44
BY: DR RAM RAKSHA PAL FNB ( MAS ) RESIDENT Energy devices in surgery
| Date post: | 14-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | ram-raksha |
| View: | 289 times |
| Download: | 4 times |

BY: DR RAM RAKSHA PALFNB(MAS) RESIDENT
Energy devices in
surgery

HISTORY
Use of electrocautery (FIRE DRILL)is
described in ancient medicine ,3000
BC
In 1881, morton: electric current in
100,000 Hz does not produce shock
Bovie made first electrosurgical
generator


BASICS OF ELECTRICITY

TEMPERATURE VS TISSUE EFFECTS
45 degree C: collagen uncoils & may reanneal; covalent bonds b/w edges and fuse
60 degree C: irreversible protein denaturation, coagulation necrosis begins; blanching
80 degree C: carbonization begins; drying and shrinkage of tissues
90-100 degree C: complete cellular destruction by vaporization; plume of gas and smoke
125degree C: complete oxidation of protein & lipids; carbon residue & eschar formation

Standard electrical current: 60 Hz
Nerve and muscle stimulation
cease at: 100KHz
An electrosurgical generator takes
60 Hz current and increases its
frequency to over 200,000 Hz


ELECTROCAUTERY IS NOT ELECTROSURGERY
The terms electrocautery and electrosurgery are
frequently used interchangeably; however,
these terms define two distinctly different
modalities.
Electrocautery: use of electricity to heat an
object that is then used to burn a specific site
e.g. a hot wire
Electrosurgery: the electrical current heats the
tissue. The current must pass through the tissue
to produce the desired effect..
MONOPOLAR ELECTROSURGERY

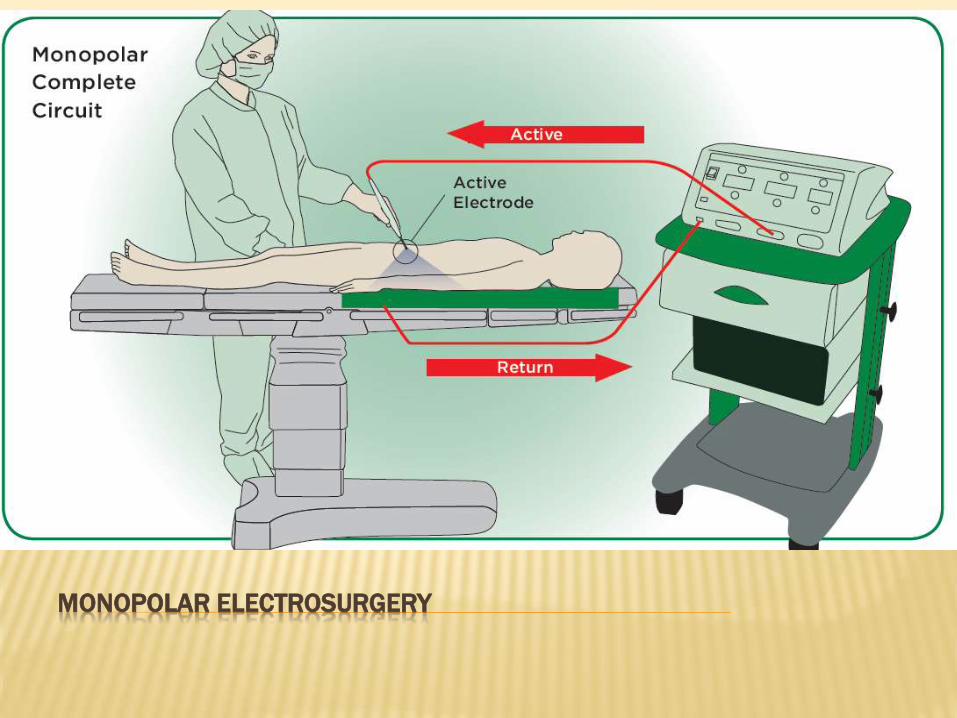
MONOPOLAR ELECTROSURGERY
Most commonly used electrosurgical
modality.
The active electrode is in the wound.
Patient return electrode is attached
somewhere else on the patient.
4 components: generator, active electrode,
patient, patient return electrode
Produce variety of tissue effects depending
on waveform

TISSUE EFFECTS WITH WAVEFORM MODIFICATION
Cut waveform: Duty cycle(“on” time) is high,
continuous waveform
vaporize or cut tissue,
Produce heat very rapidly
Coagulation waveform: intermittent waveform
Duty cycle (“on” time) reduced,
Produce less heat so coagulum is formed
Blended current : not a mixture of cutting and
coagulation, but a modification of duty cycle
Only variable that determine
vaporization or coagulation is rate of
heat
High heat, more rapidly : vaporization
Low heat, more slowly : coagulum

ELECTROSURGICAL TISSUE EFFECTS
Cutting: divide tissue with
electric sparks that focus intense
heat at surgical site
-By sparking we acheive maximum
current concentration
Fulguration: sparking with
coagulation waveform
-coagulates and chars the tissue
over a wide area, result in coagulum
-high voltage coag current is
used(duty cycle 6%)

ELECTROSURGICAL TISSUE EFFECTS
Desiccation: occurs when electrode is in direct
contact with the tissue
--Achieved most efficiently with cutting current
--by touching electrode to the tissue, current
concentration reduced, result in less heat and no
cutting action
--cells dry out and form a coagulum

We can cut with coag current and
coagulate with cutting current.
Benefit of coagulating with cutting
current is that we use far less voltage.
it has important implications in MIS
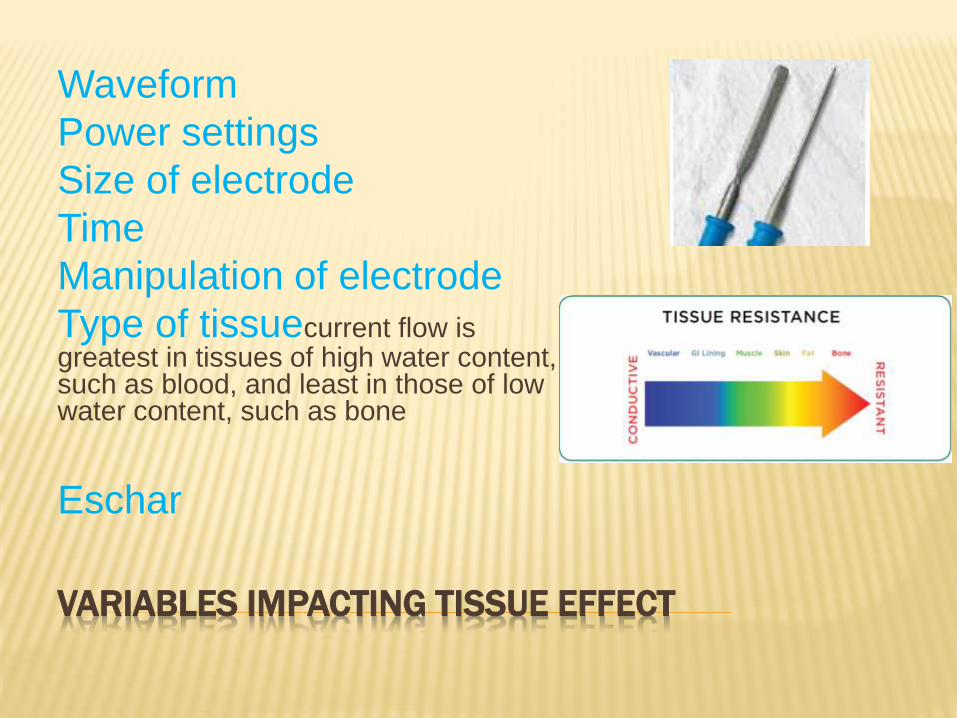
VARIABLES IMPACTING TISSUE EFFECT
Waveform
Power settings
Size of electrode
Time
Manipulation of electrode
Type of tissuecurrent flow is greatest in tissues of high water content, such as blood, and least in those of low water content, such as bone
Eschar

ELECTROSURGICAL GENERATORS
two types of electrosurgical generators:
• Ground referenced generators (typically
older, outdated units)
• Isolated generators (today’s state-of-art
technology)

GROUNDED ELECTROSURGICAL SYSTEMS
The current passes through the patient and returns to the generator, which is linked to ground.
The problem is the current can go to any grounded object other than the pateientreturn electrode (ECG electrodes, OR bed, metal objects) and cause alternate site burns.
outdated technology
Current division:
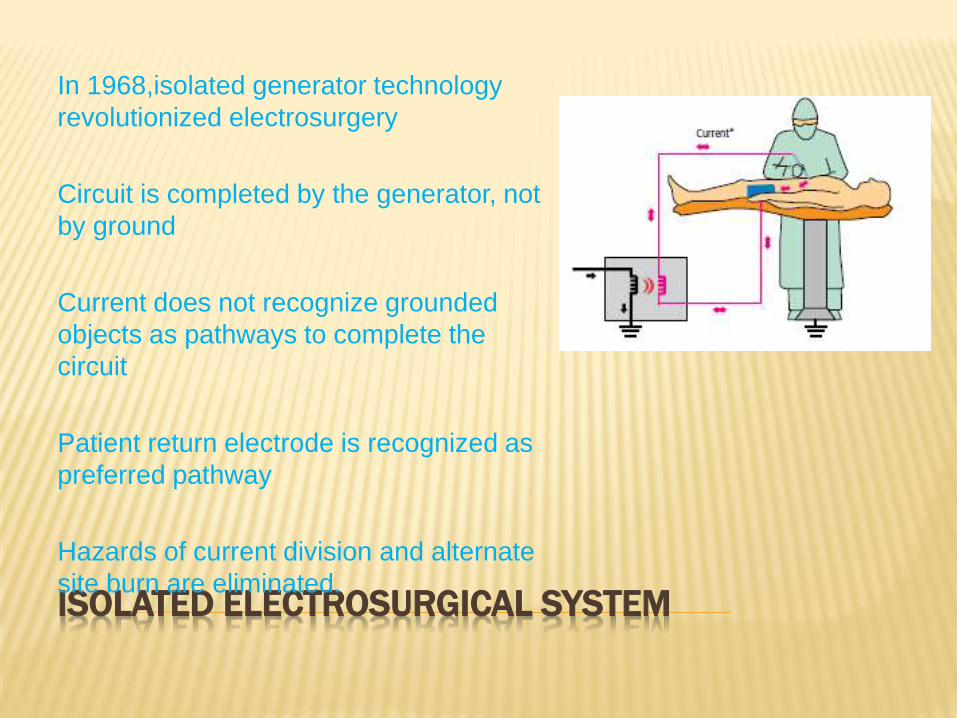
ISOLATED ELECTROSURGICAL SYSTEM
In 1968,isolated generator technology
revolutionized electrosurgery
Circuit is completed by the generator, not
by ground
Current does not recognize grounded
objects as pathways to complete the
circuit
Patient return electrode is recognized as
preferred pathway
Hazards of current division and alternate
site burn are eliminated.

ISOLATED ELECTROSURGICAL SYSTEM
Generators with isolated circuits do not
protect from return electrode site burn
A return electrode burn occurs when the
heat produced, over time, is not safely
dissipated by the size or conductivity of
the patient return electrode.

PATIENT RETURN ELECTRODE
The only difference b/w active
electrode and patient return electrode
is their relative size and conductivity
At patient return electrode site:
reduced contact area- current
concentration increased- temperature
increased- burn
surface area impedance can be
increased by excessive hair, adipose
tissue, bony prominences, fluid
invasion, adhesive failure, scar tissue

PATIENT RETURN ELECTRODE MONITORING TECHNOLOGY
REM contact quality monitoring(RECQM)
-protects patient from pad site burn
-monitor impedance at the patient/pad
interface
-system deactivate if impedance is high
-such electrode can be identified by its split
appearance i.e. two separate areas and a
special plug with center pin.

INSTANT RESPONSE TECHNOLOGY


SAFETY CONSIDERATIONS DURING MIS
Direct Coupling
occurs when the active electrode touches another metal instrument.
The electrical current flows from one to the other and then proceeds to tissue resulting in unintended burn.
This can also occur if an active electrode is activated while in contact with a metal clip.
So, do not activate the generator while the active electrode is touching a metal object or not in vision.


INSULATION FAILURE
Insulation failure can occur when the insulation covering of an endoscopic instrument has been damaged
Cracks or breaks in the shaft’s insulation allow the electrical energy to escape and burn unintended tissue.
The insulation of endoscopic instruments must be inspected before, during and after each use
Most damage to insulation occurs during instrument processing, specifically during sterilization. Heat with subsequent cooling causes insulation to shrink and then expand. During this process cracks and breaks can occur.

INSULATION FAILURE
Coagulation waveform is high in
voltage, which can spark
through compromised
insulation. Also high voltage can
blow holes in weak insulation.
We can get the desired
coagulation effect without high
voltage , simply by using the
‘cutting’ current by holding the
electrode in direct contact with
tissue

CAPACITIVE COUPLING
During MIS procedure, an inadvertent capacitor may be
created by the surgical instruments
An electrostatic field created b/w two conductors,
resulting induced current in second conductor
Hybrid cannula are worst , metal part will create a
capacitor but plastic anchor will prevent the current
from dissipating through abd wall.This current may exit
to some adjacent tissue, result in significant injury
Use the lowest power setting
Use the lower voltage setting such as “Cut,” rather than
“Coag” or “Spray Coag.”
Keep the electrode eschar free
Use larger diameter trocars and smaller diameter
electrodes

ACTIVE ELECTRODE MONITORING
shielded and monitored instruments continuously direct stray energy, away from the patient via a protective shield.
When insulation failure occurs or capacitively coupled energy reaches dangerous levels, the electrosurgical unit (ESU) shuts down automatically and the surgical staff are alerted.
AEM system detects even the smallest full thickness insulation breaks on Laparscopic instruments, virtually eliminating accidental burns due to faulty insulation, saving costs and reducing the possibility of patient injury.

BIPOLAR ELECTROSURGERY
The two tines forceps
function active and return
electrodes.
Only the tissue grasped is
included in circuit.
No patient return electrode
Better hemostasis
Less thermal injury
Safer than monopolar

RECOMMENDATIONS TO AVOID
ELECTROSURGICAL COMPLICATIONS IN MIS
Inspect insulation carefully
Use lowest possible power settings
Use a low voltage waveform(cut)
Use brief intermittent activation vs prolonged
activation
Do not activate in open circuit
Do not activate in close proximity or direct
contact with other instrument

RECOMMENDATIONS TO AVOID
ELECTROSURGICAL COMPLICATIONS IN MIS
Use bipolar electrosurgery when
appropriate
Do not use hybrid canula. Select an all
metal canula system as the safest
choice.
Active electrode monitoring system: to
avoid problems of insulation failure and
capacitive coupling

VESSEL SEALING TECHNOLOGY
•Combination of pressure and energy
to create a seal.
•Feedback controlled output so
reliable seal in minimal time
•Seals vessels up to 7 mm with a
single activation.
•Seal strength comparable to
sutures/clips, can withstand >3 times
normal SBP.
•Lateral thermal spread :
-ligasure: 0 - 4.5 mm
-enseal trio: 1 mm
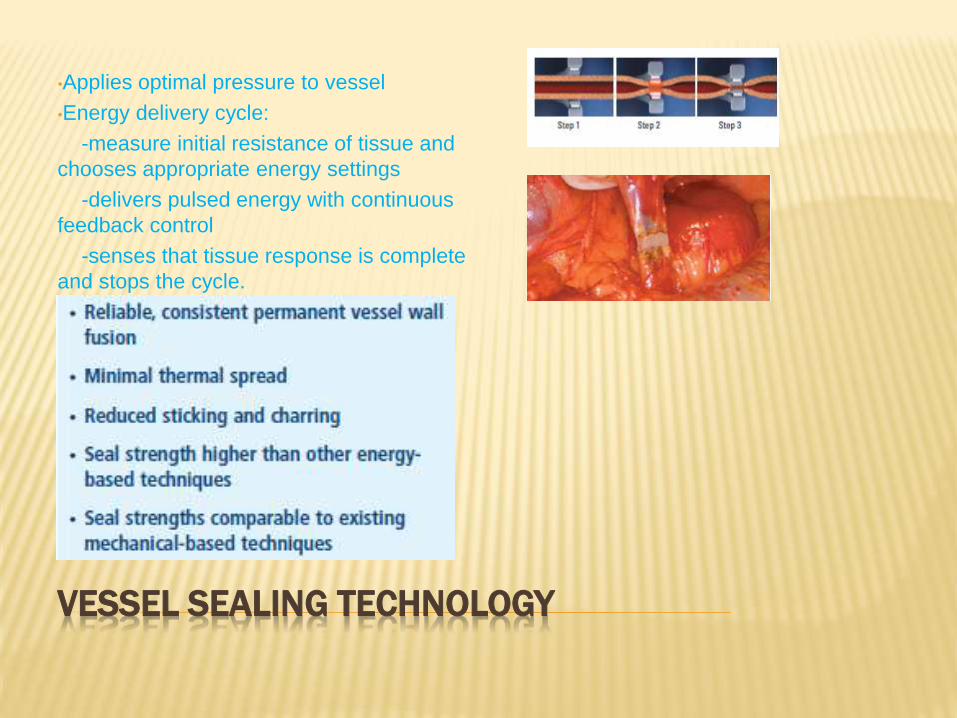
VESSEL SEALING TECHNOLOGY
•Applies optimal pressure to vessel
•Energy delivery cycle:
-measure initial resistance of tissue and
chooses appropriate energy settings
-delivers pulsed energy with continuous
feedback control
-senses that tissue response is complete
and stops the cycle.

ULTRASONIC ENERGY DEVICES
Ultrasonic shears employ both compression and friction to deliver mechanical energy to target tissue
Amino acids unwind and reshape and hydrogen bonds break resulting in sticky coagulum
Ultrasonic shears contain piezoelectric diskes, that converts electric energy into mechanical energy which is amplified by silicone element
Instrument blade vibrate at 55500 hz along the long axis
Safely coagulates and transect vessels upto 5 mm


ULTRASONIC ENERGY DEVICES
• provide excellent hemostasis, efficient
transection, minimal lateral thermal damage,
low smoke generation, and no risk of
electrical current passage to the patient.
• optimization of the energy delivery during
application can improve them further


HARMONIC ACE+ SHEARS
The new Adaptive Tissue
Technology
achieving better control of
energy delivery to the tissue,
seals vessels with supra-
physiological burst pressures,
low thermal damage.

THUNDERBEAT
THUNDERBEAT is
integration of both bipolar
and ultrasonic energies
delivered simultaneously
from a single versatile
instrument.
benefits of each individual
energy; the ability to rapidly
cut tissue with ultrasonic
energy; and the ability to
create reliable vessel seals
with bipolar energy.


THUNDERBEAT
THUNDERBEAT provides
unprecedented
versatility, including:
· Reliable 7 mm vessel
sealing
· Minimal thermal spread
· Quickest in-its-class
cutting
· Reduced mist generation
for improved visibility
· Fine dissection with fine
jaw design
· Fewer instrument
exchanges Revolutionary
jaw design

ARGON ENHANCED ELECTROSURGERY

CAVITRON ULTRASONIC SURGICAL ASPIRATOR(CUSA)
CUSA is a dissecting device that uses ultrasonic
frequencies to fragment tissue.
Utilizing a hollow titanium tip that vibrates along its
longitudinal axis, fragmentation of susceptible tissue
occurs while concurrently lavaging and aspirating
material from the surgical site.
The CUSA selectively ablates tissues with high water
content such as liver parenchyma, glandular, and
neoplastic tissue.
This instrument is most useful when removing
purportedly “non-resectable” brain and spine tumors.
With a gentle wand-like motion, the CUSA enables a
“layer by layer” surgical excision without affecting vital
structures

















