52
Enrico Romagnoli MD, PhD Interventional Cardiology Unit, San Raffaele Hospital, Milan Torino 14 Novembre 2007 DRUG-ELUTING STENTS: DRUG-ELUTING STENTS: WHICH AND TO WHOM? WHICH AND TO WHOM?
| Date post: | 29-Dec-2015 |
| Category: |
Documents |
| Upload: | simon-aldous-howard |
| View: | 217 times |
| Download: | 0 times |
Enrico Romagnoli MD, PhDInterventional Cardiology Unit,
San Raffaele Hospital, Milan
Torino14 Novembre 2007
DRUG-ELUTING STENTS: DRUG-ELUTING STENTS: WHICH AND TO WHOM?WHICH AND TO WHOM?
DES & restenosis
Drug-eluting stents represent a major advance Drug-eluting stents represent a major advance for reduction of restenosisfor reduction of restenosis
Drug-eluting stents consistently have been shown Drug-eluting stents consistently have been shown to reduce the amount of to reduce the amount of late lumen loss late lumen loss in months in months following implantation represent a major advance following implantation represent a major advance for reduction of restenosis, compared to bare for reduction of restenosis, compared to bare metal stentmetal stent
This difference translated in a marked reduction This difference translated in a marked reduction in in restenosis rate restenosis rate and need for and need for target vessel target vessel revascularizationrevascularization in randomized controlled trials in randomized controlled trials
DES caveat
Early DES trials were performed in low-risk population
End-points (usually late loss) were considered as the surrogate of clinical events
Routine Angiographic follow-up not clinically driven
DES versus BMS of similar design (not necessarily the best BMS)
DES trials vs. DES registry
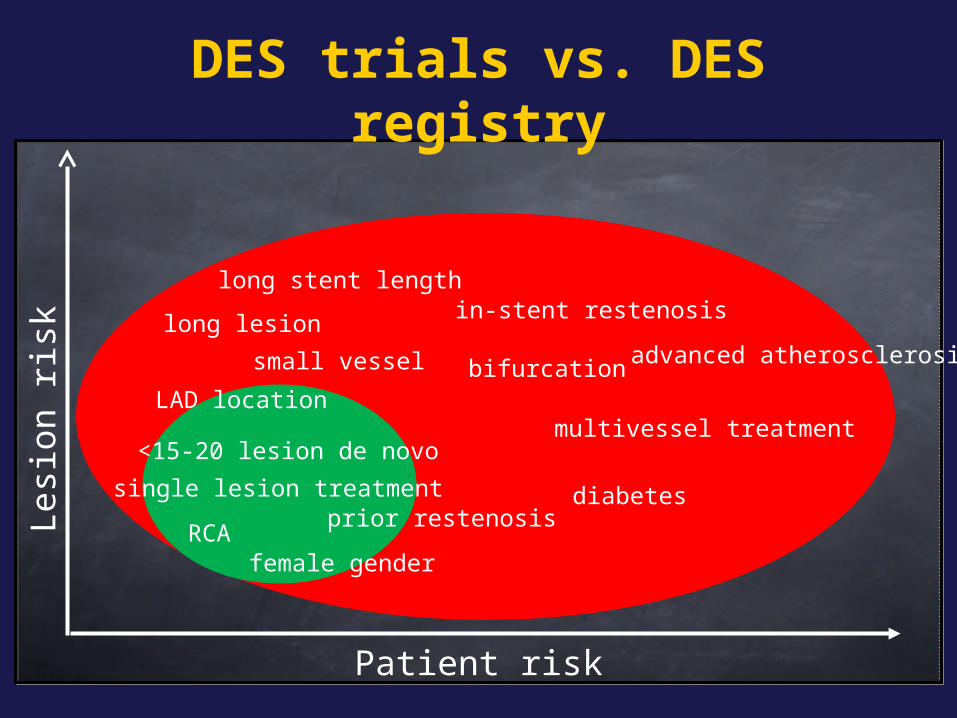
LAD location
single lesion treatmentprior restenosis
female genderRCA
<15-20 lesion de novo
small vessel
long lesion
long stent lengthin-stent restenosis
bifurcation
multivessel treatment
advanced atherosclerosis
diabetes
Patient risk
Lesi
on
ris
k
DES caveat
Early DES trials were performed in low-risk population
End-points (usually late loss) were considered as the surrogate of clinical events
Routine Angiographic follow-up not clinically driven
DES versus BMS of similar design (not necessarily the best BMS)
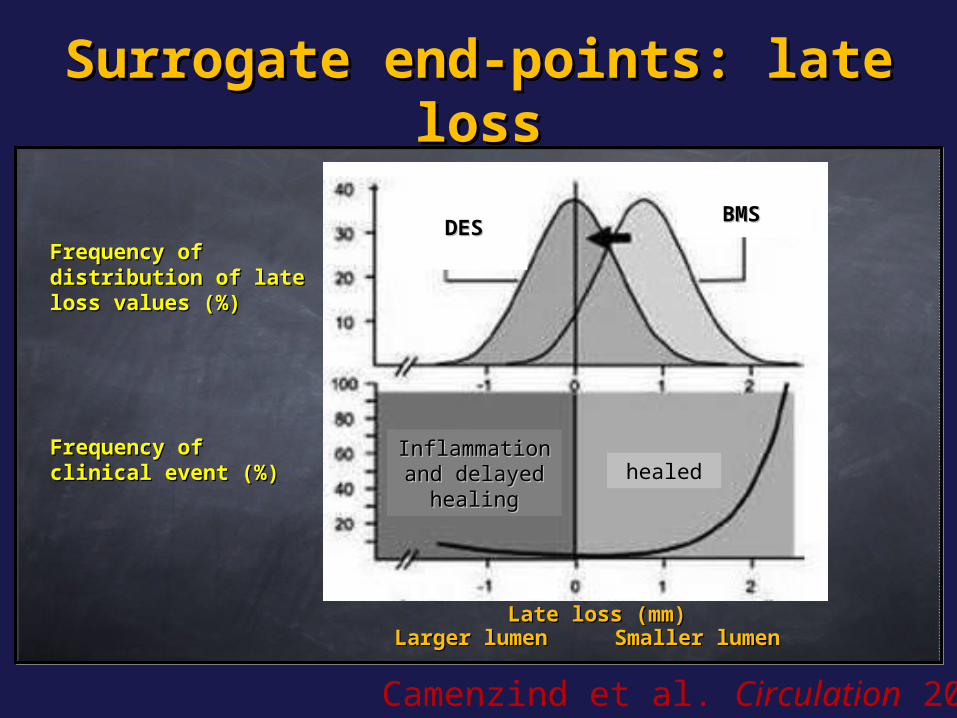
Surrogate end-points: late Surrogate end-points: late lossloss
Camenzind et al. Circulation 2007
Frequency of Frequency of distribution of late distribution of late loss values (%)loss values (%)
Frequency of Frequency of clinical event (%)clinical event (%)
Larger lumenLarger lumen Smaller lumenSmaller lumenLate loss (mm)Late loss (mm)
DES DES
BMSBMS
healedhealedInflammation Inflammation and delayed and delayed
healinghealing

There is no evidence of correlation between angiographic late lumen loss and clinical events
The use of late loss as an end point tended to overestimate the difference in restenosis, and the derived effect seemed to be overemphasized with respect to the real risk.
We don’t know the real clinical effect of late loss and its reliability as an end-point in direct comparative drug-eluting stent trials
Surrogate end-points: late Surrogate end-points: late lossloss
Agostoni et al. Am J Cardiol. 2006
DES caveat
Early DES trials were performed in low-risk population
End-points (usually late loss) were considered as the surrogate of clinical events
Routine Angiographic follow-up not clinically driven
DES versus BMS of similar design (not necessarily the best BMS)

DES caveat
Early DES trials were performed in low-risk population
End-points (usually late loss) were considered as the surrogate of clinical events
Routine Angiographic follow-up not clinically driven
DES versus BMS of similar design (not necessarily the best BMS)

BASKET trialBASKET trialThe primary endpoint was cost-effectiveness after 6 months, with effectiveness defined as reduction of major adverse cardiac events
Total costs at 6 months were higher with DES € 10,544than with BMS € 9,639;
The higher stent costs of DES were not compensated for by lower follow-up costs
Kaiser C. Lancet 2005
p<0.0001
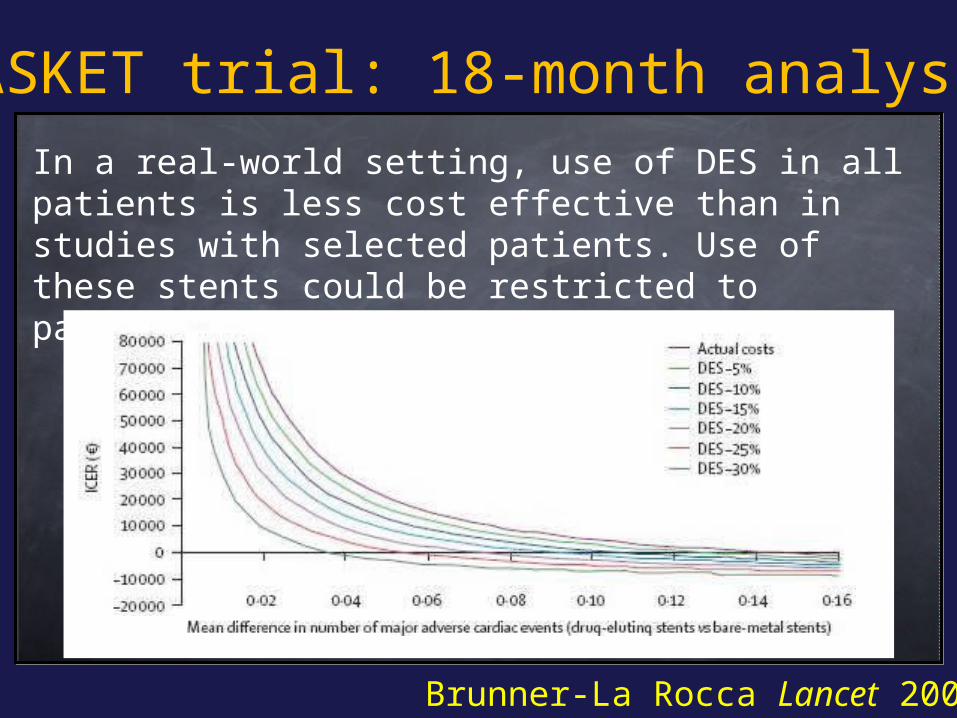
BASKET trial: 18-month analysisIn a real-world setting, use of DES in all patients is less cost effective than in studies with selected patients. Use of these stents could be restricted to patients in high-risk groups
Brunner-La Rocca Lancet 2007
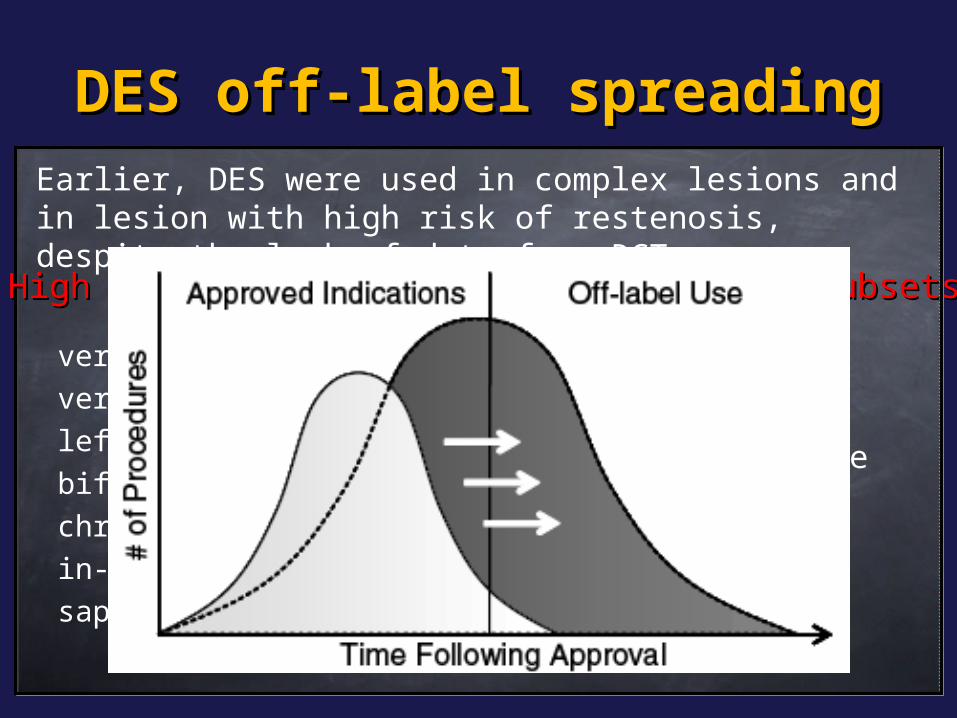
DES off-label spreadingDES off-label spreading
very small vessel/stent !very long lesion !left main diseasebifurcation lesionschronic total occlusion in-stent restenosis !!saphenous vein graft
acute myocardial infarction
multivessel diseasediabetics !!!severe LVEF dysfunctionrenal dysfunction
High risk patient subsetsHigh risk patient subsetsHigh risk lesion subsetsHigh risk lesion subsets
Earlier, DES were used in complex lesions and in lesion with high risk of restenosis, despite the lack of data from RCT
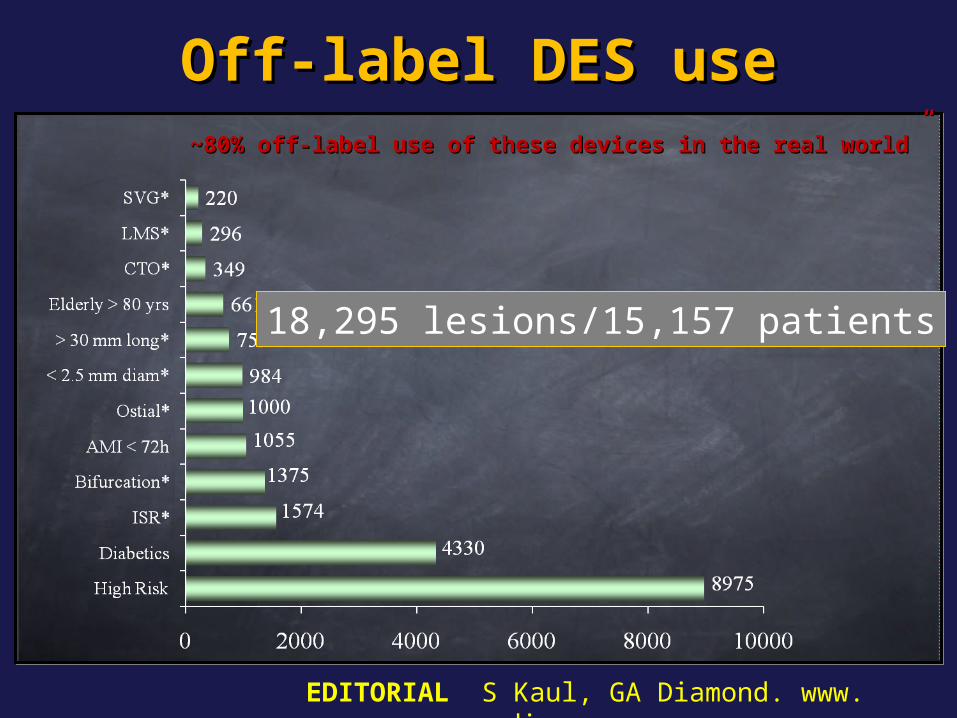
Off-label DES useOff-label DES use~80% ~80% off-label use of these devices in the real world”off-label use of these devices in the real world”
18,295 lesions/15,157 patients
EDITORIAL S Kaul, GA Diamond. www. cardiosource.com
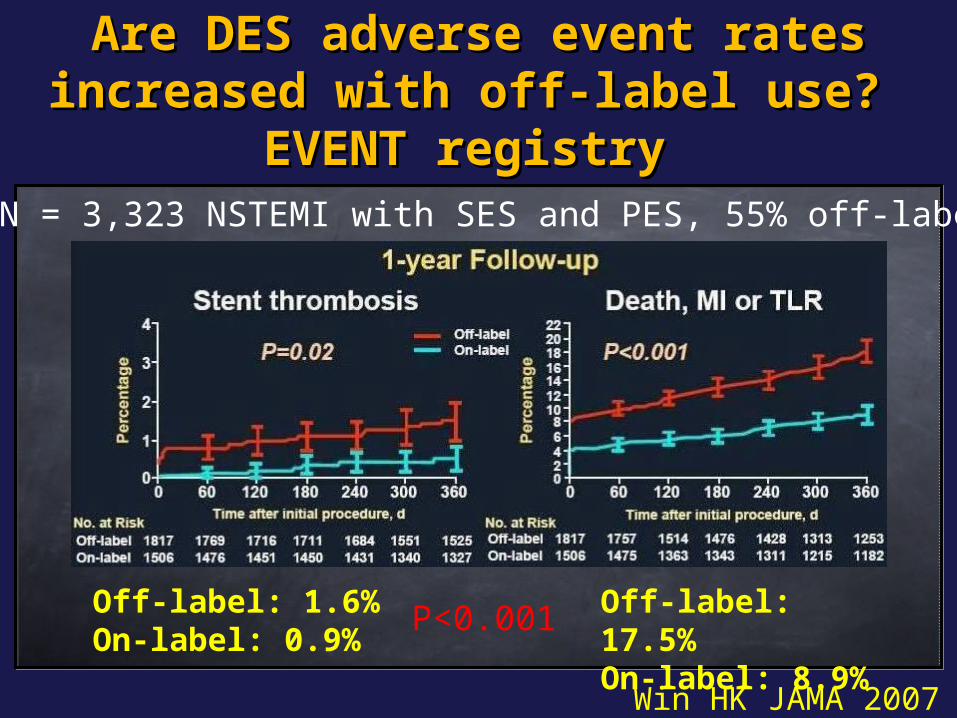
Are DES adverse event rates Are DES adverse event rates increased with off-label use? increased with off-label use?
EVENT registry EVENT registry N = 3,323 NSTEMI with SES and PES, 55% off-label
Off-label: 1.6%On-label: 0.9%
Off-label: 17.5%On-label: 8.9%
P<0.001
Win HK JAMA 2007
Off-label questionOff-label question
Is there any reason to assume that DES won’t work equally Is there any reason to assume that DES won’t work equally as well in other lesion subsets?as well in other lesion subsets?
Lack of approval is related to many factors: Lack of approval is related to many factors:
already widely used off-label (no commercial reason)already widely used off-label (no commercial reason)
logistically difficult to conduct study (no financial logistically difficult to conduct study (no financial reason)reason)
previous studies conducted did not meet the required previous studies conducted did not meet the required standards for approval standards for approval Off label use is not subject to a rigorous Off label use is not subject to a rigorous pre-market approval processpre-market approval process
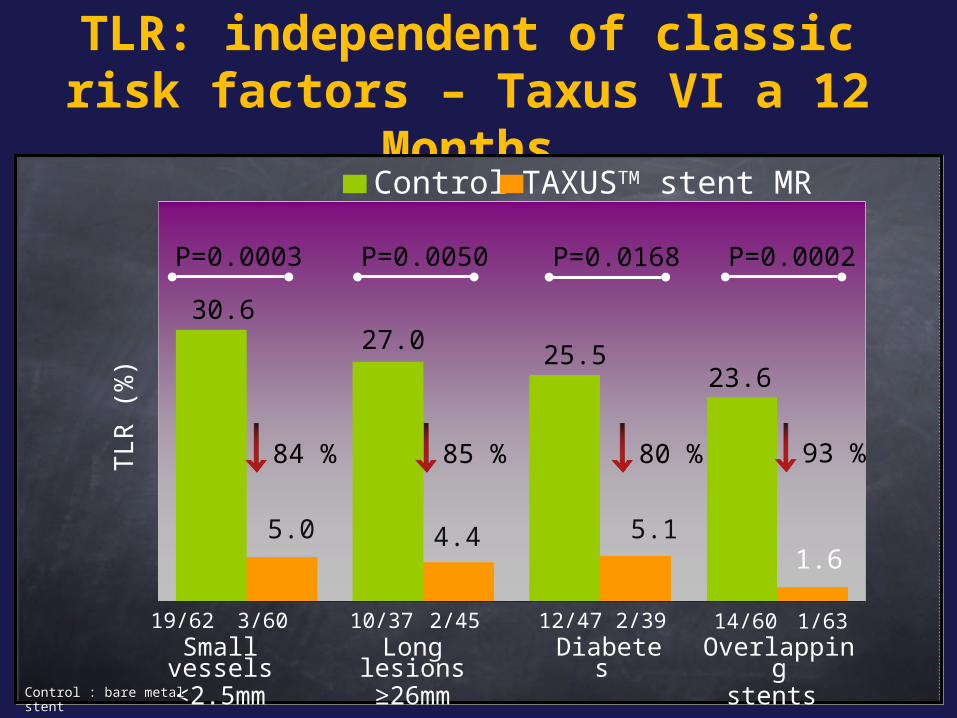
TLR: independent of classic risk factors – Taxus VI a 12 Months
P=0.0003 P=0.0050
TL
R (
%)
Control TAXUSTM stent MR
30.6
5.0
19/62 3/60
4.4
27.0
10/37 2/45
25.5
5.1
12/47 2/39
P=0.0002
Small vessels<2.5mm
Long lesions≥26mm
Diabetes
84 % 85 % 80 %
Overlappingstents
14/60 1/63
23.6
1.6
93 %
P=0.0168
Control : bare metal stentControl : bare metal stent
2006 DES storm
SCAAR SCAAR registry registry
Lagerqvist NEJM 2007 356;1009-19Lagerqvist NEJM 2007 356;1009-19
Cum
ula
tive R
isk
Cum
ula
tive R
isk
00 0.5 0.5 1.01.0 1.51.5 2.02.02.52.5
Time (years)Time (years)
RR: 1.32 (1.11-RR: 1.32 (1.11-1.57)1.57)
BMSBMSDESDES
BMSBMS 1288012880 1247312473 1235412354 1221312213 929892985960 5960
DESDES 57705770 56045604 55415541 54685468 3434343417761776
0.00.000
0.00.022
0.00.044
0.00.066
0.00.088
0.10.100
RR: 1.03(0.84-RR: 1.03(0.84-1.26)1.26)
3-year mortality increased 18% with DES
Stent registryStent registry
Wake forest experience
4.9%
7.1%
P = 0.03
Applegate AJC 2007
DES in OntarioDES in Ontario
Tu JV NEJM 2007Western Denmark Western Denmark registryregistry
Jensen LO JACC 2007
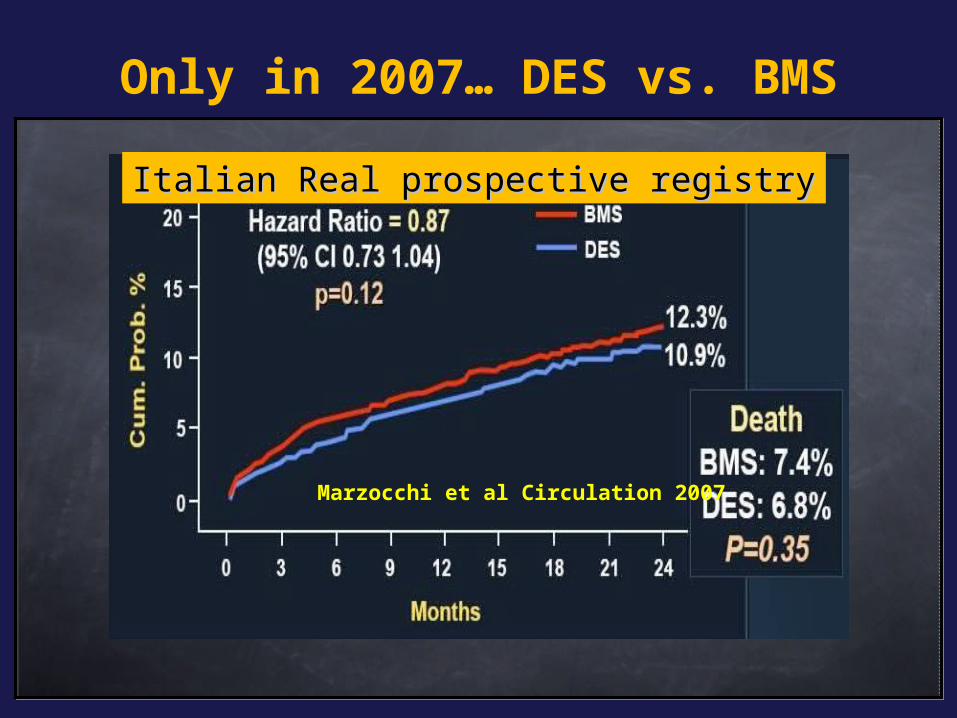
Marzocchi et al Circulation 2007
Italian Real prospective registryItalian Real prospective registry
Only in 2007… DES vs. BMS
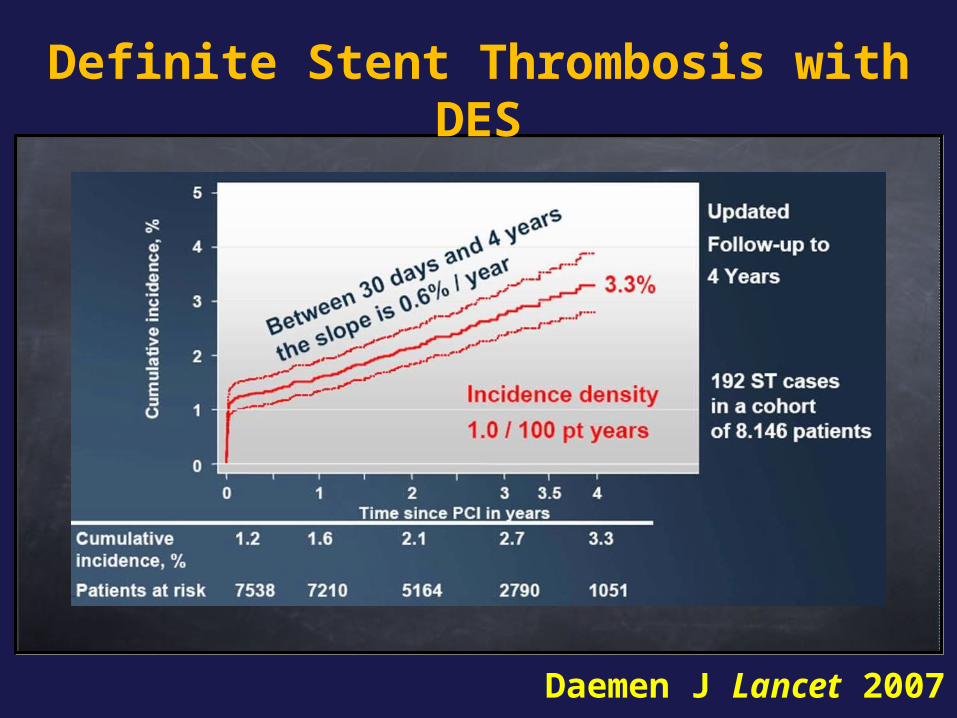
Definite Stent Thrombosis with DES
Daemen J Lancet 2007
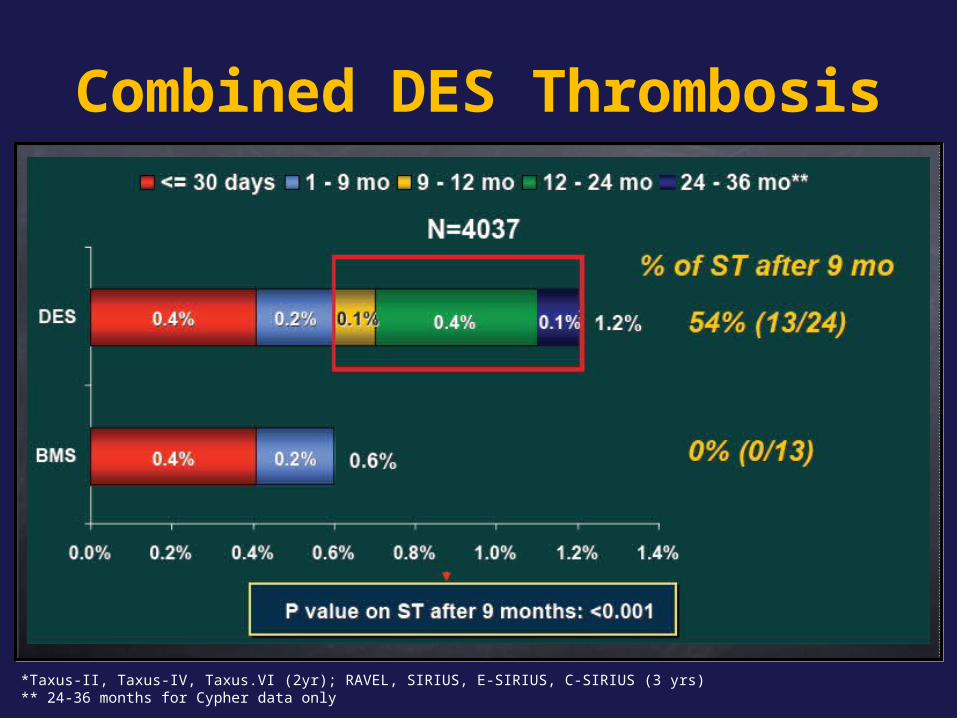
Combined DES Thrombosis
*Taxus-II, Taxus-IV, Taxus.VI (2yr); RAVEL, SIRIUS, E-SIRIUS, C-SIRIUS (3 yrs)** 24-36 months for Cypher data only

DES “a chi”?
• Thesis: Thesis: TLR reduction with no beneficial TLR reduction with no beneficial effect on death and re-infarction was effect on death and re-infarction was observed in RCTobserved in RCT
• AntithesisAntithesis: there are still concerns regarding : there are still concerns regarding generalization of DES to the population-at-generalization of DES to the population-at-large (potentially armful)large (potentially armful)
• Synthesis: do we have to apply evidence based medicine?
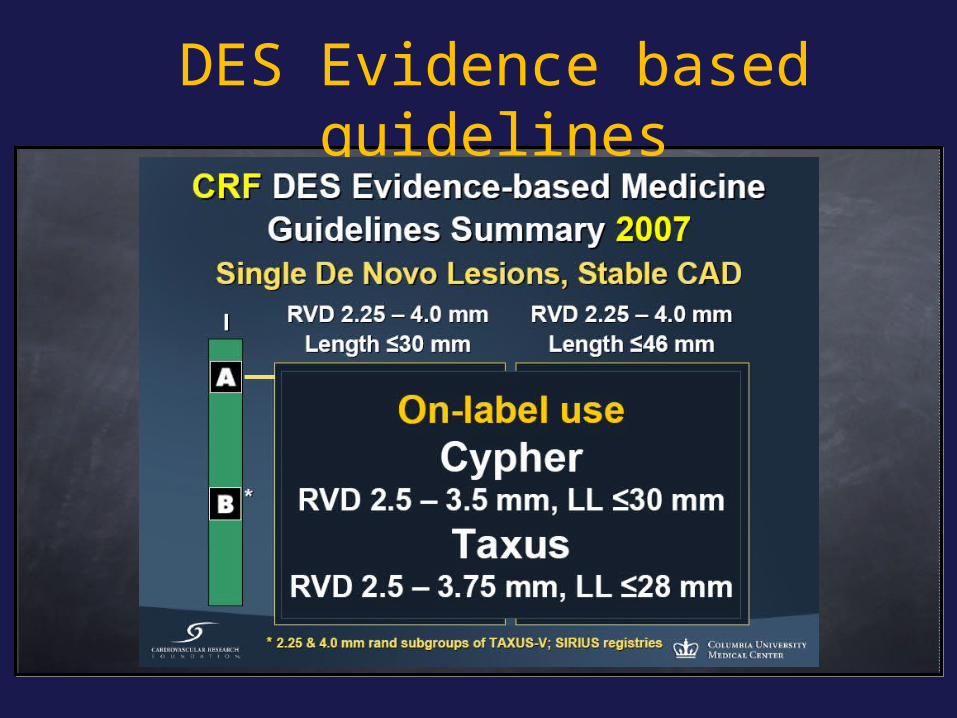
DES Evidence based guidelines
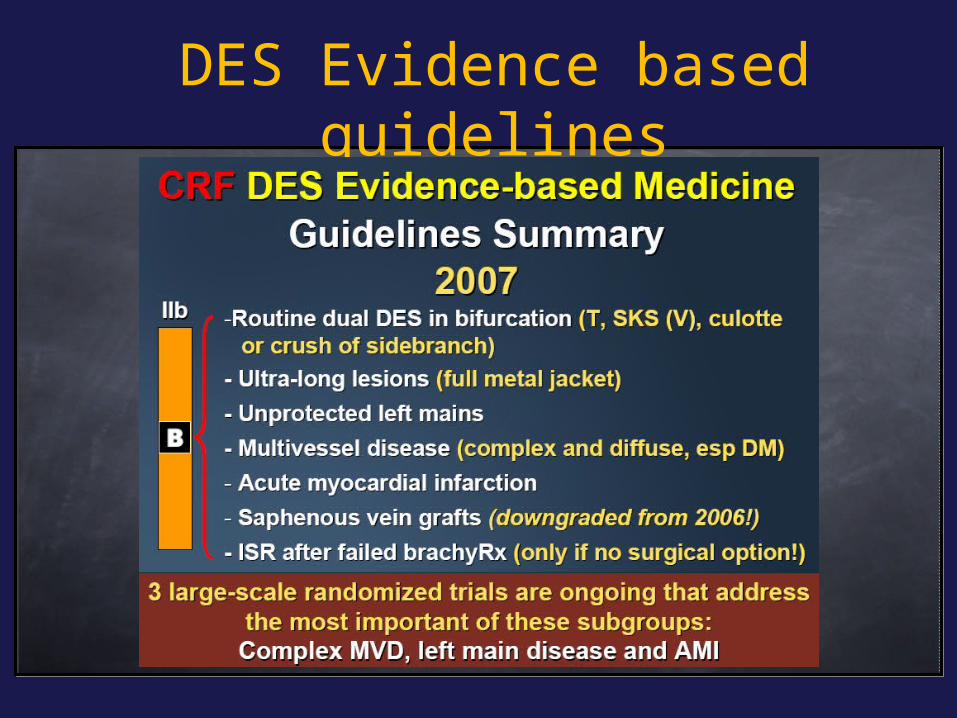
DES Evidence based guidelines
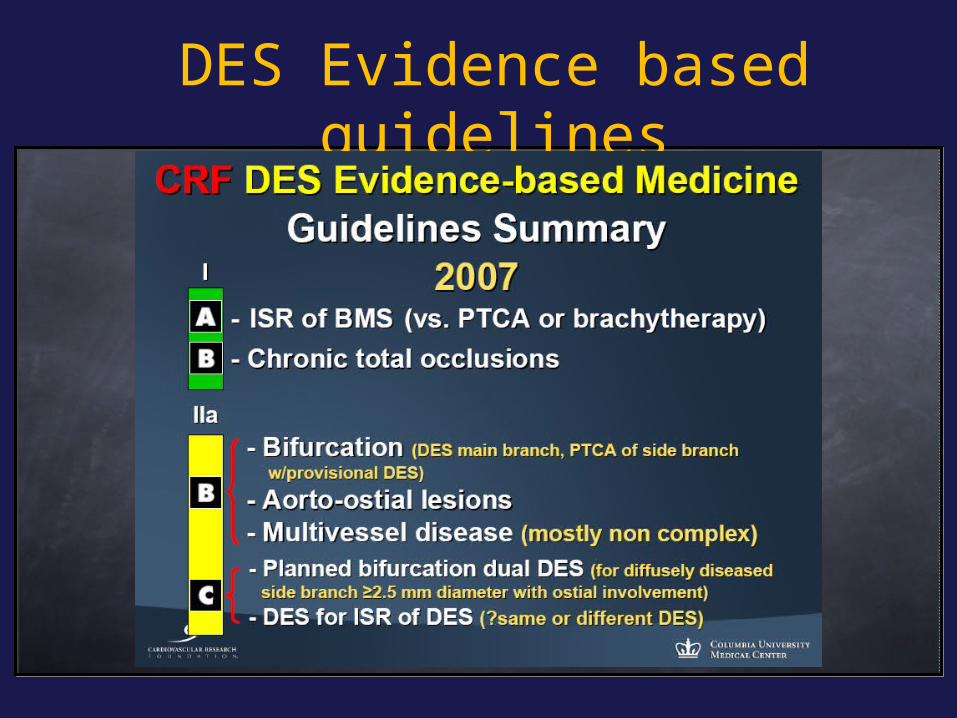
DES Evidence based guidelines

What is the Evidence?What is the Evidence?
Randomized controlled trials(selective patients, underpowered)
Observational Cohort registries(different strategies, unblinded, biased)
Meta-analyses (meta-analysis have been proven wrong 35% of the time by large RCT!)
Treatment strategy studies (biased, underpowered)

DES and Lesions/Patients Characteristics: the Fact
DES have been revolutionary in cardiology
Failure rates are increasing with increasing complexity of disease treated
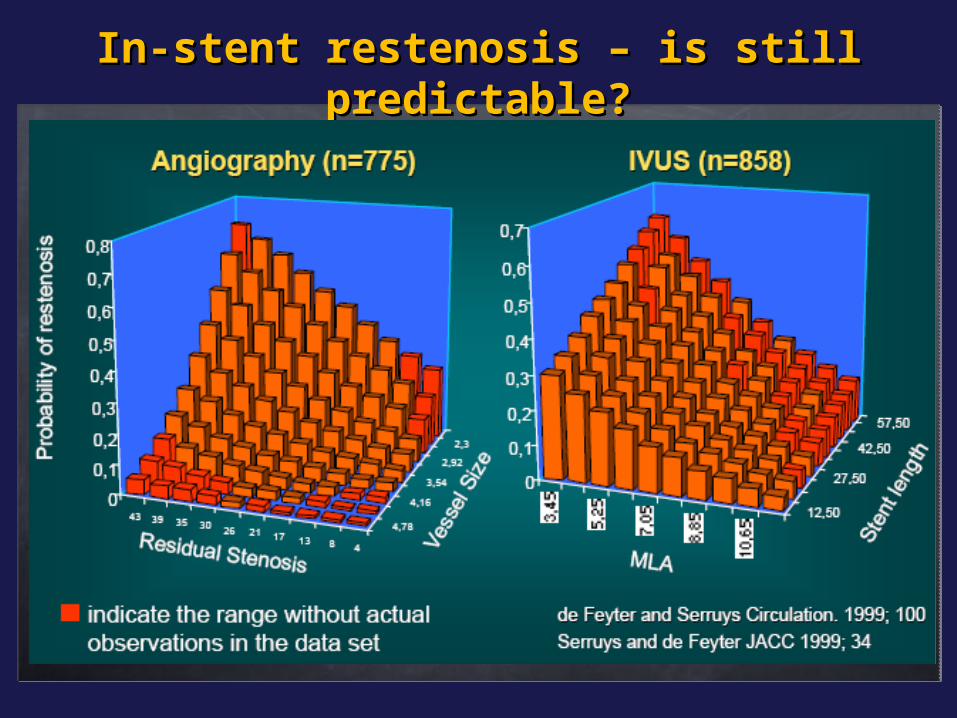
In-stent restenosis – is still In-stent restenosis – is still predictable?predictable?
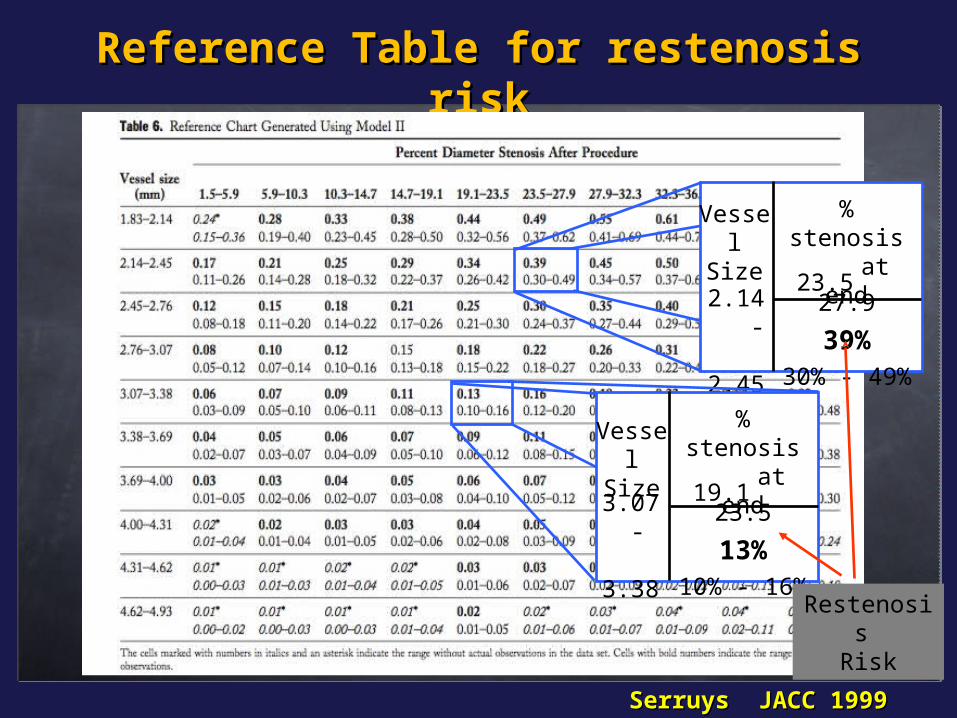
Reference Table for restenosis riskReference Table for restenosis risk
Serruys JACC 1999Serruys JACC 1999
% stenosis
at end
Vessel Size
2.14 - 2.45
23.5 27.9
39%30% - 49%
% stenosis
at end
Vessel Size
3.07 - 3.38
19.1 23.5
13%10% - 16%
Restenosis Risk

BASKET trial: 18-month analysisUsed in all patients, drug-eluting stents are not good value for money, even if prices were substantially reduced.
Brunner-La Rocca Lancet 2007
High-risk patients
Drug-eluting stents are cost effective in patients needing small vessel or bypass graft stenting, but not in those who require large native vessel stenting
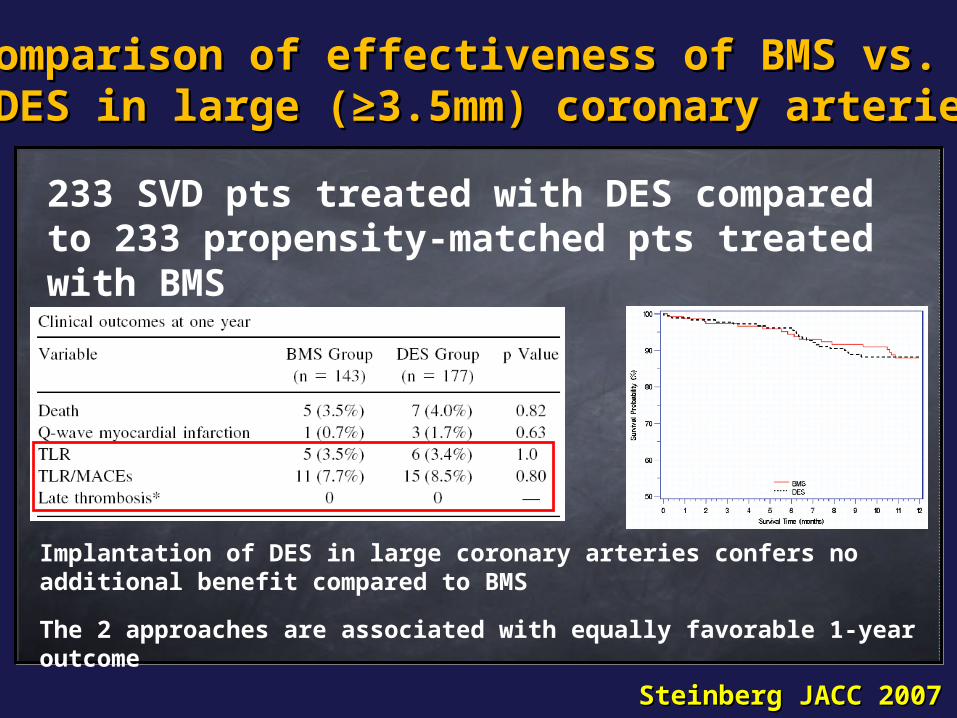
Implantation of DES in large coronary arteries confers no additional benefit compared to BMS
The 2 approaches are associated with equally favorable 1-year outcome
Steinberg JACC 2007Steinberg JACC 2007
233 SVD pts treated with DES compared to 233 propensity-matched pts treated with BMS
Comparison of effectiveness of BMS vs.Comparison of effectiveness of BMS vs. DES in large (≥3.5mm) coronary arteriesDES in large (≥3.5mm) coronary arteries
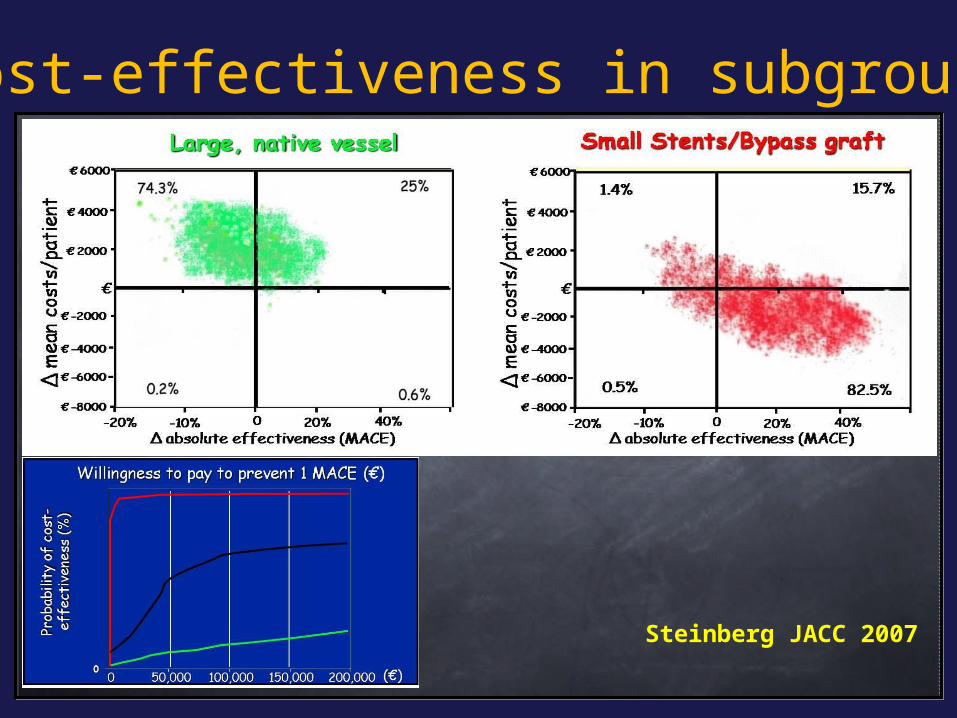
Cost-effectiveness in subgroups
Steinberg JACC 2007
Adjusted for type of lesion, stent diameter and length
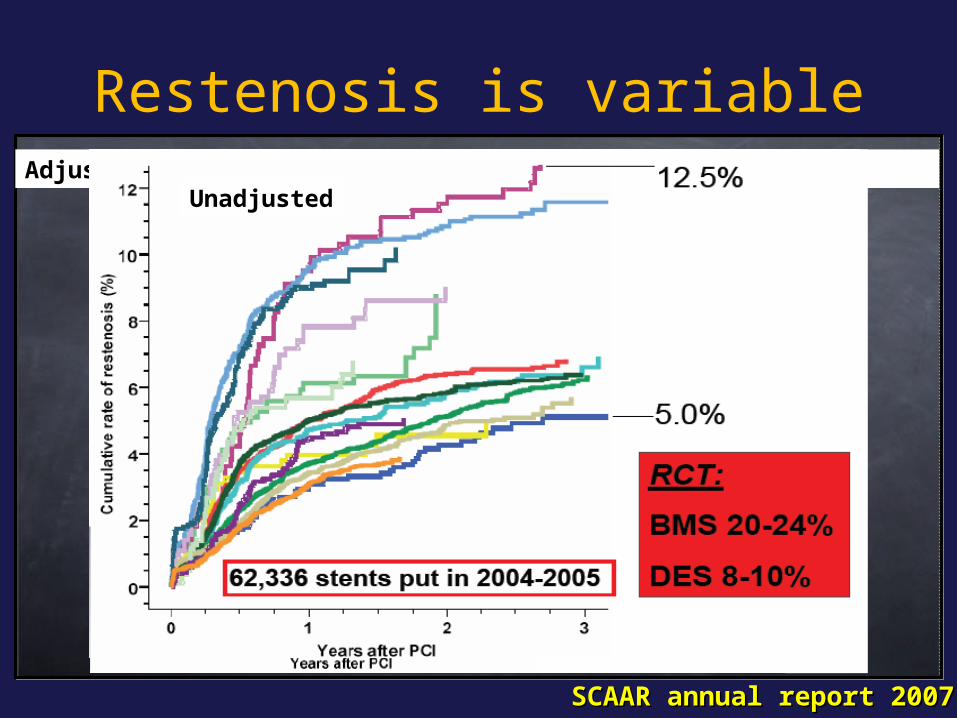
Restenosis is variable
SCAAR annual report 2007SCAAR annual report 2007
Unadjusted

Predictors of stent thrombosis
Moses CIT 2006Moses CIT 2006
DES pending questions
ISR lesion (esp. Diffuse proliferative and s/p VBT)
Bifurcation (ostial side branch)
SVGs
LM disease (esp. Distal bifurcation)
Acute MI and thrombus-containing lesions
Quale DES?Quale DES?

ManifacturerManifacturer NameName DrugDrug Stent Stent MaterialMaterial PolymerPolymer
BiosensorsBiosensors AxxionAxxion PaclitaxelPaclitaxel Stainless SteelStainless Steel NoneNone
BiosensorsBiosensors BioMatrixBioMatrix Biolimus-A-9Biolimus-A-9 Stainless SteelStainless Steel BioabsorbableBioabsorbable
Boston ScientificBoston Scientific Taxus LibertéTaxus Liberté PaclitaxelPaclitaxel Stainless SteelStainless Steel DurableDurable
Boston ScientificBoston Scientific PromusPromus EverolimusEverolimus Cobalt Cobalt ChromiumChromium
DurableDurable
Cordis / J&JCordis / J&J Cypher SelectCypher Select SirolimusSirolimus Stainless SteelStainless Steel DurableDurable
Cordis / J&JCordis / J&J Cypher NeoCypher Neo SirolimusSirolimus Cobalt Cobalt ChromiumChromium
DurableDurable
EurocorEurocor Genius TaxcorGenius Taxcor PaclitaxelPaclitaxel Stainless SteelStainless Steel NoneNone
Guidant/AbbottGuidant/Abbott ChampionChampion EverolimusEverolimus Stainless SteelStainless Steel BioabsorbableBioabsorbable
Guidant/AbbottGuidant/Abbott Xience VXience V EverolimusEverolimus Cobalt Cobalt ChromiumChromium
DurableDurable
MedtronicMedtronic EndeavorEndeavor ZotarolimusZotarolimus Cobalt Cobalt ChromiumChromium
DurableDurable
SorinSorin JanusJanus TacrolimusTacrolimus Stainless SteelStainless Steel NoneNone
SMTSMTTransluminaTranslumina
InfinniumInfinniumYukonYukon
PaclitaxelPaclitaxelSirolimusSirolimus
Stainless SteelStainless SteelStainless stelStainless stel
BioabsorbableBioabsorbableNpneNpne
TerumoTerumo NoboriNobori Biolimus-A-9Biolimus-A-9 Stainless SteelStainless Steel BioabsorbableBioabsorbable
DES Summary - 2007 in Italy: DES Summary - 2007 in Italy: 10 DES With CE Mark in Yellow10 DES With CE Mark in Yellow
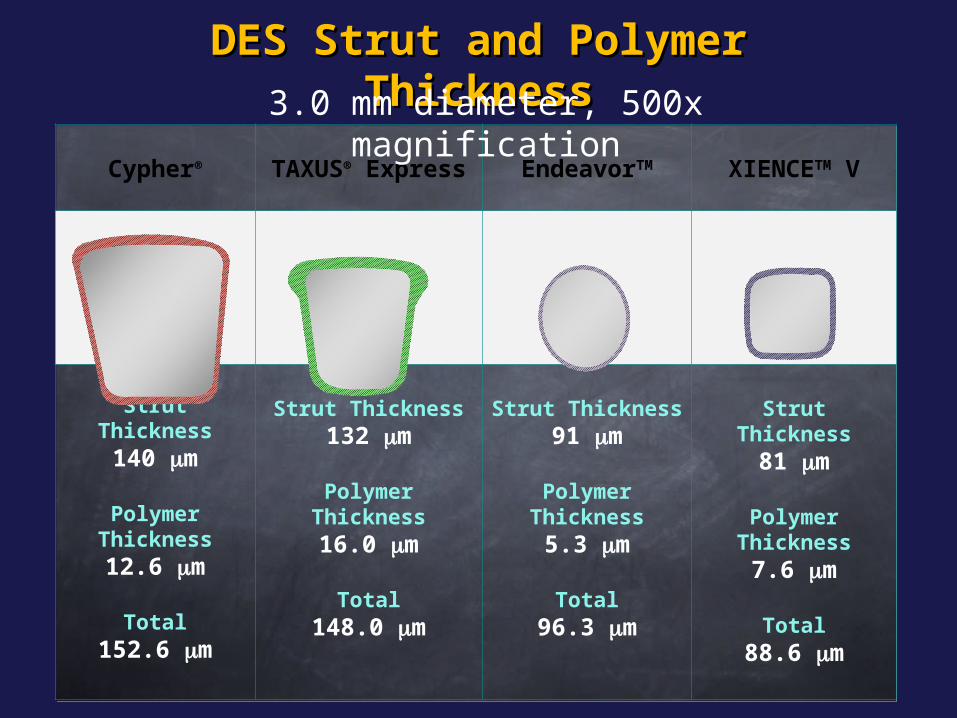
DES Strut and Polymer DES Strut and Polymer ThicknessThickness
Cypher® TAXUS® Express
EndeavorTM XIENCETM V
Strut Thickness140 m
Polymer Thickness12.6 m
Total152.6 m
Strut Thickness132 m
Polymer Thickness16.0 m
Total148.0 m
Strut Thickness91 m
Polymer Thickness5.3 m
Total96.3 m
Strut Thickness81 m
Polymer Thickness7.6 m
Total88.6 m
3.0 mm diameter, 500x magnification
Some DES do not workSome DES do not work
Quanam – Taxane (polymer sleeve)Quanam – Taxane (polymer sleeve)
Guidant – Actinomycin D (polymer matrix)Guidant – Actinomycin D (polymer matrix)
Guidant/Cook – Placlitaxel (direct application)Guidant/Cook – Placlitaxel (direct application)
Abbott – Batimastat (PC coating)Abbott – Batimastat (PC coating)
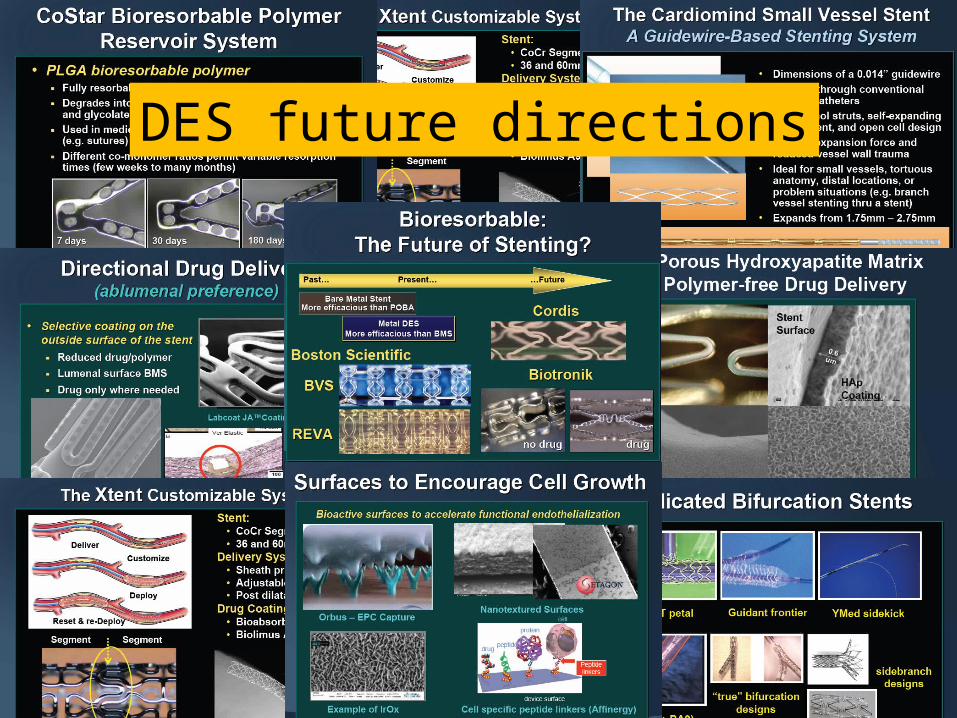
DES future directions
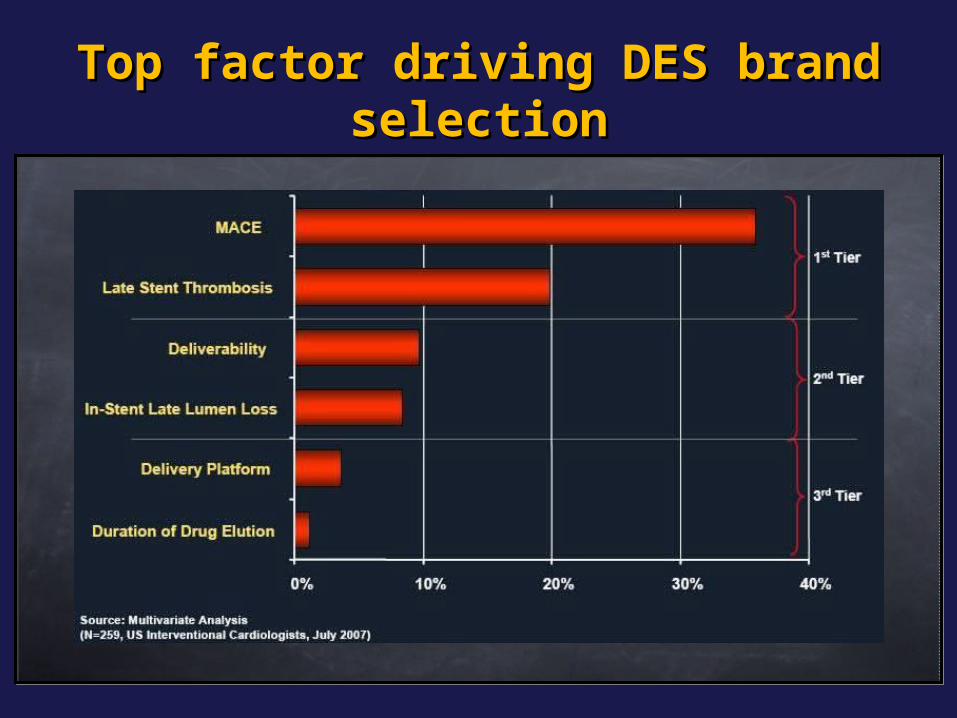
Top factor driving DES brand Top factor driving DES brand selectionselection
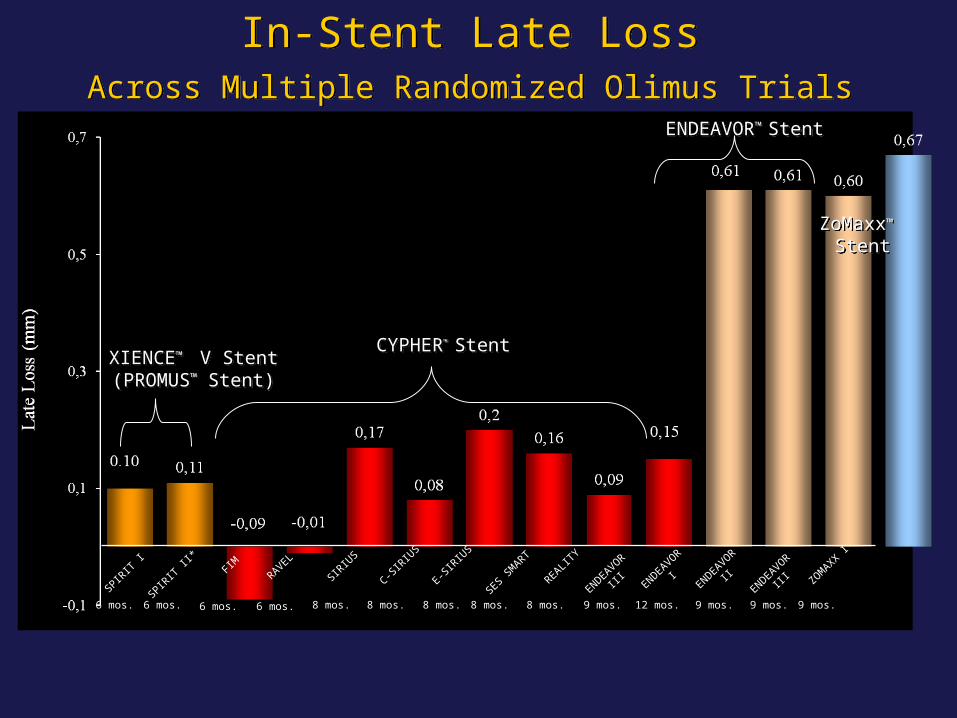
In-Stent Late Loss Across Multiple Randomized Olimus Trials
In-Stent Late Loss Across Multiple Randomized Olimus Trials
CYPHER™ StentCYPHER™ Stent
ENDEAVOR™ StentENDEAVOR™ Stent
XIENCE™ V Stent(PROMUS™ Stent)XIENCE™ V Stent(PROMUS™ Stent)
ZoMaxx™
StentZoMaxx™
Stent
8 mos.6 mos.
SPIRIT
I
6 mos.
SPIRIT
II*
FIMRAVEL
SIRIU
S
C-SIR
IUS
E-SIR
IUS
SES SM
ART
REALITY
ENDEAVOR
III ENDEAVOR
IENDEAVOR
II ZOMAXX I
6 mos. 6 mos. 8 mos. 8 mos. 8 mos. 8 mos.ENDEAVOR
III
9 mos.12 mos. 9 mos.9 mos. 9 mos.

Does lesion characteristics Does lesion characteristics dictate stent selection?dictate stent selection?
Any specific Any specific suggestions?suggestions?
A)A)To limit restenosis To limit restenosis
B)B)To limit thrombosisTo limit thrombosis
C) To limit costsC) To limit costs
What have we learned… about DES?
Dual antiplatelet therapy is crucial for a Dual antiplatelet therapy is crucial for a longer duration then for BMS (longer duration then for BMS (how long?how long?))
Risk of complication (death, MI, ST) are Risk of complication (death, MI, ST) are higher for patients receiving DES off-label higher for patients receiving DES off-label vs on-label (vs on-label (is it different for BMS?is it different for BMS?))
Timing and mechanisms of stent Timing and mechanisms of stent thrombosis seem different than for BMS thrombosis seem different than for BMS ((which is the overall incidence?which is the overall incidence?))
““Do the right choice…” Do the right choice…”
DES DES
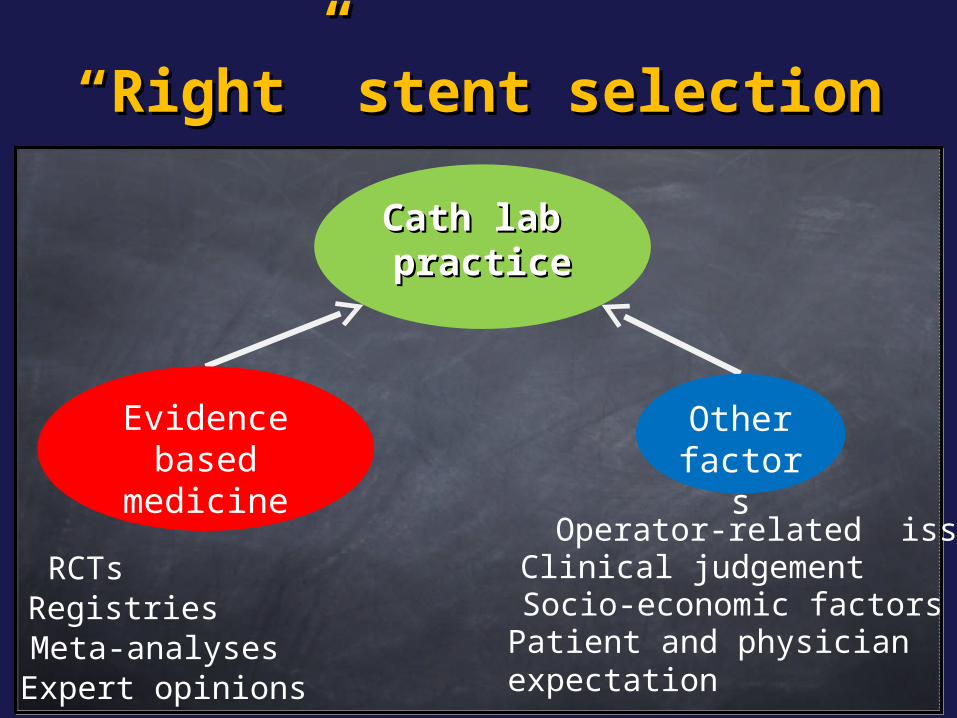
““Right” stent selectionRight” stent selection
Cath lab Cath lab practicepractice
RCTsRegistriesMeta-analysesExpert opinions
Clinical judgement
Patient and physician expectation
Operator-related issues
Socio-economic factors
Evidence based
medicine
Other factors

Innovative Technology Innovative Technology LifecycleLifecycle
Rapid Adoption
(data > perception)
UnbridledEnthusiasm(perception > dara)
UntowardComplications
(perception > data)
Technology
New technology + new data
Realistic application
(data > perception)
We are here
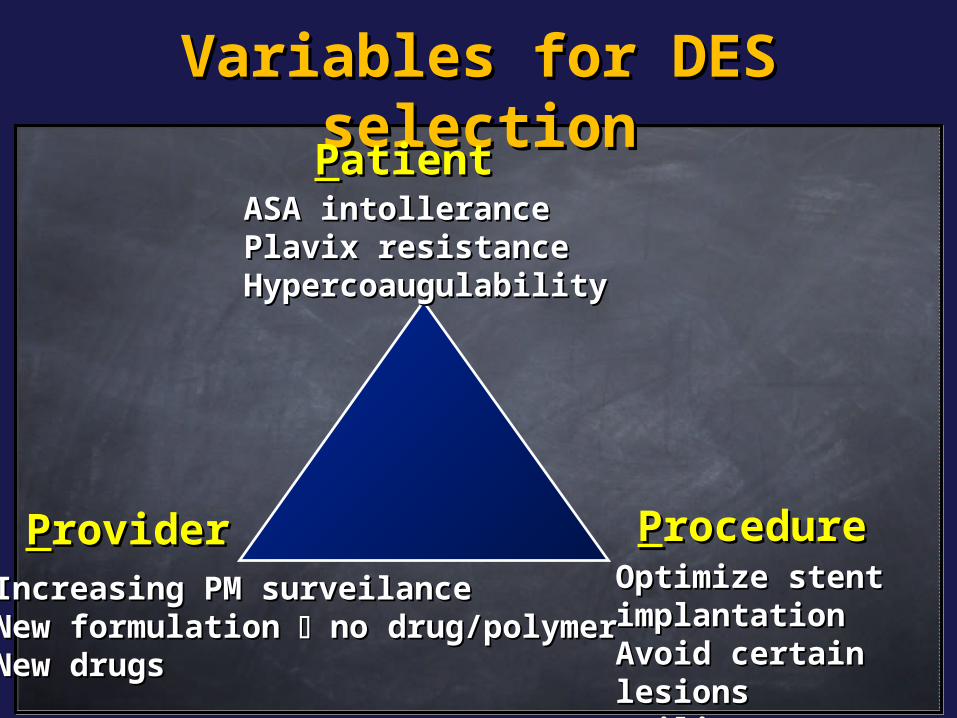
Variables for DES Variables for DES selectionselectionPPatientatient
ASA intolleranceASA intollerancePlavix resistancePlavix resistanceHypercoaugulabilityHypercoaugulability
PProcedurerocedureOptimize stent Optimize stent implantationimplantationAvoid certain Avoid certain lesionslesionsUtilize IVUSUtilize IVUS
PProviderroviderIncreasing PM surveilance Increasing PM surveilance New formulation New formulation no drug/polymer no drug/polymer New drugsNew drugs
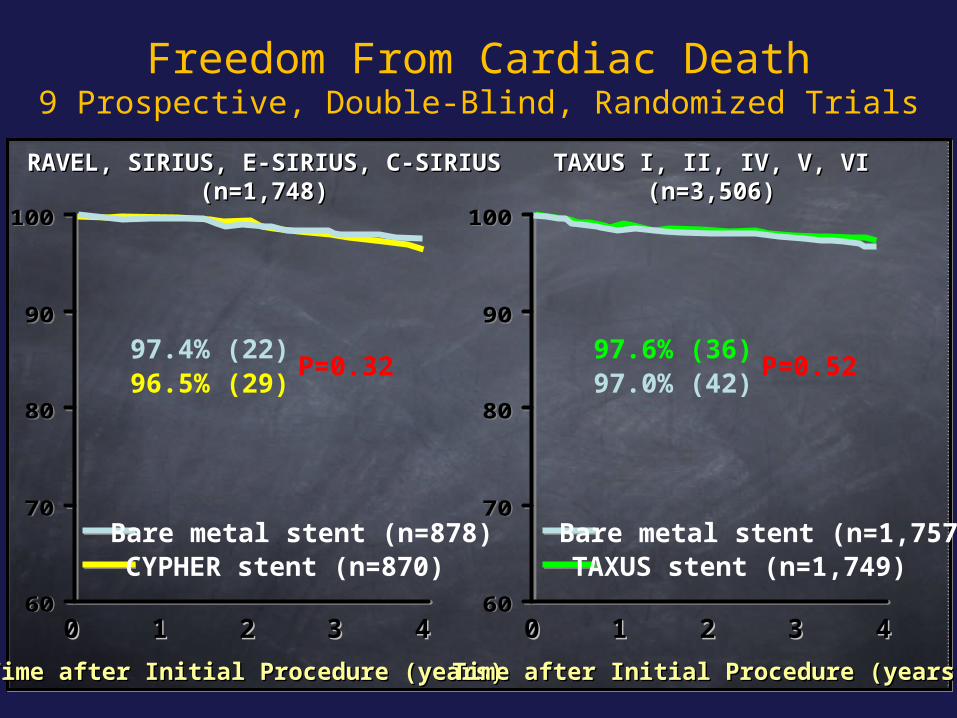
Freedom From Cardiac Death9 Prospective, Double-Blind, Randomized Trials
60
70
80
90
100
60
70
80
90
100
Time after Initial Procedure (years)Time after Initial Procedure (years)
00 11 22 33 44
Time after Initial Procedure (years)Time after Initial Procedure (years)
TAXUS I, II, IV, V, VITAXUS I, II, IV, V, VI(n=3,506)(n=3,506)
RAVEL, SIRIUS, E-SIRIUS, C-SIRIUSRAVEL, SIRIUS, E-SIRIUS, C-SIRIUS(n=1,748)(n=1,748)
P=0.3297.4% (22)96.5% (29)
CYPHER stent (n=870) Bare metal stent (n=878)
00 11 22 33 4460
70
80
90
100
60
70
80
90
100
P=0.5297.0% (42)97.6% (36)
TAXUS stent (n=1,749) Bare metal stent (n=1,757)
60
70
80
90
100
60
70
80
90
100
Time after Initial Procedure (years)Time after Initial Procedure (years)
00 11 22 33 44
Time after Initial Procedure (years)Time after Initial Procedure (years)
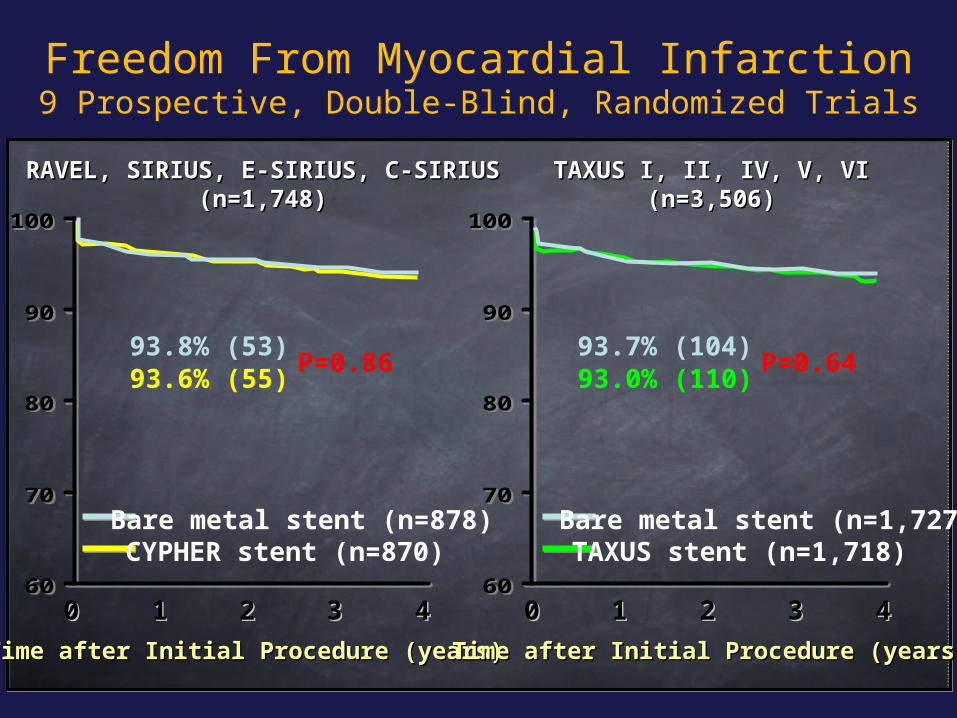
TAXUS I, II, IV, V, VITAXUS I, II, IV, V, VI(n=3,506)(n=3,506)
RAVEL, SIRIUS, E-SIRIUS, C-SIRIUSRAVEL, SIRIUS, E-SIRIUS, C-SIRIUS(n=1,748)(n=1,748)
P=0.8693.8% (53)93.6% (55)
CYPHER stent (n=870) Bare metal stent (n=878)
00 11 22 33 4460
70
80
90
100
60
70
80
90
100
P=0.6493.7% (104)93.0% (110)
TAXUS stent (n=1,718) Bare metal stent (n=1,727)
Freedom From Myocardial Infarction9 Prospective, Double-Blind, Randomized Trials
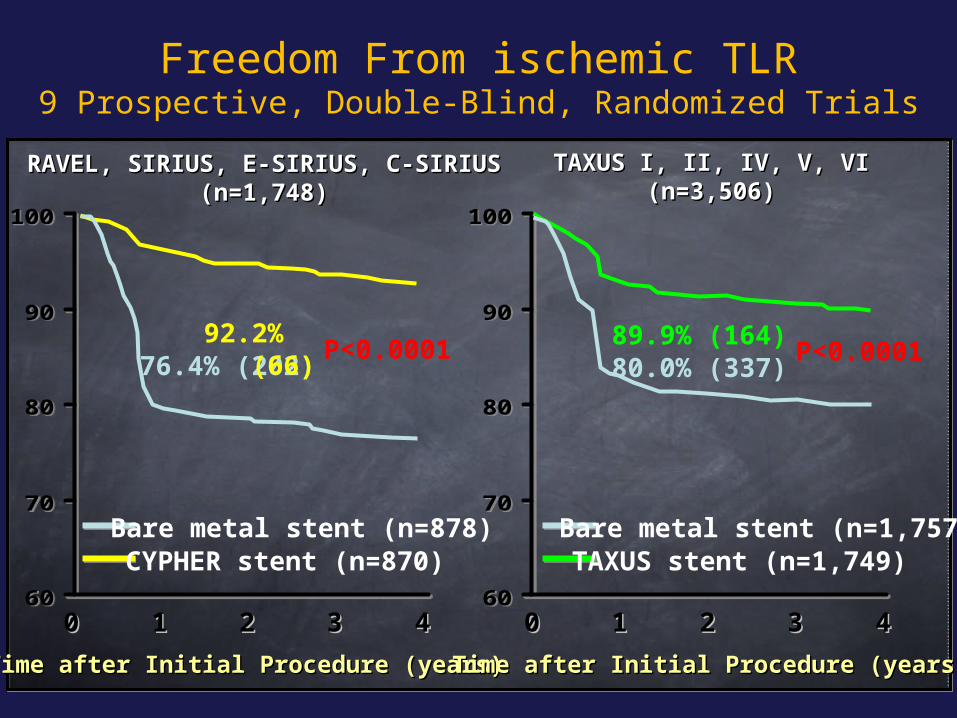
Freedom From ischemic TLR9 Prospective, Double-Blind, Randomized Trials
60
70
80
90
100
60
70
80
90
100
Time after Initial Procedure (years)Time after Initial Procedure (years)
00 11 22 33 44
Time after Initial Procedure (years)Time after Initial Procedure (years)
TAXUS I, II, IV, V, VITAXUS I, II, IV, V, VI(n=3,506)(n=3,506)
RAVEL, SIRIUS, E-SIRIUS, C-SIRIUSRAVEL, SIRIUS, E-SIRIUS, C-SIRIUS(n=1,748)(n=1,748)
P<0.000176.4% (202)92.2% (66)
CYPHER stent (n=870) Bare metal stent (n=878)
00 11 22 33 4460
70
80
90
100
60
70
80
90
100
P<0.000180.0% (337)89.9% (164)
TAXUS stent (n=1,749) Bare metal stent (n=1,757)
For further slides on these topics please feel free to visit the metcardio.org website:
http://www.metcardio.org/slides.html

















