INTERNATIONAL JOURNAL OF LEPROSY ^ Volume 52, Number I Printed in the Erythema Nodosum Leprosum (ENL). Ultrastructure of the Connective Tissue Response' Marian J. Ridley, Chris J. Heather, and Dennis S. Ridley 2 Recently we concluded that erythema no- dosum leprosum (ENL) supervenes in lep- romatous leprosy (LL) at a particular local antigen-antibody ratio when extravascular immune complexes are formed in slight an- tigen excess. The antigen is degraded cell walls, particulate acid-fast debris and a dif- fuse I3CG positive component, which can be detected in macrophages and neutrophils at the reaction site. lmmunoglobulin and complement are also present in these cells ( 4 ). We postulated that necrosis and edema associated with the reaction could cause dis- persal of antigen which might account for the connective tissue response in ENL. Al- though we could demonstrate immunoglob- ulins, complement, lysozyme, the coagula- tion protein plasminogen, and the acute phase reactants C-reactive protein (CRP) and 0-lipoprotein, bound to damaged con- nective tissue and elastic fibrils in the der- mis, we failed to demonstrate any antigen by light microscopy. Thus it was not clear whether the collagen damage was directly related to the leprosy bacilli. We therefore undertook this electron microscopic study to search for Mycobacterium leprac antigen in ENL of the New Guinea type with par- ticular attention to connective tissue. In these patients, the connective tissue re- sponse in the dermis is often very severe ( 2 ). Okada, et al. ( 1 ) have already demonstrated the presence of mycobacteria in association with ferritin-bound antibody in an ultra- structural study of ENL, but they were not concerned with the connective tissue far re- moved from the area of reaction. I Received for publication on 27 April 1983; ac- cepted for publication on 21 September 1983. 2 M. J. Ridley, B.Sc., Ph.D., Research Fellow, His- topathology, Hospital for Tropical Diseases, St. Pan- cras Way, London NW1 OPE; C. J. Heather, B.Sc., Ph.D., Electron Microscopist, Royal Army Medical College, Millbank, London SW1; D. S. Ridley, M.D., F.R.C.Path., Consultant Pathologist, Hospital for Tropical Diseases, St. Pancras Way, London NW1 Ol'E. England. MATERIAL AND METHODS Two biopsies of ENL included previously in histopathological studies ( 2 . 4 ) were avail- able for electron microscopy. The samples were finely divided into 1 mm 3 pieces and fixed in cold 3% glutaraldehyde in cacodyl- ate buffer, pH 7.4, for 3 hr before being transferred to a cacodylate-sucrose washing buffer. They were post-fixed in 1% osmium tetroxide, processed and embedded in epon. One micron sections were used for orien- tation of the block. Both biopsies came from New Guinea; biopsy A was from an acute dermal ENL and biopsy B was from an early resolving subacute lesion. RESULTS The connective tissue of both the acute as well as the subacute lesions is equally involved in the reaction. In both cases, most striking is the abundance of foamy mem- brane-bound sacs containing bacterial de- bris, widely distributed over the connective tissue, intimately impacted between colla- gen (Figs. 1 and 2). They appear to be intact phagosomes containing a serous material in which the debris is embedded. Some of the debris has the electron-transparent halo characteristic of mycobacteria. The debris comprises bits of cell wall which is the main component, and some electron-dense bac- terial cell bodies, presumably cytoplasm which is contained within degenerate cell walls. When the phagosome ruptures, the degenerate cell walls and debris are released into the extracellular space. The space is occupied by a homogeneous amorphous material and degenerate aggregated collagen fibrils on which bacterial debris is depos- ited. Elsewhere intact new collagen of band- ed appearance predominates, especially in the resolving lesion (Figs. 3 and 4). In the acute lesion, rounded monocytes have ingested large quantities of dispersed phagosomes (Fig. 5). The nucleus of these cells is similar to that of tissue macrophages. 61
Transcript
INTERNATIONAL JOURNAL OF LEPROSY^ Volume 52, Number I
Printed in the
Erythema Nodosum Leprosum (ENL). Ultrastructure of theConnective Tissue Response'
Marian J. Ridley, Chris J. Heather, and Dennis S. Ridley 2
Recently we concluded that erythema no-dosum leprosum (ENL) supervenes in lep-romatous leprosy (LL) at a particular localantigen-antibody ratio when extravascularimmune complexes are formed in slight an-tigen excess. The antigen is degraded cellwalls, particulate acid-fast debris and a dif-fuse I3CG positive component, which canbe detected in macrophages and neutrophilsat the reaction site. lmmunoglobulin andcomplement are also present in these cells( 4). We postulated that necrosis and edemaassociated with the reaction could cause dis-persal of antigen which might account forthe connective tissue response in ENL. Al-though we could demonstrate immunoglob-ulins, complement, lysozyme, the coagula-tion protein plasminogen, and the acutephase reactants C-reactive protein (CRP)and 0-lipoprotein, bound to damaged con-nective tissue and elastic fibrils in the der-mis, we failed to demonstrate any antigenby light microscopy. Thus it was not clearwhether the collagen damage was directlyrelated to the leprosy bacilli. We thereforeundertook this electron microscopic studyto search for Mycobacterium leprac antigenin ENL of the New Guinea type with par-ticular attention to connective tissue. Inthese patients, the connective tissue re-sponse in the dermis is often very severe ( 2 ).Okada, et al. ( 1 ) have already demonstratedthe presence of mycobacteria in associationwith ferritin-bound antibody in an ultra-structural study of ENL, but they were notconcerned with the connective tissue far re-moved from the area of reaction.
I Received for publication on 27 April 1983; ac-cepted for publication on 21 September 1983.
2 M. J. Ridley, B.Sc., Ph.D., Research Fellow, His-topathology, Hospital for Tropical Diseases, St. Pan-cras Way, London NW1 OPE; C. J. Heather, B.Sc.,Ph.D., Electron Microscopist, Royal Army MedicalCollege, Millbank, London SW1; D. S. Ridley, M.D.,F.R.C.Path., Consultant Pathologist, Hospital forTropical Diseases, St. Pancras Way, London NW1 Ol'E.England.
MATERIAL AND METHODSTwo biopsies of ENL included previously
in histopathological studies ( 2 . 4) were avail-able for electron microscopy. The sampleswere finely divided into 1 mm 3 pieces andfixed in cold 3% glutaraldehyde in cacodyl-ate buffer, pH 7.4, for 3 hr before beingtransferred to a cacodylate-sucrose washingbuffer. They were post-fixed in 1% osmiumtetroxide, processed and embedded in epon.One micron sections were used for orien-tation of the block. Both biopsies came fromNew Guinea; biopsy A was from an acutedermal ENL and biopsy B was from an earlyresolving subacute lesion.
RESULTSThe connective tissue of both the acute
as well as the subacute lesions is equallyinvolved in the reaction. In both cases, moststriking is the abundance of foamy mem-brane-bound sacs containing bacterial de-bris, widely distributed over the connectivetissue, intimately impacted between colla-gen (Figs. 1 and 2). They appear to be intactphagosomes containing a serous material inwhich the debris is embedded. Some of thedebris has the electron-transparent halocharacteristic of mycobacteria. The debriscomprises bits of cell wall which is the maincomponent, and some electron-dense bac-terial cell bodies, presumably cytoplasmwhich is contained within degenerate cellwalls. When the phagosome ruptures, thedegenerate cell walls and debris are releasedinto the extracellular space. The space isoccupied by a homogeneous amorphousmaterial and degenerate aggregated collagenfibrils on which bacterial debris is depos-ited. Elsewhere intact new collagen of band-ed appearance predominates, especially inthe resolving lesion (Figs. 3 and 4).
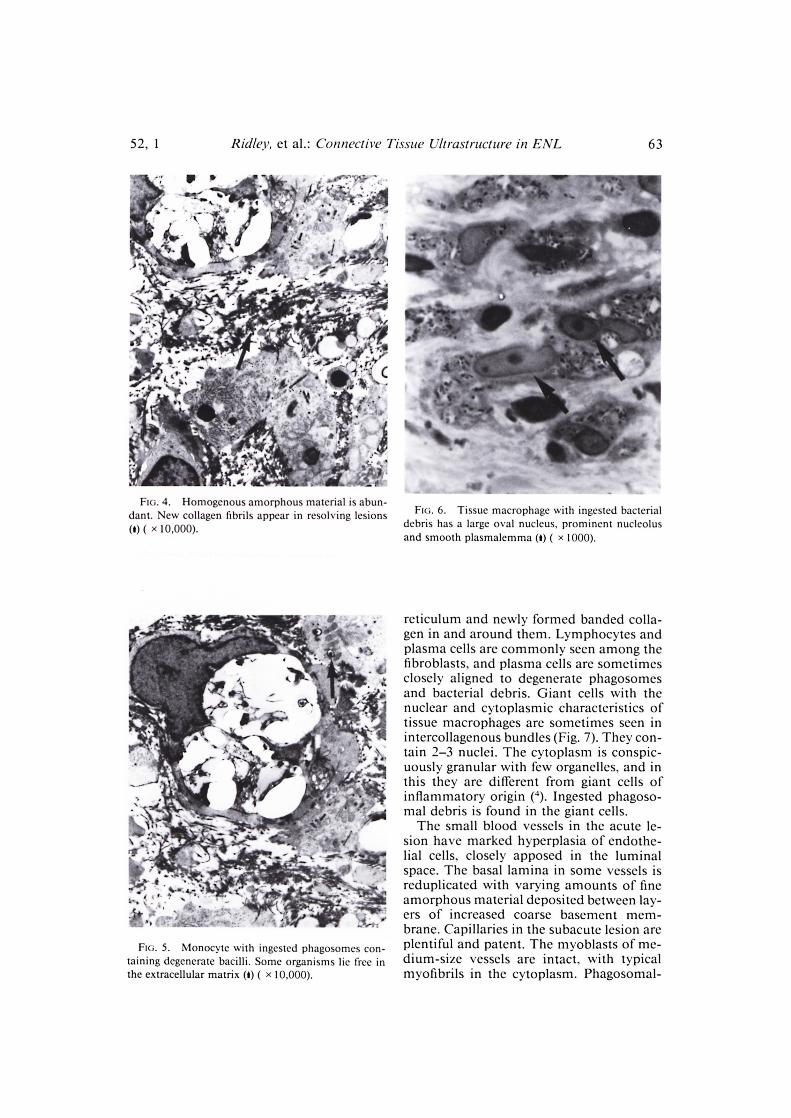
In the acute lesion, rounded monocyteshave ingested large quantities of dispersedphagosomes (Fig. 5). The nucleus of thesecells is similar to that of tissue macrophages.
FIG. I. Membrane-bound sacs containing unstain-able bacterial debris are distributed over collagen, caus-ing disruption of elastic (I) ( x 1000).
FRi. 2. Membrane-bound sacs appear to be intactphagosomes containing decayed bacterial debris (W.Degenerate collagen fibrils arc seen in a homogenousmatrix (I) ( x 10.000).
FIG. 3. Abundant degenerate bacterial debris de-posits in connective tissue far removed from the re-action site (I) ( x 500).
It is large with marginated chromatin andsometimes a conspicuous nucleolus is pres-ent. The scanty cytoplasm contains few or-ganelles. Other cells present in the edema-tous connective tissue are librocytes whichare very elongated cells with a slender palenucleus and inactive cytoplasm. Mast cellsare also seen, many of them showing de-generative changes.
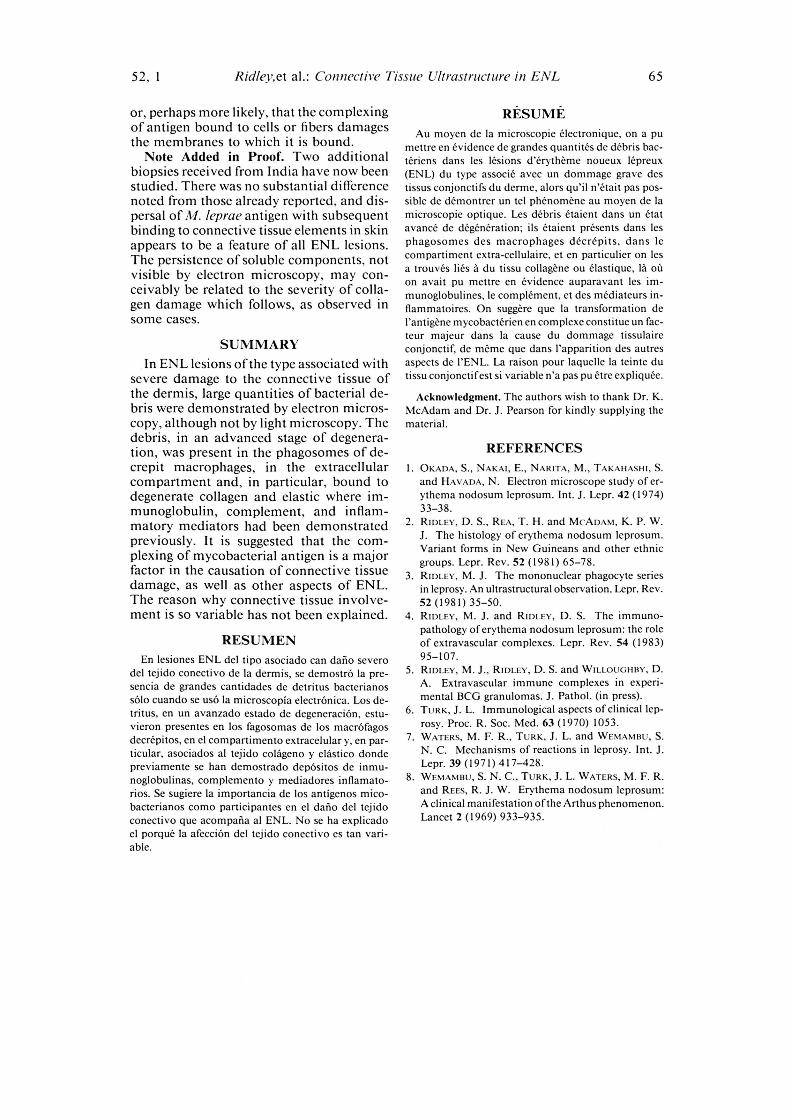
Spindle-shaped tissue macrophages arerecognized by a large pale oval nucleus witha rim of chromatin and prominent nucleo-lus. The cytoplasm is uniformly granularwith few organelles, inconspicuous Golgiapparatus, mitochondria, secretory vesi-cles, and varying amounts of ingestedphagosomes containing bacterial debris.They have a notably smooth plasmalemma(Fig. 6). Inflammatory macrophages, bycontrast, have an irregular nucleus and ac-tive plasmalemma. Closely associated withthe tissue macrophages are fibroblasts, dis-tinguished by distended rough endoplasmic
•411111111106`‘.1111117 4-1.7P4P s115•■■^•
52, 1^Ridley, et al.: Connective Tissue Ultrastruciure in ENL^63
FIG. 4. Homogenous amorphous material is abun-dant. New collagen fibrils appear in resolving lesions(I) ( x 10,000).
FIG. 6. Tissue macrophage with ingested bacterialdebris has a large oval nucleus, prominent nucleolusand smooth plasmalemma (t) ( x 1000).
FIG. 5. Monocyte with ingested phagosomes con-taining degenerate bacilli. Some organisms lie free inthe extracellular matrix (t) ( x 10,000).
reticulum and newly formed banded colla-gen in and around them. Lymphocytes andplasma cells are commonly seen among thefibroblasts, and plasma cells are sometimesclosely aligned to degenerate phagosomesand bacterial debris. Giant cells with thenuclear and cytoplasmic characteristics oftissue macrophages are sometimes seen inintercollagenous bundles (Fig. 7). They con-tain 2-3 nuclei. The cytoplasm is conspic-uously granular with few organelles, and inthis they are difkrent from giant cells ofinflammatory origin ( 4). Ingested phagoso-mal debris is found in the giant cells.
The small blood vessels in the acute le-sion have marked hyperplasia of endothe-lial cells, closely apposed in the luminalspace. The basal lamina in some vessels isreduplicated with varying amounts of fineamorphous material deposited between lay-ers of increased coarse basement mem-brane. Capillaries in the subacute lesion areplentiful and patent. The myoblasts of me-dium-size vessels are intact, with typicalmyofibrils in the cytoplasm. Phagosomal-
•
1
4.4
64^
International Journal of Leprosy^ 1984
FIG. 7. Giant cell has oval nuclei with prominentnucleolus and cytoplasm with few organelles. Ingestedphagosomes are seen containing decaying bacterial de-bris ( x 10,000).
bacterial debris is found between adjacentcells. Some perithelial cells have smallamounts of ingested bacterial debris andperithelial edema is present. The dermalnerves are unaffected by the reaction al-though they contain leprosy bacilli. Ncutro-phils are not seen around degenerating col-lagen.
DISCUSSIONBacterial antigen is detected with diffi-
culty in ENL using immunofluorescence,possibly because the antigen is degraded toan undetectable form ( 6 . 7 . 8). By the im-munoperoxidase technique and silver im-pregnation, bacterial components could bedetected more readily in and around thedegenerate macrophages on which the re-action was centered ( 4). But bacterial antigenwas often sparse or absent in the areas ofsevere acute and subacute connective tissuedamage in the dermis, which typifies theNew Guinean form of ENL ( 2 ) and is presentto some extent in other forms of ENL. Inthe present study, electron microscopydemonstrated a much greater amount of ex-
tracellular bacterial antigen in the form ofdegenerate organisms and debris, much ofit in the phagosomes set free by the disin-tegration of the macrophages. Although thestudy was confined to the New Guinea typeof ENL, it would be surprising if this findingdid not apply also to the other types in whichthe granulomatous involvement is moreprominent.
In the areas of connective tissue damageaway from the granuloma, degenerate col-lagen was seen to be embedded in a ho-mogeneous and edematous mass of tissuedebris, in which we had previously dem-onstrated immunoglobulins, complementcomponents and CRP, but not bacterial an-tigen. By electron microscopy, however,bacterial debris was easily demonstrableand, where present, it was associated withdegeneration of collagen or elastic fibers. Thebacterial debris was in an advanced stage ofdecay, which suggests that the failure to de-tect it by light microscopy was because muchof it had diffused away. The debris in theconnective tissue areas persisted into thesubacute phase of the reaction, in which col-lagen damage is still very evident. Combin-ing the evidence of the present study andearlier immunoperoxidase results, it is dem-onstrated that all of the components of my-cobactcrial immune complexes are presentin the areas of connective tissue damage,and there is no necessity to postulate non-mycobacterial antigens or auto-immunemechanisms to explain the connective tis-sue damage. However, it is not clear whythe damage should be so much greater insome forms of ENL than in others, or whythere should apparently be an ethnic pre-disposition to it.
It is highly unlikely that an organism withsuch a low toxicity for human tissue as Al.leprae should be responsible, per se, for acutedestruction of collagen and elastic tissue.Nor is there evidence that the degraded bac-terial components or the free antigen is muchmore toxic than the intact bacilli in the ab-sence ofdelayed hypersensitivity, which was,of course, lacking in our patients. This sup-ports our contention that immune com-plexes at an appropriate antigen-antibodyratio (probably near equivalence) may bemore damaging to tissue than uncomplexedantigen of a non-toxic sort ( -4 5). It may beeither that the complex itself is destructive
52, 1^Rid/ey,et al.: Connective Tissue Ultrastructure in EAT^65
or, perhaps more likely, that the complexingof antigen hound to cells or fibers damagesthe membranes to which it is bound.
Note Added in Proof. Two additionalbiopsies received from India have now beenstudied. There was no substantial differencenoted from those already reported, and dis-persal of M. leprae antigen with subsequentbinding to connective tissue elements in skinappears to be a feature of all ENL lesions.The persistence of soluble components, notvisible by electron microscopy, may con-ceivably be related to the severity of colla-gen damage which follows, as observed insome cases.
SUMMARYIn ENL lesions of the type associated with
severe damage to the connective tissue ofthe dermis, large quantities of bacterial de-bris were demonstrated by electron micros-copy, although not by light microscopy. Thedebris, in an advanced stage of degenera-tion, was present in the phagosomes of de-crepit macrophages, in the extracellularcompartment and, in particular, bound todegenerate collagen and elastic where im-munoglobulin, complement, and inflam-matory mediators had been demonstratedpreviously. It is suggested that the com-plexing of mycobacterial antigen is a majorfactor in the causation of connective tissuedamage, as well as other aspects of ENL.The reason why connective tissue involve-ment is so variable has not been explained.
RESUMENEn lesiones ENL del tipo asociado can dant) sever°
del tejido conectivo de la dermis, se demostrO la pre-sencia de grandes cantidades de detritus bacterianossolo cuando se use la microscopia electrOnica. Los de-tritus, en un avanzado estado de degeneraciOn, estu-vicron presentes en los fagosomas de los macrofagosdecrepitos, en el compartimento extracelular y, en par-ticular, asociados al tejido coldgeno y elastic° dondepreviamente se han demostrado depOsitos de inmu-noglobulinas, complemento y mediadores inflamato-rios. Se sugiere la importancia de los antigenos mico-bacterianos como participanles en el daft° del tejidoconectivo que acompana al ENL. No se ha explicadoel porque la afecciOn del tejido conectivo es tan vari-able.
RESUMEAu moycn de la microscopic electronique, on a pu
mcttre en evidence de grandes guanines de debris bac-teriens dans les lesions d'erytheme noueux lepreux(ENL) du type associe avec un dommage grave destissus conjonctifs du derme, alors qu'il n'etait pas pos-sible de demontrer un tel phenomene au moyen de lamicroscopic optique. Les debris etaient dans un etatavance de degeneration; ils etaient presents dans lesphagosomes des macrophages decrepits, dans lecompartimcnt extra-cellulaire, et en particulier on lesa trouves lies a du tissu collagene ou elastique, la onon await pu mettre en evidence auparavant les im-munoglobulines, le complement, et des maliateurs in-Ilammatoires. On suggere que la transformation del'antigene mycobacterien en complexe constitue un fac-teur majeur dans la cause du dommage tissulaireconjonctif, de meme que dans l'apparition des autresaspects de l'ENL. La raison pour laquelle la teinte dutissu conjonctifest si variable n'a pas pu etre expliguee.
Acknowledgment. The authors wish to thank Dr. K.McAdam and Dr. J. Pearson for kindly supplying thematerial.
REFERENCESI. OKADA, S., NAKAI, E., NARITA, M., TAKAHASHI, S.
and HAVADA, N. Electron microscope study of er-ythema nodosum leprosum. Int. J. Lepr. 42 (1974)33-38.
2. RIDLEY, D. S., REA, T. H. and McADANI, K. P. W.J. The histology of erythema nodosum leprosum.Variant forms in New Guincans and other ethnicgroups. Lepr. Rev. 52 (1981) 65-78.
3. RIDLEY, M. J. The mononuclear phagocyte seriesin leprosy. An ultrastructural observation. Lepr. Rev.52 (1981) 35-50.
4. RIDLEY, M. J. and R[DTTN, D. S. The immuno-pathology of erythema nodosum leprosum: the roleof extravascular complexes. Lepr. Rev. 54 (1983)95-107.
5. RIDTTv, M. J., RIDLEY, D. S. and WILLOUGHBY, D.A. Extravascular immune complexes in experi-mental 13CG granulomas. J. Pathol. (in press).
6. TURK, J. L. Immunological aspects of clinical lep-rosy. Proc. R. Soc. Med. 63 (1970) 1053.
7. WATERS, M. F. R., TURK, J. L. and WENIANIBIT, S.N. C. Mechanisms of reactions in leprosy. Int. J.Lepr. 39 (1971) 417-428.
8. WENIANIBU, S. N. C., TURK, J. L. WATERS, M. F. R.and REES, R. J. W. Erythema nodosum leprosum:A clinical manifestation of the Arthus phenomenon.Lancet 2 (1969) 933-935.