Establishment of Reference Methodsfor Lipids, Lipoproteins and Apolipoproteins1)
By G. R. Cooper, G. L. Myers and L. O. Henderson
Centers for Disease Control, Public Health Service, U.S. Department of Health and Human Services, Atlanta,Georgia, USA
(Received January 22, 1991)
, Summary: Reference methods for lipids, lipoproteins, and apolipoproteins have been developed for use äspart of an accuracy base .for institutional, national, or international reference Systems. A widely acceptedreference method exists only for total cholesterol. Well described Interim or institutional in-house referencemethods have been established for the other lipids, lipoproteins, and apolipoproteins. The major criteria fora reference method are
1) scientific basis,
2) sound principles,
3) available calibration and control materials,
4) traceability to a definitive method or a point of reference, and
5) applicability to reference materials that provide traceability to clinical methods and transferability to otherreference laboratories.
The total cholesterol reference method of the U. S. National Reference System demonstrates how a referencemethod can be developed and applied. Reference methods now available can lead to an accepted internationalaccuracy base for the clinically useful lipid, lipoprotein, and apolipoprotein measurements.
n ro uc on a reference method and reference material play aReference methods are esseiitial coinponents of the significant role in tränsferring the accuracy base of aaccuracy base of any established reference System for definitive method to the clinical laboratory. Referencelipids, lipoproteins, and apolipoproteins. A stable ac- methods afe considered acceptable when they possesscuracy base depends upon availability, of a stable x ^ . . . .reference method and reference materials. Together, *> known ™mmum bias versus a definitive method,
2) known sound scientific basis,*) Contribution of the International Föderation of Clinical _ N ._ t , t ._ , ,. - ^
Chemistry (IFCC) Working Group on Apolipoprotein Ref- 3) available calibration and quality control referenceerence Methods established at the Centers for Disease Cori- material, andtrol and the IFCC Committee on Apolipoproteins (S. M. . .Marcovina, chairman, /. /. Albers, J. C. Fruchart, M. Ros- 4) traceability to clinical methods and their secondaryseneu, J. Shepherd) of the IFCC Scientific Division (H. Grel· serum reference material.fing, chairman, M. M. Müller, vice chairman).Based on a lecture given at the Symposium "Reference Meth- The more widely available reference methods designedods in Clinical Chemistry - Objectives Trends, Problems" f widespread use and application must be validatedof the Congress Biochemische Analytik 90, München, May ^ *;*;8y 1990 by the less available definitive method (1). A punfied
270 Symposium: Referencc Methods in Clinical Chemistry
primary Standard is required to calibrate the definitivemethod and reference method while commutable sec-ondary serum reference materials are used to calibrateclinical methods of lipids, lipoproteins, and apolipo-proteins. A higher productivity or throughput thanthe definitive method provides is desirable to satisfymultiple demands placed upon a reference method.
Reference methods are developed to assure accuracyof clinically useful laboratory procedures. Proceduresfor lipid, lipoprotein, and apolipoprotein consideredhighly useful to the clinicians in the detection, pre-vention, and control of coronary heart disease andsecondary hyperlipidaemia diseases are quantitativemeasurements of total cholesterol, triacylglycerol,high-density lipoprotein (HDL)2) and low-density li-poprotein (LDL), cholesterol, and apolipoproteins -
and B. These therefore will be discussed here.
Reference methods have been established at the Cen-ters for Disease Control (CDC) for total cholesterol,triacylglycerol, HDL cholesterol, and apolipoproteinA-1 and B (2). The total cholesterol method has beenaccepted äs the total cholesterol reference method ofthe US National Reference System for Cholesterolestablished by the National Committee for ClinicalLaboratory Standards (NCCLS) (3). The US Na.tional Reference System for Cholesterol comprises theisotope dilution and mass spectrometric definitivemethod of the National Institute of Standards andTechnology (NIST) (4), CDC modified Abell-Levy-Brodie—Kendall (5) total cholesterol reference method(6, 7), NIST-certified pure cholesterol Standard, andNIST- and CDC-certified serum based secondary ref-erence material (8). The NCCLS has accepted theCDC in-house reference methods for triacylglyceroland HDL cholesterol äs NCCLS Interim referencemethodological principles for the U. S. National Ref-erence System. CDC and the Committee on Apoli-poproteins of the International Federation of ClinicalChemistry (IFCC) are collaborating in studies de-signed to select candidate reference methods for apo-lipoproteins A-l and B.The total cholesterol reference method will be dis-cussed in greater detail than those of the other lipids,in order to illustrate the characteristics, requisites,and applications of a reference method and its rolein standardization.2) Non-standard abbreviations:
CDC Centers for Disease Control„ NIST National Institute for Standards and Technology
SRM Standard Reference MaterialRIA radioimmunoassayVLDL very low-density lipoproteinIDL intermediate-density lipoproteinLDL low-density lipoproteinHDL high-density lipoprotein
Essential Characteristics of a Reference Method
The major criteria for a reference method are
1) scientific basis,
2) sound principles,• r
3) available calibration and control materials,
4) traceability to a definitive method or a point ofreference,
5) applicability to reference materials that providetraceability to clinical methods, and
6) transferability to(9-12).
other reference laboratories
The scientific basis is judged by accuracy, precison,linearity of dose-response, specificity, stability of re-agents, interferences, recovery, and ruggedness. Soundprinciples demand that each analytical step must bedefined and controlled, possess appropriate sensitiv-ity, permit accurate sampling and dilutions, use stableequipment, cälculate results by accepted procedures,and be subject to acceptable analysis of variaüce. Eachreference method should use a defined purified pri-mary Standard or defined serum biolögicäl referencepreparation for use in calibration or monitoring. Theserum reference materials should have minimum ma-trix effects, be stable over time, and permit validassignment of mass values. Directions for the refer-ence method should be written so clearly that thereference method caii be transferred to other labora-tories without any instructions other than the direc-tions. These essential characteristics form the criteriathat a method must meet to be considered äs a can-didate reference method for the measurement of lip-ids, lipoproteins, and apolipoproteins in serum orother body fluids.
Total Cholesterol Reference Method
In 1975, the Cholesterol Reference Method StudyGroup of the American Associätion for ClinicalChemistry (AACC) invited the CDC to .develop-acandidate total cholesterol reference method. Duringthe five-year develöpment pefiod (1977-1982), fivePotential candidate methods were selected, optimized,and compared. The top two methods (Abell—Levy—Brodie-^-Kendall (5) and an enzymic procedure) wereselected on the basis of these studies, and were thencompared with the NIST-developed Isotope dilution-mass spectrometric definitive method (4). On the basisof these comparisons, the American Associätion forClinical Chemistry Cholesterol Reference MethodStudy Group selected the Abell^ Levy—Brodle—Ken-
Cooper et al.: Reference methods for lipids, lipoproteins and apolipoproteins 271
dall method äs the recommended total cholesterolreference method (5). The Abell—Levy — Brodie —Kendall method was next subjected to extensive vali-dation studies (6) and a transferability study with 14collaborating lipid laboratories throughout theUnited States (7). The transferability study demon-strated that the recommended reference method per-mits laboratories to attain a coefficient of Variation(CV) of less than 1.5% within the laboratory and CVof less than 3.0% among the 14 laboratories. Themean percent bias value of the 14 laboratories com-pared with that of the CDC was less than l % for sixof the 14 laboratories, less than 1.5% for 12, and lessthan 3% for all 14 laboratories (7). Interestingly, apreliminary readiness testing and competence evalu-ation predicted the quality of analytical performanceexhibited during the transferability testing.
The total cholesterol reference method procedure in-| cludes the following steps: a 0.5-ml sample in 20 g/l| alcoholic KOH undergoes hydrolysis at 50 °C for l h;! the hydrolysate is extracted with hexane by vigorous; shaking at 25 °C for 15 min; an aliquot of hexane is1 evaporated in a vacuum oven at 55 °C; colour isdeveloped by reaction with a reagent formed from 20parts acetic anhydride, l part H2SO4, and 10 partsglacial acetic acid at 25 °C for exactly 30 min; and anabsorbance reading is taken at 620 nm in a flow-through cuvette.
Calibration is performed with NIST pure cholesterolStandard reference material 911b (6). Since 1978, an-alytical performance of the total cholesterol referencemethod at CDC has exhibited a CV of less than l %and a bias rarely above 1% on frozen serum pools(tab. 1).
CDC and NIST have collaborated since 1978 to main-tain a defined accuracy base with the CDC referencemethod and the NIST definitive method. Five frozenserum pools were used originally to compare the ref-erence method with the definitive method. The agree-ment between the two methods was considered excel-lent with a difference of less than 1.0% of all fivepools (2). In 1989, comparisons of the referencemethod and definitive method revealed excellentagreement (0.41 %) on Standard Solutions (SRM 91 Ib)and good agreement (1.6%) on fresh, frozen, or ly-ophilized sera (l 3). Unpublished experimental studiesat CDC on potential interferences in the referencemethod indicate that this difference in level of resultsbetween the reference method and definitive methodresults largely from sterols in serum (14).
Since 1961, the CDC total cholesterol referencemethod has served äs a part of the accuracy base forthe CDC-National Heart, Lung, and Blood InstituteLipid Standardization Programme. This accuracybase has been transferred through frozen serum ref-erence materials distributed to the several hundredU.S. participants, äs well äs to many internationallaboratories. The reliability of the reference methodhas made it possible to assure the accuracy of labo-ratories supporting more than 30 cardiovascular epi-demiologic or clinical investigations coordinated byCDC-National Heart, Lung, and Blood Institute,such äs the Coronary Drug Project (15), the LipidResearch Clinics (16), Multiple Risk Factor Interven-tion Trial (17), and the Hypertension Detection andFollow-up Study (18).
The NCCLS's National Reference System for theClinical Laboratory Council has adopted the CDCreference method äs its national reference method forcholesterol (19). The National Reference System forthe Clinical Laboratory Council has designated theNIST definitive method, the CDC reference method,the NIST certified pure cholesterol SRM 911, and theCDC^certified serum-based secondary reference ma-terials äs the components of the National ReferenceSystem for Cholesterol (3).
The National Reference Method Laboratory Networkhas been formed by CDC to provide resources foracourate calibration of manufacturers' total choles-terol analytical diagnostic products and accurate con-firmatory analysis for clinical laboratories (2). Cali-bration with fresh specimens has been necessary forsome of the new total cholesterol reagent analyticalSystems that exhibit matrix effects with liquid, frozen,or lyophilized reference materials. The protocol usedby the Network utilizes the NCCLS recommendationon procedure for comparison of methods using fresh
272 Symposium: Reference Methods in Clinical Chemistry
patient specimens (20). Currently, the network in-cludes nine laboratories in the United States and onein the Netherlands: University of Minnesota, BaylorCollege of Medicine, Wisconsin State Laboratory ofHygiene, Cleveland Clinic Foundation, New YorkState Department of Health, Northwest Lipid Re-search Center in Seattle, Pennsylvania State Depart-ment of Health, Washington University in St. Louis,USDA Nutrition Research Center on Aging at TuftsUniversity, and Rotterdam Academic Hospital. Net-work laboratories must document a CV of less than2% and a bias of less than 1.5% at 3-month intervalsin the CDC-National Heart, Lung, and Blood Insti-tute Lipid Standardization Program.
Interim Triacylglycerol Reference Method
An in-house triacylglycerol reference method was es-tablished at CDC in 1963 on the basis of the methodof Carlson (21, 22) and the techniques of Van Handel& Zilversmii (23) and Lofland (24). The in-housemethod involves silicic acid-chloroform extraction forl h at 25 °C, evaporation of an aliquot in a vacuumoven at 50 °C, chemical hydrolysis with 2.5 g/l alco-holic KOH for 30 min at 70 °C, allowing the solutionto stand overnight at 4 °C after neutralization with0.1 mol/1 H2SO4, colour development by metaperiod-ate-arsenite-chromotropic acid reagent at 95 °C, andreading of the cooled solution in flow cell at 570 nm.The specificity of this method is largely due to thechloroform-silicic acid extraction procedure that re-moves free glycerol and retains minimally monoacyl-glycerol and diacylglycerol. The primary Standard canbe either pure triolein, pure palmitin, or a 2: l mix-ture, respectively. Glycerol or mannitol can be usedäs a primary Standard in calibrating or monitoringthe last step in the method that analyzes the freeglycerol. Laboratories' findings can lack comparabil-ity if different primary Standards are used, unlessresults are expressed in mmol/1. True bias is not
known, because a definitive method is not available.The attainable precision usually ranges between 3%and5%CV(tab.2).
The major problems with the use of this triacylglycerolmethod äs a reference method at CDC are
1) extraction with carcinogenic CHC13,
2) difficulty arising from the presence of silicic acid"fines" or very small pärticles in extracts,
3) impurity, instability and a potentially different de-gree of hydrolysis of different triacylglycerols,
4) unknown commutability of lyophilized referencematerial, and
5) questionable transferability of this chromotropicacid method.
Investigators are searching for a triacylglycerol ref-erence method that may cireumvent these problems'.
This CDC in-house triacylglycerol reference methodhas been designated äs the Interim triacylglycerol can-didate reference method for the National ReferenceSystem and serves äs the selected reference methodfor the CDC-maintained accuracy base for the CDC-National Heart, Lung, and Blood Institute LipidStandardization Programme and for the dedicatedlaboratories of National Heart, Lung, and Blood In-stitute clinical and epidemiologic cardiovascular iii-vestigations and trials.
Interim HDL Cholesterol Reference Method
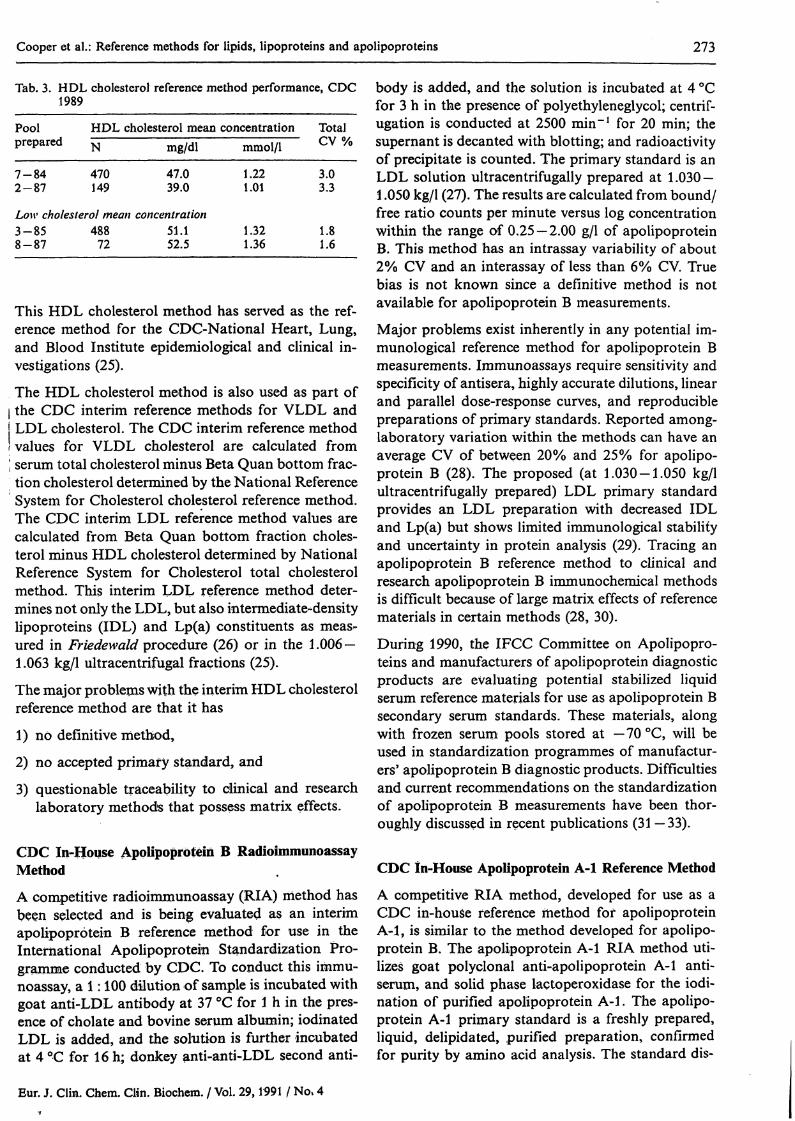
A CDC in-house HDL cholesterol reference methodcombines removal of very low density lipoproteincholesterol (VLDL) by the Beta Quan ultracentrifugalprocedure (25), isolation of HDL cholesterol by pre-cipitation of LDL cholesterol from the l .006 kg/l BetaQuan bottom fraction by 46 mmol/1 manganese and1.3 g/l heparin reagent (25), and cholesterol analysisof the HDL cholesterol supernate by the NationalReference System for Cholesterol total cholesterolreference method (6,7). The primary Standard is NISTcholesterol SRM 911 (8), and it must cover the lowränge öf serum HDL cholesterol values, which isdifferent from the ränge of serum total cholesterol.HDL cholesterol measurements are monitored withboth pure cholesterol and frözen, fresh serum second-ary Standards. Precision for the CDC in-house HDLcholesterol reference method on low cholesterol prl·mary Standards is between 1% and 2% CV, and onfrözen serum secondary reference niaterials, it is be-tween 2.5% and 4% (tab. 3). True bias is not knownbecause a definitive inethod is not available for HDLcholesterol measuremeiits. , *
Cooper et al.: Reference methods for lipids, lipoproteins and apolipoproteins 273
Tab. 3. HOL cholesterol reference method performance, CDC1989
Poolprepared
7-842-87
HDL cholesterol meanN mg/dl
470 47.0149 39.0
concentrationmmol/1
1.221.01
TotalCV %
3.03.3
Low cholesterol mean concentration3-858-87
488 51.172 52.5
1.321.36
1.81.6
This HDL cholesterol method has served äs the ref-erence method for the CDC-National Heart, Lung,and Blood Institute epidemiological and clinical in-vestigations (25).
The HDL cholesterol method is also used äs part ofl the CDC interim reference methods for VLDL andj LDL cholesterol. The CDC interim reference method! values for VLDL cholesterol are calculated fromI serum total cholesterol minus Beta Quan bottom frac-tion cholesterol determined by the National ReferenceSystem for Cholesterol cholesterol reference method.The CDC interim LDL reference method values arecalculated from Beta Quan bottom fraction choles-terol minus HDL cholesterol determined by NationalReference System for Cholesterol total cholesterolmethod. This interim LDL reference method deter-mines not only the LDL, but also intermediate-densitylipoproteins (IDL) and Lp(a) constituents äs rneas-ured in Friedewald procedure (26) or in the l .006 —1.063 kg/l ultracentrifugal fractions (25).
The major problems with the interim HDL cholesterolreference method are that it has
1) nö definitive method,
2) no accepted primary Standard, and
3) questionable traceability to clinical and researchlaboratory methods that possess matrix effects.
CDC In-House Apolipoprotein B RadioimmunoassayMethodA competitive radioimmunoassay (RIA) method hasbeen selected and is being evaluated äs an interimapolipoprotein B reference method for use in theInternational Apolipoprotein Standardization Pro-gramme conducted by CDC. To conduct this immu-noassay, a l: 100 dilution of sample is incubated withgoat anti-LDL antibody at 37 °C for l h in the pres-ence of cholate and bovine serum albumin; iodinatedLDL is added, and the solution is further incubatedat 4 °C for 16h; donkey anti-anti-LDL second anti-
body is added, and the solution is incubated at 4 °Cfor 3 h in the presence of polyethyleneglycol; centrif-ugation is conducted at 2500 min""1 for 20 min; thesupernant is decanted with blotting; and radioactivityof precipitate is counted. The primary Standard is anLDL solution ultracentrifugally prepared at 1.030 —l .050 kg/l (27). The results are calculated from bound/free ratio counts per minute versus log concentrationwithin the ränge of 0.25 — 2.00 g/l of apolipoproteinB. This method has an intrassay variability of about2% CV and an interassay of less than 6% CV. Truebias is not known since a definitive method is notavailable for apolipoprotein B measurements.
Major problems exist inherently in any potential im-munological reference method for apolipoprotein Bmeasurements. Immunoassays require sensitivity andspecificity of antisera, highly accurate dilutions, linearand parallel dose-response curves, and reproduciblepreparations of primary Standards. Reported among-laboratory Variation within the methods can have anaverage CV of between 20% and 25% for apolipo-protein B (28). The proposed (at 1.030-1.050 kg/lultracentrifugally prepared) LDL primary Standardprovides an LDL preparation with decreased IDLand Lp(a) but shows limited immunological stabilityand uncertainty in protein analysis (29). Tracing anapolipoprotein B reference method to clinical andresearch apolipoprotein B immunochemical methodsis difficult because of large matrix effects of referencematerials in certain methods (28, 30).
During 1990, the IFCC Committee on Apolipopro-teins and manufacturers of apolipoprotein diagnosticproducts are evalüating potential stabilized liquidserum reference materials for use äs apolipoprotein Bsecondary serum Standards. These materials, alongwith frozen serum pools stored at — 70 °C, will beused in Standardization programmes of manufactur-ers' apolipoprotein B diagnostic products. Difficultiesand current recommendations on the Standardizationof apolipoprotein B measurements have been thor-oughly discussed in recent publications (31 —33).
CDC In-House Apolipoprotein A-l Reference Method
A competitive RIA method, developed for use äs aCDC in-house reference method for apolipoproteinA-l, is similar to the method developed for apolipo-protein B. The apolipoprotein A-l RIA method uti-lizes goat polyclonal anti-apolipoprotein A-l anti-serum, and solid phase lactoperoxidase for the iodi-nation of purified apolipoprotein A-l. The apolipo-protein A-l primary Standard is a freshly prepared,liquid, delipidated, purified preparation, confirmedfor purity by amino acid analysis. The Standard dis-
274 Symposium: Referencc Methods in Clinical Chemistry
placement curve ranges between 0.50 and 2.0 g/l whereserum samples are diluted l : 100 in one Step. Precisionmeasurements give an intra-assay CV of about 2%,and an inter-assay CV of less than 6%. Tracing clin-ical methods to a reference method for apolipoproteinA-l should not be difficult since among-methodsource of Variation is negligible for apolipoprotein Α-Ι measurements (28).
A lyophilized, purified, and delipidated proposed apo-lipoprotein A-l primary Standard is currently beingevaluated by the European Cummunity Bureau ofReference in Br ssels and the IFCC Committee onApolipoproteins. Manufacturers of apolipoprotein di-agnostic products and this IFCC committee are col-laborating to develop a commutable lyophilized apo-lipoprotein A-l serum secondary Standard. This proj-ect seeks to gain comparability of results among com-
mercial apolipoprotein A-l diagnostic products. TheCDC is supporting this effort by analysing these ref-erence materials with the RIA method and studyingPotential primary Standards and their problems.
Conclusions - r
A reference method has been developed for totalcholesterol for national and international referenceSystems. Interim reference methods are being used fortriacylglycerol, HDL cholesterol and LDL cholesterolmeasurements. Potential candidate reference methodsare being developed and evaluated for apolipoproteinΑ-Λ and B measurements by different apolipoproteininvestig tors. Continuing worldwide efforts to im-prove the methodology should lead to an acceptedinternational accuracy base for the clinically usefullipid, lipoprotein, and apolipoprotein measurements.
References1. Brown, S. S., B ttner, J., Mitchell, F. L., Rubin, M. &
Cooper, G. R. (1976) Response to Neu, D. W. & Doggart,J. R. When is a Reference Method a Reference Method?Clin. Chem. 22, 285-286.
2. Myers, G. L., Cooper, G. R., Winn, C. L. & Smith, S. J.(1989) The Centers for Disease Control-National Heart,Lung, and Blood Institute Lipid Standardization Program:An Approach to Accurate and Precise Lipid Measurements.In: Cholesterol Screening (Rifkind, B. M. & Lippel, K.,eds.) pp. 105-136, W.B. Saunders Co., Philadelphia.
3. Vanderlinde, R. E., Bowers, G. N., Schaffer, R. & Edwards,G. C. (1989) The National Reference System for Choles-terol. In: Cholesterol Screening (Rifkind, B. M. & Lippel,K., eds.) pp. 89-104, W.B. Saunders Co., Philadelphia.
4. Cohen, A., Hertz, H. S., Mandel, J., Paule, R. C., Schaffer,R., Sniegoski, L. T, Sun, T, Welch, M. J. & White, E. V.(1980) Total Serum Cholesterol by Isotope Dilution-MassSpectrometry: A Candidate Definitive Method. Clin. Chem.26, 854-860.
5. Abell, L. L., Levy, B. B., Brodie, B. B. & Kendall, F. E.(1952) A Simplified Method for the Estimation of TotalCholesterol in Serum and Demonstration of its Specificity.J. Biol. Chem. 195, 357-366.
6. Duncan, I. W., Mather, A. & Cooper, G. R. (1982) TheProcedure for the Proposed Cholesterol Reference Method.Lipid Standardization Activity, Center for EnvironmentalHealth, Centers for Disease Control, MS F20, Atlanta,Georgia 30333.
7. Cooper, G. R., Smith, S. J., Duncan, I. W, Mather, A.,and 14 collaborating groups (1986) Interlaboratory Testingof the Transferability of a Candidate Reference Method forTotal Cholesterol in Serum. Clin. Chem. 32, 921-929.
8. National Institute of Standards and Technology, Office ofStandard Reference Materials, Gaithersburg, Maryland,20899.
9. National Committee for Clinical Laboratory Standards(1984) Tentative Guideline NRSCC-T. Development of Ref-erence Methods in Clinical Chemistry for the NationalReference System. NCCLS, Villanova, Pennsylvania 19085
10. Stender, S. (1989) Reference methods - with Special Ref-erence to Cholesterol. Scand. J. Clin. Lab. Invest. 49 (Suppl194), 63-67. FF"
11. Stamm, D. (1979) Reference Materials and ReferenceMethods in Clinical Chemistry. J. Clin. Chem. ClinBiochem. 77,283-287.
12. Boutwell, J. H. (1978) Proceedings of the Conference on aNational Understanding for the Development of ReferenceMaterials and Methods for Clinical Chemistry meeting.American Association for Clinical Chemistry, Washington,D. C. 20006.
13. Ellerbe, P., Myers, G. L., Cooper, G. R., Hertz, H. S.,Sniegoski, L. T., Welch, M. J. & White, E. V. (1990) ACornparison of Results for Cholesterol in Human SerumObtained by the Reference Method and by the DefinitiveMethod of the National Reference System for Cholesterol.Clin. Chem. 36,370-375.
14. Bernert, J. T. Jr. (1990) Evaluation of the Accuraey of theNRS Total Cholesterol Reference Method. Clin. Chem. (Inpress)
15. Coronary Drug Project Research Group (1975) Clofibrateand Niacin in Coronary Hear't Disease. J. Am. Med. Ass.257, 360-381.
16. Lipid Research CHnics Program (1984) The Lipid ResearchClinics Coronary Primary Prevention Trial Results. Reduc-tion in Incidence of Coronary Heart Disease. J. Am. Med.Ass. 257, 351-364.
17. Multiple Risk Factor Intervention Trial Research Group(1982) Multiple Risk Factor Intervention Trial: Risk FactorChanges and Mortality Results. J. Am. Med. Ass. 248,1465-1477.
18. Hypertension Detection and Follow-up Program Cooper-ative Group (1979) Five-year Findings of the HypertensionDetection of Follow-up Program. I. Reduction in Mortalityof Persons with High Blood Pressure, including Mild Hy-pertehsion. J. Am. Med. Ass. 242, 2562-2577.
19. National Committee for Clinical Laboratory' Standards(1987) NCCLS Document RS3-A. Cholesterol: ApprovedSummary of Methods and Materials Credentialed by theNRSCL Council. NCCLS, Villanova, Pennsylvania 19085.
20. National Committee for Clinical Laboratory Standards(1986) NCCLS Document EP9-P. User Comparison ofQuantitative Clinical Laboratory Methods. using PatientSamples. NCCLS, Villanova, Pennsylvania 19085.
21. Carlson, L. A. & Wadstrom, L. B. (1959) Determinationof Glycerides in Blood Serum. Clin, Chim. Acta 4, 197-205.
22. Carlson, L. A. (1963) Determination of Serum Triglycer-„ ides. J. Atherosclerosis Res. 3, 334—336.
23. Van Handel, E. & Zilversmit, D, .B. (1957) Micromethodfor the Direct Determination of Tfiglycerides. J. Lab. Clin.Med. 50, 152-157.
Cooper et al.: Rcference methods fbr lipids, lipoproteins and apolipoproteins 275
24. Lofland, H. B. Jr. (1964) A Semiaulomated Procedure forthe Determination of Triglycerides in Serum. Anal.Biochem. 9, 393-400.
25. Lipid Research Clinics Program (1982) Hainline, A. Jr.,Karon, J. & Lippel, K. (eds.) Manual of Laboratory Op-erations, Lipid and Lipoprotein Analysis, 2nd ed., HEWPubl. No. (NIH) 75-628 (revised). National Heart, Lung,and Blood Institute Bethesda, Maryland (U. S. GovernmentPrinting Office No. 1982-361-132:678).
26. Friedewald, W.T., Levy, R. 1. & Fredrickson, D.S. (1972)Estimation of the Concentration of Low-Density Lipopro-tein Cholesterol in Plasma, Without the Use of the Prepa-rative Ultracentrifuge. Cün. Chem. 18, 499-502.
27. Albers, J. J., Lodge, M. S. & Curtiss, L. K. (1989) Evalu-ation of a Monoclonal Antibody-based Linked Immuno-sorben t Assay äs a Candidate Reference Method for theMeasurement of Apolipoprotein B-100. J. Lipid Res. 30,1445-1458.
28. Smith, S. J., Henderson, L. O., Hannon, W. H. & Cooper,G. R. (1990) Effects of Analytical Method and LyophilizedSerum on Measurements of Apolipoproteins A-l and B:An International Study. Clin. Chem. 36, 290—296.
29. Henderson, L. O., Powell, M. K., Smith, S. J., Hannon,W. H., Cooper, G. R. & Marcovina, S. M. (1990) Impactof Protein Measurements on Standardization of Apolipo-proteins A-l and B Assays. Clin. Chem. 36, 1911-1917.
30. Marcovina, S. M., Adolphson, J. L., Parlavecchia, M. &Albers, J. J. (1990) Effects of Lyophitization of Serum onthe Measurements of Apolipoprotein A-l and B. Clin.Chem. 36, 366-369.
31. Albers, J. J. & Marcovina, S. M. (1989) Standardizationof Apolipoprotein B and A-l Measurements. Clin. Chem.35, 1357-1361.
32. Marcovina, S. M. & Albers, J. J. (1989) Guidelines for theStandardization of the Immunochemical Determination ofApolipoprotein A-l and B. IFCC Meeting for Standard-ization of Apolipoprotein A-l and B Measurements, (basisfor future consensus), Vienna, Austria, April 18 — 19, 1989.Clin. Chem. 35, 2009-2015.
33. Cooper, G. R., Smith, S. J., Henderson, L. O., Hannon,W. H. (1988) Standardization of Apolipoprotein Measure-ments. In: Recent aspects of diagnosis and treatment oflipoprotein disorders: impact of prevention of atheroscleroticdiseases (Widhalm, K. & Naito, H. K., eds.) pp. 155-174,Alan R. Liss, New York.
Dr. Gerald R. CooperCenters for Disease ControlMailstop: F20AtlantaGeorgia 30333U. S. A.