90
Enteral feeding methods Dr Dharma Rajiv gandhi cancer institute, Delhi.
| Date post: | 16-Jul-2015 |
| Category: |
Healthcare |
| Upload: | dharma-punia |
| View: | 385 times |
| Download: | 1 times |

Enteral feeding methods
Dr Dharma Rajiv gandhi cancer institute, Delhi.

CONTENT
• Introduction
• Access methods
• Administration.
• Complications
• summary

INTRODUCTION
• “Dietary foods for special medical purposes’’
• independent of the route of application.
• It includes
– oral nutritional supplements
– tube feeding
» the European legal regulation of the commission directive 1999

EPIDEMIOLOGY
• Approximately 5% of apparently ‘‘healthy’’ UK adults were shown to have a body mass index (BMI) ,20 m/kg2.
• This increased to 10% or more for the chronically sick and patients with cancer, gastrointestinal disease, respiratory problems, and neurological or psychiatric conditions
Advantages - Enteral vs PN
• Preserves gut integrity• Possibly decreases bacterial translocation• Preserves immunological function of gut• Fewer infectious complications• Safer &cost effective• EN is only likely to benefit nutritionally depleted patients
or those at risk of becoming depleted.
ASPEN. The science and practice of nutrition support. A case-based core curriculum. 2001; 147
Indications for Enteral Nutrition
• Malnourished (unable to eat) >5-7 days• Normally nourished patient (unable to eat)>7-9 days• Adaptive phase of short bowel syndrome• Increased needs that cannot be met through oral intake
(e.g.,burns, trauma)
ASPEN. The science and practice of nutrition support. A case-Based Core curriculum.
2001; 143

Contraindications for EN
• Inability to gain access
• hemodynamic instability
• High output proximal fistula, Intractable vomiting or diarrhea, paralytic ileus, Intestinal obstruction, Severe G.I. Bleed.
• Expected need less than 5-7 days if malnourished or 7-9 days if normally nourished.

ACCESS TECHNIQUES
• Up to 4–6 weeks
– NG or NJ tubes,
• Beyond 4-6 week with life expectancy more than 3months
– percutaneous gastrostomy or jejunostomy

ACCESS TECHNIQUES

Naso gastric (NG) feeding
Indications:
• Short term feedings required
• Intact gag reflex
• Gastric function not compromised
• Low risk for aspiration
Naso gastric (NG) feeding
• Fine bore 5–8 French NG tubes are now used
• Large bore PVC tubes they irritate the nose and oesophagus and increase the risks of gastric reflux and aspiration.
• Polyurethane and silicone tubes
• Position of tube tip..

Naso gastric (NG) feeding
Advantages•NG tubes can be inserted bedside.•It allow the use of hypertonic feeds, higher feeding rates, and bolus feeding.•Better tolerated.•Easy to check gastric residuals
Disadvantages:• Increases risk of
aspiration (maybe).• Not suitable for
patients with compromised gastric function
• May promote nasal necrosis and esophagitis
• Impacts patient quality of life.

Naso jejunal tubes
• Jejunal feeding may be indicated if there are
– problems with gastric reflux or delayed gastric emptying.
– It should also be used in unconscious patients who have to be nursed flat.
– In patients who have more than 250-500ml GRV or formula reflux in two consecutive measures.
• Fine bore (6–10 French gauge).

…cont
…cont
• Post pyloric placement can be difficult and various techniques are used.
• Even in experienced hands, bedside placement of nasojejunal (NJ) tubes is difficult and has a low success rate of 15% to 30%.

..cont
• Hence endoscopic placement is indicated in most instances.
• Direct visualization methods
• Direct manipulation
• Through the scope (TTS)

• PRCT by Heyland et al demonstrated that
– Trend toward higher frequency of pulmonary aspiration in intragastric feeding compared to postpyloric feeding (7.5% vs. 3.9%) statistical nonsignficant.
– statistically signficantly higher gastroesophageal reluxbetween gastric feeding and postpyloric feeding (39.8% vs. 24.9%, P = 0.04).

NG vs NJ.
• Recent meta analysis did not show any difference regarding mortality/ ICU stay between either method.
• Recent ASPEN guidelines suggest only indication for NJ tube is Gastric intolerance.
» Heyland, Ho KM and Marik et al
• Contraindications to NG and NJ intubation include– obstruction of the nasopharynx and esophagus, – Recent foregut surgery that may predispose to
perforation– craniofacial fractures. – Intolerance to pre pyloric feeds, abdominal pain with
feeding, and repeated regurgitation of the feeding solution
• Relative contraindications to NG tube placement include – severe gastroesophageal relux, – coagulopathy, and – esophageal variceal bleeding.

Feeding enterostomies• Gastrostomy
– Surgically placed • STAMM open / lap• JANEWAY open / lap
– Endoscopically• PEG
– Radiologically• RPG
• Jejunostomy.• Needle • witzel
• Other methods– Percutaneous gastrojejunostomy– Percutaneous transesophageal gastrostomy tube– Mini-laparoscopically guided percutaneous gastrostomy– The segmentaion-based lossless image coded (slic) technique– Direct percutaneous endoscopic jejunostomy– Magnetically guided feeding tubes

Indications of enterostomies
• Who require long-term (>30 days) access to the GI tract.
• They most commonly provide enteral nutrition in those with
– Impaired swallowing/ cognition from neurologic conditions
– Neoplastic diseases of the oropharynx, larynx, and esophagus.

Contraindications of enterostomies.
– life expectancy less than 3months
– uncorrectable coagulopathy,
– peritonitis
• Cautions warrented in
– massive ascites,
– the morbidly obese,
– distended loops of small bowel,

STAMM GASTROSTOMY
– Egeberg in 1837
– Sellidot in 1849
Was gold standard before advent of PEG.
Laparoscopic SG Less invasive than traditional open gastrostomy but more invasive than PEG tubes, it is currently recommended for patients who require long-term feeding access but who are not candidates for endoscopic placement.

JANEWAY GASTROSTOMY
• Used when there is risk of inadvertent removal of the gastrostomy, as in a confused and uncooperative patient
Laparoscopic Janeway Gastrostomy

PEG
• In 1980 a percutaneous endoscopic gastrostomy(PEG) technique was developed by Ponsky and Gauderer as an alternative method to obtain gastric access.
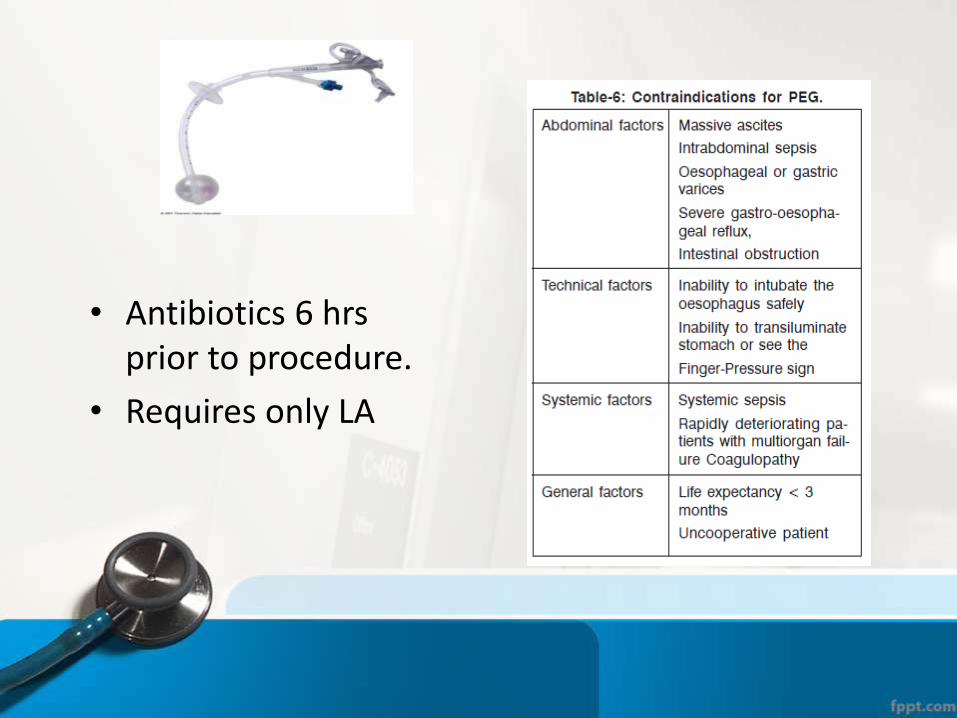
• Antibiotics 6 hrs prior to procedure.
• Requires only LA


Push Technique (Sacks-Vine)
• This is similar to the pull method except that the PEG tube is pushed over the taut guidewire.
Introducer (Russell) Technique
• It uses Seldinger technique for the placement of a balloon-tipped PEG tube directly into the stomach, using direct endoscopic Visualization.

POST -OP
• Not fed through PEG tube in the first 12-24 hours after its placement. However recent evidence suggest early innitiation of feeding.
• vital signs monitored-bleeding and leakage at the PEG site.
• PEG should not be removed for at least 14 days after insertion to ensure that a fibrous tract is established that will prevent intra peritoneal leakage.
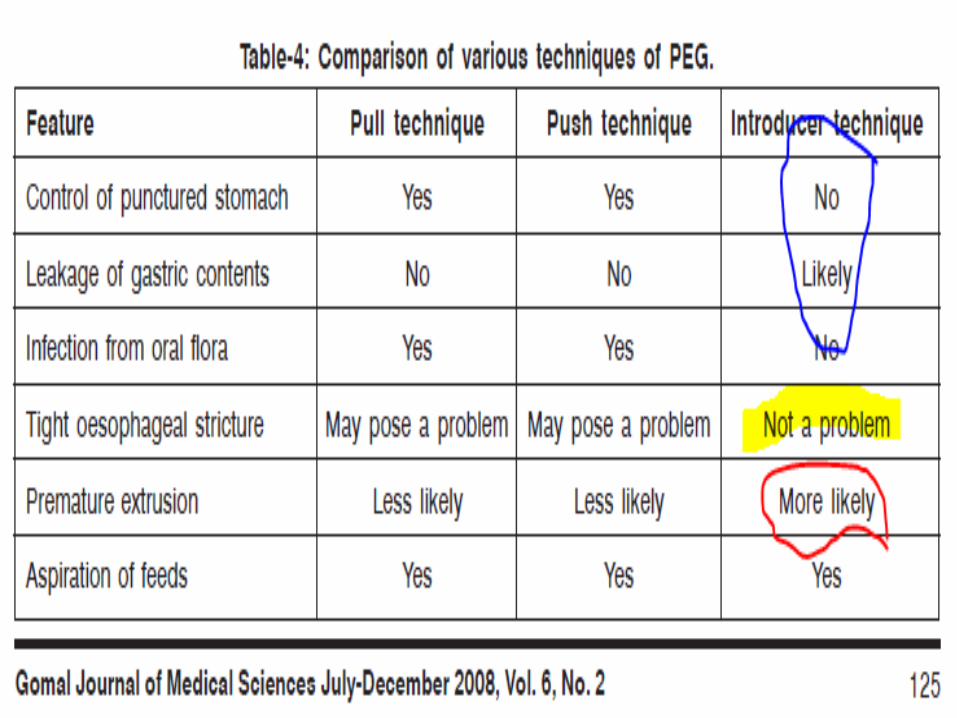
• The pull, push, and introducer techniques have all been found to be effective and safe methods
• A well-trained Gatroenterologist should be familiar with all three standard methods and be able to select which one best suits a patient’s needs.
• Overall incidence of 10% to 16% based on large cumulative retrospective studies.
– Mortality is 1%,
– major complication rate of 3%
– minor complication rate of 13%.
• Wound infection• Buried bumper syndrome• Leakage of feedings into
the peritoneal cavity• Gastrocolic fistula • Pneumoperitoneum(0.3%• Neoplastic seeding• Aspiration with
subsequent pneumonitis
Larson D, Burton D, Schroeder K: Percutaneous endoscopic gastrostomy:Indications, success, complications and mortality in 315consecutive patients. Gastroenterology 93:48, 1987

Radiologically Placed Gastrostomy
• They use Seldinger technique as described for the introducer method.
• Common indications
– esophageal stenosis from malignant or benign stricture,
– When endoscopy is contra indicated, or unable to localize safe puncture site.

• Per cutaneously pass a needle through the left lobe of the liver, into the lumen of the remnant stomach, filled with air and contrast.
• Needle put in stomach at different site.
• Then with seldinger method put the FT.

• Gauderer MWL, Stellato TA. Gastrostomies:
• Evalution, techniques, indications and complications.
• Curr Prob Surg 1986; 23: 661-719.
JEJUNOSTOMY
• This is commonly performed surgical enterostomy for EN.
– Can be used in patients who have had a gastrectomy.
– When stomach is to be used for surgery later on like in ca esophagus.
– Usually placed at the time of other surgery, although laparascopic placement has also been described.
Needle jejunostomy
– by inserting a 14- to 16G needle is to create a subserosal tunnel approximately 30 to 40 cm distal to the ligament of Treitz and the tip redirected into the jejunal lumen.
– A 9F catheter is inserted through the needle and advanced 30 to 40 cm distally.
– The needle is removed and the loop of jejunum is anchored to the anterior abdominal wall with silk sutures internally.

The Witzel technique
This is the gold standard for placing jejunostomy tube.
Laparoscopic Jejunostomy
SliC technique • This technique is a variation on the introducer technique.• Endoscopic access to the stomach is obtained in the standard
fashion and the ideal location for percutaneous access is determined.
• Instead of placing an introducer and outer peel-away sheath, a 7- to 8-mm radially expanding Step trocar is used to penetrate the abdominal wall and gain access to the stomach.
• A PEG tube is then inserted through this trocar. • The trocar is removed and the tube is secured in the usual fashion.• This method is advantageous because it allows for the placement of
a larger-diameter 20F Malecot tube that is more resistant to plugging and accidental removal.
• In addition, abdominal or PEG site seeding of oropharyngealcancers is avoided with this technique as it circumvents dragging the tube through the oral cavity or esophagus

MINI-LAPAROSCOPICALLY GUIDEDPERCUTANEOUS GASTROSTOMY
• In patients in whom
– transillumination of the abdominal wall is not possible,
– who have had previous gastrectomies,
– who have failed radiologic gastrostomy tube placement,
• First pneumoperitoneum established.
• With simultaneous use of laparoscope and endoscope, the optimal insertion point is determined in the stomach or jejunum.

PERCUTANEOUS TRANSESOPHAGEALGASTROSTOMY TUBE
• First reported by Oishi in Japan in 1998, the PTEG technique allows for placement of a gastrostomy tube via the cervical esophagus, which avoids going through the abdominal wall.
• It is especially useful in the – presence of tense ascites, – morbid obesity, – distended loops of bowel anterior to the stomach, or – in patients with carcinomatosis.
• The patient is placed in a supine position and conscious sedation administered.
• A guide wire is inserted through the nose and into the esophagus. • Correct positioning of the wire is confirmed via fluoroscopy. A rupture-free
balloon (RFB) is advanced over the wire into the distal esophagus and then inflated with approximately 20 mL of dilute contrast and retracted until resistance is met at the cricopharyngeus.
• Ultrasound is used to verify position of the balloon. • The optimal puncture site is determined by trans cutaneous ultrasound
and the overlying skin is anesthetized.

• A small needle with an outer sheath is placed through the left neck and into the RFB under ultrasound and fluoroscopic guidance.
• Aspiration of contrast material into the syringe confirms proper placement of the needle.
• The needle is removed and a guidewire is inserted through the sheath into the balloon. The sheath is removed and the guidewire is grasped at skin level and the RFB delated and advanced into the distal esophagus, allowing the cervical guidewire to come out of the lumen of the balloon and remain in the esophagus.26
• The guidewire is then removed from the balloon and advanced into the stomach. The original nasal guidewire and the RFB are then removed.
• A small incision is made over the cervical guidewire and a 16F dilator with an outer peel-away sheath is placed over the wire into the esophageal lumen to upsize the percutaneous
• esophageal access. The wire and dilator are removed and the PTEG balloon catheter is advanced into the stomach.
• Once in the stomach, the balloon is inflated and pulled upward with the tip of the catheter resting just below the GEJ. After catheter placement, contrast injection conirms correct placement.

DIRECT PERCUTANEOUS ENDOSCOPICJEJUNOSTOMY
• It is indicated in patients who are unable to tolerate oral nutrition and in whom conventional percutaneous endoscopic gastrostomyinsertion was unsuccessful or inappropriate (secondary to gastric resection, malignancy, or dysmotility).
• The procedure may be performed with the use of conscious sedation.
• The procedure begins with the passing of the endoscope into the first loop of the jejunum and confirming its position by transilluminationand finger indentation in the left upper quadrant.
• A 4-cm 21-gauge pilot needle is advanced through the abdominal wall and used to locate the jejunal lumen.
• Intermittent fluoroscopy may be used to help guide the needle into the gut lumen.
• After the appropriate puncture site has been determined, a drainage access needle is advanced alongside of the pilot needle into the bowel lumen where it may be snared. At this point, the procedure proceeds in the same manner as a pull PEG tube insertion.

MAGNETICALLY GUIDED FEEDING TUBES• This procedure may be performed at the patient’s bedside by
one person without the use of fluoroscopy or endoscopy.
• The feeding tube is placed via the nares into the stomach and the position confirmed by auscultating over the epigastrium during air insuflation.
• A hand-held magnet is then placed externally over the epigastrium to establish magnetic coupling to the specialized feeding tube, which contains a small earth magnet at its tip.
• The external magnet is then moved slowly across the surface of the abdomen to the right upper quadrant, then inferiorly, and initially toward the midline to follow the curvature of the duodenum. A plain abdominal
• radiograph is used to confirm proper position.

Administration and
feeding protocol

• Enteral feedings should be started postoperatively in surgical patients without waiting for flatus or a bowel movement, (initiated within 24-48 hours)
• A PEG tube may be utilized for feedings within several hours of placement, (within 2 hours in adults and 6 hours in infants and children.)
• Delivery method and initiation and advancement of EN regimens on
– patient condition,
– age,
– enteral route (gastric vs small bowel),
– Nutrition requirements
– GI status

• Choose full strength, isotonic formulas for initial feeding regimen.
• Diluting formulas may increase the risk of microbial contamination intolerance due to diarrhea.

• Gastric feeding and stable patients.
– Initiate with full strength formula @ 50 ml/hr, X 3-8 times bolus/gravity method.
– Increase upto 50-100ml/hr every 10-12 hrs till goal volume.(usually 24-48hrs)

• Small-bowel feedings and
• Gastric feedings in critically ill patients or severlymalnourished patients.
– A pump is generally required.
– as the slower administration rate of continuous feedings often enhances tolerance.
• Start as full strength (iso/hyperosmolar/elemental) @10-40ml/hr 3-8 feeds, if tolerates well increase by 10-20ml/hr every 10-12 hrly till goal reached.
• Elevate the backrest to a minimum of 30º, and preferably to 45º, for all patients receiving EN unless a medical contraindication exists.

• Flush feeding tubes with
– 30 mL of water every 4 hours during continuous feeding.
– Before and after bolus/intermittent feedings in an adult patient.
– after measuring GRV.
• Sterile water is usually recommended, for flushing and mixing medications.

GRV
• No adequately powered studies have demonstrated that elevated GRVs are reliable markers for increased risk of aspiration pneumonia.
• “the elevated residual volumes by themselves have little clinical meaning and that only when combined with vomiting, sepsis, sedation, or the need for pressor agents does the correlation with worsening patient outcome emerge.”
» McClave SA, Lukan JE, Stefater JA, et al. Poor validity of residual volume as a marker for risk of aspiration in critically ill patients. Crit Care Med. 2005;33:324-330.
• GRV every 4 hlry for first 48 hrs till goal reached Then 6-8 hrly, if patient stable.
• If patient is critically ill, GRV measurment should be 4 hrly.
• If the GRV is > 250 mL x2 times a promotility agent should be considered in adult patients.

• A GRV >500 mL holding EN and reassessing patient tolerance by use of an established algorithm including physical assessment, GI assessment, evaluation of glycemic control, minimization of sedation, and consideration of promotility agent use, if not already prescribed.
• Consideration of a feeding tube placed below the ligament of Treitz when GRVs are consistently measured at > 500 mL.

Administration
• Bolus
• Intermittent
• Continuous

Bolus feeding
• Infusion of up to 500 ml of enteral formula into the stomach over 15 (5-20 ) minutes, usually by gravity or with a large-bore syringe.
Indications:
• Recommended for gastric feedings
• Requires intact gag reflex
• Normal gastric function.

Advantages:• More physiologic• Enteral pump not
required• Inexpensive and easy
administration• Limits feeding time so
patient is free to ambulate,
• Makes it more likely patient will receive full amount of formula
Disadvantages:
• Increases risk for aspiration
• Hypertonic, high fat, or high fiber formulas may delay gastric emptying or result in osmotic diarrhea

Continuous Feedings
• It is administered through pump or gravity, usually over 8- 24 hrs continuosly .
Indications:
• Initiation of feedings in acutely ill patients
• Feeding into small bowel
• Intolerance to other feeding technique.
Advantages:
• May improve tolerance
• May reduce risk of aspiration
• Increased time for nutrient absorption
Disadvantages:
• May reduce 24-hour infusion
• May restrict ambulation
• More expensive for home support
• Pumps are required

Intermittent Feedings
Definition• Enteral formula administered at specified times
throughout the day; generally in smaller volume and at slower rate than a bolus feeding but in larger volume and faster rate than continuous drip feeding
• Typically 200-300 ml is given over 30-60 minutes q 4-6 hours
• Precede and follow with 30-ml flush of tap waterIndications:• Intolerance to bolus administration• Initiation of support without pump• Preparation of patient for rehab services or discharge
to home

Advantages:• May enhance quality
of life– Allows greater
mobility between feedings
– More physiologic– May be better
tolerated than bolus
Disadvantages:
• Increased risk for aspiration
• Gastric distention
• Delayed gastric emptying
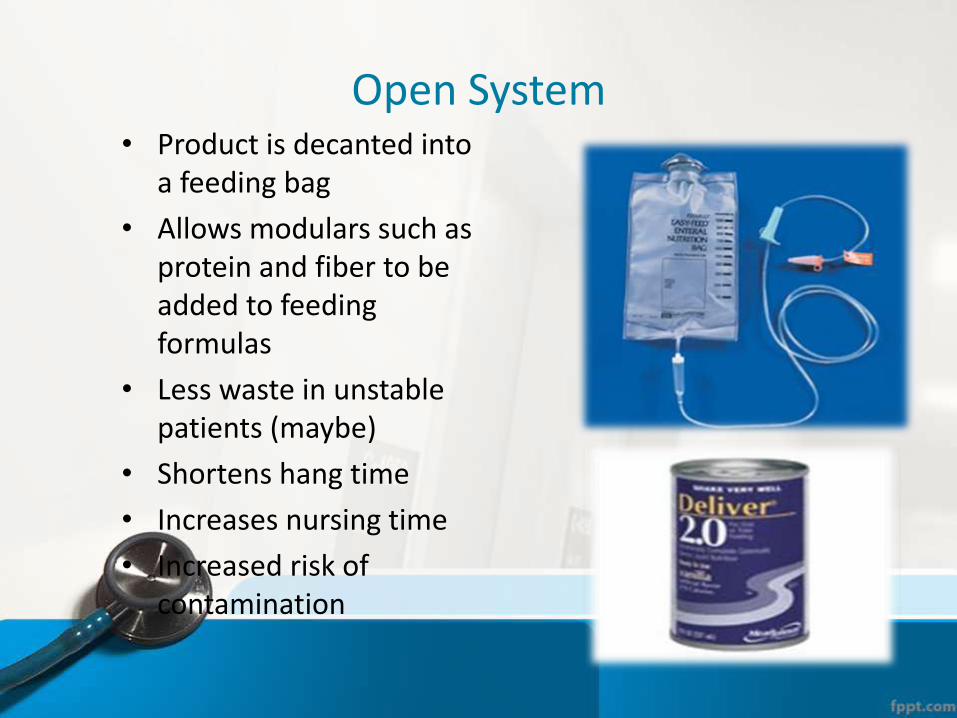
Open System• Product is decanted into
a feeding bag
• Allows modulars such as protein and fiber to be added to feeding formulas
• Less waste in unstable patients (maybe)
• Shortens hang time
• Increases nursing time
• Increased risk of contamination

Closed System or Ready to Hang
• Containers sterile until spiked for hanging
• Can be used for continuous or bolus delivery
• No flexibility in formula additives• Less nursing time• Increases safe hang time• Less risk of contamination• More expensive than canned formula
Closed vs Open System
Open System• Hang time 8 hours for
decanted formula; 4 hours for formula mixtures
• Feeding bag and tubing should be rinsed each time formula replenished
• Contaminated feedings are associated with pt morbidity
Closed System• Hang time 24-48 hours
based on mfr recommendations
• Y port can be used to deliver additional fluid and modulars
• May result in less formula waste as open system formula should be discarded p 8 hours
Enteral Feeding Complications
• Mechanical
• Gastrointestinal
• Metabolic
• Infectious

Mechanical
• Feeding tube obstruction
• Feeding tube dislodged
• Nasal irritation
• Skin irritation/excoriation at entrerostomy site

Causes of Feeding Tube Obstruction
• Concentrated, viscous, and fiber-containing feeding products
• Tube feeding contamination
• Checking of gastric residuals
• Small diameter tubes
• Powdered or crushed medication flushed through tubes
• Acidic or alkaline medications passed through tubes
• Tubes not routinely flushed after feedings are stopped

Prevention of Feeding Tube Obstruction
• Flush the feeding tube, especially before and after medication administration and bolus/intermittent feedings
• Use liquid formulations of medicines where possible (but be careful of osmolarity)
• Do not mix medications with enteral feedings unless shown to be compatible
• Avoid crushing sustained-release or enteric-coated tablets

Treatment of Feeding Tube Obstruction
• Declog with irrigants (warm water) or sodium bicarbonate/pancrealipase mixture or by mechanical means
• Cola beverages, cranberry juice, and tea not recommended
The A.S.P.E.N. Nutrition Support Practice Manual, 2nd Edition, 2005

Aspiration
• Reported incidence of aspiration in tubefed patients varies from .8% to 95%. Clinically significant aspiration 5% gastric-fed pts
• Many aspiration events are “silent” and often involve oropharyngeal secretions
• Symptoms include dyspnea, tachycardia, wheezing, rales, anxiety, agitation, cyanosis
• May lead to aspiration pneumonia

Aspiration Prevention
• Keep head of bed elevated 30-45 degrees during and 30-40 minutes after feedings
• Small, frequent feedings or continuous drip
• Use of promotility agents
• Monitoring of gastric residuals may be helpful in identifying delayed gastric emptying and increased risk of aspiration.
The A.S.P.E.N. Nutrition Support Practice Manual, 2nd Edition, 2005

Gastrointestinal Complications
• Diarrhea
• Constipation
• Gastric distention/bloating
• Gastric residuals/delayed gastric emptying
• Nausea/vomiting

Diarrhea• Definition:
– >500 ml every 8 hours
– or more than 3 stools a day for at least two consecutive days, Relates more to stool consistency than frequency
• Diarrhea was a common consequence of enteralfeedings when hyperosmolar feedings were routinely delivered via syringe
• Occurs in 2 to 63% of enterally-fed pts depending on how defined
Causes/Treatments of Diarrhea
• Intestinal atrophy due to malnutrition
• Bolus feeding in the small intestine: results in dumping syndrome.
– Use an infusion pump to regulate flow
The A.S.P.E.N. Nutrition Support Practice Manual, 2nd Edition, 2005
Causes/Treatments of Diarrhea
• Bacterial overgrowth of intestinal tract or contamination of the enteral feeding
– Avoid prolonged use of broad-spectrum antibiotics
– Use clean technique and closed system in handling enteral feedings
– Limit hang time of open system formulas to 8 hours (4 hours for mixtures)
– Change bag and tubing per protocol
– Test for C difficile and other pathogens before using anti-motility agents

Causes/Treatments of Diarrhea
• Steatorrhea: characterized by frothy, odiferous stools that float on water; caused by fat intolerance
– Use lowfat enteral formula or one with higher percentage of MCT; pancreatic enzymes may help in pancreatic insufficiency

Causes/Treatments of Diarrhea
• Lactose intolerance
– Most enteral products are lactose free but this may occur with initiation of full liquid diet. Eliminate milk and dairy products
• Drug-induced diarrhea
– Meds may cause up to 61% of diarrhea in tubefedpts due to hypertonicity or direct laxative action (magnesium, sorbitol, potassium), antibiotics.
The A.S.P.E.N. Nutrition Support Practice Manual, 2nd Edition, 2005

Treatment of Diarrhea in General
• Add soluble fiber (such as banana flakes or Benefiber) or insoluble fiber such as psillium
• Consider an enteral formula with added fiber
• Use an antidiarrheal agent (loperamide, diphenoxylate, paregoric, octreotide)
• Change the formula
Nausea/Vomiting
• 20% of patients on EN report nausea/vomiting
• Often related to delayed gastric emptying caused by hypotension, sepsis, stress, anesthesia, medications (analgesics and anticholinergics), surgery
Nausea/Vomiting Treatment• Consider reducing/discontinuing narcotic
medications
• Switch to a low fat formula
• Administer feeding solution at room temperature
• Reduce rate of infusion by 20-25 ml/hr
• Administer prokinetic agent (metoclopramide, erythromycin, domperidone, bethanechol)
• Check gastric residuals
• Consider antiemetics
Metabolic
• Fluid and Electrolyte abnormalities
• Glucose intolerance
• Ca++, Mg++, PO4 abnormalities

Fluid and Electrolyte Disturbances
• May result from long term nutrition deficits, acute stress, medications, medical conditions, improper nutrient prescription
• Electrolytes lost via stool, urine, ostomy or fistula drainage
Hyperglycemia
• Often reflects acute stress, infection, medications (especially steroids) or latent diabetes
• Macronutrient distribution: is generally not the primary issue; most enteral feeding formulas fall within established guidelines; could try formula lower in carbohydrate
• Insulin management

Refeeding Syndrome
• At risk: when refeeding those with marginal body nutrient stores, stressed, depleted patients, those who have been unfed for 7-10 days, persons with anorexia nervosa, chronic alcoholism, weight loss.
• Symptoms: Hypokalemia, hypophosphatemia and hypomagnesemia; cardiac arrhythmias, heart failure; acute respiratory failure

Refeeding Syndrome
• Correct electrolyte abnormalities (via oral, enteral, parenteral route) before initiating nutrition support
• Administer volume and energy slowly
• Monitor pulse rate, intake and output, and electrolyte levels
• Provide appropriate vitamin supplementation
• Avoid overfeeding
Infectious Complications
• Formula contamination
• Unsanitary equipment
• Failure to follow appropriate protocols re handling of enteral feedings/changing of bags and tubing

Monitoring of Patients on EN• Electrolytes
• BUN/Cr
• Albumin/prealbumin
• Ca++, PO4, Mg++
• Weight
• Input/output
• Vital signs
• Stool frequency/consistency
• Abdominal examination

SUMMARY
• Mal nutrition is highly prevalent in developing country like india.
• Knowledge of enteral nutrition is essential for treating personnel.
• Indivualize feeding methods, protocols
• Each institution should define an ongoing quality control process for EN formula preparation, distribution, storage, handling, and administration.

















