Page 1
1
Ethics & Decision MakingEthics & Decision Making
a case of providing RRT in Thailanda case of providing RRT in Thailand
Yot Teerawattananon
International Health Policy Program
Journal club, 17 March 2006
Page 2
2
Background
• Introduction of universal health
insurance (NHS-like system) in 2001
• Dialysis for chronic renal disease
(CRD) was excluded from the health
service package
• Disease incidence is 10,000
patients/year. Only 5% of patients with
CRD can afford for dialysis (~ £6,000
per year)
Page 3
3
VS.
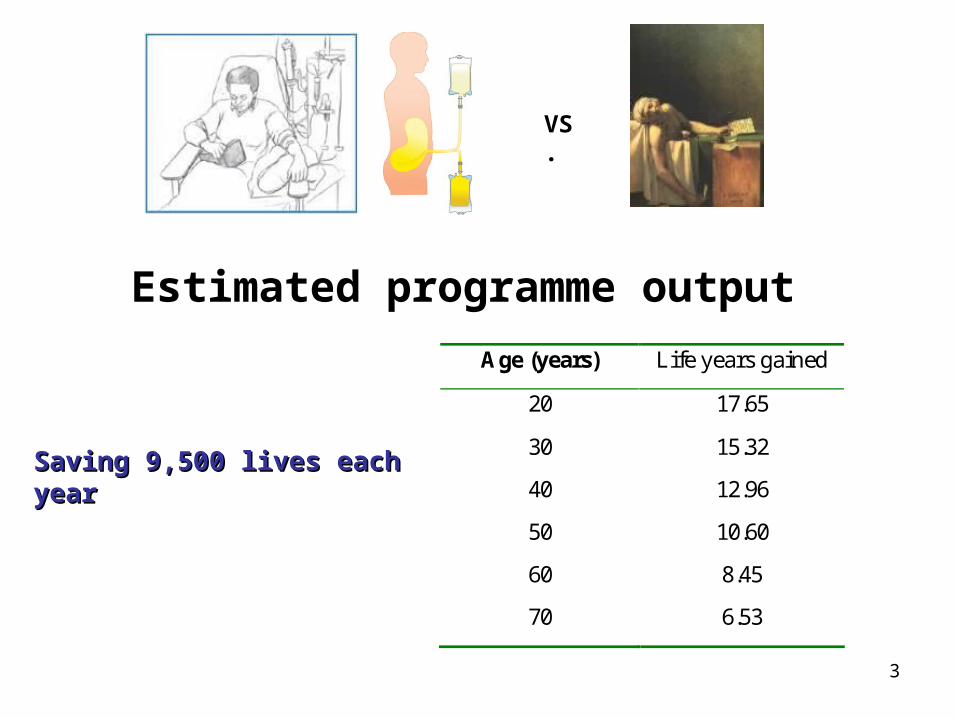
Age (years) Life years gained
20 17.65
30 15.32
40 12.96
50 10.60
60 8.45
70 6.53
Estimated programme output
Saving 9,500 lives each yearSaving 9,500 lives each year
Page 4
4
Cost effectiveness analysis– Renal Replacement Therapy (RRT)
• Cost per life year saved (Teerawattananon et al 2005)– Peritoneal dialysis 10,170 US$
– Hemodialysis 10,490 US$
– Anti Retroviral Therapy - ART • Cost per life year saved (Lertiendumrong et al 2005)
– Antiretroviral Therapy 590 US$
– GNI Thailand • US$ 2,540 per capita (2006 WDR)
– RRT is not cost-effective, as cost per life year saved is • 4 times of GNI per capita,
• 18 times as expensive as the current national ART program.
Page 5
5
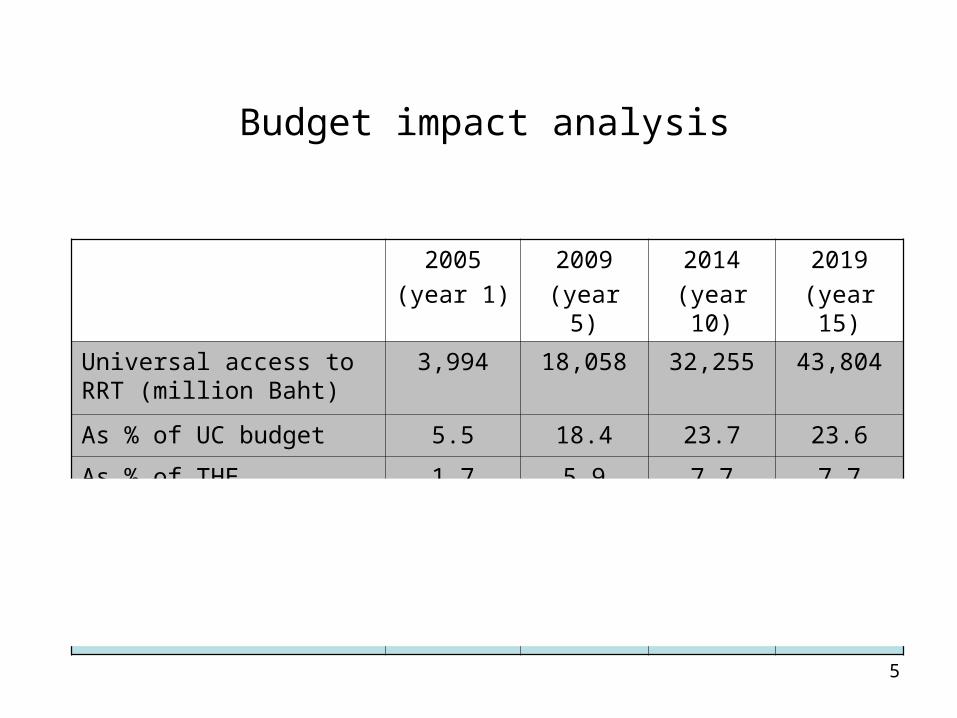
Budget impact analysis
2005
(year 1)
2009
(year 5)
2014
(year 10)
2019
(year 15)
Universal access to RRT (million Baht)
3,994 18,058 32,255 43,804
As % of UC budget 5.5 18.4 23.7 23.6
As % of THE 1.7 5.9 7.7 7.7
RRT for KT eligible (mil Baht)
1,981 8,944 15,966 21,625
As % of UC budget 2.7 9.1 11.7 11.7
As % of THE 0.9 2.9 3.8 3.8
Page 6
6
Question?
Given resource constraints and substantial budget is needed to spend on dialysis programme, is the programme justifiable on ethical and moral grounds?
Page 7
7
Options
Fund the dialysis programmeNot fund the dialysis
programme but spend on other cost-effective programme
Page 8
8
Options
Fund the dialysis programmeNot fund the dialysis
programme but spend on other cost-effective programme
Saving lives regardless its cost
Page 10
10
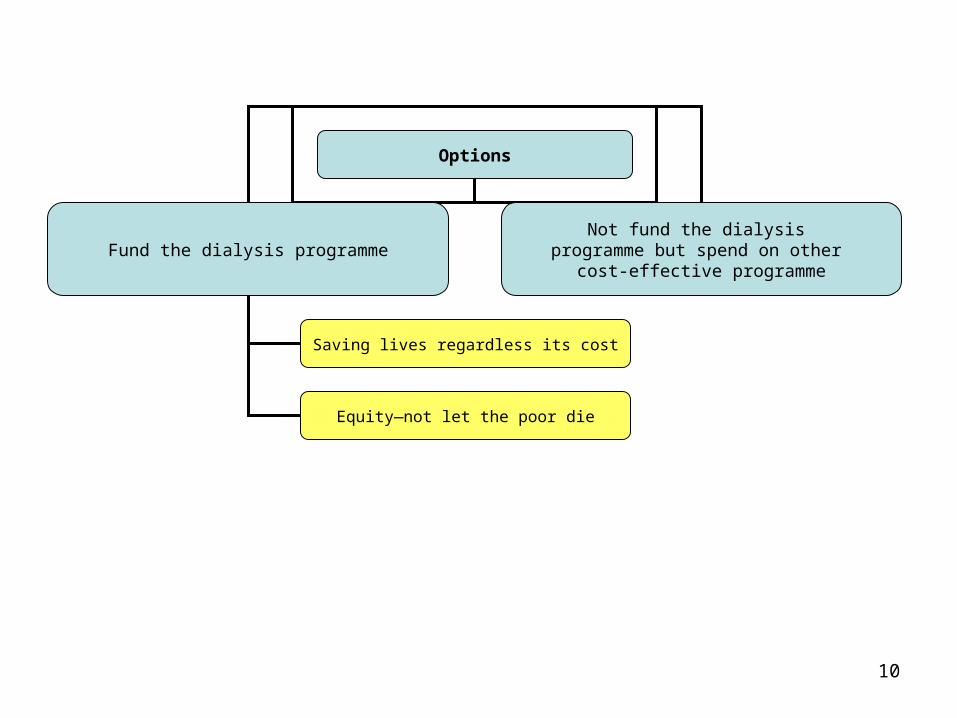
Options
Fund the dialysis programmeNot fund the dialysis
programme but spend on other cost-effective programme
Saving lives regardless its cost
Equity—not let the poor die
Page 11
11
Options
Fund the dialysis programmeNot fund the dialysis
programme but spend on other cost-effective programme
Saving lives regardless its cost
Equity—not let the poor die
Share risks and benefits
Page 12
12
We should not let some people in our society suffered without help!
Page 13
13
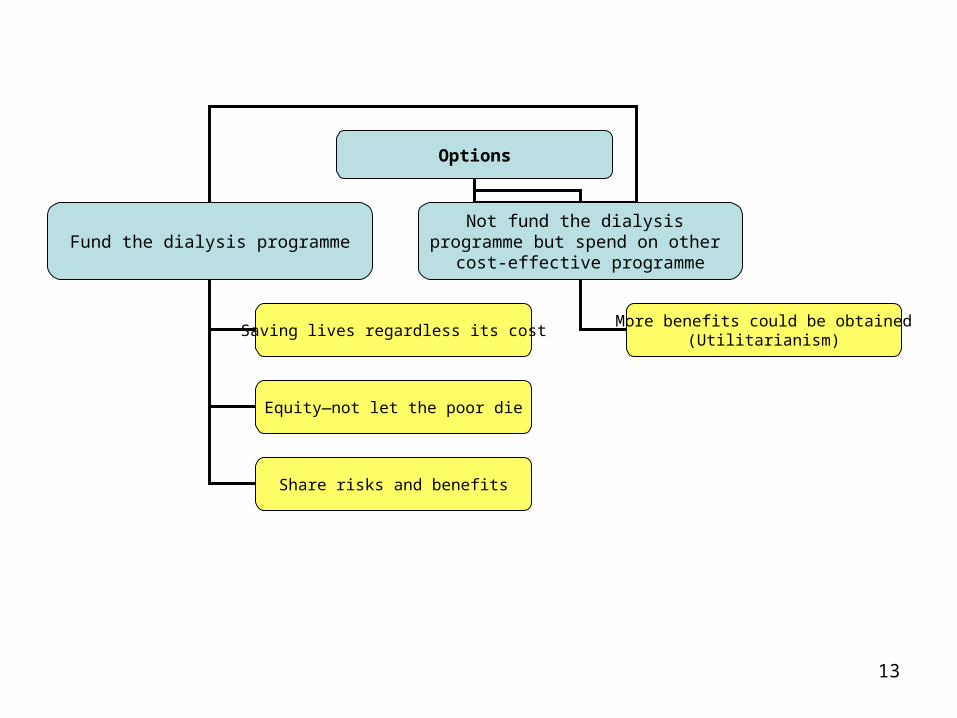
Options
Fund the dialysis programmeNot fund the dialysis
programme but spend on other cost-effective programme
Saving lives regardless its cost
Equity—not let the poor die
Share risks and benefits
More benefits could be obtained(Utilitarianism)
Page 14
14
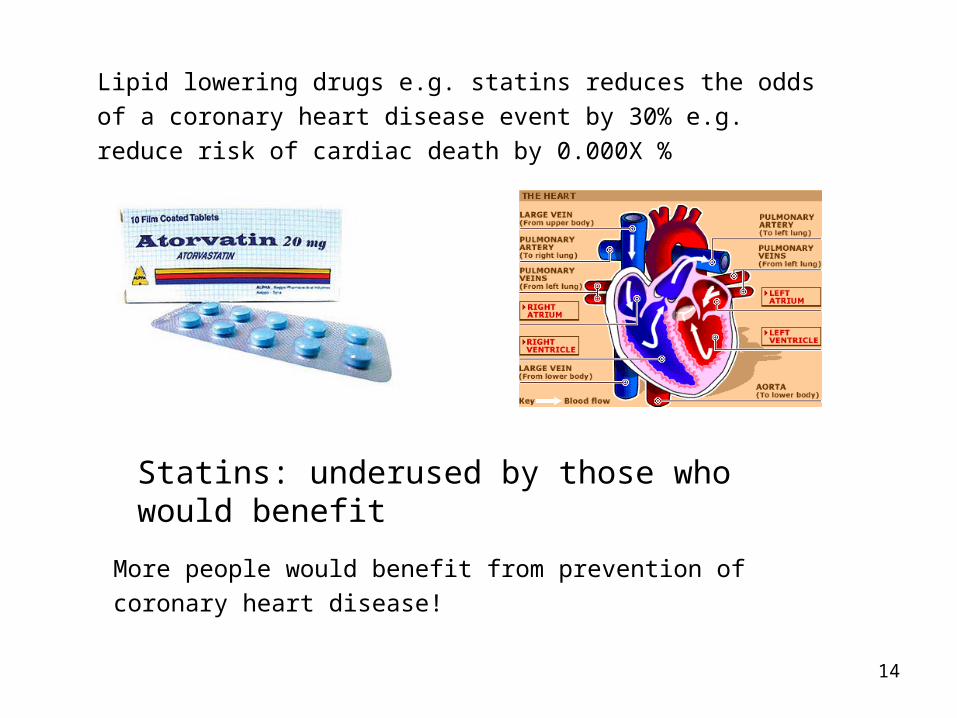
Statins: underused by those who would benefit
More people would benefit from prevention of coronary heart disease!
Lipid lowering drugs e.g. statins reduces the odds of a coronary heart
disease event by 30% e.g. reduce risk of cardiac death by 0.000X %
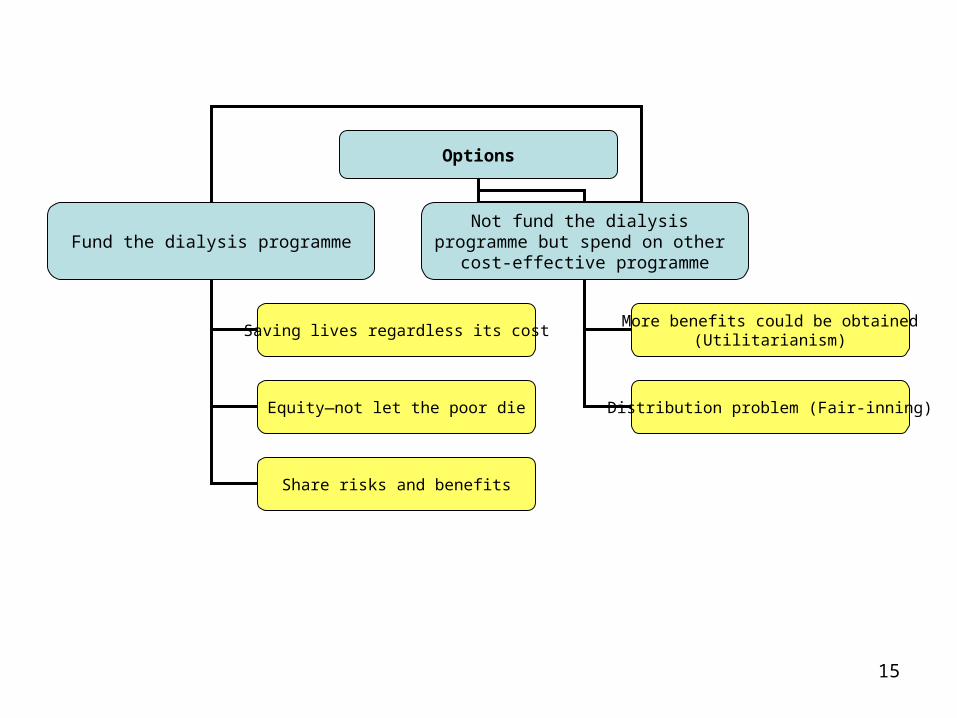
Page 15
15
Options
Fund the dialysis programmeNot fund the dialysis
programme but spend on other cost-effective programme
Saving lives regardless its cost
Equity—not let the poor die
Share risks and benefits
More benefits could be obtained(Utilitarianism)
Distribution problem (Fair-inning)
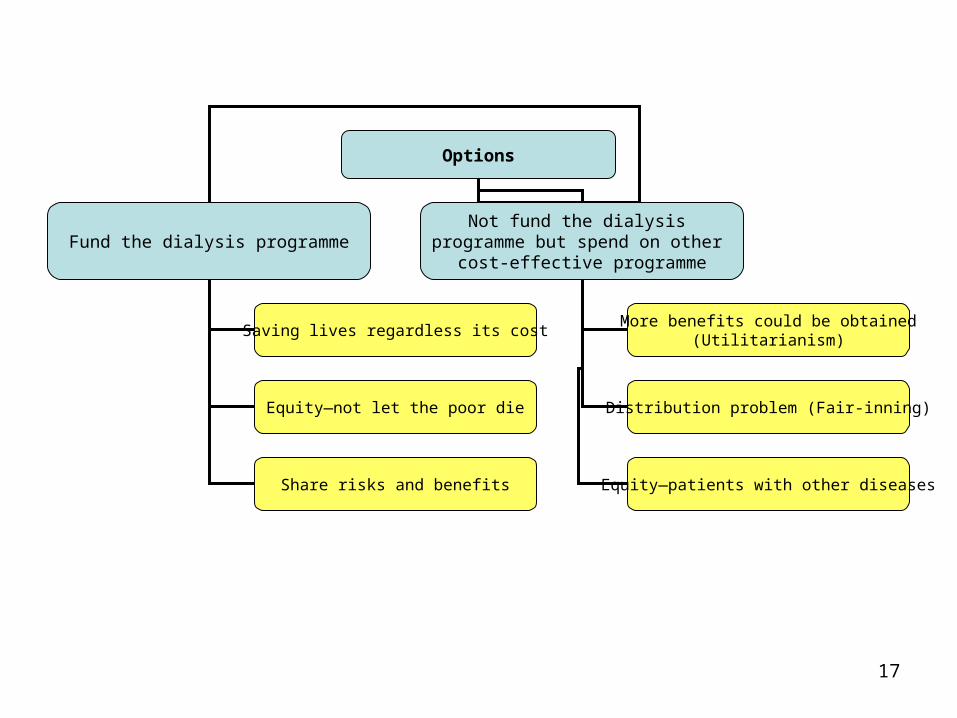
Page 17
17
Options
Fund the dialysis programmeNot fund the dialysis
programme but spend on other cost-effective programme
Saving lives regardless its cost
Equity—not let the poor die
Share risks and benefits
More benefits could be obtained(Utilitarianism)
Distribution problem (Fair-inning)
Equity—patients with other diseases
Page 19
19
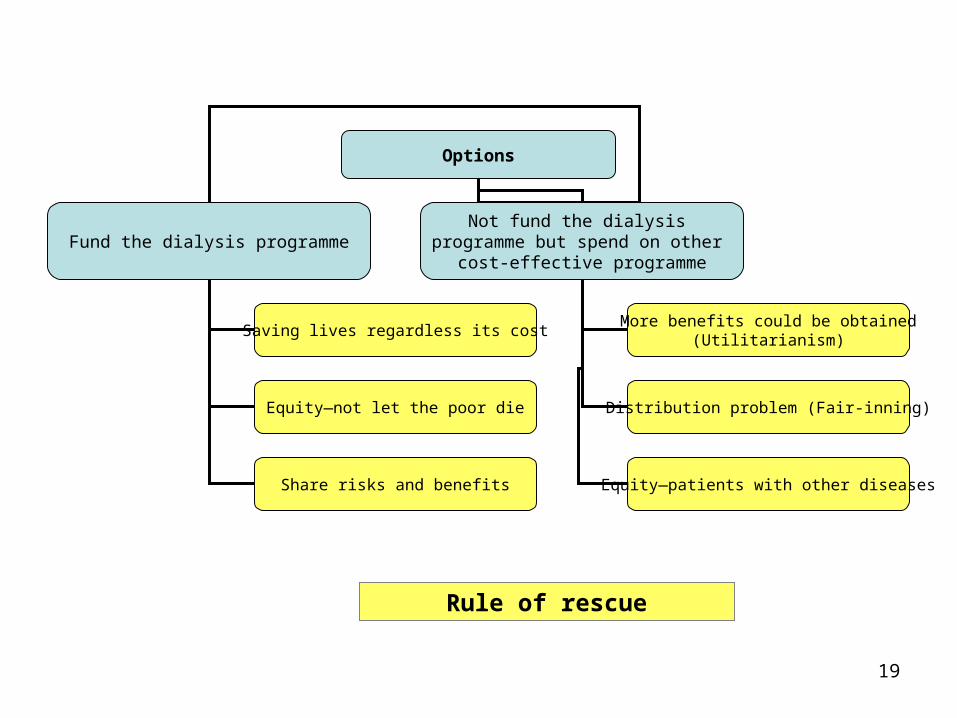
Options
Fund the dialysis programmeNot fund the dialysis
programme but spend on other cost-effective programme
Saving lives regardless its cost
Equity—not let the poor die
Share risks and benefits
More benefits could be obtained(Utilitarianism)
Distribution problem (Fair-inning)
Equity—patients with other diseases
Rule of rescue
Page 20
20
The rule of rescue
• There is an identified person whose life is
at risk
• There exists an intervention which has a
good change of saving the person’s life
• It is justified to save this person’s life
rather than others who cannot be identified
e.g. a case of lipid lowering drugs
Page 21
21
For• Death is a very
significant harm but a very small chance of death is by no mean a great harm
• In our lives, all of us trades small increase in the chance of death against really quite small benefits!
Page 22
22
AgainstA women trapped in a house-fired. Without rescue she will die. She
can be saved if a large number of people doing a rescue. Do you
think you will join/support?
-If you face 1:1000 risk of death in doing so
-if 3,000 people joining the rescue
Page 24
24
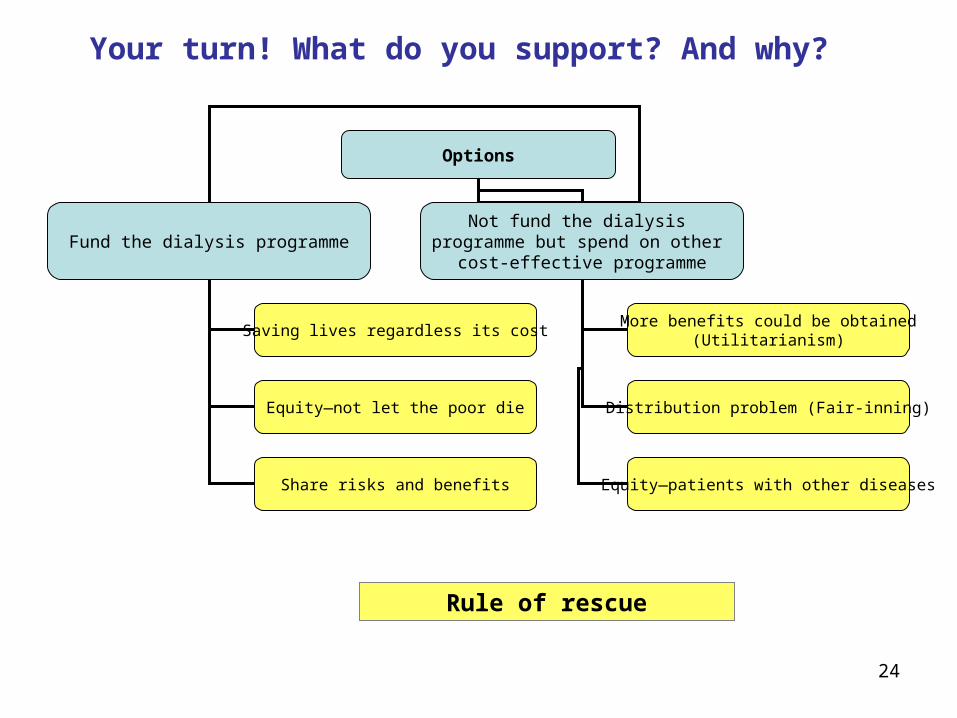
Options
Fund the dialysis programmeNot fund the dialysis
programme but spend on other cost-effective programme
Saving lives regardless its cost
Equity—not let the poor die
Share risks and benefits
More benefits could be obtained(Utilitarianism)
Distribution problem (Fair-inning)
Equity—patients with other diseases
Rule of rescue
Your turn! What do you support? And why?
Page 25
25
Utilitarianism vs. Kant’s moral theory
Page 26
26
Utilitarianism
• The conversion of all things is to
happiness or pleasure or utility
• Everything has a common denominator—
ready-made formula for assessing of what
one should do morally
• It downplays respect, human dignity,
individual rights etc.
Page 27
27
Checking utilitarianism
• A case of Somsri and her rich uncle
Page 28
28
Kant’s moral theory
• The will to do the right thing only for the sake of doing the right thing regardless of its consequences
• The moral principle should be ‘universalizable’ and ‘categorical imperative’
Page 29
29
Checking Kant’s moral theory
• A case of Somchai and a hiding would-be victim for a pursuing criminal
Page 30
30
Reference1. Thomson A. Critical reasoning in ethics: a practical introduction.
London: Routledge, 1999.
2. Hope T. Medical ethics: a very short introduction. Oxford: Oxford
University Press, 2004.
3. Cookson R, Dolan P. Principles of justice in health care rationing. J
Med Ethics 2000;26(5):323-9.
4. Pinkerton SD, Johnson-Masotti AP, Derse A, Layde PM. Ethical issues
in cost-effectiveness analysis. Evaluation and Program Planning
2002;25(1):71-83.
5. Pignone M, Phillips C, Mulrow C. Use of lipid lowering drugs for
primary prevention of coronary heart disease: meta-analysis of
randomised trials 10.1136/bmj.321.7267.983. BMJ
2000;321(7267):983-986.