24
Enfermedad cerebro vascular Neurología
| Date post: | 02-Aug-2015 |
| Category: |
Documents |
| Upload: | mi-rincon-de-medicina |
| View: | 979 times |
| Download: | 4 times |
Enfermedad cerebro vascular
Neurología
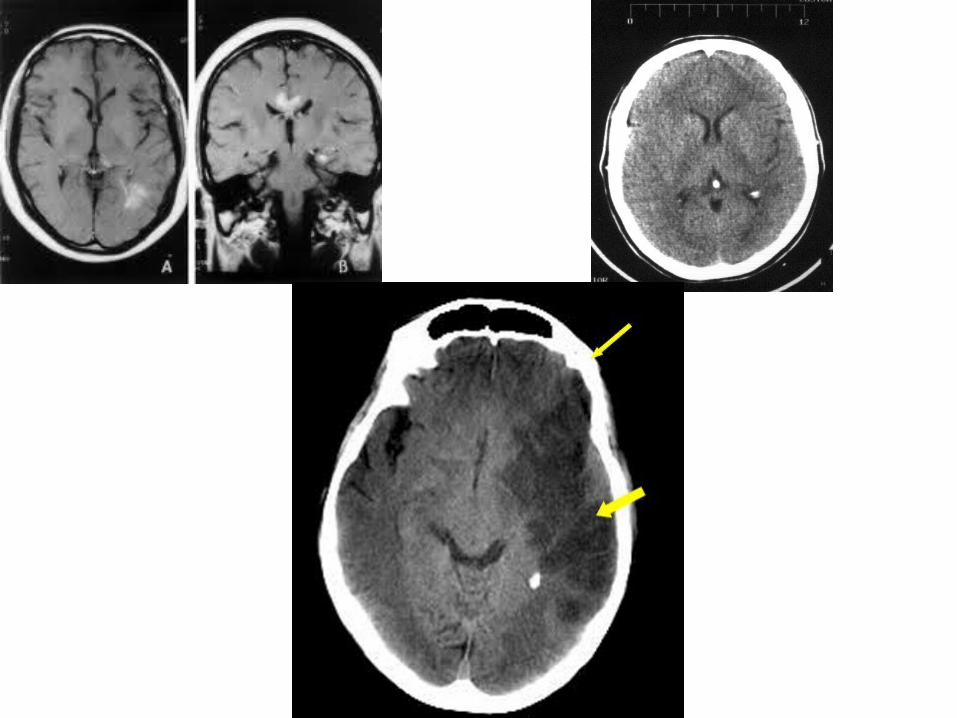
• Stroke is characterized by the sudden loss of blood circulation to an area of the brain, resulting in a corresponding loss of neurologic function.
• Also previously called cerebrovascular accident (CVA) or stroke syndrome, stroke is a nonspecific term encompassing a heterogeneous group of pathophysiologic causes, including thrombosis, embolism, and hemorrhage.
Epidemiologia
• 750,000 nuevos casos cada ano.• 3era causa de muerte.• 1era causa de discapacidad en adultos• 160,000 muertes cada ano.• Sobrevivientes, 30% requieren asistencia de la
vida diaria• 20% asistencia con ambulación• 16% cuidados institucional.• Costo financiero y humano (41 billones).
Factores de riesgo
Modificables • HTA• DM• Dislipidemia• Enfermedad cardiaca• Tabaco• Alcohol• Índice de masa corporal
No modificables• Edad• Masculino• Raza negra• Nivel socioeconómico bajo• Historia familiar• Microcirculacion• Medioambiental
• Less common causes of thrombosis include polycythemia, sickle cell anemia, protein C deficiency, fibromuscular dysplasia of the cerebral arteries, and prolonged vasoconstriction from migraine headache disorders.
• The sources of cardiogenic emboli include valvular thrombi (eg, in mitral stenosis, endocarditis, prosthetic valve), mural thrombi (myocardial infarction [MI], atrial fibrillation [AF], dilated cardiomyopathy, severe congestive heart failure [CHF]), and atrial myxoma.
• MI is associated with a 2-3% incidence of embolic stroke, of which 85% occur in the first month after MI.
• Stroke symptoms can result from inadequate cerebral blood flow due to decreased blood pressure (and specifically decreased cerebral perfusion pressure) or due to hematologic hyperviscosity due to sickle cell disease or other hematologic illnesses such as multiple myeloma and polycythemia vera. In these instances, cerebral injury may occur in the presence of damage to other organ systems.
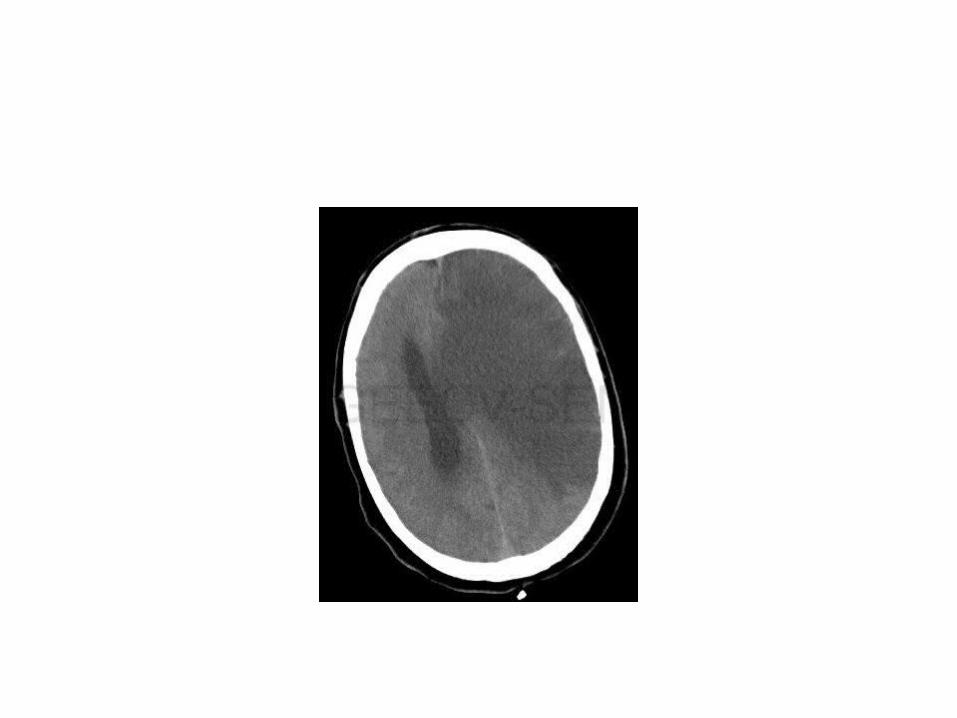
• Stroke should be considered in any patient presenting with an acute neurologic deficit (focal or global) or altered level of consciousness.
• No historical feature distinguishes ischemic from hemorrhagic stroke, although nausea, vomiting, headache, and change in level of consciousness are more common in hemorrhagic strokes.
• Common symptoms of stroke include abrupt onset of hemiparesis, monoparesis, or quadriparesis; monocular or binocular visual loss; visual field deficits; diplopia; dysarthria; ataxia; vertigo; aphasia; or sudden decrease in the level of consciousness.
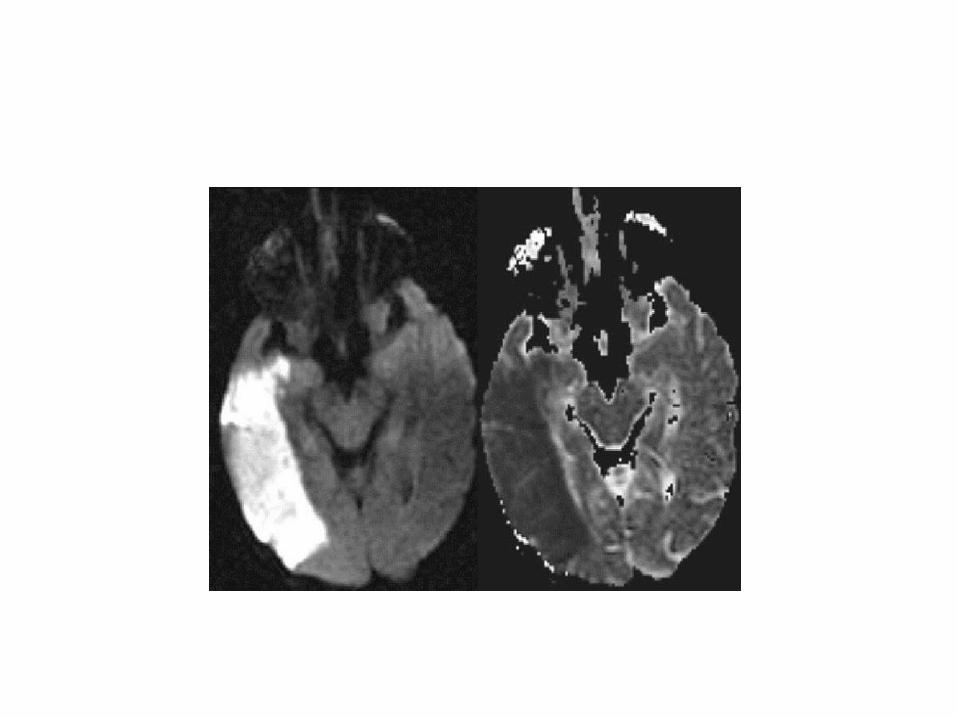
Fisiopatologia
• Interrupcion completa de flujo sanguineo cerebral causa supresion de la actividad electrica en 12-15 segundos, inhibicion de excitabilidad sinaptica de neuronas corticales despues de 2-4 minutos e inhibicion de excitabilidad electrica despues de 4-6 minutos.
• El flujo sanguineo cerebral normal es de 50-55 mL/100 gr/minuto y la tasa metabolica cerebral de oxigeno es de 165 mmol/100 gr/minuto.
• Cuando el flujo sanguineo disminuye a 18 mL/100 gr/minunto el uumbral electrico falla. Aunque estas neuronas no estan normalmente funcionando son potencialmente recuperables.
• El segundo nivel conocido como umbral de fallo de membrana ocurre cuando el flujo sanguineo disminuye a 8 mL/100 gr/minuto. Resultando en muerte celular. Este es el nivel de penumbra o pobre perfusion.
Arteria cerebral media• Middle cerebral artery (MCA) occlusion commonly
produces contralateral hemiparesis, contralateral hypesthesia, ipsilateral hemianopsia, and gaze preference toward the side of the lesion.
• Agnosia is common, and receptive or expressive aphasia may result if the lesion occurs in the dominant hemisphere.
• Neglect, inattention, and extinction of double simultaneous stimulation may occur in nondominant hemisphere lesions.
• Since the MCA supplies the upper extremity motor strip, weakness of the arm and face is usually worse than that of the lower limb.
Arteria cerebral anterior
• primarily affect frontal lobe function and can result in dis-inhibition and speech perseveration, producing primitive reflexes (grasping, sucking reflexes), altered mental status, impaired judgment, contralateral weakness (greater in legs than arms), contralateral cortical sensory deficits gait apraxia, and urinary incontinence.
Arteria cerebral posterior
• Posterior cerebral artery occlusions affect vision and thought, producing contralateral homonymous hemianopsia, cortical blindness, visual agnosia, altered mental status, and impaired memory.
• Vertebrobasilar artery occlusions are notoriously difficult to detect because they cause a wide variety of cranial nerve, cerebellar, and brainstem deficits.
• These include vertigo, nystagmus, diplopia, visual field deficits, dysphagia, dysarthria, facial hypesthesia, syncope, and ataxia.
• A hallmark of posterior circulation stroke is that there are crossed findings: ipsilateral cranial nerve deficits and contralateral motor deficits.
• This is contrasted to anterior stroke, which produces only unilateral findings.
Transient ischemic attack
– Transient ischemic attack (TIA) has come to be known as a neurologic deficit that resolves within 24 hours. Roughly 80% resolve within 60 minutes. Tissue-based definitions are being proposed with magnetic resonance imaging.
– TIA can result from any of the aforementioned mechanisms of stroke. Data suggest that roughly 10% of patients with TIA suffer stroke within 90 days and half of these patients suffer stroke within 2 days
Ataque isquémico transitorio
• 80% circulación carotidea• 20% vertebro basilar• Es un indicador pronostico de Stroke• 1/3 de TIA no tratados tendrán ACV en 5 anos• Eventos cardiacos son principal causa de
muerte en TIA.• 5-6% mortalidad anual después de un TIA es
causada principalmente por IAM
• TIA es un deficit neurologico focal, temporal y de inicio subito; relacionado a isquemia del cerebro, retina o coclea, y dura por lo menos 24 horas.
• Cefalea es un sintoma frecuente.• Sintomas tipicos:• Amaurosis fugaz ipsilateral• Deficit motor o sensitivo contralateral• Afasia• Hemianopsia homonima contralateral• diplopia aislada, vertigo, disfagia y disartria no deben de
ser consideradas TIA, a menos que sean combinadas con otros sintomas.
Diagnostico diferencial de TIA
• Lesiones ocupantes de espacio• HSA, intraparenquimatosa y subdural.• Convulsiones• Hipoglucemia• Migrañas• Sincopes• Desordenes laberinticos.
Síndrome Lacunar
• Isquemia debida a enfermedad arterial penetrante o pequeños vasos.
• Pequeños infartos isquémicos en regiones profundas del cerebro y tallo cerebral de 0.5-15 mm.
• 13-20% de todos los infartos.• Oclusión de arterias penetrante como CoA, CM, CP y
basilar.• También por arterioesclerosis o micro embolismo.• Pueden ser únicos, múltiples, sintomáticos o
asintomáticos.
Tipos o síndromes lacunares• Hemiparesis motora pura• Sensitivo puro• Sensitivo motor• Ataxia y paresis crural• Disartria mano torpe.• Asociado con déficit cognitivo adquirido.• La cefalea es infrecuente.
Síntomas • 1. Capsula interna, base del puente o corona radiata. Caracterizada
por hemiplejia contralateral completa acompañada de disartria. No puede haber afasia, agnosia ni síntomas visuales o sensitivos.
• 2. Núcleo VPL del tálamo. Hay parestesias, hormigueo y déficit sensitivo contralateral que afecta cara, brazo, tronco y pierna.
• 3.Capsula interna y tálamo, o brazo posterior de capsula interna. Existe déficit motor contralateral con déficit sensitivo superimpuesto.
• 4. Brazo posterior contralateral de capsula interna o base del puente. Caracterizado por debilidad en miembro inferior e incoordinación ipsilateral de la mano y el pie.
• 5. Áreas profundas del puente caracterizado por debilidad facial supranuclear, disartria, disfagia, perdida del control motor fino de la mano y signo de Babinski.
Síndromes del sistema arterial carotideo.
• Amaurosis fugaz perdida monocular de la visión de inicio súbito, duración 1-5 minutos, menos de 30, debido a disminución del flujo sanguíneo de la retina. Luego visión restaurada completamente.
• Descrito en 15-20% de pacientes.• Infarto ACM• Hemiplejia contralateral• Desviación conjugada de la mirada hacia el lado del infarto.• Hemianestesia• Hemianopsia homónima• Afasia global y hemineglect si es hemisferio dominante.• Lesión de ACM, hemiplejia predomina en cara y brazo mas que en
miembro inferior.• Afasia de Broca, de Wernicke en lado dominante.• Alexia, agrafia lesión en gyrus angular izquierdo
• Síndrome de Gerstmann: agnosia, acalculia, agrafia y desorientación derecha-izquierda.
• Lesión parietal en hemisferio dominante.• Anosognosia, inatención, apraxia, confusión y agitación en
hemisferio derecho.• ACA son infrecuentes los infartos (HSA), 3%.• Debilidad del miembro inferior contralateral, abulia, mutismo
akinetico, alteración de memoria y conducta.• Desviación de cabeza y ojos hacia el lado de la lesión.• Perdida de sensibilidad propioceptiva y discriminativa en miembros
inferiores.• Incontinencia de esfínter, síndrome de desconexión anterior.
Tratamiento • Emergency Department Care• Airway and breathing• Circulation • Blood glucose control (90-140 mg/dL)• Head positioning • Blood pressure control • Fever control • Cerebral edema control occurs in up to 15% of patients with ischemic
stroke• Seizure control occur in 2-23% within the first days after stroke. Although
seizure prophylaxis is not indicated, prevention of subsequent seizures with standard antiepileptic therapy is recommended.12
• Acute decompensation or escalation