Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.
VA
SCU
LAR
/IN
TER
VEN
TIO
NA
L R
AD
IOLO
GY
1120
Historical Perspective: Eponyms of Vascular Radiology1
Eponyms are ubiquitous throughout the medical literature, espe-cially the radiology lexicon. In particular, vascular radiology is re-plete with dozens of eponyms named after pathologic and anatomic features and various medical devices. Several disease processes are known exclusively by their eponyms or by both their eponyms and their descriptive names. Although some authors advocate abandon-ing eponyms in favor of more descriptive terms, the established history and common use of eponyms make it unlikely that they will disappear from the vocabulary. Radiologists should be familiar with both the eponymous and descriptive names of disease processes to ensure effective communication and prevent erroneous identifica-tion. Study of these eponyms provides information about these disease processes and other medical knowledge for use in daily practice. In addition, biographic information about the pertinent physicians can yield insights into the sometimes surprising origins of these eponyms. The authors provide biographic sketches of these physicians and discuss the clinical relevance of the anatomic fea-tures, malformations, and syndromes that bear their names.
Jason DiPoce, MD Guillermo Jimenez, MD Joshua Weintraub, MD
Abbreviations: IMA = inferior mesenteric ar-tery, SMA = superior mesenteric artery
RadioGraphics 2014; 34:1120–1140
Published online 10.1148/rg.344130125
Content Code: 1From the Department of Radiology, Colum-bia University Medical Center, New York, NY. Recipient of a Certificate of Merit award for an education exhibit at the 2012 RSNA Annual Meeting. Received August 21, 2013; revision requested August 30 and received November 11; accepted November 22. All authors have no financial relationships to disclose. Address cor-respondence to J.D., Department of Radiol-ogy, Hadassah Medical Organization, Hadassah Campus, POB 12000, Jerusalem 91120, Israel (e-mail: [email protected]).
IntroductionThe historical context of scientific innovation is tightly interwoven with advances in medicine, with eponyms being a continual reminder of this ever-expanding tapestry. Individuals who contributed to our understanding of medicine are honored by later generations through the use of eponyms. Although our understanding of disease processes continues to increase, the passage of time erodes our familiarity with the exceptional individuals for whom the entities are named. A study of these individuals, their circumstances, their methods, and, in some instances, their vast contributions serves as an inspiration.
Many disease processes are known exclusively by their eponyms, and an understanding of these eponyms is necessary for avoiding their misuse. Some authors advocate abandoning the use of ep-onyms for more descriptive terms; however, the pervasiveness of eponyms throughout everyday medical practice makes it unlikely that they will disappear. Therefore, to ensure effective communica-tion, radiologists should be familiar with both eponymous and de-scriptive disease names.
RG • Volume 34 Number 4 DiPoce et al 1121
Figure 1. Charles Stent (1807–1885).
article, we attempt to familiarize radiologists with the physicians behind the eponyms and provide a short, illustrated description of each eponym’s clinical relevance.
Artery of AdamkiewiczAlbert Wojciech Adamkiewicz (1850–1921) (Fig 2a) was a Polish neuropathologist who was interested in the vascular supply to the nervous system and tumor development. His monumental study of anatomy paved the way for modern neurosurgery. Specifically, Adamkie-wicz discovered the magnus ramus radicularis anterior or arteria magna spinalis, also known as the great anterior segmental medullary ar-tery or, more commonly, the artery of Adam-kiewicz. The artery of Adamkiewicz is the only radiculo medullary artery that supplies the tho-racolumbar region of the spinal cord (Fig 2b). Identification of this artery before spinal surgery or vascular procedures is critical to the preven-tion of unintended occlusion and subsequent paralysis. Much notoriety and Adamkiewicz’s academic downfall occurred when he purported to discover an anticancer antitoxin that he called cancroin and a carcinogenic parasite that he called Coccidium sacrolytus (2).
Marginal Artery of DrummondDavid Drummond (1852–1932) (Fig 3a) dem-onstrated the existence of the eponymous mar-ginal artery of Drummond by occluding the proximal right, middle, left colic, and sigmoid arteries in cadavers, followed by injection of contrast medium into the ileocolic artery. Visu-alization of contrast material from the cecum to
Vascular radiology is replete with dozens of eponyms named after pathologic and anatomic features and devices. These words are used so commonly that it is possible to overlook their ori-gin. For example, the word “stent” is in fact an eponym named after Charles Stent (1807–1885) (Fig 1), a British dentist who, in 1856, experi-mented with a material that was both durable and plastic to make dental impressions. Almost 40 years after Stent’s death, a Dutch surgeon used Stent’s material to apply skin grafts to wounded soldiers during World War I in a process called stenting. Eventually the eponym was borrowed by other specialties, including vascular radiology (1).
Many eponyms are commonly used in vascu-lar and interventional radiology (Table). In this
Eponymous Vascular Anatomic Features, Mal-formations, and Syndromes
Anatomic features Artery of Adamkiewicz Marginal artery of Drummond Arc of Riolan Brödel bloodless line Circle of Willis Recurrent artery of Heubner Artery of Percheron Basal vein of RosenthalMalformations Abernethy malformation Dieulafoy lesion Kommerell diverticulum Vein of Galen aneurysmal malformationSyndromes Behçet syndrome Budd-Chiari syndrome Buerger disease Churg-Strauss syndrome Harjola-Marable syndrome Kasabach-Merritt syndrome Kawasaki syndrome Klippel-Trénaunay-Weber syndrome Kussmaul disease Lemierre syndrome Leriche syndrome Maffucci syndrome Marfan syndrome May-Thurner syndrome Paget-Schroetter syndrome Raynaud phenomenon Sinus of Valsalva aneurysm Takayasu arteritis Wunderlich syndrome
1122 July-August 2014 radiographics.rsna.org
Figure 3. (a) David Drummond (1852–1932). (b) Angiogram of the inferior mesen-teric artery (IMA) (straight white arrow) shows its branching vessels. The left colic artery branches (arrowhead) are followed by the ascending branch of the left colic artery (curved arrow). The marginal artery of Drummond (black arrows) is seen as the most lateral ves-sel, which travels just medial to the descending colon. * = Griffith critical point.
Figure 2. (a) Albert Wojciech Adamkiewicz (1850–1921). (b) Digital subtraction angio-graphic image obtained during embolization of an opacified bronchial artery (arrowhead) demonstrates the characteristic hairpin turn (arrow) of the Adamkiewicz artery. The Adam-kiewicz artery must be identified before bronchial artery embolization is performed to prevent nonselective embolization and subsequent spinal cord infarction.
artery of Drummond; in this region, known as the Griffiths critical point (after J. D. Griffiths), the colon is susceptible to ischemia (3,4).
Arc of RiolanJean Riolan (1580–1657) (Fig 4a) was an anato-mist who defended Galen’s approach to the circulation of blood and strongly opposed the now-recognized correct theory of blood circula-
the distal colon led to the identification of the eponymous artery (Fig 3b), which extends the entire length of the colon, with branches from the right, middle, and left colic arteries contrib-uting to its supply. Normally, the marginal ar-tery of Drummond is small in caliber; however, it may enlarge when the IMA or superior mes-enteric artery (SMA) is occluded. A potential hypovascular region exists along the marginal
RG • Volume 34 Number 4 DiPoce et al 1123
Figure 5. Paul Heinrich Max Brödel (1870–1941).
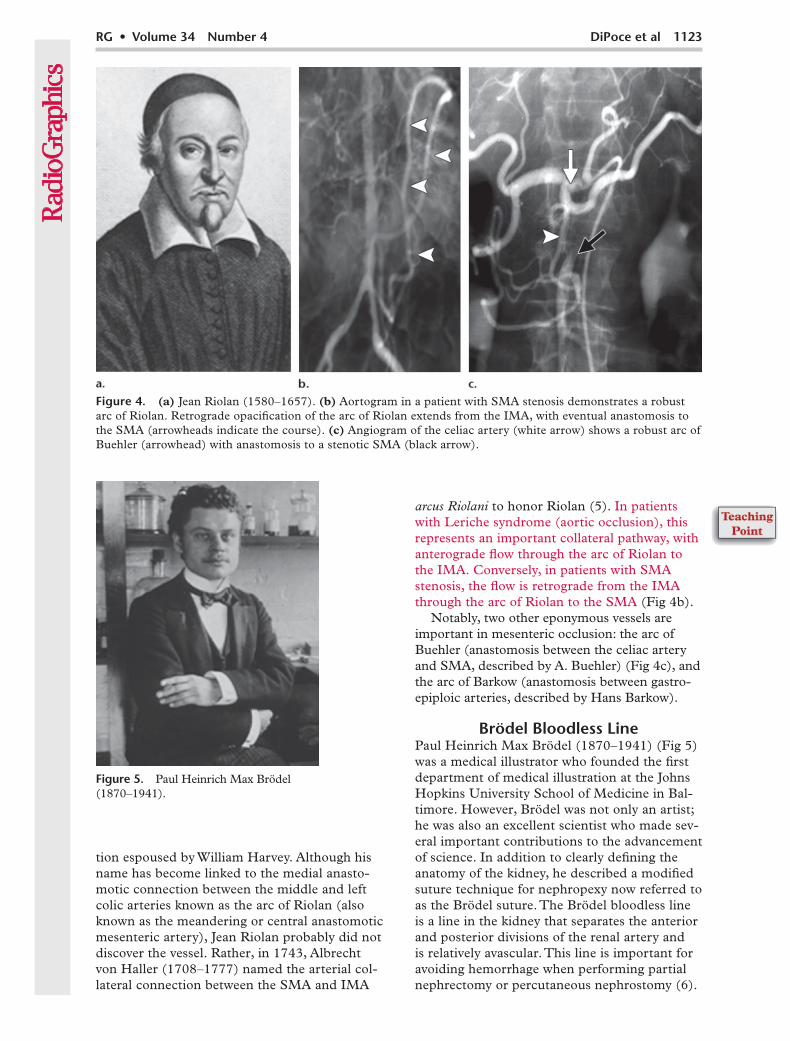
Figure 4. (a) Jean Riolan (1580–1657). (b) Aortogram in a patient with SMA stenosis demonstrates a robust arc of Riolan. Retrograde opacification of the arc of Riolan extends from the IMA, with eventual anastomosis to the SMA (arrowheads indicate the course). (c) Angiogram of the celiac artery (white arrow) shows a robust arc of Buehler (arrowhead) with anastomosis to a stenotic SMA (black arrow).
tion espoused by William Harvey. Although his name has become linked to the medial anasto-motic connection between the middle and left colic arteries known as the arc of Riolan (also known as the meandering or central anastomotic mesenteric artery), Jean Riolan probably did not discover the vessel. Rather, in 1743, Albrecht von Haller (1708–1777) named the arterial col-lateral connection between the SMA and IMA
arcus Riolani to honor Riolan (5). In patients with Leriche syndrome (aortic occlusion), this represents an important collateral pathway, with anterograde flow through the arc of Riolan to the IMA. Conversely, in patients with SMA stenosis, the flow is retrograde from the IMA through the arc of Riolan to the SMA (Fig 4b).
Notably, two other eponymous vessels are important in mesenteric occlusion: the arc of Buehler (anastomosis between the celiac artery and SMA, described by A. Buehler) (Fig 4c), and the arc of Barkow (anastomosis between gastro-epiploic arteries, described by Hans Barkow).
Brödel Bloodless LinePaul Heinrich Max Brödel (1870–1941) (Fig 5) was a medical illustrator who founded the first department of medical illustration at the Johns Hopkins University School of Medicine in Bal-timore. However, Brödel was not only an artist; he was also an excellent scientist who made sev-eral important contributions to the advancement of science. In addition to clearly defining the anatomy of the kidney, he described a modified suture technique for nephropexy now referred to as the Brödel suture. The Brödel bloodless line is a line in the kidney that separates the anterior and posterior divisions of the renal artery and is relatively avascular. This line is important for avoiding hemorrhage when performing partial nephrectomy or percutaneous nephrostomy (6).
1124 July-August 2014 radiographics.rsna.org
Circle of WillisThomas Willis (1621–1675) (Fig 6a) was a Brit-ish anatomist who performed important research on what is now known as the circle of Willis, call-ing it the circulus arteriosus cerebri. However, his accomplishments were much broader: He was the first to coin the words “neurology” and “mellitus” (as in diabetes mellitus), and he conducted influ-ential research in each of these areas. In addition, he numbered the cranial nerves as they are today. Willis was a founding member of the Royal Soci-ety of Medicine (7).
The circle of Willis (Fig 6b, 6c) is actually a polygon formed by the internal carotid arter-ies, proximal anterior cerebral arterial segments, anterior communicating artery, two posterior communicating arteries, and basilar arterial and
proximal posterior cerebral arterial segments. It is a major source of collateral circulation, should one of the major vessels become occluded. There-fore, an incomplete circle of Willis leaves the pa-tient more vulnerable to infarction. Nevertheless, almost 60% of the general population have varia-tions of the circle of Willis (8).
Recurrent Artery of Heubner and Artery of Percheron
Johann Otto Leonhardt Heubner (1843–1926) (Fig 7a) was a German pediatrician who devel-oped the nutritional quotient, discovered that heating milk for sterilization destroyed heat-sen-sitive vitamins, introduced electrocardiography for children, and described celiac disease (known in Germany as Heubner-Herter disease). Early in
Figure 6. (a) Thomas Willis (1621–1675). (b) Drawing by illustrator Christopher Wren, who worked closely with Thomas Willis, shows the circle of Willis. (c) Axial maximum inten-sity projection computed tomographic (CT) image shows the circle of Willis (circle).
RG • Volume 34 Number 4 DiPoce et al 1125
Figure 7. (a) Johann Otto Leonhardt Heubner (1843–1926). (b) Axial fluid-attenuated inversion recovery magnetic resonance (MR) image in a 55-year-old man who presented with acute ataxia and dysarthria demonstrates bilateral increased signal intensity in the thalami (arrows). CT angiography demonstrated a large clot in the right vertebral artery that resulted in occlusion of the artery of Percheron. (Courtesy of Daniel Klein, MD, USC Medical Center, Los Angeles, Calif.)
his career, he performed research on the circula-tion of blood in the brain. Through meticulous dissection, Heubner was able to describe the cerebral arterial supply, identifying the medial striate artery that bears his name. In addition, he described syphilitic endarteritis, also known as Heubner disease.
The artery of Percheron is an uncommon anatomic variant consisting of a solitary arterial trunk arising from a proximal segment of one of the posterior cerebral arteries. It is the source
of a bilateral supply of blood to the paramedian thalami and the rostral midbrain. Consequently, occlusion of this artery can result in infarction of both thalami (Fig 7b). The artery of Percheron is named after the French scientist Gerard Perche-ron, who first described it (9).
Basal Vein of RosenthalFriedrich Christian Rosenthal (1780–1829) (Fig 8) was a German anatomist who specialized in the olfactory system and ichthyology. He died of complications of tuberculosis at 49 years of age. Two eponymous structures bear his name because of his research in neuroanatomy: the Rosenthal canal (also known as the spiral canal of the cochlea, a section of the bony labyrinth of the inner ear), and the basal vein of Rosenthal, which drains into the vein of Galen (10).
Abernethy MalformationJohn Abernethy (1764–1831) (Fig 9a) first de-scribed extrahepatic portosystemic shunts in 1793. Much of Abernethy’s success resulted from his study of comparative anatomy; he even wrote a book describing whale anatomy. Because his classes were so well attended, the hospital at
Figure 8. Friedrich Christian Rosenthal (1780–1829).
1126 July-August 2014 radiographics.rsna.org
Figure 9. (a) John Abernethy (1764–1831). (b) Contrast material–enhanced T1-weighted MR image in a 19-year-old man with Abernethy syndrome demonstrates an aneurysmal main portal vein (P) that drains into the inferior vena cava (I), abrupt termination of the right portal vein (arrow-head), and absence of the left portal vein.
which he lectured built an auditorium for him, from which St Bartholomew’s Hospital Medical School began (11).
Abernethy malformations are anomalies of the venous system in which a congenital porto-systemic shunt results from the persistence of embryonic vessels (Fig 9b). They are classified as type 1 (absence of portal vein with complete diversion of portal blood into systemic veins) or type 2 (hypoplastic portal vein with diversion of portal blood into the vena cava). This shunting may lead to encephalopathy (12).
Dieulafoy LesionPaul Georges Dieulafoy (1839–1911) was a French surgeon who first characterized a bleed-ing arteriole within the gastric mucosa, calling it an exulceratio simplex (Fig 10a). In his initial post-mortem study of 10 patients who had presented with massive hematemesis, he described a bleed-ing vessel surrounded by nonulcerated tissue. Although most of these vessels occur in the proxi-mal stomach as Dieulafoy observed, today the term applies more broadly to vessels anywhere in the gastrointestinal tract. Dieulafoy lesions are characterized by a single submucosal arteriole with abnormal branching or increased caliber (Fig 10b, 10c). The pulsatile arteriole erodes through the mucosa, resulting in hemorrhage. Management includes endoscopic thermal abla-tion, clipping, and mechanical banding, although embolization may be successful as well. Refrac-tory cases may require gastrectomy (13,14).
Kommerell DiverticulumBurckhard Kommerell (1901–1990) (Fig 11a), a German radiologist, was the first to describe a diverticulum that he identified in a live patient in 1936. However, it was his subsequent successful defense of his thesis on the radiologic diagnosis of gallstones that secured him an appointment as a university lecturer (15). Although a Kommerell diverticulum is most frequently encountered with a right-sided aortic arch and an aberrant left sub-clavian artery, Kommerell made his observation in a patient with a left-sided arch and an aberrant right subclavian artery (Fig 11b) (16).
Vein of Galen Aneurysmal Malformation
Aelius Galenus of Pergamon (129–200) (Fig 12a) was a Greek philosopher-physician whose pro-lific writings make up one-half of all the ancient Greek medical literature available to us today. His patients included gladiators as well as emperor Marcus Aurelius. Galen’s research into anatomy was considered definitive for the next 1500 years. Among his myriad contributions was naming the great cerebral vein of Galen, although he prob-ably did not understand its significance (17).
The term vein of Galen aneurysmal malforma-tion is a misnomer; the malformation is really an arteriovenous fistula. Furthermore, a true vein of Galen aneurysmal malformation actually involves the embryonic median prosencephalic vein of Markowski, which regresses during nor-mal development. Clinically, the arteriovenous
RG • Volume 34 Number 4 DiPoce et al 1127
connection may result in high-volume heart failure, seizures, developmental delay, hydro-cephalus, and, rarely, subarachnoid hemorrhage. Endovascular embolization has become the standard of care (Fig 12b) (18).
Behçet SyndromeHulusi Behçet (1889–1948) (Fig 13a) was a Turkish dermatologist whose keen observations of a few patients over several years resulted in the discovery of a new disease. One of these patients had been followed up for more than 40 years and had been examined by physicians from as far away as Europe. Behçet published his findings in 1936, but it was not until 1947 that his name was given to the disease and its existence universally accepted (19). Behçet syndrome is characterized as a multisystem, relapsing inflammatory disorder with nonspecific vasculitis. Notably, Behçet syn-drome may involve arteries or veins of any size,
a characteristic that contributes to the variable manifestation of the syndrome (Fig 13b). Unfor-tunately, there is no pathognomonic finding, and the diagnosis is made clinically (20).
Budd-Chiari SyndromeBudd-Chiari syndrome is caused by hepatic venous outflow obstruction, which may be clas-sified as primary or secondary. Primary obstruc-tion results from an endoluminal source (eg, thrombus or a membrane), whereas secondary obstruction results from an external source (eg, external compression) (21). Some imag-ing findings include the presence of an enlarged caudate lobe, ascites, direct visualization of clot, and “spiderweb” collateral vessels seen at venography (Fig 14a) (22). Transjugular intra-hepatic portosystemic shunt placement may be performed to relieve fulminant hepatic failure resulting from Budd-Chiari syndrome (23).
Figure 10. (a) Paul Georges Dieulafoy (1839–1911). (b) Endoscopic image in a 68-year-old man with recurrent episodes of upper gastroin-testinal bleeding. Multiple endoscopies initially demonstrated a Dieu-lafoy lesion within the fundus. Two clips were placed endoscopically, followed by placement of three more clips 2 weeks later as bleeding con-tinued. (c) Angiogram shows an actively bleeding Dieulafoy lesion. Be-cause bleeding continued after endoscopic placement of the second clip, a coil was placed in the left gastric artery (arrow). The artery is promi-nent, with tortuous vasculature in the region of the endoscopic surgical clips (arrowhead) without an early draining vein to suggest arteriovenous malformation. Note also the blush of contrast material (*), a finding that is consistent with active extravasation. Coil placement proved ad-equate for treatment of the lesion, with cessation of hemorrhage.
1128 July-August 2014 radiographics.rsna.org
Figure 12. (a) Aelius Galenus of Pergamon (129–200). (b) Angiographic image in a 3-day-old male neonate depicts a large vein of Galen aneurysmal malformation (diagnosed postna-tally) with an early draining vein. The aneurysm is predominantly fed by a large right posterior cerebral artery, with drainage via the straight sinus. Treatment was delayed for 7 months because the patient was not experiencing heart failure; however, the patient did develop hy-drocephalus, which necessitated ventriculostomy. Catheter-directed coil embolization proved adequate, decreasing flow into the malformation by 90%.
George Budd (1808–1882) (Fig 14b) first described hepatic venous inflammation without defining the clinical parameters. Hans Chiari (1851–1916) (Fig 14c) later described in detail the clinical and pathologic underpinnings of hepatic venous occlusion, which he believed was secondary to syphilis (24). Chiari is perhaps better known for
his description of hindbrain malformations, now known as Chiari malformations. In addition, Chiari was the first to describe choriocarcinoma (25).
Buerger DiseaseFelix von Winiwarter (1852–1931) first de-scribed a patient’s loss of leg arteries and veins
Figure 11. (a) Burckhard Kom-merell (1901–1990). (b) Three-dimen-sional reconstructed CT image depicts a right-sided arch with an aberrant left subclavian artery (arrow). Note the diverticulum (ar-rowhead) at the ori-gin of the artery.
RG • Volume 34 Number 4 DiPoce et al 1129
Figure 14. (a) Venographic image depicts thrombus in a hepatic venous branch. Note the spiderweb collateral ves-sels in the thrombosed hepatic vein. Decompression of the vein was achieved with placement of a transhepatic por-tovenous shunt. (b) George Budd (1808–1882). (c) Hans Chiari (1851–1916).
Figure 13. (a) Hulusi Behçet (1889–1948). (b) Axial contrast-enhanced CT images through the abdomen in a 22-year-old woman with Behçet syndrome show multiple aneurysms in unusual locations (arrows), including the spleen and right lumbar artery.
in 1872, which he ascribed to overgrowth of the intima. He called the disease endarteri-tis obliterans. Leo Buerger (1879–1943) (Fig 15a), while at Mount Sinai Hospital in 1908, noted that the inflammation of the vascular wall caused thrombus formation, calling the disease thromboangiitis obliterans (26). Buerger disease (also known as Winiwarter-Buerger syndrome) is characterized as a nonatherosclerotic segmental inflammatory disease that is strongly associated with tobacco use (Fig 15b). Small and medium-sized arteries and veins in the extremities are affected. The disease may progress to the point where amputation is required; however, cessa-tion of smoking may reverse this progression. Unfortunately, revascularization and angioplasty
are not effective because of the diffuse and often distal distribution of the disease (27).
Churg-Strauss SyndromeJacob Churg (1910–2005) (Fig 16a) and Lotte Strauss (1913–1985) (Fig 16b) were pathologists who worked at the Mount Sinai School of Medi-cine after immigrating to the United States from Europe in the 1930s. In 1951, they collaborated in describing a condition that they called allergic granulomatosis, now known as Churg-Strauss syndrome. Churg-Strauss syndrome is a small-vessel vasculitis associated with asthma and eo-sinophilia. Pulmonary findings are most common and include bilateral subpleural consolidations with a lobular distribution, centrilobular nodules
1130 July-August 2014 radiographics.rsna.org
Figure 15. (a) Leo Buerger (1879–1943). (b) Arteriogram of the hand in a young male patient demonstrates the char-acteristic “corkscrew” appear-ance of the vessels and multiple occlusions (arrowhead) that involve the small and medium-sized arteries.
Figure 16. (a) Jacob Churg (1910–2005). (b) Lotte Strauss (1913–1985). (c) Axial CT image of the chest in a 64-year-old man with Churg-Strauss syndrome demon-strates bilateral subpleural consoli-dations (arrow), centrilobular nod-ules, and peribronchial thickening.
RG • Volume 34 Number 4 DiPoce et al 1131
Figure 17. Aortographic image in a patient with Harjola-Marable syndrome who reported experiencing postprandial pain shows the effect of respiratory motion on celiac artery stenosis. On expiration, the stenosis (arrowhead) is exac-erbated, with a kink and poststenotic dilatation. The stenosis improved on inspiration.
(especially in areas of ground-glass opacity), and multiple nodules with bronchial wall thickening (Fig 16c) (28,29).
Churg also made contributions to the field of renal pathology by introducing new stains, and he helped link asbestos exposure to mesothe-lioma. Strauss is considered one of the pioneers of pediatric and perinatal pathology (30).
Harjola-Marable SyndromeHarjola-Marable syndrome (also known as me-dian arcuate syndrome or celiac arterial compres-sion syndrome) is caused by compression of the celiac artery by the median arcuate ligament, with subsequent abdominal pain. The median arcuate ligament is a muscular band that joins the right and left diaphragmatic crura. Variations in respiratory motion are characteristic, and stenosis is exacerbated on expiration (Fig 17). CT arteri-ography is excellent for demonstrating the vascu-lar pathologic abnormality as well as the median arcuate ligament (31). Patients present with vague symptoms and, sometimes, postprandial pain. The anatomic basis for celiac artery com-pression was first observed by Benjamin Lipshutz in 1917. Further research by Pekka-Tapani Har-jola in 1963 and by J. David Dunbar and Samuel Marable in 1965 was conducted to define the clinical syndrome (32).
Kasabach-Merritt SyndromeKatharine Krom Merritt (1886–1986) and Haig Haigouni Kasabach (1898–1943) reported a case of thrombopenic purpura associated with benign hemangioma in an infant seen at the Columbia University Babies Hospital in 1940 (33). Since this initial description, the term Kasabach-Merritt syndrome has been loosely applied to common infantile hemangiomas and other vascular mal-formations associated with mild thrombocyto-penia (platelet counts of [100–150] × 103/mL, or [100–150] × 109/L). Other authors have argued that use of the term should be limited to cases of tufted angiomas or kaposiform hemangioendo-theliomas with more profound thrombocytopenia (platelet counts < 100 × 103/mL [100 × 109/L]). Kasabach-Merritt syndrome is believed to result from platelet trapping within the tumor, which in turn leads to intralesional bleeding and heman-gioma enlargement (34).
Kawasaki SyndromeTomisaku Kawasaki (1925– ) (Fig 18a) first observed a case of rash and fever in a 4-year-old child at the Red Cross Hospital in Tokyo, Japan, in 1961 (35). During the ensuing 6 years, he noted similar findings in 50 more patients, which prompted a report of his findings in 1967. Initially, he believed this disease to be self-lim-iting, but a subsequent Japanese case study of 10 autopsies indicated a link to sudden cardiac death. Although Kawasaki syndrome is now rec-ognized as the most common vasculitis of child-hood, some investigators have suggested that it may not have existed before 1950 (36).
Radiologic manifestations include aneurysms, stenosis, and occlusions of the coronary arteries (Fig 18b). Conventional angiography is con-sidered to be a high-risk examination in these patients for several reasons, including the risk of vessel thrombosis in a hypercoagulable postin-flammatory state (37). Therefore, noninvasive techniques, such as MR imaging and CT, have emerged as desirable alternatives for initial as-sessment and subsequent observation.
Klippel- Trénaunay-Weber Syndrome
Klippel-Trénaunay-Weber syndrome is character-ized by capillary, venous, and lymphatic malforma-tions with soft-tissue and bone hypertrophy (Fig 19a). Some authors distinguish between Klippel-Trénaunay and Parks-Weber syndrome, with the latter being characterized by the presence of arterio-venous shunting. The lower limb is most commonly affected, and when the syndrome affects the trunk, it almost never crosses the hemiabdomen (38).
1132 July-August 2014 radiographics.rsna.org
Figure 18. (a) Tomisaku Kawasaki (1925– ). (b) Axial contrast-enhanced CT image of the chest in an 11-year-old girl with a history of Kawasaki syndrome shows a massive saccular aneurysm of the left main coronary artery (arrow).
Figure 19. (a) Axial CT image in a 27-year-old woman with Klippel-Trénaunay-Weber syndrome depicts a massive vascular malformation. The malformation is seen in both the intraperitoneal compartment and the subcutaneous tissues that extend from the left hemiabdomen to the femur. Note also the inferior vena cava filter (arrow) in this patient, who had a history of deep venous thrombosis and pulmo-nary embolism (a known complication of Klippel-Trénau-nay-Weber syndrome). (b) Maurice Klippel (1858–1942). (c) Frederick Parkes Weber (1863–1962).
RG • Volume 34 Number 4 DiPoce et al 1133
Figure 21. (a) Axial contrast-enhanced CT image of the neck in an 18-year-old man with Lemierre syndrome shows a filling defect in the left internal jugular vein (arrow). The patient also had septic emboli to the lungs. (b) Andre Lemierre (1875–1956).
Maurice Klippel (Fig 19b) (1858–1942) and Paul Trénaunay (1875–1938) described the cardi-nal features of a syndrome they called naevus vari-queux osteohypertrophique in 1900. Seven years later, Frederick Parkes Weber (Fig 19c) (1863–1962) described similar conditions in three additional pa-tients. Klippel’s and Weber’s names are also used to describe several other conditions that they investi-gated: Klippel-Feil deformity, Klippel disease, Klip-pel-Feldstein syndrome, Sturge-Weber syndrome, Osler-Weber-Rendu syndrome, Weber-Cockayne syndrome, and Weber-Christian disease (39,40).
Kussmaul DiseaseAdolf Kussmaul (1822–1902) (Fig 20a) and Ro-dolf Maier (1824–1888) described the findings of polyarteritis nodosa in 1866. Initially, they called the condition human worm aneurysm, believing that the aneurysms were the result of parasitic infestation. However, microscopic examination demonstrated that the condition had an inflam-matory cause. Their complete evaluation of the disease, from laboratory testing to clinical exami-nation, was a novel way to investigate disease and set the tone for the coming century. Kussmaul
Figure 20. (a) Adolf Kuss-maul (1822–1902). (b) Arte-riogram in a patient with Kuss-maul disease demonstrates the characteristic finding of multi-ple variable-sized aneurysms in the kidney. Note the occlusion of vessels (arrow), as well as the beaded appearance of the small and medium-sized vessels. The large vessels are normal.
1134 July-August 2014 radiographics.rsna.org
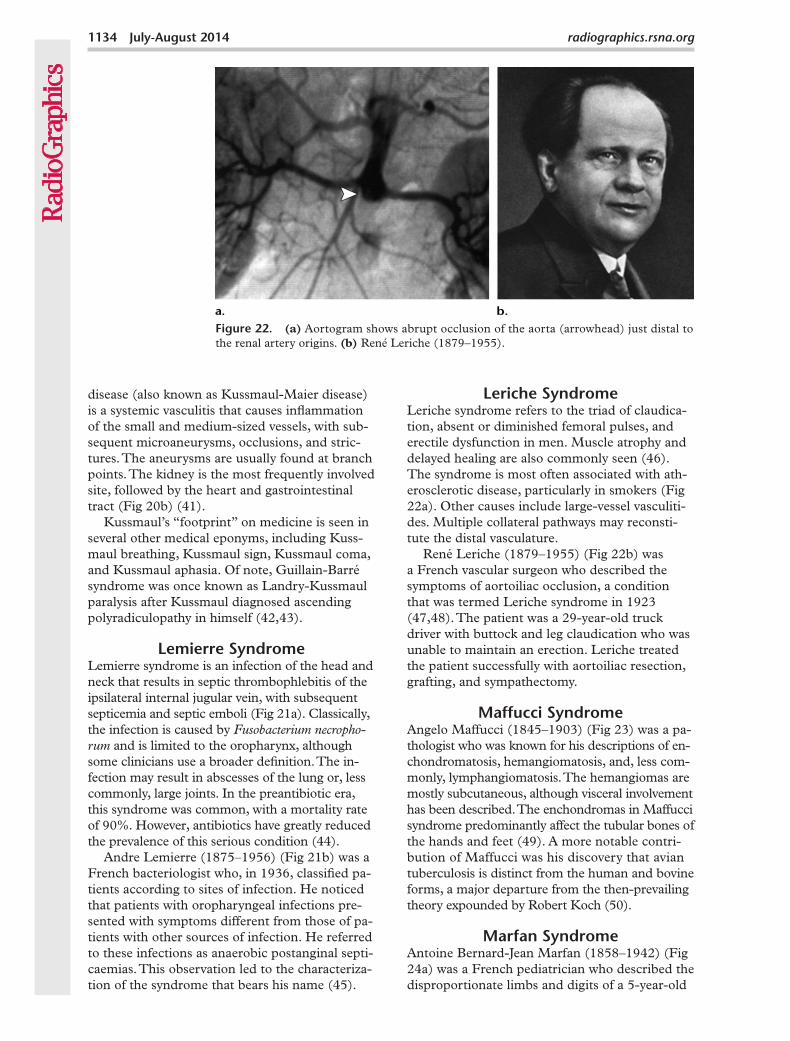
Figure 22. (a) Aortogram shows abrupt occlusion of the aorta (arrowhead) just distal to the renal artery origins. (b) René Leriche (1879–1955).
disease (also known as Kussmaul-Maier disease) is a systemic vasculitis that causes inflammation of the small and medium-sized vessels, with sub-sequent microaneurysms, occlusions, and stric-tures. The aneurysms are usually found at branch points. The kidney is the most frequently involved site, followed by the heart and gastrointestinal tract (Fig 20b) (41).
Kussmaul’s “footprint” on medicine is seen in several other medical eponyms, including Kuss-maul breathing, Kussmaul sign, Kussmaul coma, and Kussmaul aphasia. Of note, Guillain-Barré syndrome was once known as Landry-Kussmaul paralysis after Kussmaul diagnosed ascending polyradiculopathy in himself (42,43).
Lemierre SyndromeLemierre syndrome is an infection of the head and neck that results in septic thrombophlebitis of the ipsilateral internal jugular vein, with subsequent septicemia and septic emboli (Fig 21a). Classically, the infection is caused by Fusobacterium necropho-rum and is limited to the oropharynx, although some clinicians use a broader definition. The in-fection may result in abscesses of the lung or, less commonly, large joints. In the preantibiotic era, this syndrome was common, with a mortality rate of 90%. However, antibiotics have greatly reduced the prevalence of this serious condition (44).
Andre Lemierre (1875–1956) (Fig 21b) was a French bacteriologist who, in 1936, classified pa-tients according to sites of infection. He noticed that patients with oropharyngeal infections pre-sented with symptoms different from those of pa-tients with other sources of infection. He referred to these infections as anaerobic postanginal septi-caemias. This observation led to the characteriza-tion of the syndrome that bears his name (45).
Leriche SyndromeLeriche syndrome refers to the triad of claudica-tion, absent or diminished femoral pulses, and erectile dysfunction in men. Muscle atrophy and delayed healing are also commonly seen (46). The syndrome is most often associated with ath-erosclerotic disease, particularly in smokers (Fig 22a). Other causes include large-vessel vasculiti-des. Multiple collateral pathways may reconsti-tute the distal vasculature.
René Leriche (1879–1955) (Fig 22b) was a French vascular surgeon who described the symptoms of aortoiliac occlusion, a condition that was termed Leriche syndrome in 1923 (47,48). The patient was a 29-year-old truck driver with buttock and leg claudication who was unable to maintain an erection. Leriche treated the patient successfully with aortoiliac resection, grafting, and sympathectomy.
Maffucci SyndromeAngelo Maffucci (1845–1903) (Fig 23) was a pa-thologist who was known for his descriptions of en-chondromatosis, hemangiomatosis, and, less com-monly, lymphangiomatosis. The hemangiomas are mostly subcutaneous, although visceral involvement has been described. The enchondromas in Maffucci syndrome predominantly affect the tubular bones of the hands and feet (49). A more notable contri-bution of Maffucci was his discovery that avian tuberculosis is distinct from the human and bovine forms, a major departure from the then-prevailing theory expounded by Robert Koch (50).
Marfan SyndromeAntoine Bernard-Jean Marfan (1858–1942) (Fig 24a) was a French pediatrician who described the disproportionate limbs and digits of a 5-year-old
RG • Volume 34 Number 4 DiPoce et al 1135
Figure 24. (a) Antoine Bernard-Jean Marfan (1858–1942). (b) Axial contrast-enhanced CT image in a 33-year-old woman with Marfan syndrome shows a complication of this pathologic condition. Note the large aneurysm in the ascending aorta, as well as acute dissec-tion of both the ascending and descending aorta (arrows). Pericardial and right-sided pleural effusions are also seen. The patient required urgent replacement of the aortic root and hemiarch and fenestration of the distal aorta.
Figure 23. Angelo Maffucci (1845–1903).
girl named Gabrielle P. in 1896 (51). Marfan called the syndrome dolichosténomélie, meaning “slender limbs.” Marfan syndrome is an autosomal-domi-nant disorder with cardiovascular, musculoskeletal, integumentary, central nervous system, and ocular manifestations (52). The major cardiovascular diagnostic criteria for Marfan syndrome include annuloaortic ectasia and ascending aorta dissec-tion. The minor diagnostic criteria include mitral valve prolapse, mitral annulus calcification, main pulmonary arterial enlargement, aneurysmal dilata-tion, and dissection of the descending aorta (Fig 24b). Before modern advances in management, life expectancy was greatly reduced secondary to aortic dissection, congestive heart failure, or valve disease.
Notably, follow-up of Marfan’s index case by other physicians several years later demonstrated that Gabrielle P. probably had actually had con-genital contractural arachnodactyly syndrome. Marfan is also known for his many other scien-tific insights, including Marfan’s law, which states that persons exposed to tuberculosis early in life are less likely to be affected later in life (53).
May-Thurner SyndromeIn the 1850s, Rudolf Virchow observed that iliofemoral thrombosis occurred five times more frequently in the left leg than in the right leg (54). At the beginning of the 20th century, James McMurrich proposed an anatomic expla-nation for this finding. R. May and J. Thurner
1136 July-August 2014 radiographics.rsna.org
Figure 26. (a) Angiographic image in a 22-year-old male weightlifter depicts Paget-Schroetter syndrome. Occlusion of the axillary vein (arrow) was present before thrombolysis, with a few collateral vessels. Excellent flow was obtained after thrombolysis. (b) James Paget (1814–1899). (c) Leopold Schroetter Ritter von Kristelli (1837–1908).
performed biopsies in hundreds of patients 50 years later and confirmed McMurrich’s ex-planation (55). A few years later, Cockett and Thomas (Fig 25) clarified the syndrome’s clini-cal manifestation (56). Consequently, some au-thors have referred to the condition as Cockett syndrome.
May-Thurner syndrome (also known as iliac venous compression syndrome) is defined as compression of the left common iliac vein by the right common iliac artery against the lumbar vertebra. Chronic compression leads to intimal hyperplasia and fibrosis, followed by thrombosis. This can lead to chronic venous stasis ulcers, pulmonary embolism, or phlegmasia cerulea dolens. Interventional treatment options include throm-bolysis, stent placement, and placement of an
inferior vena cava filter. Surgical options include reconstruction or bypass (57).
Paget-Schroetter SyndromePaget-Schroetter syndrome (also known as Paget–von Schroetter syndrome or effort-induced thrombosis) is defined as upper-extremity deep venous thrombosis that typically occurs in the axillary or subclavian veins (Fig 26a). It most of-ten affects young, healthy males. Although Paget-Schroetter syndrome often occurs after vigorous activity, it may develop spontaneously or as a result of thoracic outlet syndrome (58).
James Paget (1814–1899) (Fig 26b) was a British physician whose many contributions to medicine are reflected in the many other ab-normalities that bear his name: Paget disease
Figure 25. Venographic image demonstrates compression of the left common iliac vein (straight arrow) by the overlying right iliac artery. Blood return from the left lower extremity is achieved through extensive collateral vessels, ultimately returning through the right common iliac vein (curved arrow indicates direction of flow). A stent was placed in the left common iliac vein, with good results.
RG • Volume 34 Number 4 DiPoce et al 1137
Figure 28. Antonio Valsalva (1666–1723).
Figure 27. Maurice Raynaud (1834–1881).
of the bone, Paget disease of the nipple, extra-mammary Paget disease, Paget abscess, and Paget recurrent fibroid (59). In 1875, Paget first noted that venous thrombosis can cause upper-extremity swelling. Leopold Schroetter Ritter von Kristelli (1837–1908) (Fig 26c) defined the clinical presentation of affected patients in 1884 (60).
Raynaud PhenomenonMaurice Raynaud (1834–1881) (Fig 27) was a French physician who, in 1862, first defined the syndrome that bears his name as episodic digital ischemia brought on by cold and emo-tion (61). Raynaud phenomenon is character-ized by episodic vasospasm and vasoconstriction of digital arteries. It may be primary or second-ary: The primary type is exacerbated by the cold, whereas the secondary type is associated with underlying arterial abnormality. Angio-graphic findings vary but may show spasm, poor visualization of distal branches, and hyperemia. Vasodilator therapy can improve these findings (62).
Sinus of Valsalva AneurysmAntonio Valsalva (1666–1723) (Fig 28) was an Italian physician whose primary research interest was hearing. He described the intricate anatomy of the ear and named the eustachian tube. He also described the Valsalva maneuver and noted the connection between hemiplegia and the con-
tralateral location of the causative brain lesion. His most famous student was Giovanni Battista Morgagni, who published a work in which Val-salva described the aortic sinuses (63).
In contrast to the diffuse annuloectatic aneu-rysm dilatation of the aorta and the three sinuses seen with connective tissue disorders (eg, Marfan syndrome), the sinus of Valsalva aneurysm typi-cally involves enlargement of only one or two of the aortic sinuses. Most sinus of Valsalva aneu-rysms are congenital, with a defect in the elastic lamellae of the affected sinus wall.
This aneurysm is considered a rare anomaly and is more common in men and Asian popula-tions. Complications include aortic regurgitation, mass effect on surrounding structures, myocar-dial ischemia, and rupture (64).
Takayasu ArteritisMikito Takayasu (1860–1938) (Fig 29a) was a Japanese ophthalmologist. In 1908, he first re-ported the case of a 21-year-old woman in whom coronary and arteriovenous anastomosis was seen at ophthalmologic examination. At the same meeting, two other ophthalmologists, Katsutomo Onishi and Tsurukichi Kagoshima, reported the same findings, as well as loss of distal arterial pulses. Yasuzo Shinmi is credited with first using the term Takayasu arteritis in 1939. Nonetheless, other physicians perhaps more inclusively refer to the disease as Takayasu-Onishi disease (65). Takayasu arteritis most commonly affects young
1138 July-August 2014 radiographics.rsna.org
Figure 30. (a) Carl Reinhold August Wunderlich (1815–1877). (b, c) Unenhanced CT image (b) and selective angiogram (c) of the right kidney in a 38-year-old woman who presented with abdominal pain and a decrease in hematocrit from a hemorrhagic angiomyolipoma. Note the large right peri- and pararenal hematoma (arrow in b) and the abnormal neovasculature in the lower pole (arrow in c). The patient subsequently underwent emboliza-tion with polyvinyl alcohol particles, with good results.
Asian women and involves the aorta and other large vessels. The early clinical manifestations of Takayasu arteritis often go unrecognized, but radiologic findings may be suggestive. Wall thick-ening is seen during the early phase of the dis-ease, whereas during the later (pulseless) phase, dystrophic calcification of the vessel intima and media is characteristic. Angiography commonly shows stenosis and, occasionally, aneurysmal dilatation (Fig 29b) (66).
Wunderlich SyndromeCarl Reinhold August Wunderlich (1815–1877) (Fig 30a) was a German physician and pioneer psychiatrist widely known for his determina-tion of mean human body temperature of 37°C (98.6°F), which has since been critically reevalu-ated (67).
Wunderlich syndrome is defined by spon-taneous, nontraumatic hemorrhage into the subcapsular and perirenal space (Fig 30b, 30c).
Figure 29. (a) Mikito Takayasu (1860–1938). (b) Sagittal maximum intensity projection CT image in a 16-year-old boy shows marked an-eurysmal dilatation of the ascending aorta (arrow). Circumferential soft-tissue thickening of the descending aorta (bracket) indicates active disease. Dystrophic calcification (arrowhead) is also noted, which dif-fers from the calcification caused by atherosclerotic disease.
RG • Volume 34 Number 4 DiPoce et al 1139
He first described the condition as spontaneous renal capsule apoplexy. Causes of Wunderlich syndrome include tumors, vascular disease, cysts, and inflammatory processes. Patients often pre-sent with the Lenk triad of acute flank pain, a palpable mass, and hypovolemic shock (68).
ConclusionEponyms are commonly used throughout medi-cine, and vascular radiology is no exception. Proficiency with clinical manifestations of epony-mous conditions is necessary. Familiarity with the physicians and their stories provides interesting background information and, in some instances, is useful for remembering clinical scenarios. Al-though some authors argue for a more limited use of eponyms in favor of more descriptive ter-minology, the rich flavor conveyed by an eponym is irreplaceable. Either way, eponyms are likely too imbedded in colloquial use to become anti-quated. Therefore, familiarity with both eponyms and their alternatives is needed.
References 1. Morgenstern L. Stenting...where credit is due. Surg
Guthikonda M, Rengachary SS. Albert Wojciech Adamkiewicz (1850-1921): unsung hero behind the eponymic artery. Neurosurg Focus 2009;26(1):E2.
3. Gourley EJ, Gering SA. The meandering mesenteric artery: a historic review and surgical implications. Dis Colon Rectum 2005;48(5):996–1000.
4. Meyers MA. Griffiths’ point: critical anastomosis at the splenic flexure—significance in ischemia of the colon. AJR Am J Roentgenol 1976;126(1):77–94.
5. van Gulik TM, Schoots I. Anastomosis of Riolan revisited: the meandering mesenteric artery. Arch Surg 2005;140(12):1225–1229.
6. Schultheiss D, Engel RM, Crosby RW, Lees GP, Truss MC, Jonas U. Max Brödel (1870-1941) and medical illustration in urology. J Urol 2000;164(4): 1137–1142.
7. Symonds C. The circle of Willis. BMJ 1955;1(4906): 119–124.
8. Kapoor K, Singh B, Dewan LI. Variations in the configuration of the circle of Willis. Anat Sci Int 2008;83(2):96–106.
9. Agarwal N, Chaudhari A, Hansberry DR, Presti-giacomo CJ. Redefining thalamic vascularization vicariously through Gerald Percheron: a historical vignette. World Neurosurg 2014;81(1):198–201.
10. Binder DK, Clusmann H, Schaller C. Friedrich-Christian Rosenthal: surgeon and anatomist. Neu-rosurgery 2006;59(6):1328–1333.
11. Mellick SA. Abernethy and the golden age of surgi-cal teaching. Aust N Z J Surg 1997;67(8):528–533.
12. Gallego C, Miralles M, Marín C, Muyor P, González G, García-Hidalgo E. Congenital hepatic shunts. RadioGraphics 2004;24(3):755–772.
13. Senger JL, Kanthan R. The evolution of Dieulafoy’s lesion since 1897: then and now—a journey through the lens of a pediatric lesion with literature review. Gastroenterol Res Pract 2012;2012:432517.
14. Durham JD, Kumpe DA, Rothbarth LJ, Van Stiegmann G. Dieulafoy disease: arteriographic findings and treatment. Radiology 1990;174(3 pt 2): 937–941.
15. van Son JA, Konstantinov IE. Burckhard F. Kom-merell and Kommerell’s diverticulum. Tex Heart Inst J 2002;29(2):109–112.
16. Berdon WE. Rings, slings, and other things: vascular compression of the infant trachea updated from the midcentury to the millennium—the legacy of Robert E. Gross, MD, and Edward B. D. Neuhauser, MD. Radiology 2000;216(3):624–632.
17. Ustun C. Galen and his anatomic eponym: vein of Galen. Clin Anat 2004;17(6):454–457.
18. Pearl M, Gregg L, Gandhi D. Cerebral venous development in relation to developmental venous anomalies and Vein of Galen aneurysmal malfor-mations. Semin Ultrasound CT MR 2011;32(3): 252–263.
19. Saylan T. Life story of Dr. Hulusi Behçet. Yonsei Med J 1997;38(6):327–332.
20. Chae EJ, Do KH, Seo JB, et al. Radiologic and clinical findings of Behçet disease: comprehensive review of multisystemic involvement. RadioGraphics 2008;28(5):e31.
21. Brancatelli G, Vilgrain V, Federle MP, et al. Budd-Chiari syndrome: spectrum of imaging findings. AJR Am J Roentgenol 2007;188(2):W168–W176.
22. Deutsch V, Rosenthal T, Adar R, Mozes M. Budd-Chiari syndrome. Study of angiographic findings and remarks on etiology. Am J Roentgenol Radium Ther Nucl Med 1972;116(2):430–439.
23. Cura M, Haskal Z, Lopera J. Diagnostic and in-terventional radiology for Budd-Chiari syndrome. RadioGraphics 2009;29(3):669–681.
24. Stanley P. Budd-Chiari syndrome. Radiology 1989; 170(3 pt 1):625–627.
25. Loukas M, Noordeh N, Shoja MM, Pugh J, Oakes WJ, Tubbs RS. Hans Chiari (1851–1916). Childs Nerv Syst 2008;24(3):407–409.
26. Ansari A. Thromboangiitis obliterans: current per-spectives and future directions. Tex Heart Inst J 1990;17(2):112–117.
27. Olin JW. Thromboangiitis obliterans (Buerger’s dis-ease). N Engl J Med 2000;343(12):864–869.
28. Choi YH, Im JG, Han BK, Kim JH, Lee KY, My-oung NH. Thoracic manifestation of Churg-Strauss syndrome: radiologic and clinical findings. Chest 2000;117(1):117–124.
29. Guillevin L, Cohen P, Gayraud M, Lhote F, Jar-rousse B, Casassus P. Churg-Strauss syndrome. Clinical study and long-term follow-up of 96 pa-tients. Medicine (Baltimore) 1999;78(1):26–37.
30. Hall of Fame at the Lillian and Henry M. Stratton-Hans Popper Department of Pathology. The Mount Sinai Hospital. http://www.mssm.edu/departments -and-institutes/pathology/about-us/hall-of-fame. Ac-cessed February 7, 2013.
31. Horton KM, Talamini MA, Fishman EK. Median arcuate ligament syndrome: evaluation with CT an-giography. RadioGraphics 2005;25(5):1177–1182.
32. Vaziri K, Hungness ES, Pearson EG, Soper NJ. Laparoscopic treatment of celiac artery compression syndrome: case series and review of current treat-ment modalities. J Gastrointest Surg 2009;13(2): 293–298.
33. Kasabach HH, Merritt KK. Capillary hemangioma with extensive purpura: Report of a case. Am J Dis Child 1940;59(5):1063–1070.
1140 July-August 2014 radiographics.rsna.org
34. Rodriguez V, Lee A, Witman PM, Anderson PA. Kasabach-Merritt phenomenon: case series and retrospective review of the mayo clinic experience. J Pediatr Hematol Oncol 2009;31(7):522–526.
36. Burns JC, Kushner HI, Bastian JF, et al. Kawasaki disease: a brief history. Pediatrics 2000;106(2):E27.
37. Takemura A, Suzuki A, Inaba R, et al. Utility of coronary MR angiography in children with Kawa-saki disease. AJR Am J Roentgenol 2007;188(6): W534–W539.
38. Cha SH, Romeo MA, Neutze JA. Visceral mani-festations of Klippel-Trénaunay syndrome. Radio-Graphics 2005;25(6):1694–1697.
39. Patel PR, Lauerman WC. Maurice Klippel. Spine 1995;20(19):2157–2160.
40. Curth HO. Frederick Parkes Weber (1863–1962). Arch Dermatol 1963;87:649–651.
41. Jee KN, Ha HK, Lee IJ, et al. Radiologic findings of abdominal polyarteritis nodosa. AJR Am J Roent-genol 2000;174(6):1675–1679.
42. Matteson EL. History of vasculitis: the life and work of Adolf Kussmaul. Cleve Clin J Med 2012;79 (suppl 3):S54–S56.
43. Breathnach CS, Westphal W. Adolf Kussmaul (1822-1902): from youth to maturity under the influence of Virchow. J Med Biogr 2003;11(1):55–61.
44. Screaton NJ, Ravenel JG, Lehner PJ, Heitzman ER, Flower CD. Lemierre syndrome: forgotten but not extinct—report of four cases. Radiology 1999;213 (2):369–374.
45. Riordan T, Wilson M. Lemierre’s syndrome: more than a historical curiosa. Postgrad Med J 2004;80 (944):328–334.
46. Leriche R, Morel A. The syndrome of thrombotic obliteration of the aortic bifurcation. Ann Surg 1948;127(2):193–206.
47. Leriche R. Des oblitérations artérielles hautes (obli-tération de la terminaison de l’aorte) comme cause des insuffisances circulatoires des membres inféri-eurs. Bull Mem Soc Chir 1923;1(49):1404–1406.
48. René Leriche; 1879-1955. Ann R Coll Surg Engl 1956;18(2):132–133.
49. Zwenneke Flach H, Ginai AZ, Wolter Oosterhuis J. Maffucci syndrome: radiologic and pathologic find-ings. RadioGraphics 2001;21(5):1311–1316.
50. Ciranni R, Giuffra V, Marinozzi S, Fornaciari G. An-gelo Maria Maffucci (1845-1903) and the beginning of pathological anatomy in Pisa [in Italian]. Med Secoli 2004;16(1):31–41.
51. Hecht F, Beals RK. “New” syndrome of congenital contractural arachnodactyly originally described by Marfan in 1896. Pediatrics 1972;49(4):574–579.
53. Theodore CM, Forster GE, Goh BT. Re-emergence of tuberculosis. BMJ 1993;306(6876):514–515.
54. McDermott S, Oliveira G, Ergül E, Brazeau N, Wicky S, Oklu R. May-Thurner syndrome: can it be diagnosed by a single MR venography study? Diagn Interv Radiol 2013;19(1):44–48.
55. May R, Thurner J. The cause of the predominantly sinistral occurrence of thrombosis of the pelvic veins. Angiology 1957;8(5):419–427.
56. Cockett FB, Thomas ML. The iliac compression syndrome. Br J Surg 1965;52(10):816–821.
57. Cil BE, Akpinar E, Karcaaltincaba M, Akinci D. Case 76: May-Thurner syndrome. Radiology 2004; 233(2):361–365.
59. Buchanan WW. Sir James Paget (1814–1894). Rheumatology (Oxford) 2003;42(9):1107–1108.
60. Illig KA, Doyle AJ. A comprehensive review of Paget-Schroetter syndrome. J Vasc Surg 2010;51(6): 1538–1547.
61. Belch JJ. The phenomenon, syndrome and disease of Maurice Raynaud. Br J Rheumatol 1990;29(3): 162–165.
62. Wahl S, Lakritz P. In: Bakal C, Silberzweig J, Cy-namon J, Sprayregen S, eds. Vascular and interven-tional radiology: principles and practice. New York, NY: Thieme Medical Publishers, 2002; 181–182.
63. Jellinek EH. The Valsalva manoeuvre and Antonio Valsalva (1666–1723). J R Soc Med 2006;99(9): 448–451.
64. Bricker AO, Avutu B, Mohammed TL, et al. Valsalva sinus aneurysms: findings at CT and MR imaging. RadioGraphics 2010;30(1):99–110.
65. Numano F. The story of Takayasu arteritis. Rheu-matology (Oxford) 2002;41(1):103–106.
66. Matsunaga N, Hayashi K, Sakamoto I, Ogawa Y, Matsumoto T. Takayasu arteritis: protean radiologic manifestations and diagnosis. RadioGraphics 1997; 17(3):579–594.
67. Mackowiak PA, Wasserman SS, Levine MM. A criti-cal appraisal of 98.6 degrees F, the upper limit of the normal body temperature, and other legacies of Carl Reinhold August Wunderlich. JAMA 1992;268 (12):1578–1580.
68. Albi G, del Campo L, Tagarro D. Wünderlich’s syn-drome: causes, diagnosis and radiological manage-ment. Clin Radiol 2002;57(9):840–845.
RadioGraphics 2014; 34:1120–1140 • Published online 10.1148/rg.344130125 • Content Code:
Page 1123In patients with Leriche syndrome (aortic occlusion), this represents an important collateral pathway, with anterograde flow through the arc of Riolan to the IMA. Conversely, in patients with SMA steno-sis, the flow is retrograde from the IMA through the arc of Riolan to the SMA.
Page 1126Abernethy malformations are anomalies of the venous system in which a congenital portosystemic shunt results from the persistence of embryonic vessels.
Page 1126Dieulafoy lesions are characterized by a single submucosal arteriole with abnormal branching or in-creased caliber. The pulsatile arteriole erodes through the mucosa, resulting in hemorrhage.
Page 1135The major cardiovascular diagnostic criteria for Marfan syndrome include annuloaortic ectasia and ascending aorta dissection. The minor diagnostic criteria include mitral valve prolapse, mitral annulus calcification, main pulmonary arterial enlargement, aneurysmal dilatation, and dissection of the descending aorta.
Page 1138The early clinical manifestations of Takayasu arteritis often go unrecognized, but radiologic findings may be suggestive.