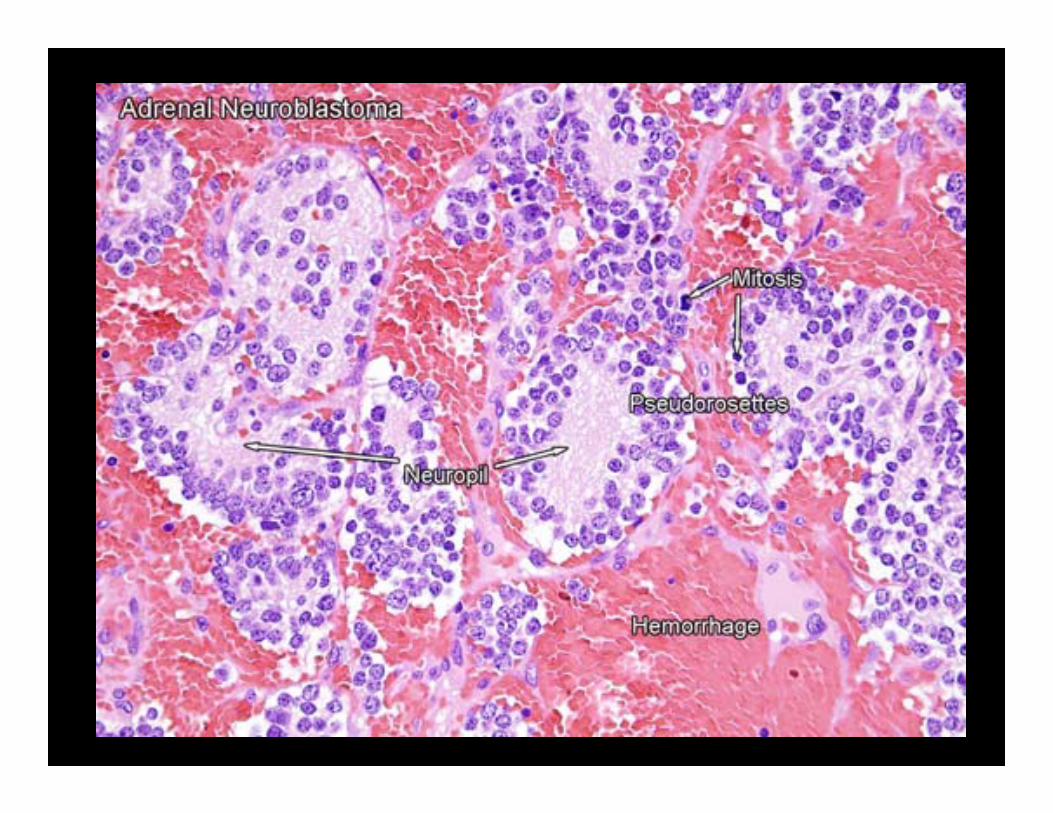


Case 25BThe tumor in this case would show:
A. C-myc overexpressionB. Triphasic growth patternC. Homer-Wright pseudorosettesD. Small blue cells and stromaE. WT-1 gene deletion
Case 26Adrenocorticocarcinomas are identified as
malignant by:
A. Nuclear atypiaB. Mitotic countC. Nucleoli countD. MetastasisE. Size


Case 27Wilm’s Tumor is identified by:
A. Homer Wright RosettesB. ProcalcitoninC. Small blue cells and neuropilD. Tubules, stroma and blastemaE. N-myc overexpression
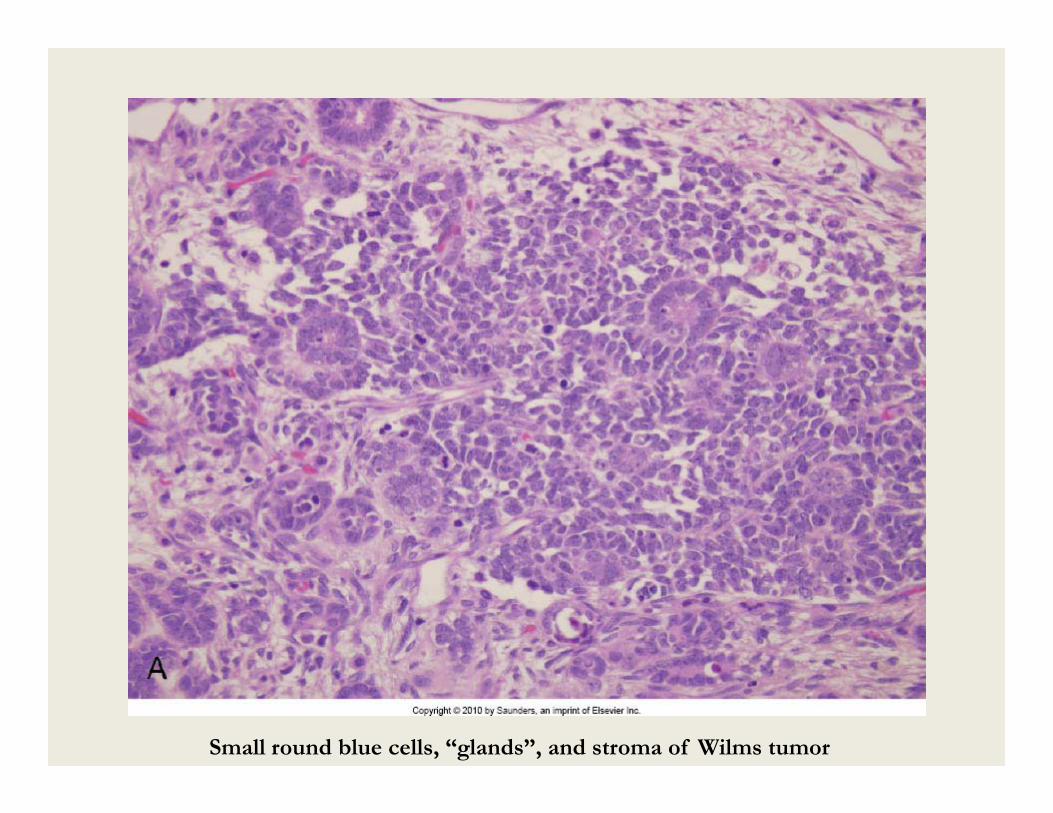
Small round blue cells, “glands”, and stroma of Wilms tumor

Wilms: blastema (blue cells); epithelium (tubules); stroma (with nuclei)
MEN Syndromes
• MEN I (Wermer syndrome)– 3 P’s = pituitary, pancreas, and parathyroid– May manifest as Zollinger-Ellison syndrome– MEN1 gene mutation
MEN Syndromes Cont.
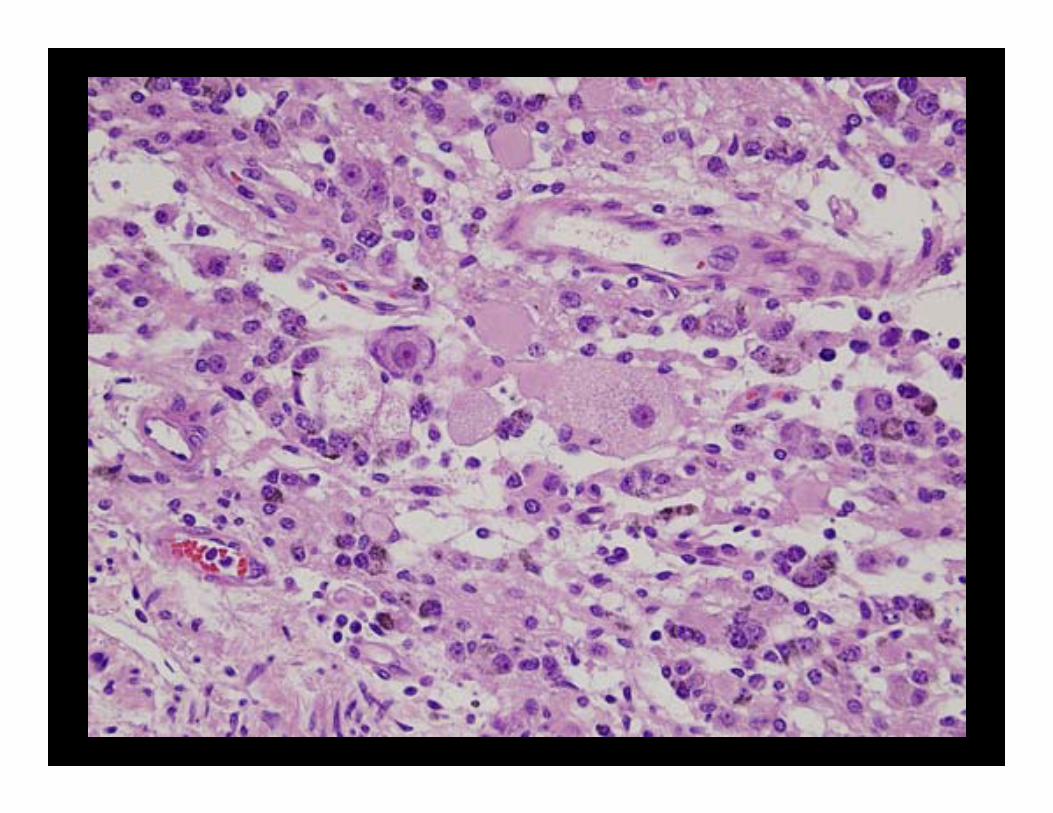
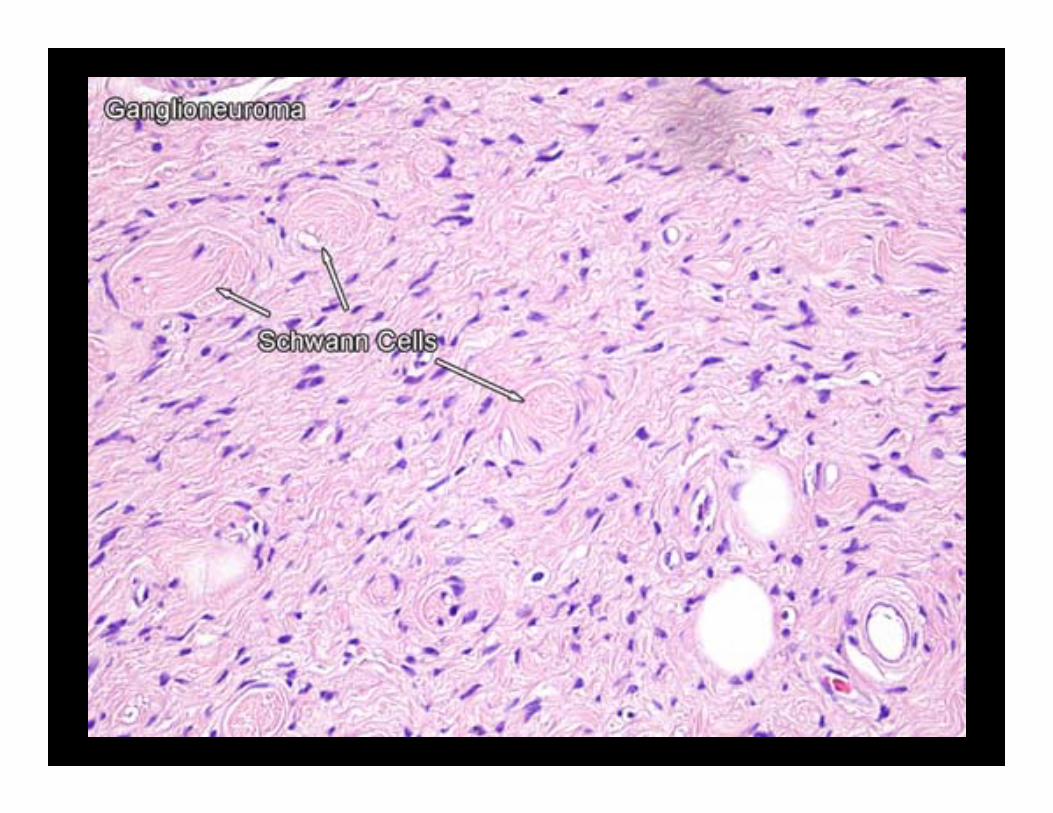
• MEN IIa (Sipple syndrome)– Pheochromocytoma– Thyroid medullary carcinoma– Parathyroid hyperplasia or tumor– Ret oncogene mutation
• MEN IIb (MEN III)– No parathyroid hyperplasia or tumor– Pheochromocytoma– Thyroid medullary carcinoma– Mucocutaneous neuromas or ganglioneuromas– Ret oncogene mutation

















