Epigenetics and Epigenetics and Cancer Cancer + Nilofer Azad, MD Nilofer Azad, MD Assistant Professor, Gastrointestinal Assistant Professor, Gastrointestinal Oncology/Phase I Program Oncology/Phase I Program Sidney Kimmel Comprehensive Cancer Center Sidney Kimmel Comprehensive Cancer Center October 19, 2010 October 19, 2010
Transcript
Epigenetics and Epigenetics and CancerCancer
++
Nilofer Azad, MDNilofer Azad, MDAssistant Professor, Gastrointestinal Oncology/Phase I ProgramAssistant Professor, Gastrointestinal Oncology/Phase I Program
Sidney Kimmel Comprehensive Cancer CenterSidney Kimmel Comprehensive Cancer CenterOctober 19, 2010October 19, 2010
CMAJ 2006;174(3):341-8
Simplified Model of Epigenetic Regulation of Gene Expression
Rationale for double epigenetic blockage in lung cancer
• Epigenetic gene silencing mediated by DNA methylation and histone deaceylation is a key contributor to lung carcinogenesis
• Preclinical studies suggest that combining DMNTi with HDACi synergistically enhances expression of silenced tumor suppressor genes
• Clinical studies combining DMNTi and HDACi have shown remarkable clinical activity in MDS/AML
• Hypothesis: similar effect in NSCLC
Trial Schema
• 5AC Dosing = 40 mg/m2 SQ daily on days 1-6 and 8-10• SNDX-275 dosing = 7 mg PO (fixed dose) days 3 and 10• Cycle length = 28 days
MS275
5-Aza
Day 1 8 15 22 29 36
SNDX-275
5-AC
Day 1 8 15 22 29 36
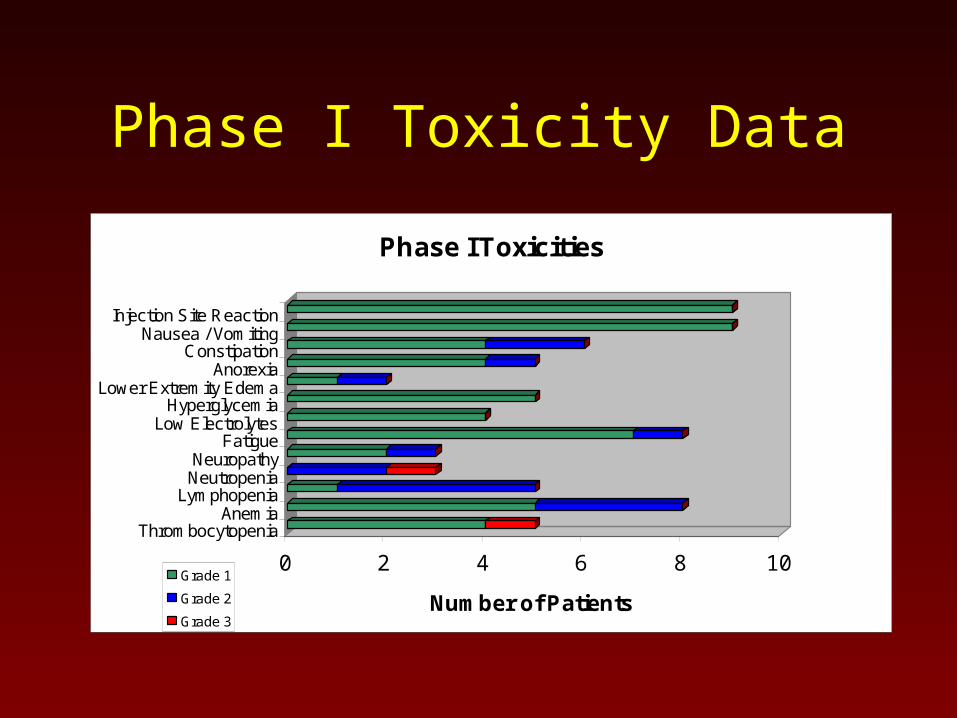
Phase I Toxicity Data
0 2 4 6 8 10
Number of Patients
Injection Site ReactionNausea / Vomiting
ConstipationAnorexia
Lower Extremity EdemaHyperglycemia
Low ElectrolytesFatigue
NeuropathyNeutropenia
LymphopeniaAnemia
Thrombocytopenia
Phase I Toxicities
Grade 1
Grade 2
Grade 3
Updated Response Data28 Evaluable Patients
• 1 Complete Response – On treatment for 14 months
• 1 Partial Response
Responded for 8 months – then new SCLC
Still no progression of his NSCLC 9 months off epigenetic therapy
• 8 Stable Disease One on treatment for 18 months; Five treated for 4 months
One treated for 3 months then stopped due to schedule
One still being treated (on cycle 12 now)
• 17 Progressive Disease
• 8 Not evaluable (finished less than 1 cycle)
• 5 Actively being treated
Overall Survival
Median OS: 8.2 months
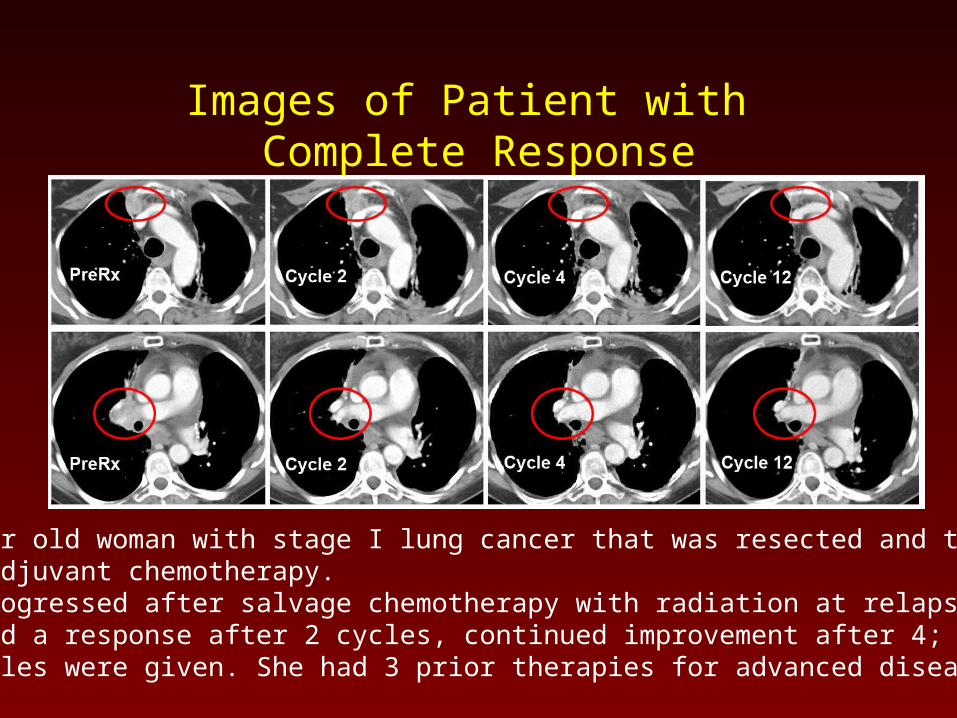
Images of Patient with Complete Response
56 year old woman with stage I lung cancer that was resected and treated with adjuvant chemotherapy.She progressed after salvage chemotherapy with radiation at relapse.She had a response after 2 cycles, continued improvement after 4; 14 cycles were given. She had 3 prior therapies for advanced disease.
Images of patient withPartial Response
58 year old male treated with 3 prior therapies; Chemotherapy refractory disease. He completed 8 cycles.
Images of patient with partial response: liver metastases
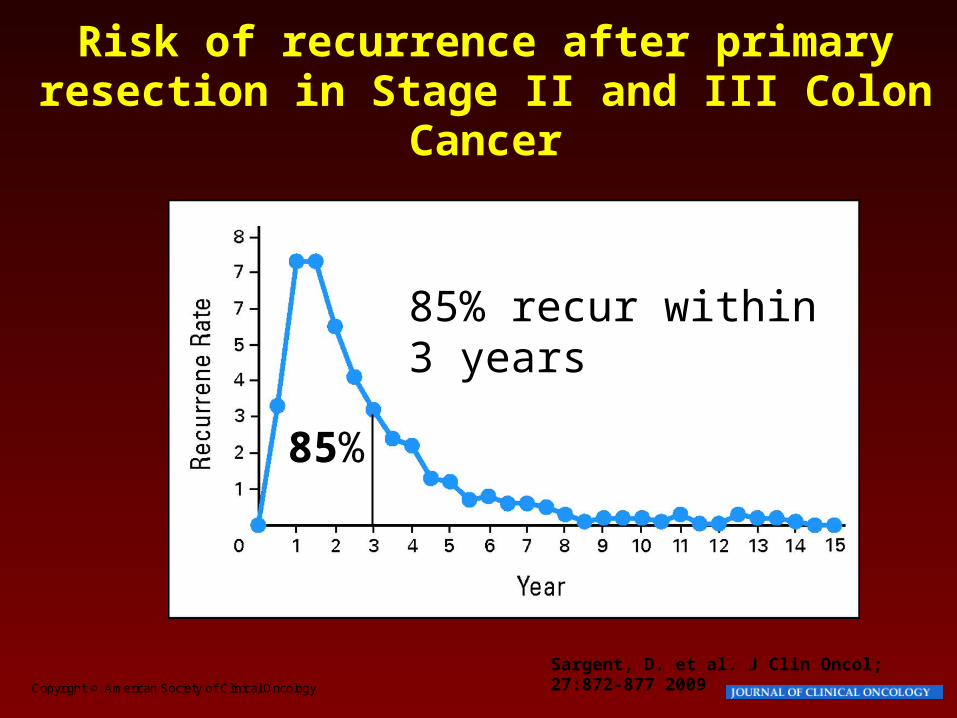
Risk of recurrence after primary resection in Stage II and III Colon
Cancer
85% recur within 3 years
85%
Metastatic Disease
History of Treatment for Colorectal CancerHistory of Treatment for Colorectal Cancer
• ~1960: 5-FU is a cornerstone of first-line therapy; bolus/infusion
• ~1985: Addition of LV (biomodulator) to 5-FU bolus regimens
• 1998: Irinotecan as single agent approved as second-line
• 2000: Irinotecan approved as first-line in CRC (bolus IFL)
• 2001: Capecitabine approved as first-line in CRC in selected pts
• 2002: Oxaliplatin approved as second-line agent (FOLFOX)
• 2004: Oxaliplatin approved as first-line agent in infusional regimen
• 2004: Approval of Cetuximab (Erbitux) & Bevacizumab (Avastin)
• 2006: Approval of Panitumumab (Vectibix)
• 2008: KRAS mutations predict lack of benefit of EGFR mAb’s
Incremental Survival Advantage in First-LineMetastatic Colorectal Cancer
No active drug
0 6 12 18 24Median OS (mo)
~4-6 mo
12-14 mo
~ 15-16 mo
20.3 mo
?
~ 20 mo
5-FU/LV
FOLFOX4
IFL + bevacizumab
IFL
21.5 moFOLFOX/FOLFIRI
FOLFOX/FOLFIRI
+ biologics
Are we hitting a wall with current drugs?
Therapy for Advanced Colorectal Cancer: Response rates and survival
First Line Second Line Third Line- FOLFOX or - FOLFOX or - Irinotecan +- CAPOX or - FOLIRI or Cetuximab - FOLFIRI - Irinotecan alone - Cetuximab +/- Bevacizumab - Irinotecan/Cetuximab - Panitumumab
+/- Bevacizumab
Response Rates in Randomized Trials:
50-60% 15% 10%Survival Benefit in Randomized Trials:
Yes Yes Yes
Epigenetics in CRC• Many genes have silenced expression due to epigenetic
changes
• Targeting epigenetically abnormal tumors may be more effective than targeting abnormal mutations in genes
• CRC may be uniquely appropriate for this strategy
• A subset of colon cancer have more gene promoter methylation
Ahuja et al.
Combination Epigenetic Therapy• First study of epigenetic therapy in CRC
• Primary Objective:
• To determine the preliminary efficacy via tumor shrinkage rate of the combination of 5-azacitadine and entinostat in patients with metastatic colorectal cancer
• Secondary Objective:
• To see what is happening in the tumor itself and circulating cells in blood before and after treatment with these drugs
Study Schema28 days
C2d1C1d3entinostat
C1d1 C1d10entinostat
C2d3entinostat
C2d10entinostat
C3d1
= plasma sampling for research purposes
= tumor sampling for research purposes
5-aza days 1-5 and 8-10 q cycle5-aza days 1-5 and 8-10 q cycle
Ongoing and Upcoming Studies
• Lung Cancer– New schedule– Adjuvant treatment of early stage disease
• Breast– Same schedule in triple negative and hormone
resistant metastatic cancer
Conclusions
• Despite progress, colon cancer is a still leading source of death
• Epigenetic therapy offers a novel way to approach treating cancer, based on the abnormal gene expression seen in cancers compared to normal cells
• We are presently enrolling a trial of patients with late-stage colon cancer an treating them with epigenetic agents, 5-azacitidine and entinostat
BREAST CANCER
Epigenetics and breast cancer
• Multiple genes are methylated and thus silenced in breast cancer1
• ER, RAR beta, cyclin D, Twist, RASSF1A, and HIN-1
1 Pu RT. Mod Pathol 2003;16(11):1095-101.
Zebularine inhibits growth of MDA-MB-231 cell lines alone
or in combination
Billam M. BCRT 2010
Clinical studies: Vorinostat in MBC
• Phase 2
SKCCC J0785/TBCRC 008A Multi-Institutional Randomized Phase II Study Evaluating Response and Surrogate Biomarkers to
Carboplatin and nab-Paclitaxel (CP) with or without Vorinostat (SAHA) in HER2- Negative Breast
Cancer
Principal Investigator: Vered Stearns, MDFellow: Roisin Connolly, MB.BCh
Eligible patients with locally advanced or metastatic breast cancer (up to 60)
Cohort A (up to 30)Triple-negative
5-AZA + entinostat
Cohort B (up to 30)Hormone-resistant5-AZA + entinostat
Disease Progression at Any Time Cohort A or Cohort B
5-AZA + etinostat + hormonal therapy
Event Monitoring
MD discretion
Study schema
Conclusions
• Epigenetics is a new way to look at cancer biology and therapy
• Ongoing trials in major tumor types in the metastatic setting
• Plans to move therapy into earlier stage disease may be even more successful