122
Essentials of Nephrology
| Date post: | 25-Dec-2015 |
| Category: |
Documents |
| Upload: | arnold-campbell |
| View: | 217 times |
| Download: | 1 times |

Essentials of Nephrology

Chronic kidney disease (CKD) can be defined as:
(A) Kidney damage as defined by pathologic abnormalities or markers in blood or urine for
1 mo(B) Kidney damage on imaging studies for 1
mo(C) Glomerular filtration rate (GFR) 60
mL/min per 1.73 m2 for 3 mo(D) Albumin to creatinine ratio of <30 mg of
albumin to 1 g of creatinine for 3 mo

Answer
• (C) Glomerular filtration rate (GFR) 60 mL/min per 1.73 m2 for 3 mo

Risk factors for CKD include which of the following?
(A) Systemic lupus (B) Bladder outlet obstruction
(C) Preeclampsia (D) All the above

Answer
• (D) All the above

In glomerulosclerosis:(A) Intraglomerular pressure
must be decreased to maintain function
(B) The efferent arteriole constricts
(C) GFR begins to decline early in disease process
(D) The mesangium becomes thin

Answer
• (B) The efferent arteriole constricts

When stratifying risk for cardiovascular disease in patients
with normal GFR and macroalbuminuria, CKD should
beconsidered a myocardial
infarction equivalent.(A) True (B) False

Answer
• (A) True

In the United Kingdom Prospective Diabetes
Study, the _______ control group had better renal
outcomes.(A) Blood pressure (BP)
(B) Glycemic
Answer
• (A) Blood pressure (BP)

Which class of antihypertensive agents appears most effective in
improving renal outcomes?(A) Calcium channel blockers(B) Angiotensin-converting
enzyme (ACE) inhibitors and angiotensin receptor blockers
(ARBs)(C) Direct renin inhibitors
(D) Beta-blockers

Answer
• (B) Angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs)

A patient with CKD is started on an ACE inhibitor to control her BP. During the first 2 to 4 wk of
therapy, a temporaryincrease in which of the
following can be expected?(A) Serum potassium
(B) Albumin to creatinine ratio(C) Serum creatinine
(D) GFR

Answer
• (C) Serum creatinine

What is considered an acceptable rise in the
creatinine after starting and ACE inhibititor?
• A. 10%
• B. 20%
• C. 30%
• D 40%

Answer
• C. 30%

Choose the correct statement about aliskiren.
(A) Blocks renin activity(B) Should be used in combination
with ACE inhibitor or ARB(C) Associated with better renal outcomes than ACE inhibitors or
ARBs(D) No significant effect on BP
control

Answer
• (A) Blocks renin activity

Which of the following drugs is contraindicated in patients with serum creatinine >1.4 mg/dL?
(A) Aliskiren (B) Amlodipene (C) Kayexalate (D) Metformin

Answer
• (D) Metformin

Dietary modifications of patients with CKD should include the
restriction of which of the following?(A) Protein
(B) Phosphate (C) Salt substitutes (D) All the above

Answer
• (D) All the above

Choose the correct statement about acute kidney injury.
(A) Characterized by rapid rise in creatinine over 1 mo
(B) Can be nonoliguric or oliguric
(C) Anuria usually associated with good prognosis
(D) Mortality rates lower in patients who require dialysis

Answer
• (B) Can be nonoliguric or oliguric

Intrinsic renal problems that lead to acute kidney injury are most
commonly caused by:(A) Pelvic cancer
(B) Vomiting (C) Congestive heart failure
(D) Medications

Answer
• (D) Medications

Values for fractional excretion of sodium are often elevated by:
(A) Diuretic use (B) Acute glomerulonephritis
(C) Rhabdomyolysis (D) Sepsis
Answer
• (A) Diuretic use

Which of the following findings on urinalysis with microscopy is
most commonly indicative of acute interstitial nephritis?
(A) Tubular epithelial cell casts (B) White blood cell casts (C) Red blood cell casts
(D) Hyaline casts
Answer
• (B) White blood cell casts

A urine dipstick can detect protein (albumin) at what level
• A. >30 mg of protein (albumin)
• B. >100 mg
• C. >300 mg
• D. >500 mg

Answer
• C. >300 mg

Which of the following is not an independent indication for emergent hemodialysis?
(A) Hyperkalemia(B) Uremic encephalopathy(C) Abnormal serum urea
nitrogen and creatinine levels(D) Metabolic acidosis

Answer
• (C) Abnormal serum urea nitrogen and creatinine levels

What is indicative of ATN
• tubular epithelial cell casts
• white cell casts without bacteria
• ask nephrologist to look for >10% eosinophils),
• red cell casts
• Hyaline casts
• oval fat bodies

Answer
• tubular epithelial cell casts

What is indicative of Nephrotic Syndrome
• tubular epithelial cell casts
• white cell casts without bacteria
• ask nephrologist to look for >10% eosinophils),
• red cell casts
• Hyaline casts
• oval fat bodies

Answer
• oval fat bodies

What is indicative of acuteinterstitial nephritis
• tubular epithelial cell casts
• white cell casts without bacteria
• ask nephrologist to look for >10% eosinophils
• red cell casts
• Hyaline casts
• oval fat bodies

Answer
• white cell casts without bacteria
• ask nephrologist to look for >10% eosinophils

What is indicative of glomerulonephritis
• tubular epithelial cell casts
• white cell casts without bacteria
• ask nephrologist to look for >10% eosinophils),
• red cell casts
• Hyaline casts
• oval fat bodies

Answer
• red cell casts

Using diuretics to convert oliguric renal failure to
nonoliguric renal failure may worsen mortality.(A) True (B) False

Answer
• (A) True

Choose the correct statement about screening for proteinuria.
(A) Can detect kidney disease even before changes in estimated
glomerular filtration rate (eGFR) occur
(B) Normal urinary protein to creatinine ratio <200 mg to 1 g
(C) 24-hr urine collection is gold standard, but prone to error
(D) All the above

Answer
• (D) All the above

A patient with an eGFR measurement of 45 mL/min per 1.73 m2 would most likely be
diagnosed with _______ chronickidney disease (CKD).
(A) Stage 1 (B) Stage 2
(C) Stage 3 (D) Stage 4

Answer
• (C) Stage 3

Prerenal is which of the following?
• A. Anything that causes decreased effective renal perfusion: Hypovolemia, CHF, Renal Artery Stenosis, Sepsis, etc. Sometines contrast-induced nephropathy
• B. ATN, AIN, Glomerulonephritides, etc
• C. Obstruction (BPH, bladder stone, bilateral ureter obstruction

Answer
• A. Anything that causes decreased effective renal perfusion: Hypovolemia, CHF, Renal Artery Stenosis, Sepsis, etc. Sometines contrast-induced nephropathy

Post renal is which of the following?
• A. Anything that causes decreased effective renal perfusion: Hypovolemia, CHF, Renal Artery Stenosis, Sepsis, etc. Sometines contrast-induced nephropathy
• B. ATN, AIN, Glomerulonephritides, etc
• C. Obstruction (BPH, bladder stone, bilateral ureter obstruction)

Answer
• C. Obstruction (BPH, bladder stone, bilateral ureter obstruction

Intrarenal is What?
• A. Anything that causes decreased effective renal perfusion: Hypovolemia, CHF, Renal Artery Stenosis, Sepsis, etc. Sometines contrast-induced nephropathy
• B. ATN, AIN, Glomerulonephritides, etc
• C. Obstruction (BPH, bladder stone, bilateral ureter obstruction
Answer
• B. ATN, AIN, Glomerulonephritides, etc

In patients with CKD, what is the recommended target level of low-
density lipoprotein?(A) <175 mg/dL (B) <150 mg/dL (C) <125 mg/dL (D) <100 mg/dL
Answer
•(D) <100 mg/dL

In patients with CKD, angiotensin-converting enzyme
inhibitor therapy should be discontinued if elevations in
creatinineoccur.
(A) True (B) False
Answer
• (B) False

What is high in Phosphorus?
A. MEATS, ETC
B. BREAD & STARCHES
C. DAIRY PRODUCTS
D. Fruits
E. Vegetables
F. A,B,C

Answer
• F. A,B,C

Acute kidney injury• Consider whether problem • Prerenal (problem of flow to kidneys)• Postrenal (obstructive process at level of ureter,
bladder, or urethra)• Or intrinsic (“is it the kidneys?”) 66% of time• Problem prerenal 10% of the time• Postrenal 33% of time• Intrinsic the rest of the time

Case presentation• man 55 yr of age with diabetes, hypertension, and degenerative joint disease (DJD) • presents with 3-day history of nausea, vomiting, diarrhea, and low oral intake• becomes oliguric, anuric, confused, and complains of pruritus• medications include benazepril hydrochlorothiazide, glipizide, and ibuprofen• physical examination—dehydration; hypotension; tachycardia; tachypnea; hypoxia; confusion• dry mucous membranes; rales on lung examination; no abdominal mass• normal prostate examination; no petechiae or purpura• laboratory studies—potassium high (6 mEq/L); sodium low (129 mEq/L); CO2 low (20 mEq/L); serum• urea nitrogen (BUN) high; creatinine high• treatment— normal saline boluses for hypotension• Foley catheter inserted to rule out obstruction (no urine excreted)• no acute changes on electrocardiography (ECG)• Hyperkalemia treated with transcellular shifting-mediated mechanism of insulin and glucose, calcium, and sodium polystyrene
to help bind potassium in gut• blood pressure (BP) medications and nonsteroidal anti-inflammatory drugs (NSAIDs) held• Urinalysis (UA) showed concentrated urine, with no red blood cells (RBCs), white blood cells (WBCs), or tubular cell casts
(acute tubular necrosis [ATN] ruled out)• renal ultrasonography (US) negative for hydronephrosis• patient's BP, urine output, mental status, BUN, and creatinine improved• Man discharged after few days with diagnosis of acute kidney injury (prerenal azotemia secondary to acute viral gastroenteritis)

Acute kidney injury• rapid rise in creatinine over 2 wk
• If baseline creatinine <2.5 mg/dL often defined as rise of 0.5 mg/dL
• if baseline creatinine >2.5 mg/dL, defined as increase in creatinine >20%
• can be nonoliguric or oliguric
• (oliguria in adults, urine output of <400 mL/day; in children <0.5 mL/kg per hr)
• anuria (urine output <100 mL/day) usually associated with poorer prognosis, except in dehydration
• mortality rates vary (25%-90%; in-hospital mortality, 50%)
• higher mortality rates usually seen in patients who require dialysis
• complications—electrolyte disorders (eg, hyperkalemia, metabolic acidosis)
• infections
• gastrointestinal (GI) bleeding
• arrhythmia
• Myocardial infarction (MI)
• pulmonary edema

Causes of acute kidney injury
• volume depletion—• decreased oral intake; vomiting; diarrhea; diuretic use; anaphylaxis; sepsis;
MI; congestive heart failure (CHF); cirrhosis;• signs of obstruction—patients often asymptomatic• abdominal or flank pain; hematuria; sudden anuria• weight loss or cancer symptoms (pelvic cancers lead to obstruction of ureters,
urethra, or bladder)• agitation• intrinsic renal problems—most commonly due to medications (eg, intravenous
[IV] contrast, aminoglycosides, amphotericin, penicillins, cephalosporins, sulfonamides); positive family history of kidney disease; personal renal history
• Autoimmune disease and vasculitis (eg, lupus, Sjögren’s syndrome)• viral diseases (eg, hepatitis B or C, HIV)

Consequences of acute kidney injury
• encephalopathy • Uremic pericarditis• CHF and fluid overload (eg, pulmonary or peripheral edema, significant hypertension)• acute platelet dysfunction• indications for dialysis• Physical examination: volume status; orthostatic vital signs;• dry mucous membranes; pericardial rub (pericarditis; emergent hemodialysis
indicated)• pulmonary edema• Bladder distention• petechiae might suggest uremic syndrome or thrombotic thrombocytopenic purpura
(TTP)• Palpable purpura suggest vasculitis• pelvic and prostate examination
Laboratory studies• complete blood cell count (CBC)• Platelet count normal in acute kidney failure• chemistry panel (CHEM- 7)• stat ECG• UA with microscopy• urine culture and renal US helpful• serum sodium and creatinine and urinary sodium and creatinine (to calculate fractional
excretion of sodium [FENa])• x-ray of kidneys, ureter, and bladder optional• computed tomog- raphy (CT) of abdomen for masses or symptoms suggestive of cancer• ECG in hyperkalemia—ventricular tachycardia or ventricular fibrillation can be
sudden or gradual• peaked T waves with prolonged PR intervals• with progression, P waves lost and QRS intervals widen with peaked T waves


Top 10 items for K+• Avocado540mg
• Cantaloupe494mg
• Tomatoes427mg
• Crimini Mushrooms390mg
• SwissChard364mg
• Spinach839mg
• Broccoli456mg
• Celery263mg
• Romaine Lettuce232mg
• Collard Green220mg

Low potassium fruits• FruitsPotassium Content (mg)Apples, peeled &
slides62Applesauce, canned78 – 92
• Apricot,1medium105
• Blueberries65Cranberry sauce36Fig (1 medium)116Fruit cocktail114Grapes (10)116Lemon (1 medium)80Peaches (canned)118Pears (canned)83Pineapple (diced)88Plums (raw)118Raspberries (raw)94Watermelon (diced)93Blackberries141Sweet cherries (10)152Grapefruit (1/2 medium)165

Low Potassium Vegetables• VegetablesPotassium Content (mg)Alfalfa
sprouts (raw)13Green beans76Bean sprouts63 - 78Cabbage (raw)72 - 86Cauliflower125Carrots (cooked)114Collards (cooked)84Collards (raw)214Corn (cooked)114Cucumbers (sliced)84Steamed eggplant119Endive (raw)79Leeks (raw)94Leeks (cooked)46Lettuce87Onions (cut into small cubes)124Peppers (raw)89Peppers (cooked)113

High Phosphorus Foods• Foods High in Phosphorus (greater than 160 mg per serving):
MEATS, ETC: Fish & Seafood (3 oz.) - Bass, Catfish, Clams, Cod, Crab (real and imitation), Flounder, Halibut, Orange Roughy, Pollack, Salmon (canned with bones), Sardines (canned with bones), Scallops (breaded and fried - 4 to 6 pieces), Shrimp (Breaded and Fried - 10 to 11 pieces), Swordfish, Trout, Tuna (canned in oil); Lamb (3 oz); Liver (3 oz); Pork (3 oz); Turkey (3 oz); Veal (3 oz)
BREAD & STARCHES: Bulgar (1/2 cup); Cornbread (prepared from dry mix) - 1 piece; Golden Grahams (3/4 cup); Frosted Mini-Wheats (1 cup); Kellogg's Raisin Bran (1 cup); Lentils, cooked (1/2 cup); Post Shredded Wheat (1 cup); Trail Mix (1/2 cup).
DAIRY PRODUCTS: Buttermilk (8 oz); Chocolate Milk (8 oz); Chocolate Pudding - instant (4 oz); Egg Nog (8 oz); Milk (8 oz.); Milkshakes (8 oz); Ricotta Cheese (1/2 cup); Swiss Cheese (1 oz); Yogurt (8 oz)
Foods Moderately High in Phosphorus (110-160 mg per serving):
MEATS, ETC: Bacon (2 slices); Beef (3 oz); Chicken (3 oz); Chicken Pot Pie (one small); Fish and Seafood (3 oz) - Lobster, Oysters, Perch, Steamed Shrimp, Tuna (canned in water)
BREAD & STARCHES: Biscuits (one 4-inch biscuit from recipe); Waffle (one from mix); Pancake (one from mix); Cheerios (1-1/4 cup); Wheaties (1 cup); Wheat CHEX (1 cup); Oatmeal (1 cup)
DAIRY PRODUCTS: Cheddar Cheese (1 oz.); Cottage Cheese (1/2 cup); Custard (1/2 cup); Fat-free Cream Cheese (2 Tbsp.); Mozzarella Cheese (1 oz.); Provolone Cheese (1 oz.); Pudding - instant, made with milk (1/2 cup)
DRIED BEANS & PEAS: Baked Beans (1/2 cup); Black-eyed Peas (1/2 cup); Black Beans (1/2 cup); Chili Beans (1/2 cup); Garbanzo Beans (1/2 cup); Kidney Beans (1/2 cup); Lima Beans (1/2 cup); Pinto Beans (1/2 cup); Refried Beans (1/2 cup)
NUTS & SEEDS: Almonds (22 nuts); Cashews (18 medium nuts); Pecans (20 halves); Pumpkin Seeds (50 seeds); Sunflower Seeds (50 seeds)
MISCELLANEOUS: Angel Food Cake (one piece); Beer (12 oz); Doughnut (one medium); Peanut Butter (2 Tbsp); Soy Milk (8 oz)

Foods Low in Phosphorus (less than 110 mg per serving)
• MEATS, ETC: Egg (one): Hot Dog (one); Sausage, fresh; Frozen Fish Sticks (two sticks)
BREAD & STARCHES: Bagel (one); all Bread (one slice); Biscuit (one made from refrigerated dough); Croissant (one); all Crackers (four); Cereals, including: Cocoa Puffs (1 cup); Corn, Rice CHEX (1 cup); Corn Flakes (1 cup); Corn Pops (1 cup); Cream of Wheat (3/4 cup); Kix (1-1/3 cup); Rice Krispies (1-1/4 cup); Special K (1 cup); English Muffin (one); Pasta (1/2 cup); Noodles (1/2 cup); Rice (1/2 cup); Popcorn (1 cup); Tortilla (one)
VEGETABLES All Vegetables are Low in Phosphorus
FRUITS: All Fruits are Low in Phosphorus
DAIRY PRODUCTS: Brie (1 oz); Cream Cheese (2 Tbsp); Feta Cheese (1 oz); Ice Cream (1/2 cup); Half & Half (1/2 cup); Grated Parmesan Cheese (2 Tbsp); Sour Cream (2 Tbsp); Whipping Cream (1/2 cup)
NUTS & SEEDS: Macadamia Nuts (12 nuts); Peanuts (28 nuts); Walnuts (14 halves)
MISCELLANEOUS: Cake (one piece); Coffee (6 oz); Cookie (one); Fruit Works; Hard Candy; Jelly Beans; Nestea COOL Iced Tea (8 oz); Non-dairy Creamer (1/2 cup); Pie (one piece); Ready-to-Eat Pudding (1/2 cup); Unenriched Rice Milk (8 oz); Snickers bar (one 2 oz bar); Soda Pop (12 oz); Tea (6 oz)

FENa• FENa—indicates how well kidneys retain sodium in setting of dehydration
• (urinary sodium/plasma sodium) ÷ (urinary creatinine/plasma creatinine) x 100
• obtain urinary and plasma values at same time of day
• <1% usually suggests prerenal etiology
• (>1% usually suggests ATN)
• FENa often elevated by diuretic use, or decreased due to certain intrinsic renal problems (eg, acute glomerulonephritis, ATN, rhabdomyolysis, contrast nephropathy, sepsis)
• Patients with chronic kidney disease can have chronically elevated FENa
• fractional excretion of urea—useful in patients with recent use of diuretic
• (urinary urea/plasma urea) ÷ (urinary creatinine/
• plasma creatinine) x 100
• <35% usually suggests prerenal etiology
• (>35% usually suggests ATN)
• more reliable than FENa; if clinical setting suggests prerenal etiology
• low urinary sodium and low fractional excretion of sodium confirm prerenal etiology
• FENa can be low in acute glomerulonephritis or vascular disorder
• in intrinsic renal problems, urinary sodium high
www.mdcalc.com fractional-excretion-of-sodium-fena
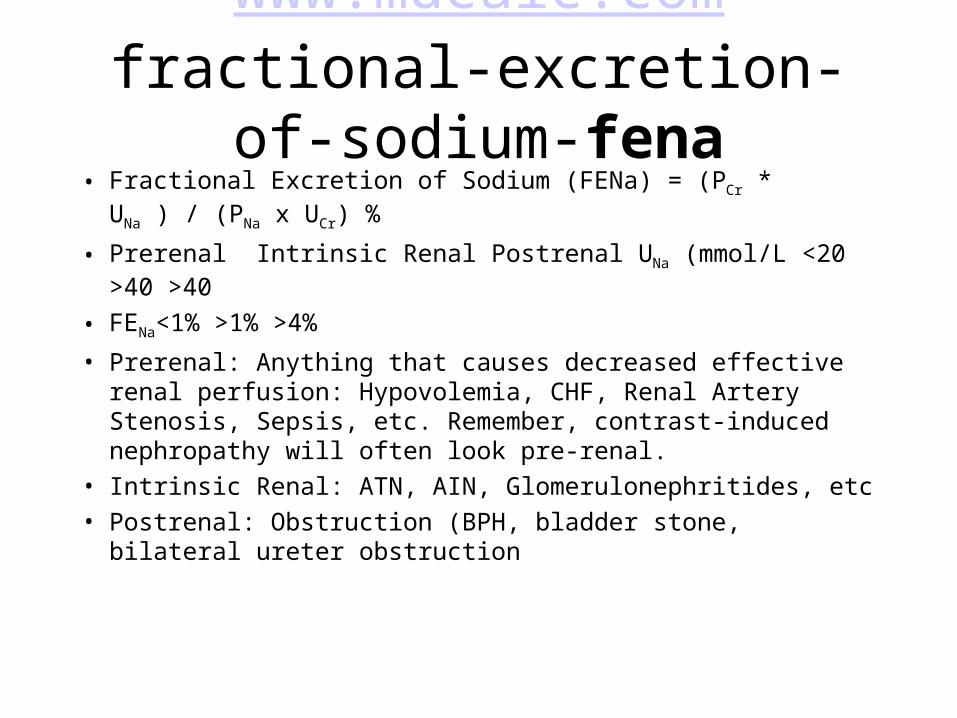
• Fractional Excretion of Sodium (FENa) = (PCr * UNa ) / (PNa x UCr) %
• Prerenal Intrinsic Renal Postrenal UNa (mmol/L <20 >40 >40
• FENa<1% >1% >4%
• Prerenal: Anything that causes decreased effective renal perfusion: Hypovolemia, CHF, Renal Artery Stenosis, Sepsis, etc. Remember, contrast-induced nephropathy will often look pre-renal.
• Intrinsic Renal: ATN, AIN, Glomerulonephritides, etc
• Postrenal: Obstruction (BPH, bladder stone, bilateral ureter obstruction

Acute tubular necrosis• Acute tubular necrosis is kidney injury characterized by acute tubular cell injury and dysfunction. Common causes are
hypotension causing renal hypoperfusion and nephrotoxic drugs. The condition is asymptomatic unless it causes renal failure. The diagnosis is suspected when azotemia develops after a hypotensive event, severe sepsis, or drug exposure and is distinguished from prerenal azotemia by laboratory testing and response to volume expansion. Treatment is supportive.
• Acute Tubular Necrosis
• Causes of acute tubular necrosis (ATN) include the following:
• Hypotension (ischemic ATN, common)
• Nephrotoxins (common)
• Sepsis (common)
• Major surgery
• Third-degree burns covering > 15% of BSA
• The heme pigments myoglobin and hemoglobin (uncommon)
• Disorders resulting in other endogenous toxins, such as tumor lysis or multiple myeloma (uncommon)
• Poisons, such as ethylene glycol (uncommon)
• Herbal and folk remedies, such as ingestion of fish gallbladder in Southeast Asia (uncommon)
• Common nephrotoxins include the following:
• Aminoglycoside antibiotics
• Amphotericin B
• Cisplatin
• Radiocontrast (particularly agents with osmolality > 100 mL)
• NSAIDs

Glomerulonephritis• Glomerulonephritis — an inflammation of the glomeruli — can damage your kidneys so that they lose their filtering ability, allowing dangerous levels of fluid
and waste to accumulate in your body (called kidney failure) and depriving your bloodstream of protein, which is excreted in your urine.
• Often the cause of glomerulonephritis is unknown. Known causes include:
• Infections
• Post-streptococcal glomerulonephritis. Glomerulonephritis may develop after a strep infection in your throat or, rarely, on your skin (impetigo). Post-infectious glomerulonephritis is becoming less common in the United States, most likely because of rapid and complete antibiotic treatment of most streptococcal infections.
• Bacterial endocarditis. Bacteria can occasionally spread through your bloodstream and lodge in your heart, causing an infection of one or more of your heart valves. Those at greatest risk are people with a heart defect, such as a damaged or artificial heart valve.
• Viral infections. Among the viral infections that may trigger glomerulonephritis are the human immunodeficiency virus (HIV), which causes AIDS, and the hepatitis B and hepatitis C viruses, which primarily affect the liver.
• Immune diseases
• Lupus. A chronic inflammatory disease, lupus can affect many parts of your body, including your skin, joints, kidneys, blood cells, heart and lungs.
• Goodpasture's syndrome. A rare immune lung disorder that may mimic pneumonia, Goodpasture's syndrome causes bleeding (hemorrhage) into your lungs as well as glomerulonephritis.
• IgA nephropathy. Characterized by recurrent episodes of blood in the urine, this primary glomerular disease results from deposits of immunoglobulin A (IgA) in the glomeruli. IgA nephropathy can progress for years with no noticeable symptoms. The disorder seems to be more common in men than in women.
• Vasculitis
• Polyarteritis. This form of vasculitis affects small and medium blood vessels in many parts of your body, such as your heart, kidneys and intestines.
• Wegener's granulomatosis. This form of vasculitis affects small and medium blood vessels in your lungs, upper airways and kidneys.
• Conditions that cause scarring of the glomeruli
• High blood pressure. Damage to your kidneys and their ability to perform their normal functions can occur as a result of high blood pressure. Glomerulonephritis can also cause high blood pressure because it reduces kidney function.
• Diabetic kidney disease. Diabetic kidney disease (diabetic nephropathy) can affect anyone with diabetes. Diabetic nephropathy usually takes years to develop. Good control of blood sugar levels and blood pressure may prevent or slow kidney damage.
• Focal segmental glomerulosclerosis. Characterized by scattered scarring of some of the glomeruli, this condition may result from another disease or occur for no known reason.

Acute Interstitial Nephritis• Overview of Acute Interstitial Nephritis (AIN)• The interstitium is the tissue that surrounds and imbeds the glomeruli (microscopic "filtering screens") and tubules (long tubes that connect with each
glomerulus and channel urine) within the kidneys. Acute interstitial nephritis (AIN) is rapidly developing inflammation that occurs within the interstitium. It can produce a variety of clinical symptoms, depending upon the severity and extent of kidney involvement.
• Causes of Acute Interstitial Nephritis (AIN)• Most AIN is caused by an acute allergic reaction to a medication, including antibiotics and nonsteroidal anti-inflammatory drugs (NSAIDs) such as:• Ibuprofen• Cephatholin• Cimetidine• Cyclosporine• Methicillin• Penicillins• AIN is also linked with certain infections and diseases such as Legionella pneumophila, collagen vascular diseases (e.g., sarcoidosis), streptococcal
infections, and transplant rejection.• Signs and Symptoms of Acute Interstitial Nephritis (AIN)• Indicators of AIN include a recent history of infection or the start of a new medication. Symptoms often include fever, rash, and generalized aches and pains.
Acute Interstitial Nephritis (AIN) Diagnosis• The definitive diagnosis of AIN requires a kidney biopsy, which reveals inflammation of the renal interstitium. Urinalysis (analysis of the urine) often reveals
eosinophils—specialized white blood cells that are seen in allergic reactions. Often one can detect increased eosinophils in the blood in patients with AIN. AIN sometimes is diagnosed by means of a gallium scan (nuclear medicine imaging method; a radiologist injects the patient with gallium-67, which will accumulate in areas of infection or malignancy and can be viewed with a special camera).
• Treatment for Acute Interstitial Nephritis (AIN)• All medication(s) believed to be responsible for the inflammation must be discontinued. If there is significant renal impairment, treatment with steroids
typically is required for 2 to 3 months. Stronger immunosuppressive agents may be needed if there is no response to the steroids. Each case of AIN must be reviewed by anephrologist (kidney specialist).
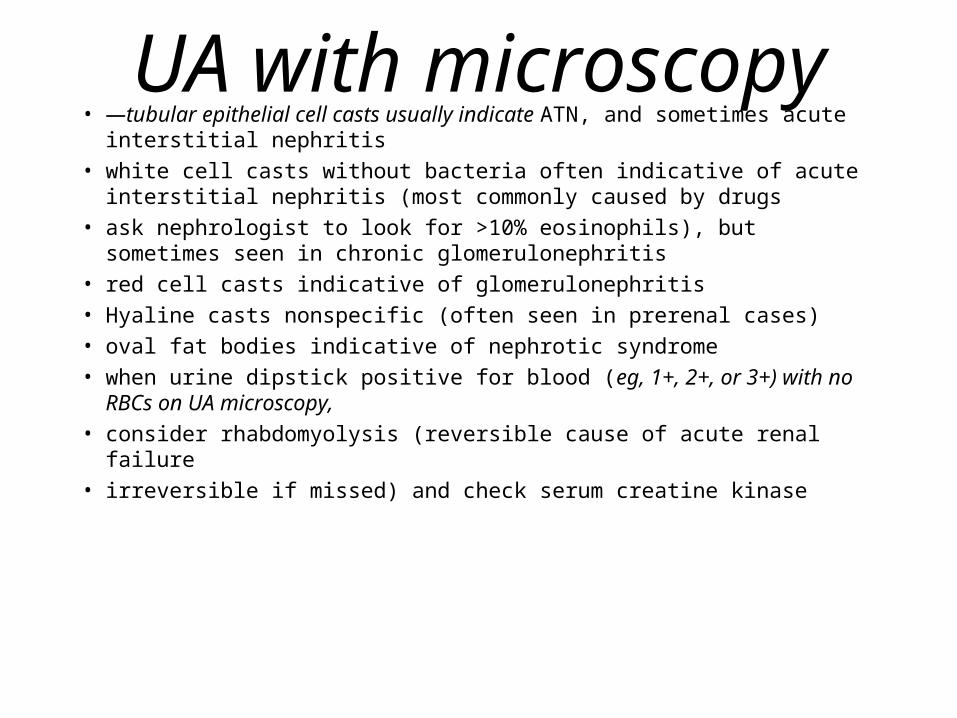
UA with microscopy• —tubular epithelial cell casts usually indicate ATN, and sometimes acute
interstitial nephritis• white cell casts without bacteria often indicative of acute interstitial nephritis
(most commonly caused by drugs• ask nephrologist to look for >10% eosinophils), but sometimes seen in
chronic glomerulonephritis• red cell casts indicative of glomerulonephritis• Hyaline casts nonspecific (often seen in prerenal cases)• oval fat bodies indicative of nephrotic syndrome• when urine dipstick positive for blood (eg, 1+, 2+, or 3+) with no RBCs on
UA microscopy,• consider rhabdomyolysis (reversible cause of acute renal failure• irreversible if missed) and check serum creatine kinase

Treatment before dialysis
• hyperkalemia—treat with glucose and insulin or IV calcium• sodium polystyrene (Kayexalate)• Furosemide• check ECG and monitor• CHF—treat with O2 and diuresis• severe acidosis—treat with sodium bicarbonate• NSAIDs and anticoagulants contraindicated in patients with
uremic pericarditis• avoid— potassium, potassium-sparing diuretics, angiotensin-
converting enzyme (ACE) inhibitors, NSAIDs, and IV contrast

Postrenal causes• Masses
• Tumors
• Stones
• anticholinergic drugs
• (eg, tricyclic antidepressants; diphenhydramine [eg, Benadryl])

Intrinsic renal causes• aortic dissection• 90% of time, due to ATN (often induced by hypotension)• most common problems due to nephrotoxic drugs and rhabdomyolysis (treat with hydration and IV
bicarbonate)• acute interstitial nephritis—can develop as late as 10 to 30 days after last drug dose• drug history important• only 33% of patients have eosinophils in urine (diagnostic finding)• vascular—less likely• emboli from left heart• aortic atheroma• Postaortic surgery• left heart endocarditis• atrial fibrillation• Renal artery stenosis (consider in young people with refractory hypertension) or thrombosis• Glomerulonephritis• Autoimmune diseases• renal infiltration (rare)

Nephritis• interstitial—clinical clues include fever, rash, and eosinophilia in blood; urine
sediment; protein in urine
• consider viral testing (for, eg, cytomegalovirus [CMV], HIV, hepatitis B virus [HBV]) and autoimmune testing (for, eg, sarcoidosis, Sjögren’s syndrome)
• Consult nephrologist before treating
• glomerulonephritis—
• clinical clues include preexisting infection (eg, Streptococcus), rash, arthritis
• urine sediment; RBC casts
• Protein in urine
• look for infections (eg, HIV, hepatitis B and C)
• in patients with rash or arthritis, look for cryoglobulinemia or lupus
• consider multiple myeloma in patients >40 yr of age (perform urine and serum protein electrophoresis)
• consult nephrologist

Vasculitis• clinical clues include fever, constitutional
symptoms, rash, respiratory symptoms
• RBC casts
• Autoimmune testing
• testing for HIV
• hepatitis B and C

Summary of acute renal failure• adjust doses of all drugs
• choose lowest dosing
• diuretics for converting oliguric to nonoliguric renal failure no longer used (benefits unclear and may worsen mortality)
• no benefit of low doses of dopamine
• prevention of contrast nephropathy—in patients with risk factors for acute renal failure (eg, advanced age, chronic kidney or liver disease)
• hold metformin, diuretics, and NSAIDs for 2 days
• start IV fluids or advise high oral fluid intake 1 day before
• giving sodium bicarbonate 1 hr before and 6 hr after may be beneficial (data conflicting);
• acetylcysteine (eg, Mucomyst; 600 mg bid) 1 day before and on day of study (controversial)

Chronic kidney disease (CKD)• definition—kidney damage as defined by pathologic abnormalities or markers in blood or urine or on
imaging studies for 3 mo• or glomerular filtration rate (GFR) <60 mL/min per 1.73 m2 for 3 mo• stage 0—presence of risk factors (eg, hypertension, diabetes), but no evidence of kidney damage• Stages 1 to 5—progressive loss of glomerular filtration (ie, renal function)• prevalence—in 1997, prevalence in United• States 10% (currently, 13.1% [26 million people])• worldwide—affects 50 million people (1 million patients on renal replacement therapy [eg, dialysis,
transplantation])• United States—474,000 people have had• renal replacement therapy• costs—total Medicare payments in 2007, $333 billion ($23 billion spent on endstage renal disease)• average lifetime cost of patients on dialysis, $250,000 to $300,000• emotional burden on patient• increased demands on caregivers• early detection and treatment can delay or prevent progression

Stages of Chronic Kidney Disease
• Stage 1 Slightly diminished function; Kidney damage with normal or relatively high GFR (>90 mL/min/1.73 m2). Kidney damage is defined as pathologic abnormalities or markers of damage, including abnormalities in blood or urine test or imaging studies.
• Stage 2 Mild reduction in GFR (60-89 mL/min/1.73 m2) with kidney damage. Kidney damage is defined as pathologic abnormalities or markers of damage, including abnormalities in blood or urine test or imaging studies.
• Stage 3 Moderate reduction in GFR (30-59 mL/min/1.73 m2). British guidelines distinguish between stage 3A (GFR 45-59) and stage 3B (GFR 30-44) for purposes of screening and referral.[4]
• Stage 4 Severe reduction in GFR (15-29 mL/min/1.73 m2) Preparation for renal replacement therapy
• Stage 5 Established kidney failure (GFR <15 mL/min/1.73 m2, or permanent renal replacement therapy (RRT)
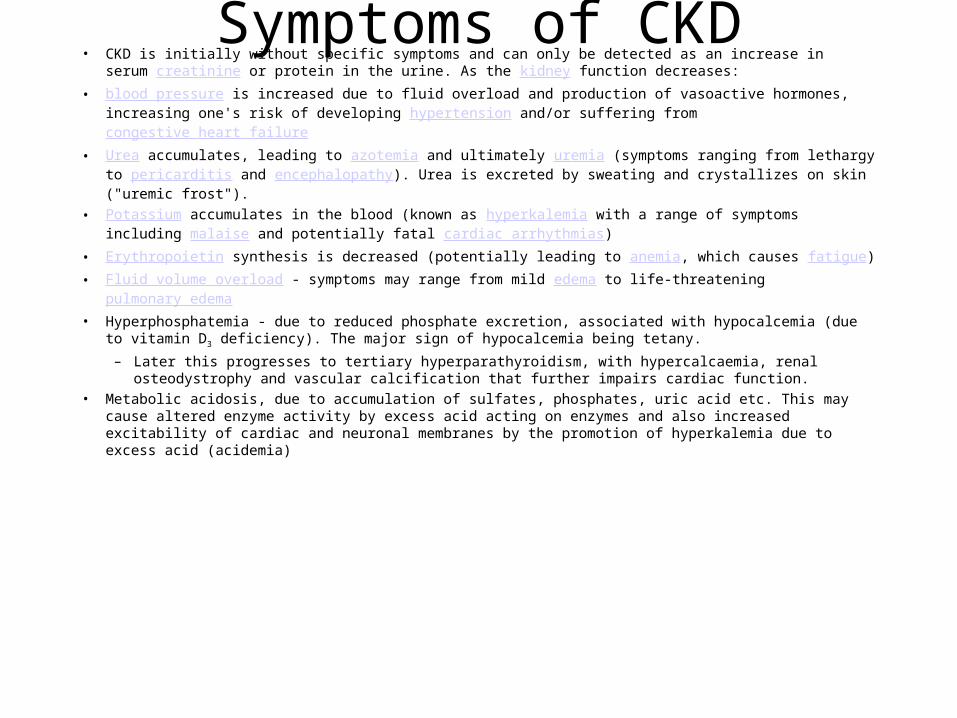
Symptoms of CKD• CKD is initially without specific symptoms and can only be detected as an increase in serum creatinine
or protein in the urine. As the kidney function decreases:
• blood pressure is increased due to fluid overload and production of vasoactive hormones, increasing one's risk of developing hypertension and/or suffering from congestive heart failure
• Urea accumulates, leading to azotemia and ultimately uremia (symptoms ranging from lethargy to pericarditis and encephalopathy). Urea is excreted by sweating and crystallizes on skin ("uremic frost").
• Potassium accumulates in the blood (known as hyperkalemia with a range of symptoms including malaise and potentially fatal cardiac arrhythmias)
• Erythropoietin synthesis is decreased (potentially leading to anemia, which causes fatigue)
• Fluid volume overload - symptoms may range from mild edema to life-threatening pulmonary edema
• Hyperphosphatemia - due to reduced phosphate excretion, associated with hypocalcemia (due to vitamin D3 deficiency). The major sign of hypocalcemia being tetany.
– Later this progresses to tertiary hyperparathyroidism, with hypercalcaemia, renal osteodystrophy and vascular calcification that further impairs cardiac function.
• Metabolic acidosis, due to accumulation of sulfates, phosphates, uric acid etc. This may cause altered enzyme activity by excess acid acting on enzymes and also increased excitability of cardiac and neuronal membranes by the promotion of hyperkalemia due to excess acid (acidemia)

Causes• The most common causes of CKD are diabetic nephropathy, hypertension,
and glomerulonephritis.[3] Together, these cause approximately 75% of all adult cases. Certain geographic areas have a high incidence of HIV nephropathy.
• Historically, kidney disease has been classified according to the part of the renal anatomy that is involved, as:[citation needed]
• Vascular, includes large vessel disease such as bilateral renal artery stenosis and small vessel disease such as ischemic nephropathy, hemolytic-uremic syndrome and vasculitis
• Glomerular, comprising a diverse group and subclassified into– Primary Glomerular disease such as focal segmental glomerulosclerosis and IgA
nephritis– Secondary Glomerular disease such as diabetic nephropathy and lupus nephritis
• Tubulointerstitial including polycystic kidney disease, drug and toxin-induced chronic tubulointerstitial nephritis and reflux nephropathy
• Obstructive such as with bilateral kidney stones and diseases of the prostate• On rare cases, pin worms infecting the kidney can also cause idiopathic nephropathy.

Treatment• The goal of therapy is to slow down or halt the otherwise relentless progression of CKD to stage 5.
Control of blood pressure and treatment of the original disease, whenever feasible, are the broad principles of management. Generally, angiotensin converting enzyme inhibitors (ACEIs) or angiotensin II receptor antagonists (ARBs) are used, as they have been found to slow the progression of CKD to stage 5.[5][6] Although the use of ACE inhibitors and ARBs represents the current standard of care for patients with CKD, patients progressively lose kidney function while on these medications, as seen in the IDNT[7] and RENAAL[8] studies, which reported a decrease over time in estimated glomerular filtration rate (an accurate measure of CKD progression, as detailed in the K/DOQI guidelines[1]) in patients treated by these conventional methods.
• Currently, several compounds are in development for CKD. These include, but are not limited to, bardoxolone methyl[9], olmesartan medoxomil,sulodexide, and avosentan[10].
• Replacement of erythropoietin and vitamin D3, two hormones processed by the kidney, is usually necessary in patients with CKD, as is calcium.Phosphate binders are used to control the serum phosphate levels, which are usually elevated in chronic kidney disease.
• When one reaches stage 5 CKD, renal replacement therapy is required, in the form of either dialysis or a transplant.
• In some cases, dietary modifications have been proven to slow and even reverse further progression. Generally this includes limiting protein intake.[citation needed]
• The normalization of hemoglobin has not been found to be of any benefit

2nd Hyperparathyroidism
• The major factors responsible for stimulating parathyroid gland function in renal failure are hypocalcemia, diminished 1,25-dihydroxyvitamin D levels, and hyperphosphatemia.
• The optimal approach for treating secondary hyperparathyroidism and mineral metabolism abnormalities in predialysis patients with stage 3, 4, and 5 chronic kidney disease (CKD) is unclear. The current management of secondary hyperparathyroidism in patients with stage 3 to 5 CKD not yet on dialysis principally involves the administration of some combination of dietary phosphate restriction, phosphate binders (either calcium or non-calcium containing binders), vitamin D analogues, calcium supplementation and/or (possibly) a calcimimetic. However, calcimimetics are NOT currently approved for patients with CKD not yet undergoing dialysis.

2nd HyperparathyroidismThe elevated phosphorus level in the blood can cause deposits of calcium and
phosphorus to form in tissues, including the blood vessels. Restricting the intake of foods that are high in phosphorus, such as dairy products, liver, legumes, nuts, and most soft drinks, lowers the phosphate concentration in the blood. Drugs that bind phosphate, such as calcium carbonate
, calcium acetate, and sevelamer
, taken by mouth, may also lower the phosphorus level in the blood. Calcium citrate should be avoided. Calcium citrate is found in many calcium supplements and is in many products as a food additive (sometimes called E333). Vitamin D
and similar drugs are often taken by mouth to reduce high levels of parathyroid hormone.

2nd Hyperparathyroidism• We suggest that the initial focus in managing secondary hyperparathyroidism should be the
management of hyperphosphatemia. Among patients with hyperphosphatemia, we suggest restricting dietary phosphate intake.
• - Among patients with hyperphosphatemia despite dietary phosphorus restriction after two to four months, we suggest the administration of phosphate binders. The two principal options are calcium and non-calcium based phosphate binders. Specific interventions are based upon serum phosphate and calcium levels.
• We also suggest that treatment with ergocalciferol be initiated if vitamin D deficiency exists, as demonstrated by a 25(OH)-vitamin D (calcidiol) level of less than 30 ng/mL.
• - If elevated PTH levels remain despite ergocalciferol and phosphate binder therapy over a six-month period, we suggest administering a low dose active oral vitamin D analog. If the serum level of corrected total calcium exceeds 10.2 mg/dL (2.54 mmol/L), we recommend that ergocalciferol therapy and all forms of vitamin D therapy should be discontinued
• - The next step is to decide whether phosphate binder therapy is sufficient or whether a vitamin D analogue should be added. This is based upon calcium, phosphate, and PTH levels that are measured when administering optimal phosphate binder therapy.

Chronic Kidney Disease (CKD)• Screening for CKD: screen patients with risk factors (eg, diabetes,
hypertension, age >60 yr)
• positive family history, history of recurrent urinary tract infection (UTI) or obstruction
• or systemic illness (eg, autoimmune disease, vasculitis)
• less common risk factors
• reasons for screening—to slow disease progression
• to prevent or reduce risk for cardiovascular disease
• check BP and creatinine
• CHEM-7
• random urine sample for protein or albumin to creatinine ratio
• UA with microscopy
Estimated glomerular filtration rate (eGFR)
• normal GFR, 95 to 120 mL/min per 1.73 m2• GFR decreases with age• Average decline is 1 mL/min/year after age 30• Renal dysfunction can occur despite normal
creatinine• eGFR better measure of kidneys’ ability to filter,
and helps detect early kidney disease• calculation based on age, sex, and ethnicity (ie,
black or white)
Pathophysiology of glomerulosclerosis
• kidney exposed to insults (ie, hypertension and hyperglycemia) and responds by dilating renal arteries
• increased flow and increased pressure due to underlying pathology cause mesangial cell injury, leading to microscopic scarring within glomerulus
• other glomeruli work harder, while exposure of nephrons to higher pressure and higher glycemic environment and scarring continue
• over time, kidney fails to adapt and GFR begins to decline further in disease process (early screening and detection important)
Adaptive mechanism to increase GFR in CKD• afferent and efferent arterioles can regulate incoming and outgoing blood
and pressure independently, or collaborate to adjust intraglomerular pressure
• in glomerulosclerosis—intraglomerular pressure must be increased to maintain function
• efferent arteriole constricts
• slightly dilated afferent arteriole and constricted efferent arteriole cause increased intraglomerular pressure
• in hypovolemia—dehydration decreases intraglomerular pressure
• afferent arteriole dilates and efferent arteriole constricts to maintain intraglomerular pressure
• Normal adaptive mechanism in hypovolemia
• maladaptive mechanism in glomerulosclerosis, since increasing intraglomerular pressure leads to more scarring

Pathophysiology of albuminuria
• normally, capillary bed (glomerulus) and surrounding capsule of interdigitating podocytes create pores that filter urea and electrolytes, while retaining proteins and sugar
• in glomerulosclerosis, thickening of mesangium leads to dysfunctional podocytes and enlarged pores, allowing passage of albumin (sensitive marker for early kidney damage)

Albumin to creatinine ratio• can be performed on spot urine• best when performed on early morning urine• Compares amount of albumin in urine compared to amount of creatinine in urine; normal, <30
mg of albumin to 1 g of creatinine• microalbuminuria, 30 to 300 mg of albumin to 1 g of creatinine• macroalbuminuria, >300 mg of albumin to 1 g of creatinine• women have higher tolerance range than Men• if abnormal for >3 mo, patient meets definition for CKD• as kidney disease worsens, albumin to creatinine ratio increases• modify therapy based on amount of excreted albumin• morphologic changes in kidney present in 50% of patients with microalbuminuria• in 25% to 50% of patients, microalbuminuria presents before evidence of retinopathy• albumin to creatinine ratio linearly correlated to risk for cardiovascular disease, central nervous
system disease, myocardial infarction (MI), and stroke• when risk stratifying patients with normal GFR and macroalbuminuria, CKD should be
considered as MI equivalent

Screening for proteinuria• can detect kidney disease even before changes in eGFR occur
• proteinuria associated with more rapid decline of kidney function
• reducing proteinuria slows progression of CKD; treat with ACE inhibitor or angiotensin receptor blocker (ARB)
• urine dipstick detects large amounts (>300 mg) of protein (albumin)
• measure albumin directly in patients with microalbuminuria
• 24-hr urine collection gold standard for protein, but inconvenient and prone to error
• measure protein or albumin to creatinine ratio
• normal urinary protein to creatinine ratio, <200 mg to 1 g (for albumin, <30 mg to 1 g)
• microalbuminuria, 30 to 300 mg of albumin to 1 g of creatinine
• macroalbuminuria, >300 mg of albumin to 1 g of creatinine
• in patients with protein in urine, obtain total protein to creatinine ratio
• In patients with risk factors and positive dipstick (protein >30 mg), perform albumin or total protein to creatinine ratio
• perform 24- hr urine for patients “in extremes” (eg, extremes of age or weight, high muscle mass) or with malnutrition, muscle diseases, paraplegia, vegetarianism, pregnancy

Estimating GFR• equation for calculating eGFR from Modification of Diet and
Renal Disease (MDRD) study— available for personal digital assistants (eg, Palm Pilots)
• based on laboratory studies that do not require 24-hr urine collection
• revised equation (CKD Epidemiology Collaboration Equation) maintains accuracy at lower GFR (eg, <60 mL/min per 1.73 m2), but more accurate at higher GFR (eg, 80-100 mL/min per 1.73 m2)
• MDRD equation highly accurate, except when 1) patient emaciated due to eg, anorexia with extremely low total body protein load (inaccuracy, 20%), or 2) patient obese (eg, body weight >400 lb)

Diagnosing CKD• presence of kidney damage for >3 mo (based on abnormal structure
on imaging study or abnormal function), or eGFR <60 mL/min per 1.73 m2 for >3 mo
• end-stage renal disease—eGFR <15 mL/min per 1.73 m2 (kidney failure)
• need for dialysis or transplantation
• stages—stage 5 most severe
• stage 3, eGFR, 30 to 60 mL/min per 1.73 m2
• eGFR underestimates renal function at normal creatinine levels
• (eg, creatinine of 0.6 mg/dL may correlate with stage 1 eGFR value
• creatinine of 0.9 mg/dL may correlate with lower eGFR)
• eGFR values <60 mL/min per 1.73 m2 reliable

Diagnosing CKD• CKD commonly caused by diabetic kidney disease, vascular problem (eg, hypertension, large
vessel disease), and glomerular diseases (eg, tubular interstitial disease, drug toxicities)• in patients with risk factors for parenterally transmitted diseases consider eg, HIV, hepatitis B
and C, associated kidney diseases• in patients with rash, consider lupus and cryoglobulinemia• laboratory studies—recent UA• CHEM-7• Urine protein or albumin to creatinine ratio• renal US—may show stones, hydronephrosis, or cysts• small hyperechoic kidneys generally indicate CKD• large kidneys may be associated with hydronephrosis (obstructive process), or infiltrating
process (eg, sarcoidosis or lymphoma)• size disparity between kidneys indicates renal vascular disease (eg, fibromuscular dysplasia or
renal artery thrombosis)• slow progression of CKD by controlling BP, glucose, and proteinuria

Evaluation• in most patients, CKD caused by diabetes and
hypertension• when cause of CKD unknown, consider antinuclear
antibody testing, serum protein electrophoresis, and complete blood count
• complement testing to screen for glomerulonephritis• perinuclear antineutrophil cytoplasmic antibody• renal ultrasonography to look for enlarged, polycystic, or
extremely small kidneys• no added value from computed tomography

Management• blood pressure (BP) control and glycemic control• evaluate cardiovascular risk• dietary modification (consider referral to nutritionist)• anticipate complications and refer to specialist• hypertension and proteinuria— independent variables that predict long-term decline of kidney
disease• kidney disease can cause hypertension• Sclerosing and fibrosing kidney leads to systemic response of elevated BP• reduction of BP reduces cardiovascular and renal risk• reduction of proteinuria lowers cardiovascular risk and improves endothelial cell function• Uncontrolled BP results in more rapid decline in renal function• United Kingdom Prospective Diabetes Study (UKPDS) found that patients with BP control had
better renal outcomes than patients with glycemic control• BP control—large studies show 3 to 4 medications needed• aggressive management needed• BP goal, 130/80 mm Hg (reducing BP too much can worsen renal failure)

(ACE) inhibitors and (ARBs)• from renal standpoint, angiotensin modulation therapy more effective than other
medications
• reduce BP with better outcomes in patients with CKD
• decrease progression to macroalbuminuria
• decrease albumin excretion
• Restore ion charge and membrane permeability components to glomerulus
• indications for ACE inhibitors—type 1 diabetes with microalbuminuria
• hypertension and type 2 diabetes with microalbuminuria
• some evidence that treating normotensive patients who have type 2 diabetes with ARB or ACE inhibitor does not affect renal outcomes
• follow-up in 1 mo
• ACE inhibitors and ARBs inhibit efferent arterioles from constricting, leading to decreased intraglomerular pressure (reduces GFR and increases serum creatinine)

(ACE) inhibitors and (ARBs)• expected changes in serum creatinine—during first 2 to 4 wk of
starting ACE inhibitor or ARB, creatinine may increase due to decreased intraglomerular pressure
• increase usually not >30% above baseline, and generally returns to baseline within 1 to 2 mo
• if increase >30%, monitor patient carefully and consider discontinuing agent
• after serum creatinine returns to baseline, check every 6 mo• risk for hyperkalemia— slightly increased risk with use of ACE
inhibitor or ARB• rare; start patients on low-potassium diet and loop diuretic• when GFR <30 mL/min per 1.73 m2, hydrochlorothiazide ineffective

(ACE) inhibitors and (ARBs)• counsel patients about avoiding nonsteroidal anti-inflammatory drugs
(NSAIDs), including ibuprofen and cyclooxygenase-2 inhibitors
• Sodium polystyrene sulfonate (SPS; eg, Kayexalate) sometimes used to maintain potassium
• combining ACE inhibitors and ARBs—may improve outcomes, but Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial (ONTARGET) showed decline in
• outcomes (eg, cardiovascular mortality, renal outcomes)
• ACE inhibitor and ARB may be combined cautiously after trying all other options for BP control
• monitor creatinine every 3 mo and watch patients carefully
• decline in outcomes seen in patients with congestive heart failure (especially those on Beta-blocker therapy)

Aliskiren• direct renin inhibitor
• blocks renin activity
• Effective for BP control
• data about renal effects limited
• recommend against combining with ACE inhibitor or ARB
• studies show ACE inhibitors and ARBs better agents for renal outcomes

Amlodipine
• trial found patients on amlodipine alone had worse renal outcomes (calcium channel blockers cause afferent arteriole to dilate more than efferent arteriole, leading to increased intraglomerular pressure)
• provides good BP control (especially in black patients)
• data show good outcomes when combined with ACE inhibitor or ARB

Nighttime dosing• trial saw statistically significant reduction
in cardiovascular mortality with nighttime dosing of antihypertensive agents

Prevention of overt nephropathy• tight glycemic control important• Diabetes Control and Complications Trial Cohort (Epidemiology of Diabetes
Interventions and Complications [EDIC] Study) showed good outcomes and reduction in nephropathy in patients with tight glycemic control
• continuous gradient exists between hyperglycemia and microvascular complications (ie, retinopathy and nephropathy)
• evidence suggests glycemic control can reduce nephropathy• Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial and Action
in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial found glycemic control not as effective as BP control (ADVANCE trial
• stopped early due to higher cardiovascular mortality in tight glycemic control group)
• metformin contraindicated in patients with serum creatinine >1.4 mg/dL

Prevention of overt nephropathy
• in ACCORD and ADVANCE trials, tight glycemic control did not improve overall cardiovascular outcomes, but renal outcomes improved
• diabetes, CKD, and cardiovascular disease must be managed together; in patients with CKD, death from cardiovascular event 10 times more likely than dialysis
• CKD predicts cardiovascular disease (consider aspirin therapy)• counsel patients about weight loss and tobacco cessation• control lipids• atorvastatin shown to improve renal function)• dietary modifications—restrict salt intake to 2.5 to 3.5 g/day (difficult;
patients at stage 4 CKD lose sense of taste)• protein restriction (difficult without assistance of nutritionist)• phosphate restriction

Complications• Hyperkalemia• Hyperphosphatemia• hypocalcemia• (secondary hyperparathyroidism)• Hyponatremia• Decreased immunoglobulins• dyslipidemia—coronary artery disease number 1 cause of mortality in patients
with CKD• animal studies suggest dyslipidemia can worsen kidney function• recent meta-analysis of 13 small studies showed lipid reduction might preserve
GFR• patients with CKD tend to have high triglycerides and elevated low-density
lipoprotein (LDL) to high-density lipoprotein (HDL) ratios

Hyperkalemia• During chronic kidney failure, fluid intake may need to be
restricted to prevent the sodium concentration in the blood from becoming too low. Foods that are extremely high in potassium, such as salt substitutes, must be avoided, and foods that are somewhat high in potassium, such as dates, figs, and many other fruits, should not be consumed in excess. (See the National Kidney Foundation's Fact Sheet on Potassium in the diet for more information.) A high potassium level in the blood increases the risk of abnormal heart rhythms and cardiac arrest. If the potassium level becomes too high, drugs such as sodium polystyrene sulfonate may help, but emergency dialysis may be required.

Complications• guidelines recommend aggressive targets (eg, LDL <100 mg/dL, triglycerides <200 mg/dL)
• hypertension—ACE inhibitors and ARBs preferentially lower glomerular pressures and reduce proteinuria
• in patients with normal urine protein, target BP, <130/80 mm Hg
• in patients with protein in urine, target BP, <125/75 mm Hg
• when starting ACE inhibitors in CKD patients, GFR initially decreases, and creatinine increases mildly <30%
• check CHEM-7 1-2 wk after initiating therapy
• do not discontinue therapy unless increase does not stabilize
• Monitor anemia—normochromic; normocytic; hypoproliferative;
• caused by low erythropoietin
• reduces quality of life
• Causes fatigue and can lead to cardiomyopathy from left ventricular
• hypertrophy; correction of anemia may help improve CKD;
• recommended hemoglobin (Hb) target, 10 g/dL to 12 g/dL
• check ferritin and supplement with iron if indicated
• Give erythropoietin to predialysis patients if Hb <10 g/dL;

Complications• Renal osteodystrophy—common
• early CKD patients have hyperphosphatemia and increased parathyroid hormone (PTH), resulting in increased bone turnover, decreased bone strength, and fractures
• check PTH and restrict dietary phosphate intake
• treat with calcium acetate and vitamin D
• refractory patients may need surgical treatment to remove parathyroid

Nutrition and lifestyle
• CKD patients at risk for malnutrition
• study showed patients on restricted protein diet did not fare better
• refer patients to nutritionist and consult nephrologist
• be aggressive about tobacco smoking cessation
• social support and screening for depression

When to refer to nephrologist
• underlying cause unclear after work-up
• need for biopsy
• diagnosis unclear
• stage 3 or 4 CKD rapid progression of CKD or superimposed acute kidney failure
• www.kidney.org or www.mdrd.com useful resources

Questions and answers• salt substitutes—should be avoided due to high potassium content
• management of CKD, proteinuria, and hypertension—control BP first
• consider increasing ACE inhibitor or ARB if indicated
• Incidental finding of trace or 1+ protein on urine dipstick in otherwise healthy patient—various proteins (eg, tubular protein, albumin) excreted in urine
• perform albumin to creatinine ratio or urine proteinelectrophoresis to identify protein
• whitecoat hypertension—diagnose hypertension based on clinical findings in patients who appear unable to provideaccurate home BP log

Questions and answers• anemia—present in stage 3 and 4 CKD• look for other causes of anemia (eg, perform colonoscopy if indicated)• proteinuria—surrogate marker for CKD• for patients with 500 to 600 mg of protein to 1 g of creatinine, monitor efficacy of BP treatment• refer patients in nephrotic range (>4000 mg of protein to 1 g of creatinine)• effects of NSAIDs—weigh risks and benefits• Glomerular effects tend to reverse when NSAID stopped• prostaglandin helps maintain vasodilation at afferent arteriole (blocking prostaglandin constricts afferent
arteriole, leading to hypotension within glomerulus)• stopping NSAID restores intraglomerular pressure• NSAIDs toxic at tubular level (ie, can lead to tubular necrosis; less common)• discuss risks with patient• ACE inhibitor can be restarted when patients hemodynamically stable• is one ACE inhibitor better than another?—class effect• some agents more studied than others• most ACE inhibitors (eg, enalapril, ramipril, lisinopril) and most ARBs (eg, telmisartan, candesartan, losartan)
shown beneficial• preeclampsia— risk factor for CKD

















